Back to Journals » International Medical Case Reports Journal » Volume 13
Coarctation of Aorta and Post-Stenotic Dissecting Aortic Aneurysm Successfully Treated with Endovascular Stent
Authors Jata B, Jahollari A, Kojqiqi A ![]() , Huti G
, Huti G
Received 14 June 2020
Accepted for publication 8 August 2020
Published 25 August 2020 Volume 2020:13 Pages 367—370
DOI https://doi.org/10.2147/IMCRJ.S267692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Video abstract presented by Artan Jahollari.
Views: 1142
Bekim Jata,1 Artan Jahollari,2 Arben Kojqiqi,3 Gentian Huti4
1Department of Invasive Cardiology, American Hospital 3, Tirana, Albania; 2Department of Cardio-Vascular Surgery, American Hospital 3, Tirana, Albania; 3Department of Cardio-Thoracic Surgery, American Hospital 3, Tirana, Albania; 4Department of Anesthesia and Reanimation, American Hospital 3, Tirana, Albania
Correspondence: Artan Jahollari Tel +355 698515745
Email [email protected]
Abstract: Coarctation associated with a dissected aneurysm is uncommon and has an incidence of less than 1%. There are few reports describing treatment of this condition with stent graft. Challenging as it may be, endovascular treatment of complex cases has become the preferred modality especially when the anatomy is amenable. We describe the case of a 36-year old male, who suffered a car accident and was diagnosed with acute type B aortic dissection (ATBAD). CT-scan revealed a coarctation associated with a large dissected aneurysm (11cm). Complexity of pathology and high risk of rupture required immediate intervention. Open repair necessitates extensive surgery with a considerable risk of morbidity and mortality. We decided to perform an endovascular repair and subsequentially the patient was successfully treated with stent graft deployment, showing durable early-midterm results. Patient remains asymptomatic to this day and CT-scan at 3-year follow-up revealed a reduced and thrombosed aneurysm.
Keywords: aortic coarctation, aneurysm, endovascular repair
Introduction
Aortic coarctation has an incidence of circa 5% among congenital cardiac anomalies.1 Frequently it is associated with aneurisms, which can be of proximal (32%) or distal location (51%). Surgery has been the main correction option since 1950ʹies. Even after surgical correction, aneurysms can occur at proximal or distal anastomotic sites.2 Endovascular procedures have opened a new dimension in treatment of thoracic aorta pathologies and are an excellent solution particularly in complex cases with high morbidity and mortality risk.3
We describe a case of coarctation complicated with a dissected aneurysm which was diagnosed incidentally after a car accident. It was considered as ATBAD and was treated successfully with emergent Thoracic Endovascular Aneurism Repair (TEVAR).
Case Report
A 36-year old male patient, without any previous diagnose, presented to the emergency room after a car accident. He was in stable hemodynamic condition and without any apparent fracture. Blood pressure was 160/100 mmHg and bilateral femoral pulses were weak. CT-scan incidentally revealed an aortic coarctation 12 mm distal to the left subclavian artery narrowing more than 70% of lumen. It showed high tortuosity and kinking at the ductal level (Figure 1). Distal to coarctation, a dissected aortic aneurysm reaching 11 cm of diameter and 10 cm of length was noticed. Acute dissection was suspected because patient described onset of a new back pain. Well developed collaterals were present and echocardiography revealed trans-coarctation gradients of mean/max 28/60 mmHg. Due to his continuous back pain and high risk of rupture emergent TEVAR under general anesthesia was planned. Right radial artery was cannulated with a 6F sheath and pigtail was advanced in ascending aorta. Initial angiogram was performed showing a detailed anatomy. Right femoral artery was cannulated under direct vision with groin incision. Retrograde advancement of guide wire was unsuccessful so we introduced a snare kit (Amplatz Goose Neck, Minnesota/USA) through right radial artery which passed antegradely through the narrowed segment, and then pulled a 0.038ʹʹ Shinobi guide wire (Cordis, USA) from diaphragmatic level. Next it was replaced with a stiff wire, narrowed segment was cautiously predilatated with 16x40 mm Zelos PTA balloon (Optimed, Ettlingen, Germany) and a 30x30x200 mm Relay Plus thoracic stent (Bolton Medical, Florida, USA) was advanced through aneurysm and coarctation. Blood pressure was reduced (80–40mmHg) using vasodilators and the stent graft was deployed partially covering left subclavian artery orifice without obstructing it. Proximal landing site had a safe zone of 10–12 mm from subclavian artery and aorta was oversized by 10–15%. Distally it was landed at healthy thoracic aorta. The aneurysm was excluded completely and no endo-leak was noticed. Post-dilatation was not needed. We did not use any spinal cord protection and the patient was extubated on the operation table, without any motor or sensory deficit of lower extremities. Patient had an uneventful course and was discharged 1 week later. He is normotensive and is using only bisoprolol 2.5 mg daily. He remains asymptomatic to this day and the last CT-scan at 3-year follow-up revealed a totally thrombosed aneurysm which has shrunk by 2 cm in diameter (Figure 2).
