Back to Journals » Open Access Journal of Contraception » Volume 16
Coagulation Profiles Among Combined Oral Contraceptive User and Non-User Women Attending at Family Guidance Association of Ethiopia, Jigjiga Medium Clinic: A Comparative Cross-Sectional Study
Authors Getu F ![]() , Tesfaye A
, Tesfaye A ![]() , Mekuria S
, Mekuria S ![]() , Ayehubizu LM
, Ayehubizu LM ![]() , Tahir B, Roble AK
, Tahir B, Roble AK ![]() , Getu E, Walle M
, Getu E, Walle M ![]()
Received 3 June 2025
Accepted for publication 28 August 2025
Published 4 September 2025 Volume 2025:16 Pages 97—110
DOI https://doi.org/10.2147/OAJC.S544527
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Fasil Getu,1 Addisu Tesfaye,1 Surafel Mekuria,1 Liyew Mekonen Ayehubizu,2 Bawlah Tahir,1 Abdurahman Kedir Roble,3 Eyob Getu,4 Muluken Walle5
1Department of Medical Laboratory Science, Institute of Health Science, Jigjiga University, Jigjiga, Ethiopia; 2Department of Public Health, Institute of Health Science, Jigjiga University, Jigjiga, Ethiopia; 3Department of Midwifery, Institute of Health Science, Jigjiga University, Jigjiga, Ethiopia; 4Department of Medical Laboratory Science, College of Medicine and Health Science, Dilla University, Dilla, Ethiopia; 5Department of Hematology and Immunohematology, School of Biomedical and Laboratory Science, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Fasil Getu, Department of Medical Laboratory Science, Institute of Health Science, Jigjiga University, Jigjiga, P.O.Box 1020, Ethiopia, Tel +251927436332, Email [email protected]
Introduction: Combined Oral Contraceptives are associated with enhanced procoagulant effects, decreased anticoagulant effects, and equivocal effects on fibrinolysis. The main aim of this study was to compare the mean value of platelet count, PT, and APTT among COC users and non-users and to determine factors associated with coagulopathy among COC users attending Family Guidance Association (FGAE), Jigjiga Medium clinic, Eastern Ethiopia.
Methods: A comparative cross-sectional study was conducted at the FGAE, Jigjiga Medium clinic. A total of 393 women were enrolled using a systematic random sampling method. Socio-demographic and clinical data were obtained via face-to-face interviews and extracted from the medical chart, respectively. To determine PT, APTT, and platelet count, 6.7 milliliters of venous blood was collected. The data were entered into Epi Info version 7.2.4.0 and then transferred to SPSS version 20 for analysis. The Shapiro–Wilk test was used to examine the distribution of the data. Data comparisons between the two groups were conducted using an independent t-test and the Mann–Whitney U-test. To determine factors associated with coagulopathy among COC users, Bivariable and multivariable logistic regression analyses were employed. P-values below 0.05 were regarded as statistically significant.
Results: A sum of 393 subjects (131 COC users and 262 age-matched non-COC-user women) were enrolled in this study. The mean age was 27.67± 4.14 (28.12± 4.49 years old for COC users and 27.45± 3.94 years old for non-COC users. The mean difference indicated that PT and APTT were lower by − 1.14 (− 1.36,-0.92) and − 2.48 (− 3.04, − 1.91), respectively, in COC user women compared to non-COC users. However, platelet count was significantly elevated in the COC users group (P-value < 0.001). The mean ±SD values were 259.5± 79.00 and 191.1± 27.98 in COC users and non-COC users, respectively. The overall prevalence of coagulopathy was 38.9% (51/131): from this abnormality, 40.5% (53/131) of the COC users showed shortened PT, and 27.5% (36/131) showed shortened APTT. Long-term use of COC (> 5 years) was significantly associated with Coagulopathy (AOR = 0.035; 95% CI: 0.004– 0.343).
Conclusion: This study showed that COC users exhibited a greater tendency toward hypercoagulability, placing these women at an increased risk of thromboembolic effects compared to COC non-users. There is a high prevalence of coagulopathy among COC users, and long-term usage of COC can lead to hypercoagulation and thrombotic abnormalities.
