Back to Journals » International Medical Case Reports Journal » Volume 15
Coexistent Lichen Amyloidosis and Acquired Reactive Perforating Collagenosis in Type 2 Diabetes Mellitus and Post-Thyroidectomy Hypothyroidism Due to Papillary Thyroid Carcinoma: A Rare Case
Authors Sutedja EK ![]() , Widjaya MRH
, Widjaya MRH ![]() , Dharmadji HP, Achdiat PA
, Dharmadji HP, Achdiat PA ![]() , Tsaqilah L
, Tsaqilah L ![]()
Received 29 September 2022
Accepted for publication 6 December 2022
Published 20 December 2022 Volume 2022:15 Pages 745—752
DOI https://doi.org/10.2147/IMCRJ.S391199
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Eva Krishna Sutedja, Muhamad Radyn Haryadi Widjaya, Hartati Purbo Dharmadji, Pati Aji Achdiat, Laila Tsaqilah
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia
Correspondence: Eva Krishna Sutedja, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel/Fax +62222032426 ext. 3449, Email [email protected]
Abstract: An abundance of endocrine receptors is expressed on the skin and becomes the target of many hormones. This was associated with various skin diseases that might occur in some endocrine diseases eg, lichen amyloidosis (LA) and acquired reactive perforating collagenosis (ARPC). Here, we report a coexistent LA and ARPC in a 55-year-old woman, characterized with multiple pruritic hyperkeratotic papules and plaques on both arms accompanied by pruritic hyperkeratotic papules and nodules on both legs. She had a history of type 2 diabetes mellitus (DM) and post-thyroidectomy hypothyroidism due to papillary thyroid carcinoma. Histopathological examination revealed amyloid deposition in the papillary dermis corresponding with LA and cup-shaped epidermal depression filled with collagen corresponding with ARPC. The hyperkeratotic papules and nodules flattened in one month after application of 0.05% clobetasol propionate ointment with occlusion on both arms and 0.05% retinoic acid gel on both legs. Hyperkeratotic papules, nodules, and plaques in a patient with a history of endocrine diseases, such as type 2 DM and thyroid disorders should undergo histopathological examination to confirm the diagnosis of skin diseases eg, LA or ARPC.
Keywords: acquired reactive perforating collagenosis, diabetes mellitus, hypothyroidism, lichen amyloidosis, papillary thyroid carcinoma
Introduction
Skin is the largest organ in the human body with 2-m2 surface area, accounting for 15% of total body mass. The main functions of human skin are to regulate the temperature and water content, to be involved in the functioning of the nervous system, and to protect the organism from mechanical injuries, microorganisms, substances, and radiation present in the environment.1 The skin also has various endocrine receptors which become the target of several hormones.2 Various skin diseases can coexist with endocrine system disorders. Some of these skin diseases are primary localized cutaneous amyloidosis (PLCA) and acquired perforating dermatosis (APD).3
Amyloidosis is a group of diseases caused by the deposition of misfolded protein, called amyloid, in certain tissues. The amyloid deposition that is confined to the skin is called PLCA. Based on the clinical manifestations, PLCA is divided into macular amyloidosis (MA), lichen amyloidosis (LA), and biphasic amyloidosis (BA). LA is the most common type of PLCA, accounting for 35% of all PLCA cases.4 Cases of LA are characterized by itchy hyperkeratotic papules and plaques, especially on the extremities.5 This skin disease is a manifestation of rearranged during transfection (RET) protein mutation in multiple endocrine neoplasia type 2A (MEN2A), in addition to medullary thyroid carcinoma, pheochromocytoma, hyperparathyroidism, and Hirschprung’s disease.6 However, LA can also occur without MEN2A, such as the case of LA in papillary thyroid carcinoma reported by Sangen et al7 in Osaka, Japan, in 2002.