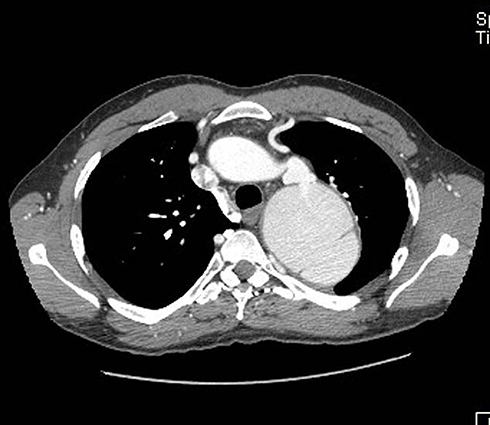 |
Figure 1 Axial view of preoperative CT-scan. Note the coarctation/kinked segment and dissected aneurysm. |
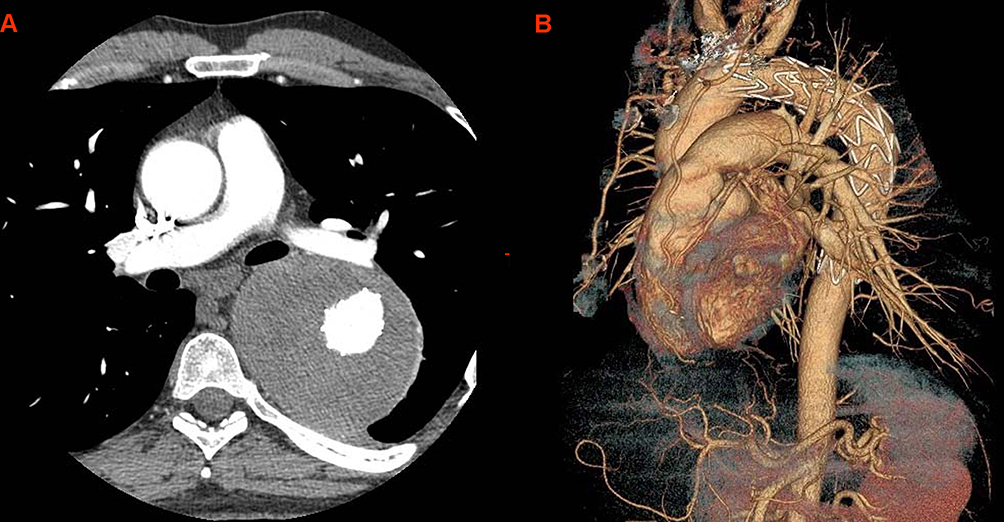 |
Figure 2 Postoperative CT-scan at 3-year follow-up. (A) axial view showing lumen and thrombosed aneurysm sac, (B) 3-dimensional aorta. |
Discussion
Coarctation of aorta is a congenital anomaly frequently associated with aneurysms due to impaired flow and abnormal aortic wall. As endovascular procedures developed, ballooning and stenting of narrowed segment emerged as treatment of choice.4 Concurrently, during the last 15 years TEVAR turned into the preferred modality of physicians dealing with thoracic aorta aneurysms and ATBAD.5
Though, facing a coarctation associated with dissected aneurysm can be demanding due to complexity of anatomy. Keeping in mind the fragility of wall, surgery can be extensive and with a considerable risk of complication. On the other hand, endovascular treatment requires meticulous planning and execution to avoid rupture, and must achieve a durable result. In literature, there are few reports of TEVAR for coarctation associated with dissected aneurysm.6,7
Nowadays TEVAR is considered a first line therapeutic option in patients with complicated ATBAD and impending aortic rupture.8 Considering our institutional experience and the patient preference we decided for TEVAR. In our case the aneurysm was post-stenotic. Whether the dissection was chronic because of coarctation or acute because of accident is debatable. However, it was considered as ATBAD and emergent as he carried high risk of rupture. Passing through the coarctation can be challenging and may require various anatomical approaches. In this case, narrowed segment showed a high degree of kinking and tortuosity and guide wire was pulled with snare introduced from the arm.