Keywords: combined oral contraceptive, coagulopathy, Jigjiga, Ethiopia
Background
Contraception refers to methods used to avoid pregnancy. This can include devices, drugs, surgical procedures, or specific behaviors.1 Oral contraceptives (OCs) represent a significant category of prescribed medications, utilized by a considerable number of women beginning in their early teenage years.2 In 1960, the initial Combined Oral Contraceptive (COC) was introduced. Since that time, the utilization of the pill has expanded significantly, surpassing other reversible contraceptive methods and providing fast, safe, and dependable pregnancy prevention.3 At present, there are three distinct types of oral contraceptive pills: extended-use or continuous pills, progesterone-only pills, and combined estrogen-progesterone pills.4
The primary hormone that helps to prevent pregnancy is progesterone. Its main mechanism of action is to inhibit ovulation; it reduces follicular development and stops the release of an ova.5 The hypothalamus employs progesterone-negative feedback to decrease the pulse frequency of gonadotropin-releasing hormone. This subsequently restricts the release of Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH).6 The mid-cycle LH surge is prevented by the progestogen-negative feedback and the absence of estrogen-positive feedback. Ovulation is inhibited because no follicle has formed, and no LH surge has occurred to release the follicle. By altering the cervical mucus to create an unfavorable environment, progesterone employs an additional key mechanism that hinders sperm from accessing the cervix and upper vaginal canal.7
Between 2015 and 2017, 64.9% of the 72.2 million women of reproductive age in the United States were utilizing contraception. The predominant methods of contraception included female sterilization (18.6%), oral contraceptive pills (12.6%), long-acting reversible contraceptives (10.3%), and male condoms (8.7%).8 The 2019 Ethiopian Mini Demographic and Health survey indicated that 28.1% of women utilized modern contraceptives, with 18.7% opting for injectables, 6% for implants, 1.4% for pills, 1% for Intra Uterine Devices, 0.4% for the Lactation Amenorrhea Method, 0.3% for female sterilization, 0.2% for male condoms, and 0.1% for the Standard Days Method.9
It is well established that the COCs raise the risk of thromboembolism by disrupting coagulation homeostasis and causing a procoagulant condition.10 The disruption of hemostasis occurs due to elevated levels of procoagulant factors like factors VII, VIII, and II, alongside a reduction in anticoagulant factors such as antithrombin and protein S.11 Another factor contributing to the thrombotic risk associated with oral contraceptives is the decreased responsiveness of plasma to Activated Protein C (APC). Protein C serves as a precursor in the anticoagulant pathway, which is triggered by the formation of the Thrombin-Thrombomodulin (TM) complex on the surface of endothelial cells. Once activated and in conjunction with its cofactor protein S, APC works to inhibit procoagulant factors Va, VII, VIIIa, and X, thereby reducing Thrombin Generation.12 Platelet activity is also increased due to enhanced aggregation, resulting in a state of hypercoagulability.13
Coagulopathy is a significant public health issue that leads to morbidity and mortality on a global scale.14 Across the globe, 26 to 45% of individuals classified as healthy reported experiencing nose and gum bleeding. This concern also impacts around 5 to 10% of women of reproductive age who pursue treatment for heavy or prolonged menstrual bleeding.15 Hormonal contraceptives are often associated with side effects, mainly nausea, headache, breast tenderness, weight gain, irregular bleeding, and mood changes.16 Oral contraceptive pills are the most commonly utilized hormonal methods of birth control and are often associated with elevated blood pressure, blood clots, heart attacks, and strokes.17 A study carried out in Saudi Arabia found that the use of oral contraceptives in the population mainly affected thrombus formation and the sensitivity to activated protein C in individuals who are overweight and obese.18 Another study carried out in the United States found that there were significant differences in age, race, alcohol use, sleep patterns, and family history of cardiovascular disease and stroke between users of COC and the control group.19
Prothrombin Time (PT), Activated Partial Thromboplastin Time (PTT), and platelet counts are among the laboratory tests utilized for identifying coagulopathy and monitoring anticoagulant therapies. PT serves as a screening examination to evaluate disorders associated with the extrinsic and common coagulation pathways (Factors I, II, V, VII, and X). APTT is employed to assess the intrinsic and common clotting pathways within the coagulation system (Factors I, II, V, VIII, IX, XI, and XII).20,21
This study was the first study that illustrate Coagulopathy among COC users and non-users in Ethiopia, particularly in the study area, Jigjiga. Prior to this research, there were notable inadequate studies that directly compared the coagulation status of COC users with non-users. Therefore, this study primarily aimed to evaluate the mean value of PT, APTT, and platelets in COC users and non-users. By analyzing these parameters, the study aimed to provide a clearer understanding of how COC usage may impact coagulation profiles. It also determined the factors associated with coagulopathy among COC users.
Methods and Materials
Study Area and Period
The study was carried out from May 1 to July 30, 2024, at FGAE: Jigjiga Modicum Clinic, which is found in the Fafan zone of the Somali Regional State, Ethiopia. Jigjiga town is located 637 km distant from the capital city of Ethiopia, Addis Ababa, in the East direction. The town has an elevation of 1934 meters above sea level and its temperature is about 21.1 °C and has “Kolla” climatic conditions. Based on the 2007 Census by the Statistical Agency of Ethiopia (CSA), Jigjiga town has a total population of 203,588, of whom 109,138 are males and 94,450 are females.22 The town has 20 kebeles and a total area of 39.37 square kilometers. Regarding health facilities, the town has one public Referral Hospital and one General Hospital, 3 health centers, 20 health posts, and 1 Family Guidance office. There is one private general hospital, 27 higher clinics, and 10 medium clinics.23
Study Design
A facility-based comparative cross-sectional study was conducted.
Population
Source population
All COC-using reproductive-age women attending the FGAE, Jigjiga Medium Clinic were taken as a source population for the case group, whereas COC non-users reproductive-age women who are attending the FGAE, Jigjiga Medium Clinic were taken as a source population for the control group.
Study Population
All reproductive-age women who were taking 35 mg of ethinyl estradiol and 0.25 mg of norgestimate COC attending the FGAE, Jigjiga Medium Clinic during the study period were taken as a study population for the case group. Age-matched reproductive-age women who were not taking COC were taken as a study group for the control group.
Sample Size Calculation and Sampling Technique
Sample Size Calculation
First Objective
The sample size was determined using a double population mean formula by taking the mean of PT in cases (14.0±1.4) and controls (13.4±1.3) from a prior study conducted in Sudan.24 95% CI (0.05 margin of error) and 95% power (β =0.05) at a 1:2 allocation ratio of a case-to-control were used in the computation.