Acquired perforating dermatosis is a skin disorder characterized by transepidermal elimination of the connective tissue component of the dermis.8 It is divided into four subtypes, which are acquired reactive perforating collagenosis (ARPC), serpiginous perforating elastosis (EPS), Kyrle’s disease (KD), and perforating folliculitis (PF).9,10 The clinical features of papules and hyperkeratotic nodules of the four subtypes are difficult to distinguish clinically. These four subtypes of APD can be distinguished based on the eliminated dermal component revealed by histopathological examination, which is collagen in ARPC, keratotic material without collagen and elastin in KD, and follicular components with or without collagen and elastin in PF.10 Kim et al11 reported that ARPC was the most common subtype of APD, occurring in 73.3% of 30 APD patients at Eulji General Hospital and Chung Ang University Hospital. Collagen is the eliminated dermal connective tissue component in ARPC.9,10,12 Zhang et al13 described ARPC cases occurring in several endocrine diseases, including 92 cases of diabetes mellitus (DM) and 4 cases of hypothyroidism. Yazdi et al12 reported a case of ARPC in a 30-year-old woman with DM and papillary thyroid carcinoma. The coexistence of ARPC and LA has not been previously reported. This case report aims to describe coexistent ARPC and LA in a patient with type 2 DM and post-thyroidectomy hypothyroidism due to papillary thyroid carcinoma.
Clinical Case
A 55-year-old Indonesian woman of the Sundanese ethnicity came for treatment at the Geriatric and Non-Infection Clinic of the Dermatology and Venereology Department, Dr Hasan Sadikin General Hospital with the main complaint of multiple papules and rough brown patches on both arms accompanied by itchy black papules on both legs.
History-taking revealed that the complaint started five years prior to consult, initially presenting as pruritic hyperkeratotic papules on both arms. These hyperkeratotic papules multiplied and aggregated to form several hyperkeratotic plaques within two months. Two years prior to treatment, the patient complained of multiple pruritic hyperkeratotic papules and nodules on both legs. Pruritus was intermittent, unrelated to temperature, sweat, or sun exposure. In the last month before treatment, the hyperkeratotic papules and nodules increased. The patient had a history of type 2 DM with uncontrolled blood glucose and HbA1C levels. Two years before treatment, the patient underwent thyroidectomy for papillary thyroid carcinoma and she was routinely followed up for the ablation therapy. She was diagnosed with hypothyroidism after thyroidectomy. Every month, the patient still visited the Internal Medicine Clinic of Dr. Hasan Sadikin General Hospital regularly. Medical record data showed that the patient’s fasting blood glucose, two-hour post-prandial blood glucose, and HbA1c levels always exceeded the normal values ranging from 7 to 10%.
Upon physical examination, the patient was found to be overweight. Dermatological status showed multiple papules and hyperkeratotic plaques, scale, lichenification, and hyperpigmented macules, some confluent, measuring 0.2×0.2 cm to 1×1 cm and 0.2×0.2x0.1 cm to 5x5x0.3 cm in size, well-defined, partially raised, dry, located regionally on the extensor surfaces of both arms (Figures 1A and B). On the extensor surfaces of both legs, multiple hyperkeratotic papules and nodules, scale, and hyperpigmented macules were seen, partially discrete, ranging from 0.2×0.2 cm to 1×1 cm and 0.2×0.2x0.1 cm to 0, 5×0.5x0.3 cm, well-defined, partially raised, dry. The Koebner phenomenon was identified (Figures 2A–C).