Another key point of the procedure was ballooning of coarctated segment. It is a controversial maneuver that has attendant risk. However, usage of covered stents leads to better results and provides additional safety, and nowadays even in straightforward simple coarctations physicians are driven toward covered stent deployment.9 Furthermore, sometimes predilatation with small-medium size balloons is mandatory to create a passage to assure stent graft advancement.10 Giving the tortuosity of coarctation we decided to balloon the lesion prior to advance stent graft.
Hybrid approaches have been performed successfully for treatment of complex coarctation with additional heart anomalies.11 Our patient did not have any other congenital defect and sole endovascular repair was sufficient. Anyhow, he is under close follow-up consisting in biannual transthoracic echocardiogram and annual CT-scan.
The outcome of endovascular repair for this uncommon case is encouraging. With proper planning and meticulous manipulation, TEVAR may be performed safely in similar patients. Follow-up with periodical imaging modalities will be necessary to determine changes of thoracic aorta in the long term.
Ethics and Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images. All procedures of this study were in accordance with the ethical standards of the institution American Hospital, Albania. Regarding the policies of the institution, institutional approval was not required to publish this case report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Allen BD, Barker AJ, Gabbour M, et al. Aortic coarctation augments changes in thoracic aortic hemodynamics in pediatric and young adult patients with bicuspid aortic valve. J Cardiovasc Magn Reson. 2013;15:P300.
2. Knyshov GV, Sitar LL, Glagola MD, Atamanyuk MY. Aortic aneurysms at the site of the repair of coarctation of the aorta: a review of 48 patients. Ann Thorac Surg. 1996;61:
3. Bai J, Liu Y, Jin J, Li J, Ji X, Qu L. Single-stage endovascular management of complicated thoracic aorta coarctation concurrent with aortic arch aneurysm using a novel fenestration device. J Thorac Dis. 2018;10(4):2474–2480. doi:10.21037/jtd.2018.03.162
4. Kische S, Schneider H, Akin I, et al. Technique of interventional repair in adult aortic coarctation. J Vasc Surg. 2010;51(6):1550–1559. doi:10.1016/j.jvs.2009.12.063
5. Mitsis A, Nienaber C. Endovascular treatment of aortic diseases 1171–1185. In: Stanger O, Pepper J, Svensson L, editors. Surgical Management of Aortic Pathology. Vienna: Springer; 2019.
6. Reddy B, Natraj Setty HS, Srinivas BC, et al. Thoracic endovascular aneurysm repair for coarctation of the aorta with dissecting aortic aneurysm: A rarity. J Nat Sci Biol Med. 2018;9:291–293. doi:10.4103/jnsbm.JNSBM_152_17
7. Di Tommaso L, Mannacio VA, Di Tommaso E, Pinna GB, Fontana I, Iannelli G. Endovascular Treatment of Distal Aortic Arch Aneurysm Associated with Coarctation of Aorta in a Jehovah’s Witness. Tex Heart Inst J. 2017;44(6):399–401. doi:10.14503/THIJ-16-6093
8. Riambau V, Böckler D, Brunkwall J. Editor’s choice - management of descending thoracic Aorta diseases: clinical practice guidelines of the European Society for Vascular Surgery (ESVS) Eur. J Vasc Endovasc Surg. 2017;53:4–52. doi:10.1016/j.ejvs.2016.06.005
9. Pedra C, Peirone A, Costa R, Bruckheimer E. Covered-stent implantation in coarctation of the aorta: indications, materials, techniques and outcomes. Interv Cardiol. 2011;3:67–77. doi:10.2217/ica.10.96
10. Pilla CB, Fontes VF, Pedra CA. Stenting for aortic coarctation. Expert Rev Cardiovasc Ther. 2005;3:879–890. doi:10.1586/14779072.3.5.879
11. Russell TA, Quarto C, Nienaber CA. A single-stage hybrid approach for the management of severely stenotic bicuspid aortic valve, ascending aortic aneurysm, and coarctation of the aorta with a literature review. J Cardiol Cases. 2018;17(6):183–186. doi:10.1016/j.jccase.2018.01.009
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.