n1 and n2 are sample sizes for group one and group two
 =1.96 at 95% CI and
=1.96 at 95% CI and  =1.64 at power 95%
=1.64 at power 95%
µ1 and µ2 are the means of the two respective groups
 Are the variances of the two respective groups
Are the variances of the two respective groups
So, from the above study µ1=14.0, µ2=13.4, δ1 =1.4 and δ2=1.3

Then by substituting the above values in the formula;
Second Objective
A population proportion formula was used to calculate the required sample size for the second objective by considering Obesity25 as the major determinant factor of Coagulopathy.
 |
|
Finally, by selecting the largest sample size from the two objectives, the initial sample size was 131 for cases and 262 for controls. A total of 393 participants (131 COC users and 262 COC-non-users women who were age-matched) were enrolled in this study.
Sampling Technique
A systematic random sampling technique was employed to select study participants. For the case group, on average, 15 reproductive-age women visit the FGAE Jigjiga Medium Clinic each day to get COC. Over the three-month data collection period, it was anticipated that 792 reproductive-age women would visit the Family Guidance office for COC acquisition. The sampling interval (K) was calculated by dividing the total expected visits (792) by the desired sample size of 131, yielding a K value of 6. A lottery method was then used to randomly select the first participant from the initial six, and subsequent participants were chosen systematically at intervals of six. Therefore, the study included every sixth woman attending the FGAE Jigjiga Medium Clinic.
Eligibility Criteria
Inclusion Criteria
All reproductive-age women who used the COC preparation consisting of 35 mg of ethinyl estradiol and 0.25 mg of norgestimate and volunteered to participate in the study were included. Age-matched non-COC user women were included as controls.
Exclusion Criteria
Reproductive-age women who were taking Blood thinners within 5–10 days before sample collection,26 a history of massive blood transfusion, women who were diagnosed with a known inherited coagulation disorder, and women who were taking estrogen or progesterone-only pills or any other method of contraception were excluded from this study.
Variables
Dependent Variables
- Mean±SD of PT, APTT, and platelet count
- Coagulopathy
Independent Variables
Socio-demographic Variables (Age, Marital status, Educational status, Occupation, Place of residency) were studied. Moreover, Clinical and behavioral variables (Blood pressure, Physical exercise habit, Body Mass Index, Habitual cigarette smoking, habitual alcohol consumption, duration of Combined Oral Contraceptives, family history of cardiovascular disease) were studied.
Operational Definition
- Regular physical exercise is scheduled. Organized and planned physical activity that has an ultimate purpose.27
- Regular smoker: A person who, in his or her lifetime, has smoked at least 100 cigarettes, and who now smokes every day.28
- BMI: Underweight= < 18.5
Normal= 18.5–24.9
Overweight= 25–29.929
Data Collection Procedure
Socio-Demographic Characteristics and Behavioral Data Collection
After obtaining informed written consent and assent, a semi-structured and pretested questionnaire was used to collect socio-demographic and behavioural data from legible women. The questionnaire was used to make face to face interviews with the participants. Some of the socio-demographic data that were collected include age, sex, occupation, residence, level of education, and others. Behavioural data, such as the habit of regular physical exercise and cigarette smoking, were collected using questionnaires and face-to-face interviews by trained data collectors.
Clinical Data Collection
Clinical data were collected by trained nurses from the medical charts using data collection sheets.
Anthropometric Measurements
The contestants’ heights were measured using a stadiometer. Participants were instructed to stand upright on the stadiometer’s floorboard with their backs against the vertical backboard. Their heels were positioned together, making contact with both the base of the vertical board and each other. The feet were placed at a 60-degree angle and slightly turned outward. Before the height measurement, participants removed their shoes and head coverings. Height was recorded to the nearest 0.1 cm without shoes or hats.30
A scale was utilized to assess the weight of each participant. Before starting the weight measurement, the scale was calibrated to zero. Participants were asked to remove any extra clothing, shoes, jewelry, and objects from their pockets before standing with their weight evenly balanced on both feet, arms at their sides, palms turned inward, and their heads upright and facing forward. Final weight readings were recorded to the nearest 0.1 kg (100 grams). The BMI was calculated by dividing the weight in kilograms (kg) by the height in meters squared (m²).30
Blood Pressure Measurement
The systolic and diastolic blood pressure of the participants was assessed with an automatic digital sphygmomanometer. Participants were instructed to take off any additional clothing, sit up straight, and rest their upper arms on the bench. Subsequently, the systolic and diastolic blood pressure were taken and recorded.
Blood Sample Collection
The vacutainer technique was employed to obtain a total volume of 6.7 milliliters of venous blood. The blood was distributed into two tubes: one tube contained tri-potassium Ethylene Diamine Tetra acetic Acid (EDTA), while the other had 0.3 milliliters of 3.2% sodium citrate. For the complete blood count (CBC) test, the blood with EDTA anticoagulant was utilized, and for the prothrombin time (PT) and activated partial thromboplastin time (APTT) tests, the blood with sodium citrate anticoagulant was used. Standard operating procedures (SOPs) were meticulously adhered to while collecting the blood sample in an aseptic manner.