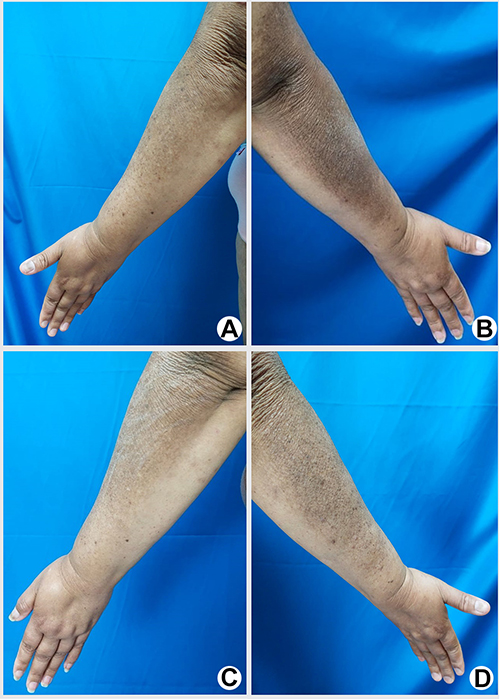 |
Figure 1 (A and B) Hyperkeratotic papules and plaques, scales, lichenification, and hyperpigmented macules on the extensor surfaces of both arms.(C and D). Clinical improvement after the 3rd month of observation. |
 |
Figure 2 (A–C) Hyperkeratotic papules and nodules, scales, and hyperpigmented macules on the extensor surfaces of both legs. (D–F) Clinical improvement after the 3rd month of observation. |
A 6-mm punch biopsy was performed on the hyperkeratotic papule on the left forearm and right leg for histopathological examination. The patient was given topical 10% urea cream to be applied twice daily on the whole body and oral 10 mg loratadine for pruritus. In the first month of observation, the pruritus was reduced but the skin lesions had not improved. Histopathological examination with hematoxylin-eosin (HE) staining from the lesion on the left arm showed an eosinophilic mass deposit in the dermal papillae, covered with hyperkeratotic and acanthotic epidermis (Figure 3A). The diagnosis was confirmed through Congo red staining to identify the presence of amyloid deposits in LA and Masson’s trichrome staining to identify the presence of collagen in ARPC (Figure 4A). Based on the patient’s history, physical examination, and histopathological examination, the working diagnoses of LA of both arms and ARPC of both legs were established. The patient received additional topical treatment, comprising 10% urea cream for the whole body, 0.05% clobetasol ointment with occlusion for skin lesions on both arms, and 0.05% retinoic acid gel for the skin lesions on both legs.
 |
Figure 3 Histopathological examination of the biopsy specimen from the right arm. (A) HE-staining showed hyperkeratosis and acanthosis of the epidermis as well as eosinophilic mass deposit in the dermis (red circles). (B) Congo red staining showed reddish-Orange amyloid deposits in the papillary dermis (yellow circles). |
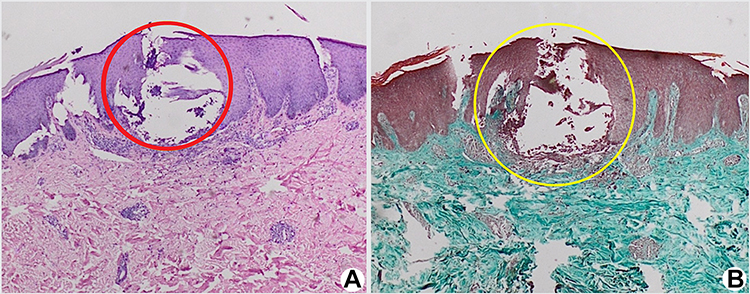 |
Figure 4 Histopathological examination of the biopsy specimen from the left leg. (A) HE-staining of the biopsy specimen from the left leg showed the epidermal surface forming a cup-like shape containing a mass of keratin and collagen (red circle), surrounded by infiltration of lymphocyte inflammatory cells. (B) Masson’s trichrome staining showed elimination of the bluish collagen mass (yellow circle) from the dermis to the epidermis. |
In the second month of observation, the patient felt less pruritus and the skin lesions were thinning, although new skin lesions still developed. Congo red staining of the biopsy specimen from the left arm revealed an orange amyloid deposit (Figure 3B), supporting the diagnosis of LA. Elimination of the bluish-colored collagen mass from the dermal reticular layer to the epidermis (Figure 4B) was identified on Masson’s trichrome staining, supporting the diagnosis of ARPC. Therefore, the treatment was continued.