Laboratory Processing
Platelet Poor Plasma Preparation
A platelet-poor plasma was prepared from all study participants. Blood that had been anticoagulated with sodium citrate was used to make the platelet-poor plasma. A 15-minute centrifugation at 1500g was performed on the sodium citrate anticoagulated whole blood sample.31
Platelet Count
The platelet count was measured using a SYSMEX K-21 automated hematological analyzer. Following the mixing of an EDTA-anticoagulated blood sample, whole blood was drawn for complete blood count analysis. The enumeration of platelets relies on the electrical impedance principle. As cells flow through the aperture, there is a change in electrical resistance that produces a voltage pulse. The frequency of these pulses corresponds directly to the count of cells, while the height of each pulse is proportionate to cell volume.32
PT and APTT Test
The coagulation profile examination was performed utilizing a HUMACLOT DUEPLUS coagulation analyzer that operates on the turbidity meter principle. The PT principle involves the stimulation of the coagulation system in plasma with the presence of tissue factors (Apo protein and phospholipid) along with CaCl2. This process results in the development of a stable clot. The duration from activation to the establishment of a stable clot was measured in seconds.33 The APTT test is based on activating the coagulation system in a plasma sample using a platelet substitute (silica), which acts as a factor XII activator, along with CaCl2. This process results in the creation of a stable clot. The duration from activation to when a stable clot is formed is measured in seconds, which is what the APTT represents. The term “partial” is used because the tissue factor is not included in this reaction mixture.34
Data Quality Control Measures
Socio-Demographic and Clinical Data Quality Control Measures
The questionnaire was prepared in English and translated into Amharic and Afe-Somali, then converted back to English to check for uniformity. The pre-test of the structured questionnaire was conducted by taking 5% of it at Karamara Hospital. All study participants were informed about the purpose and significance of the study before data collection to make them fully aware of their responses. The collected data was checked daily for consistency and accuracy. Data collection was carefully supervised by the principal investigator.
Laboratory Data Quality Control Measures
The sample’s quality was maintained by examining if it met accepted parameters such as the absence of hemolysis and clotting, adequate volume, and proper collection time. After the blood was withdrawn, it was dispensed to the wall of the test tube to avoid hemolysis. Daily temperature monitoring was performed for the refrigerators that hold the sample and the reagents. All reagents were checked for expiry dates and prepared in compliance with the manufacturer’s guidelines. The three levels of commercial HUMACLOT DUEPLUS controls (Low, Normal, and High) were run daily. Machine maintenance was performed daily, with monthly filling and preparation as required by the Clinical Laboratory Institute for standardization.
Data Processing and Analysis
The data was coded and entered into Epi Info version 7.2.4.0 and then imported to SPSS version 20 for analysis. Descriptive statistics like frequencies, tables, and figures were used to summarize the characteristics of the study population. The Shapiro–Wilks test was used to check for the normality of the data. Comparison of normally distributed data between the two groups was done by an independent t-test, and the results were expressed as mean ± standard deviation (SD), whereas the Mann–Whitney U-test was used for comparison of non-normally distributed data, and the results were presented as median and Inter-quartile Range (IQR).
The Hosmer and Lemeshow test statistics were performed to check for the goodness of fit. The chi-square test was used to determine the significance of an assumed association. To determine factors associated with coagulopathy in OC users, bivariable and multivariable logistic regression analyses were used. The odds ratio with its 95% confidence interval was used to determine the strength of association between the predictor and dependent variable. Variables whose P value of less than 0.25 on Bivariable analysis were entered jointly into a multivariable logistic regression analysis. A p-value of less than 0.05 was considered statistically significant.
Results
Socio-Demographic and Clinical Characteristics of Study Participants
A total of 393 participants (131 COC users and 262 age matched non-COC women) were enrolled in this study. The study participants’ age ranged from 18 to 38 years old with a mean age of 27.67±4.14 years (28.12±4.49 years old for COC users and 27.45±3.94 years old for non-COC-users, P=0.314). Out of the included participants, 364 (92.6%) were urban residents, and 142 (36.1%) had no formal education. The majority of the study participants were self-employed 192 (49.2%), and 183 (46.6%) were married (Table 1).
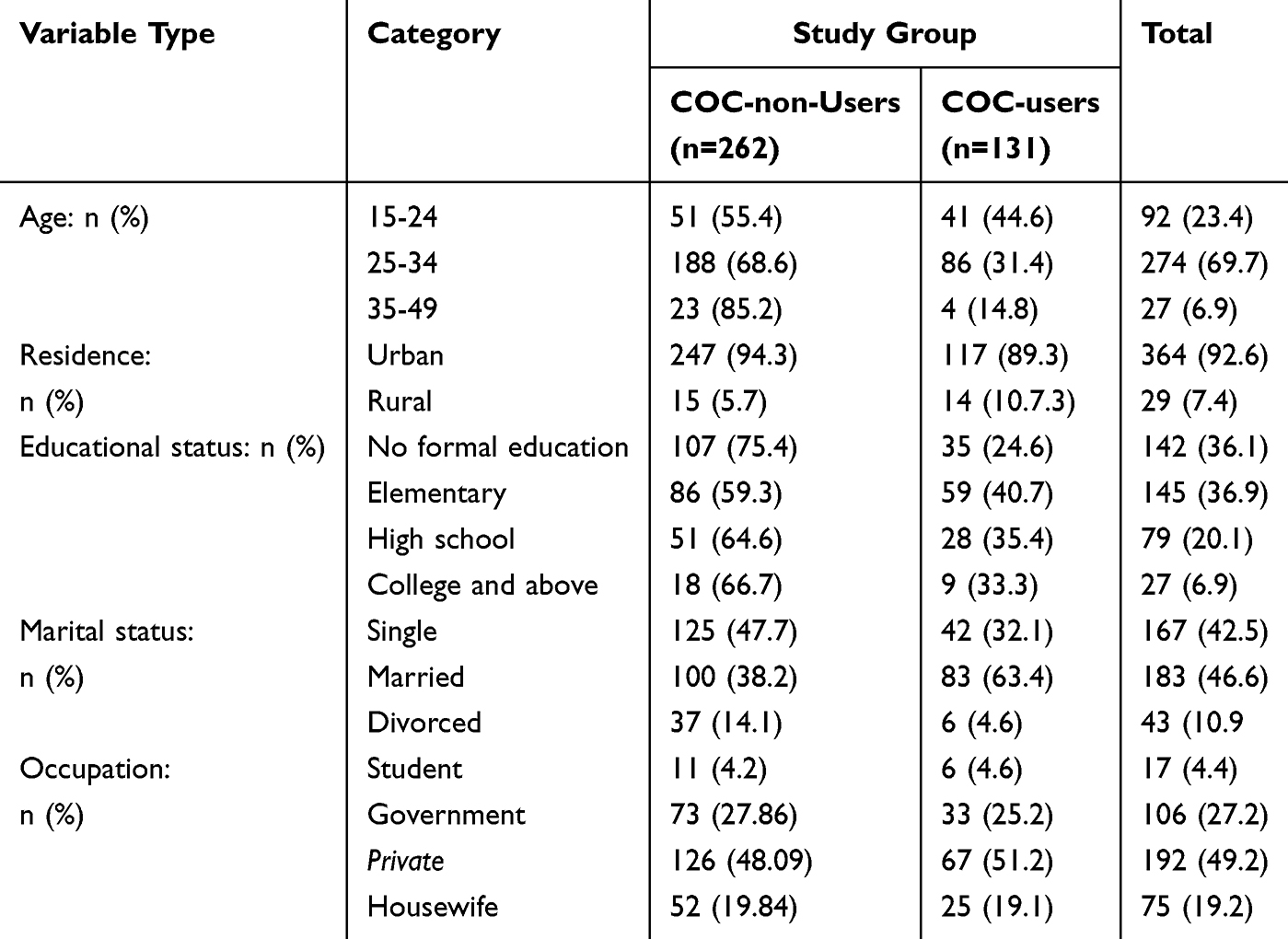 |
Table 1 Socio-Demographic Characteristics of Study Participants Attending at Family Guidance Association of Ethiopia, Jigjiga Medium Clinic (n=393) |
Clinical and Behavioral Characteristics of Study Participants
About 118 (30%) of the study participants had a habit of alcohol drinking. All of the study participants were cigarette non-smokers. Of the total study participants, 25 (6.4%) had a family history of CVD. The number of participants with hypertension were 150 (38.2%). Regarding the duration of COC usage, the majority of the participants (65.6%) have used COC for more than five years (Table 2).
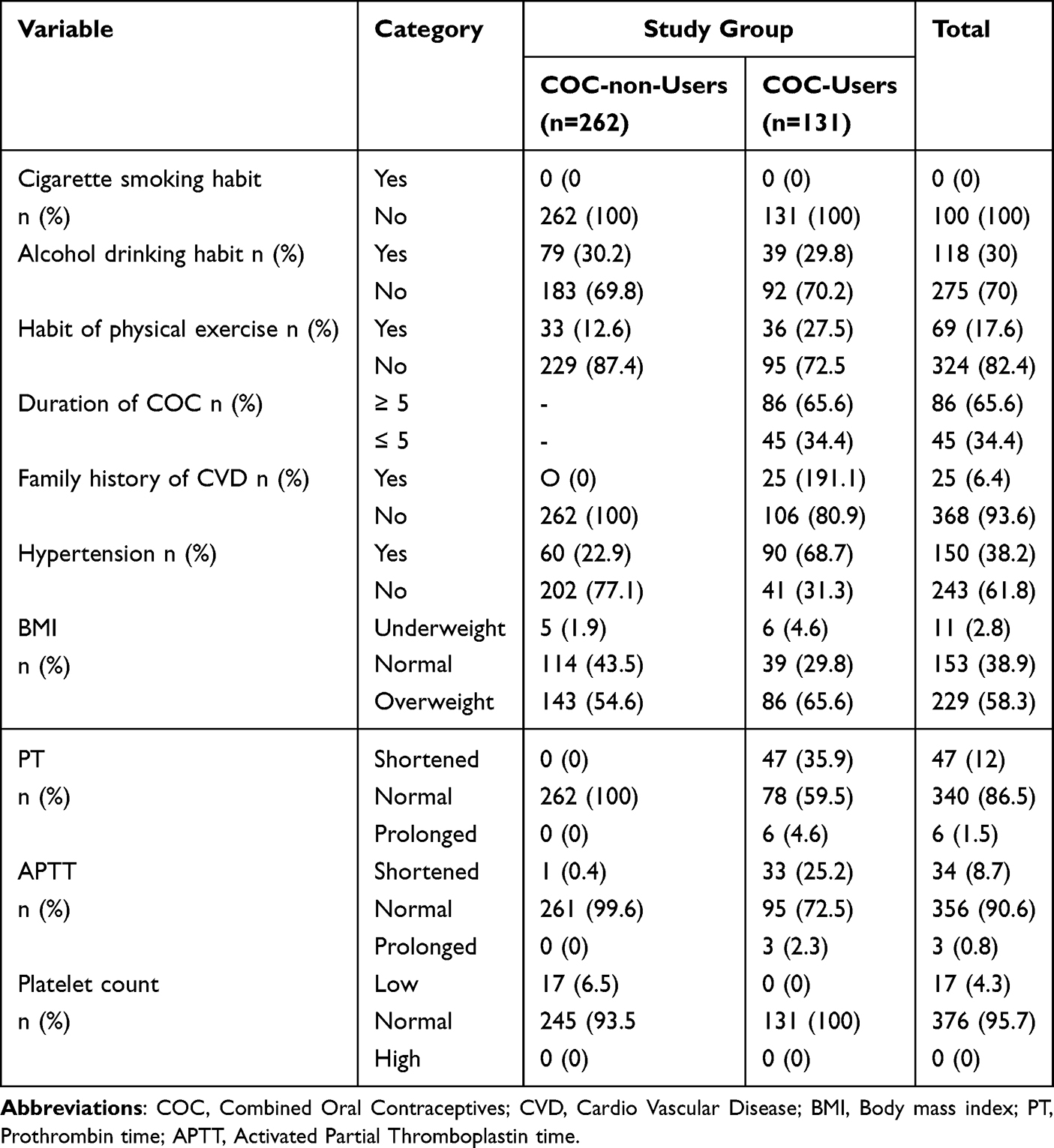 |
Table 2 Clinical and Behavioral Characteristics of the Study Participants Attending at Family Guidance Association of Ethiopia, Jigjiga Medium Clinic (n=393) |
Comparison of Coagulation Parameters Among COC-Users and Non-Users
Coagulation Profiles Among Combined Oral Contraceptive Users and Non-Users