In the third month of observation, there was a partial improvement of the skin lesions in the form of thinning of the hyperkeratotic papules and plaques on both arms (Figures 1C and D) and hyperkeratotic papules and nodules on both legs (Figures 2D–F). However, new skin lesions still developed, although the pruritus decreased. While undergoing treatment at the Geriatric and Non-Infection Clinic of the Dermatology and Venereology Department, Dr. Hasan Sadikin General Hospital, the patient also visited the Internal Medicine Clinic and had her fasting blood glucose level checked regularly. Increased fasting blood glucose levels were reported every month, which were 126 mg/dL in the first month of observation, 145 mg/dL in the second month, and 167 mg/dL in the third month.
Discussion
Lichen amyloidosis is a form of PLCA.4,14 This skin disorder is more common in men aged 50 to 60 years.9 The exact etiology of LA is not fully understood. Several possible predisposing factors include genetics,15 Epstein–Barr virus infection, and environmental factors. However, the most common triggering factors are trauma,16 friction, or chronic scratching.35 Other skin diseases associated with LA include atopic dermatitis, lichen planus, hepatitis C, and mycosis fungoides.17 Sangen et al7 reported a case of LA in a patient with papillary thyroid carcinoma. The precipitating factor for LA in this case report was chronic scratching with a predisposition of papillary thyroid carcinoma. The patient in this case report was a 55-year-old woman with a history of dry skin who often scratched her skin due to pruritus. The patient had no history of atopic dermatitis, lichen planus, or hepatitis C.
The association between LA and thyroid cancer may be due to pleiotropic genes with or without paracrine stimulation of growth factors.7 Pleiotropy is a state of one genetic locus that can affect several traits.18 RET gene mutations can be found in both LA19 and papillary thyroid carcinoma.20 Lichen amyloidosis is characterized by pruritus, hyperpigmentation, and lichenification.15,21 Skin lesions are initially linear, hyperpigmented, hyperkeratotic papules that can develop into plaques.4 The predilections of LA are the legs (86.4%), arms (63.6%), upper back (45.5%), abdomen (18.9%), and neck (13.6%).21 The skin lesions of the patient in this case report were multiple pruritic hyperkeratotic and scaly papules and plaques on both arms. These features are in accordance with the signs, symptoms, and predilection of LA.
Histopathological examination is required to establish the diagnosis of LA with HE staining and further detection using Congo red staining. Histopathological findings of LA with HE staining showed amorphous eosinophilic amyloid deposits in the papillary dermis, accompanied by hyperkeratosis, pigment incontinence, elongation of the rete-ridges, and perivascular infiltration.5 Venugopal et al5 stated that Congo red staining is the gold standard for confirming the diagnosis of LA with 100% sensitivity. Amyloid appears as reddish-orange features under a light microscope.5 Histopathological examination of the hyperkeratotic papule on the left arm showed eosinophilic amyloid deposits. With Congo red staining, amyloid deposits appear reddish-orange in color.
Acquired reactive perforating collagenosis is a subtype of APD characterized by transepidermal elimination of dermal collagen.12,13 Satti et al23 reported that ARPC occurred four times more frequently in women than in men, with a mean age of onset of 54 years and an age range of 37–72 years. Zhang et al13 described that this disease is often accompanied by various systemic diseases, the most frequent being 92 cases of DM, 60 cases of chronic kidney failure, and 31 cases of hypertension. This disease was also reported in four patients with hypothyroidism.11,13 Yazdi et al12 reported a case of ARPC in a 30-year-old woman with DM and papillary thyroid carcinoma. The patient in this case report was a 55-year-old woman with a history of type 2 DM for 13 years and hypothyroidism for two years after thyroidectomy due to papillary thyroid carcinoma. There was no history of chronic renal failure, hypertension, or other systemic diseases in this patient.