The independent sample T-test analysis revealed that both PT and APTT were significantly lower among COC-user women compared to the control non-COC-user women. The mean difference indicated that PT and APTT were lower by −1.14 (−1.36,-0.92) and −2.48 (−3.04, −1.91), respectively, in COC user women in reference to their age-matched non-COC user counterparts. However, platelet count was significantly elevated in the COC users group (P-value <0.001). The mean ±SD value for platelet count was 259.5±79.00 and 191.1±27.98 for COC users and non-users, respectively (Table 3).
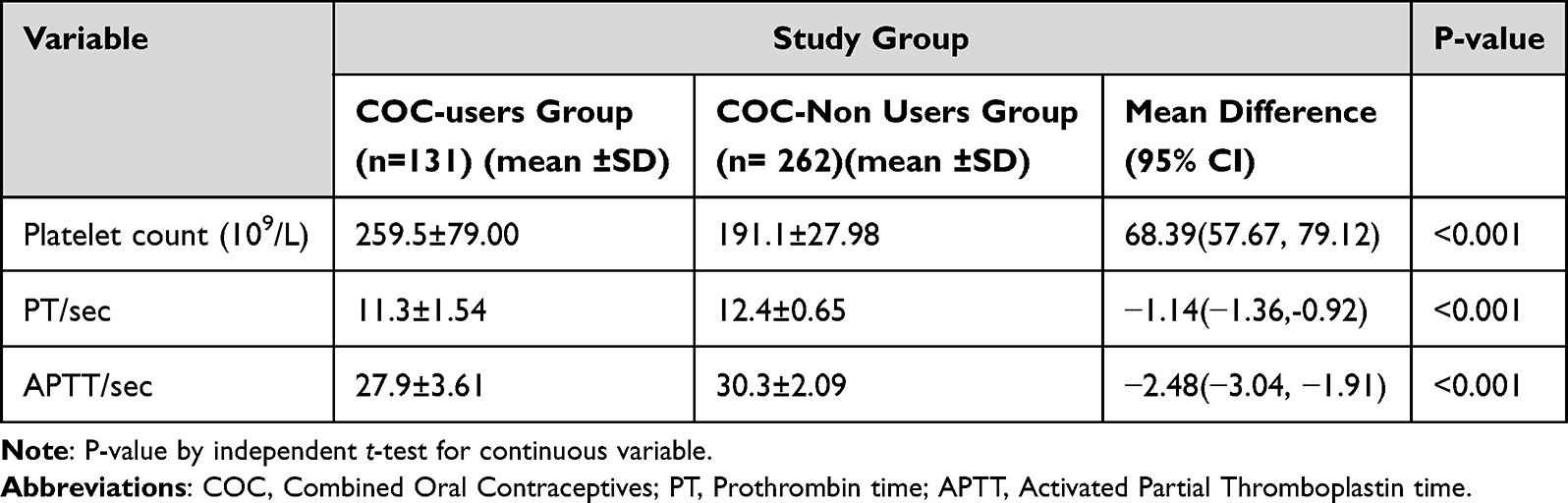 |
Table 3 Comparisons of Coagulation Parameters Between COC Users and Non-Users Women Attending at the Family Guidance Association of Ethiopia, Jigjiga Medium Clinic (n=393) |
Prevalence of Coagulopathy Among COC Users
The overall prevalence of coagulopathy among COC users was 38.9% (51/131): 40.5% (53/131) and 27.5% (36/131) of the COC users showed shortened PT and shortened APTT, respectively. On the other hand, the platelet count of all COC users was within the normal adult reference range (Figure 1).
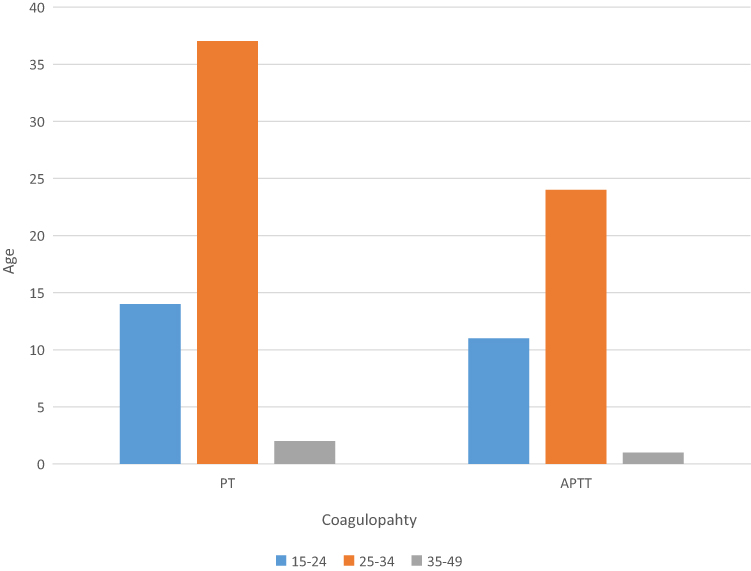 |
Figure 1 Type of coagulopathy identified from COC users. |
Factors Associated with Coagulopathy Among COC Users
To identify factors associated with coagulopathy, bivariable and multivariable logistic regression analyses were done. In bivariable logistic regression analysis, Residency ((COR) = 4.0; 95% CI: 1.18–13.5), Level of education ((Elementary, (COR) = 0.04; 95% CI: 0.005–0.396), High school (COR) = 0.06; 95% CI: 0.007–0.549)), Occupation ((Government, (COR) = 5.70; 95% CI: 0.619–53.426), Private (COR) = 8.47; 95% CI: 1.70–42.03), Housewife (COR) = 11.16; 95% CI: 2.44–51.15)), Duration of COC use (COR) = 0.02; 95% CI: 0.01–0.08), Hypertension (COR) = 0.06; 95% CI: 0.02–0.20) and BMI (Overweight (COR) = 0.08; 95% CI: 0.03–0.24)) showed association with coagulopathy. Consequently, these variables were subjected to multivariable logistic regression. On the other hand, the study participants’ age, marital status, Alcohol drinking habits, smoking, physical exercise, and family history of CVD did not show any association with coagulopathy.
However, in multivariable analysis, the Duration of COC for >5 years (AOR = 0.035; 95% CI: 0.004–0.343) was significantly associated with coagulopathy. On the other hand, Residency, Level of education, Occupation, Hypertension, and BMI did not show any statistically significant association with coagulopathy (Table 4).
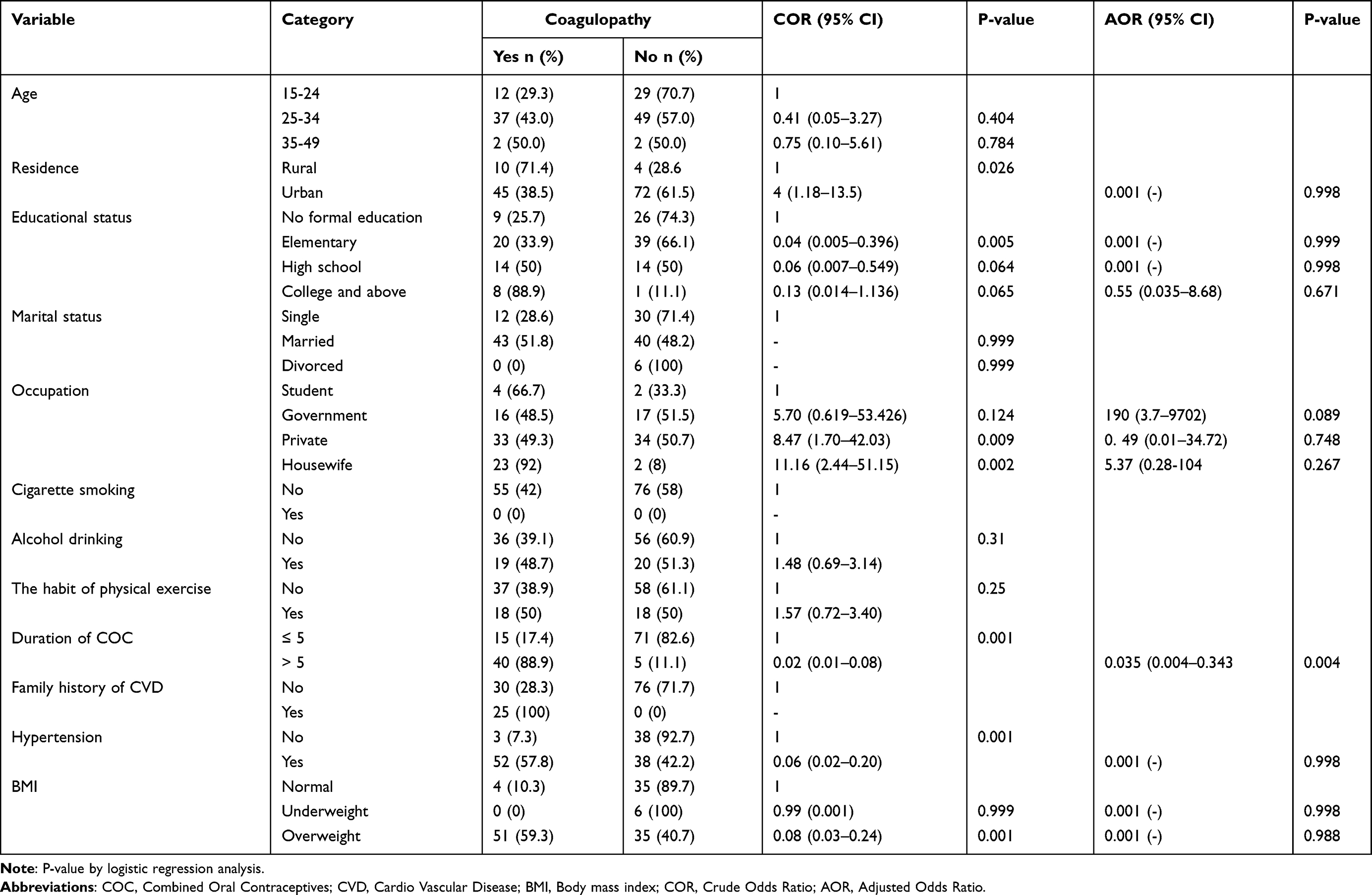 |
Table 4 Factors Associated with Coagulopathy Among COC Users |
Discussion
Coagulopathy is a chief cause of public health issues that lead to morbidity or mortality worldwide.35 Globally, about 5–10% of women in their reproductive years seek therapy for heavy menstrual bleeding.15 Hence, this study aimed to evaluate the mean value of platelet count, PT, and APTT among COC users and non-users and to determine factors associated with coagulopathy among COC users attending the FGAE, Jigjiga Medium Clinic, Eastern Ethiopia.
The combined oral contraceptive is designed to be taken orally by women to avoid pregnancy.36 It is the oral version of combined hormonal contraception that includes synthetic forms of both estrogen and progestin. A significant number of women continue to use COC to prevent unintended pregnancies, accounting for 8.8% of contraceptive prevalence, with this figure rising to 15.4% in developed nations.37 COC has been linked to various side effects, including increased thromboembolic risks, Cardiovascular Issues, and coagulation abnormalities.38