The main pathogenesis of ARPC is transepidermal elimination of abnormal dermal collagen.13 Several pathological hypotheses have been proposed, including superficial microtrauma due to pruritus and repeated scratching, and changes in the epidermis and dermis due to metabolic abnormalities.12,24 Microdeposits, such as uric acid and calcium pyrophosphate, in patients with chronic renal failure, can lead to local inflammation and tissue degradation.24 Microangiopathy due to DM is thought to be another cause of ARPC because elevated blood glucose levels cause an increase in glycosylation of proteins and other compounds that play a role in hyalinization and structural abnormalities of collagen.13
The initial lesion of ARPC appears as a pinpoint papule, generally hyperkeratotic, which develops into a very pruritic crusted lesion with umbilication.22,25 Ulceration may develop in the later stages of ARPC. Regression may occur within a few weeks which leaves hyperpigmented macules.24,25 The trunk and extensor surfaces of the extremities are the main predilections for ARPC, but skin lesions may also occur on the entire body surface. New skin lesions will appear as the Koebner phenomenon due to repeated skin scratching.25 The patient in this case report presented with a complaint of pruritic hyperkeratotic papules with some erosions on the extensor surfaces of both legs. Some lesions were distributed as the Koebner phenomenon. Hyperpigmented macules were also found.
Histopathological examination of ARPC lesions showed fairly specific findings in the early and late lesions. The initial lesion appears to be an accumulation of basophilic collagen in the papillary dermis. Later lesions showed an epidermal invagination shaped like a saucer or dome, containing parakeratotic plugs, degeneration of collagen fibers, and debris.24 In this case report, histopathological findings of the hyperkeratotic papule lesion on the right leg showed a portion of the epidermis forming a cup-like shape into the dermis, containing masses of keratin and collagen. Collagenous connective tissue, lightly dusted with inflammatory cells and lymphocytes was also found in the papillary dermis. These findings were in accordance with the histopathological features of ARPC.
The main principle of LA therapy is to break the itch-scratch cycle by overcoming the pruritus that can induce scratching, thus reducing the amyloid and improving the skin lesions. To date, there have been no standard guidelines for LA management.26 Several options for treatment modalities include topical or intralesional corticosteroids injection, topical calcineurin inhibitors, oral cyclophosphamide, cyclosporine, dermabrasion, topical or systemic retinoids, carbon-dioxide lasers, pulsed-dye laser (PDL), or neodymium-doped yttrium-aluminum garnet (Nd:YAG) laser, and narrowband ultraviolet B (NB-UVB) therapy.4,27 The therapeutic efficacy of these modalities varies from person to person, and most patients do not exhibit good response. The high recurrence rate of LA presents a challenge.16 Topical corticosteroids are the gold standard therapy for various inflammatory skin diseases.28 The therapeutic effects of corticosteroids include anti-inflammatory, immunosuppressive, antiproliferative, and vasoconstrictor properties.29 Very potent topical corticosteroids should be used on thick lesions and in areas other than intertriginous areas.30 In this case report, the hyperkeratotic papules on both arms were given twice daily 0.05% clobetasol propionate ointment, a very potent corticosteroid, with occlusion to increase absorption and reduce the evaporation of the topical drugs. Some of the hyperkeratotic papules and plaques on both arms turned into hyperpigmented macules within one month after the administration of 0.05% clobetasol propionate ointment with occlusion.
To date, there is no standard therapy for ARPC due to its rarity.24 The main principle of ARPC management is to control pruritus and the underlying diseases.13 Ghosh et al31 reported an improvement of ARPC lesions within six weeks after topical administration of 0.05% retinoids and oral antihistamines. Chronic hyperglycemia in DM patients causes structural changes in long-lived proteins, such as collagen, which produces advanced glycation end products (AGEs) and increases the activity of matrix metalloproteinase. Keratinocytes express several types of AGE receptors (RAGE), such as class B scavenger receptor type I (SR-BI), cluster of differentiation 36 (CD36), and galectin-3 (Gal-3). Scratching damages the basement membrane, leading to the interaction between keratinocytes and collagen AGEs through RAGE. Keratinocytes differentiate superficially along with bound collagen.32 Collagen stimulates an immune response following transepidermal elimination. Leukocyte infiltration in ARPC lesions releases interleukin-1 (IL-1) which stimulates metalloproteinase synthesis and subsequently degrades the extracellular matrix components, including collagen fibers.24 Retinoids can improve the protective function of the epidermis, protect collagen from degradation, and inhibit metalloproteinase activity.33 Administration of moisturizers and oral antihistamines can relieve itching in ARPC.13 Improvement of the hyperkeratotic papules and nodules in our patient was shown within one month after the administration of moisturizers, 0.05% retinoic acid gel, and oral antihistamines. However, new skin lesions still developed. The patient’s fasting blood glucose level never lower to normal values. In addition, the ablation therapy for the residual mass of papillary thyroid carcinoma had not been completed.
The amyloid deposits in various internal organs lead to a high mortality rate. In LA, there are no amyloid deposits in internal organs,21 so the quo ad vitam prognosis of our patients was relatively good. Complaints of severe pruritus in LA can cause a decrease in the patient’s quality of life. LA itself is a chronic, refractory, and recurrent disease caused by amyloid deposits in the skin.34
Mortality data regarding APD is very limited. Garrido et al35 reported a 6-month mortality rate of 8.8% in patients diagnosed with APD. Mortality in APD is associated with the underlying systemic disease.35,36 Surgical treatment and ablation of papillary thyroid carcinoma can increase the initial 10-year survival rate to 90% longer.37 Tachkov et al37 reported that the mean survival rate of patients with type 1 DM is 70.96 years compared to 75.19 years in patients with type 2 DM. Li et al38 reported that the death of patients with DM was mainly caused by cardiovascular disease, chronic lower respiratory tract disease, cerebrovascular disease, kidney disease, Alzheimer’s disease, and pneumonia. In this case report, the patient had a history of papillary thyroid carcinoma, had undergone thyroidectomy, and was still undergoing ablation therapy. There was no history of cardiovascular disease, chronic lower respiratory tract disease, cerebrovascular disease, kidney disease, Alzheimer’s, and pneumonia accompanying DM in our patient. Therefore, we determined that the quo ad vitam prognosis of the patient was relatively good. ARPC skin lesions can regress spontaneously, leaving areas of persistent hypopigmentation and atrophic scars.13,24 Akoglu et al36 reported recurrence in 12% of APD cases.
Conclusion
Histopathological examination is required in patients with a history of endocrine diseases, such as type 2 DM and thyroid disorders complaining of skin abnormalities such as papules, nodules, or hyperkeratotic plaques to confirm the diagnosis of skin diseases, such as ARPC or LA. Treatment of those kind of dermatoses that are related to endocrine diseases should not only rely on dermatological treatment but also appropriate treatment regarding the underlying endocrine diseases. Thus, multidisciplinary care might be required. The patients should be explained that the skin disorder highly associated with the underlying systemic disease to increase their obedience for the treatment.
Ethics Statement
The publications of images were included in the patient’s consent for publication of the case. Institutional approval has been obtained to publish the case details.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of the case details and images.
Acknowledgments
The authors would like to thank the staff of the Dermatology and Venereology Department, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dabrowska AK, Spano F, Derler S, Adlhart C, Spencer ND, Rossi RM. The relationship between skin function, barrier properties, and body-dependent factors. Skin Res Tech. 2017;24(2):165–174. doi:10.1111/srt.12424
2. Jin R, Luo L, Zheng J. The trinity of the skin: skin homeostasis as a neuro-endocrine-immune organ. Life. 2022;12(725):1–11. doi:10.3390/life12050725
3. Dermikesen C. Skin manifestations of endocrine diseases. Turk Patoloji Derg. 2015;31:145–154.
4. Gorevic PD, Phelps RG. Amyloidosis. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, editors. Fitzpatrick’s Dermatology.
5. Venugopal SB, Muralidhar A. Primary localized cutaneous amyloidosis—a clinicopathological study. Arch Med Health Sci. 2019;7:38–41. doi:10.4103/amhs.amhs_122_18
6. Mansoor M, Kapadia N, Talat H, et al. Lichen amyloidosis. Professional Med J. 2017;24(07):1020–1026.
7. Sangen Y, Kawada A, Maeda A, Aragane Y, Tezuka T. Primary localized cutaneous amyloidosis in association with papillary thyroid carcinoma. J Cutan Med Surg. 2002;6(4):332–334. doi:10.1177/120347540200600404
8. Karadag AS, Ozlu E, Lavery MJ. Cutaneous manifestations of diabetes mellitus and the metabolic syndrome. Clin Dermatol. 2018;36:89–93. doi:10.1016/j.clindermatol.2017.09.015
9. Sabban ECS. Dermatoses most frequently related to diabetes mellitus. In: Sabban ENC, Miguel F, Kenneth C, editors. Dermatology and Diabetes. New York: Springer; 2018:p145–77.
10. Nair PA, Jivani NB, Diwan NG. Kyrle’s disease in a patient of diabetes mellitus and chronic renal failure on dialysis. J Family Med Prim Care. 2015;4(2):284–286. doi:10.4103/2249-4863.154678
11. Kim SW, Kim MS, Lee JH, et al. A clinicopathologic study of thirty cases of acquired perforating dermatosis. Ann Dermatol. 2014;26(2):162–171. doi:10.5021/ad.2014.26.2.162
12. Yazdi S, Saadat P, Young S, Hamidi R, Vadmal S. Acquired reactive perforating collagenosis associated with papillary thyroid carcinoma: a paraneoplastic phenomenon? Clin Exp Dermatol. 2010;35:152–155. doi:10.1111/j.1365-2230.2009.03211.x
13. Zhang X, Yang Y, Shao S. Acquired reactive perforating collagenosis. Medicine. 2020;99(22):1–7.
14. Krishna A, Nath B, Dhir GG, Kumari R, Budhiraja V, Singh K. Study on epidemiology of cutaneous amyloidosis in northern India and effectiveness of dimethylsulphoxide in cutaneous amyloidosis. Indian Dermatol Online J. 2012;3(3):182. doi:10.4103/2229-5178.101814
15. Salim T, Shenol SD, Balachandran C, Mehta VR. Lichen amyloidosis: a study of clinical, histopathologic and immunofluorescence findings in 30 cases. Indian J Dermatol Venereol Leprol. 2005;71(3):166–169. doi:10.4103/0378-6323.16230
16. Loffreda MD, Kim Y, Chung CG. Lichen amyloidosis of the scalp and forehead. Dermatol Online J. 2017;23(11):1–3.
17. Matsumura N, Yamamoto T. Lichen amyloidosis associated with chronic renal failure. Our Dermatol Online. 2017;8(2):237–238. doi:10.7241/ourd.20172.67
18. Hackinger S, Zeggini E. Statistical methods to detect pleiotropy in human complex traits. Open Biol. 2017;29(9):1–13.
19. Malhotra R, Boro H, Shamim SA, Khadgwat R. Multiple endocrine neoplasia type 2A with cutaneous lichen amyloidosis. BMJ Case Rep. 2020;13:1–2. doi:10.1136/bcr-2020-238423
20. Staubitz JI, Schad A, Springer E, et al. Novel rearrangements involving the RET gene in papillary thyroid carcinoma. Cancer Genet. 2019;230:13–20. doi:10.1016/j.cancergen.2018.11.002
21. Wu FF, Rong ZL, Fang C, et al. Clinical and genetic features of Chinese patients with lichen and macular primary localized cutaneous amyloidosis. Clin Exp Dermatol. 2019;44(4):110–117. doi:10.1111/ced.13925
22. Reich D, Psomadakis CE, Buka B. Lichen simplex chronicus. In: Top 50 Dermatology Case Studies for Primary Care. New York: Springer; 2017:p221–6.
23. Satti MB, Aref AH, Raddadi AA, Al-Ghamdi FA. Acquired reactive perforating collagenosis: a clinicopathologic study of 15 cases from Saudi Arabia. J Eur Acad Dermatol Venereol. 2010;24:223–227. doi:10.1111/j.1468-3083.2009.03333.x
24. Lo YP, Snehal D, Deng LH, Chang CH, Shih CJ. Successful treatment of acquired perforating collagenosis induced by pregnancy with allopurinol: a case report with review of literature. Dermatol Sin. 2019;37:162–165. doi:10.4103/ds.ds_47_18
25. Reid J, Almond L, Matthewman N, et al. A case of acquired reactive perforating collagenosis. Australas J Dermatol. 2018;59:75–76. doi:10.1111/ajd.12618
26. Koh WS, Oh EH, Kim JE, Ro YS. Alitretinoin treatment of lichen amyloidosis. Dermatol Ther. 2017;8(2):237.
27. Humeda Korbi M, Akkari H, Soua Y, et al. Lichen amyloidosis successfully treated with fractional ablative laser CO2: a new alternative therapeutic. J Cosmet Laser Ther. 2019;21(1):1–3. doi:10.1080/14764172.2017.1406605
28. Humeda Y, Beasley J, Calder K. Clinical resolution of generalized lichen amyloidosis with dupilumab: a new alternative therapy. Dermatol Onl J. 2020;26(12):1–5.
29. Kwatra G, Mukhopadhyay S. Topical corticosteroids: pharmacology. In: Lahiri K, editor. A Treatise on Topical Corticosteroids in Dermatology. New York: Springer; 2018:p11–22.
30. Uva L, Miguel D, Pinheiro C, et al. Mechanism of action of topical corticosteroids in psoriasis. Int J Endocrinol. 2012;1–6. doi:10.1155/2012/561018
31. Ghosh SK, Bandyopadhyay D, Chatterjee G. Acquired reactive perforating collagenosis following insect bite. Indian J Dermatol Venereol Leprol. 2009;75(3):306–307. doi:10.4103/0378-6323.51269
32. Fujimoto E, Kobayashi T, Fujimoto N, Akiyama M, Tajima S, Nagai R. AGE-modified collagens I and III induce keratinocyte terminal differentiation through AGE receptor CD36: epidermal–dermal interaction in acquired perforating dermatosis. J Invest Dermatol. 2010;130:405–414. doi:10.1038/jid.2009.269
33. Zasada M, Budzisz E. Retinoids: active molecules influencing skin structure formation in cosmetic and dermatological treatments. Adv Dermatol Allergol. 2019;36(4):392–397. doi:10.5114/ada.2019.87443
34. Wang M, Lin Y, Wu W, et al. Treatment of lichen amyloidosis with fractional CO2 laser and topical steroid: a preliminary study of 10 cases. Lasers Med Sci. 2020;11(3):1–5.
35. Garrido PM, Queiros C, Costa JB, Almeida LS, Filipe P. Acquired perforating dermatosis: clinicopathologic study of a 10-year period at tertiary teaching hospital. Int J Dermatol. 2019;59(4):1–6.
36. Akoglu G, Emre S, Sungu N, Kurtoglu G, Metin A. Clinicopathological features of 25 patients with acquired perforating dermatosis. Eur J Dermatol. 2013;23(6):864–871. doi:10.1684/ejd.2013.2237
37. Tachkov K, Mitov K, Koleva Y, et al. Life expectancy and survival analysis of patients with diabetes compared to the non diabetic population in Bulgaria. PLoS One. 2020;15(5):1–16. doi:10.1371/journal.pone.0232815
38. Li S, Wang J, Zhang B, Li X, Liu Y. Diabetes mellitus and cause-specific mortality: a population based study. Diabetes Metab J. 2019;43:319–341. doi:10.4093/dmj.2018.0060
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.