In this study, PT and APTT were shortened in COC user women compared to their age-matched non-COC user counterparts with a mean difference of −1.14/sec and −2.48/sec, respectively. This might be due to the hormone estrogen, which is associated with several prothrombotic pathways that alter coagulation proteins and shift the hemostatic balance in favor of a prothrombotic condition. Some of these alterations include activated protein C resistance, decreased levels of protein S, antithrombin (AT), and increased prothrombin levels, which produce a net prothrombotic effect.39 The administered COC is known to affect the coagulation system by increasing the hepatic production of several coagulation factors, such as elevated amounts of factors II, VII, VIII, X, and fibrinogen. Consequently, these changes may result in shortened PT and APTT in COC user women.40
This finding is in agreement with other similar studies by Tsakok et al in Singapore,41 Ayesha et al in the USA,42 Stocco et al in Brazil,43 AL-Husaynee et al in Iraq,44 and Babatunde et al in Nigeria.45 However, this finding is in contradiction with a study conducted by Ayesha et al in the USA42 and Erhabor et al in Nigeria46 that reported an insignificant decrement in APTT among COC users. Furthermore, a study conducted by Elsayid et al in Sudan reported a significantly elevated APTT value among oral contraceptive users.24 These disagreements may have been caused by variations in the study population, the sample size, the study design and the reference range used for the coagulation tests.
Furthermore, this study assessed platelet count among COC users and non-users. The mean ±SD value of platelet count was 259.5±79.00 and 191.1±27.98 in COC users and non-COC users, respectively. The independent T-test indicated that platelet count was significantly elevated in the COC user woman by 68.39 × 109/L compared to non-COC users (P-value <0.001). The elevated platelet count observed in women using COC can be attributed to several physiological mechanisms associated with hormonal changes induced by these medications. During the reproductive years, estrogen administration dramatically boosts the division and proliferation of HSCs in women, which may account for the rise in platelets.40 The finding of platelet count is in line with similar studies conducted by Samsunnahar et al in Bangladesh,13 AL-Husaynee et al in Iraq,44 and Babatunde et al in Nigeria.45
In addition, this study also assessed the prevalence and associated factors of coagulopathy among COC users. The overall prevalence of coagulopathy was 38.9%: from this abnormality, 40.5% of the COC users showed shortened PT, and 27.5% showed shortened APTT. However, the COC users had platelet counts within the normal range. The shortening of both PT and APTT is associated with enhanced procoagulant effects, decreased anticoagulant effects, and equivocal effects on fibrinolysis. Oral contraceptives have a net prothrombotic impact (with increases in the activity of the antifibrinolytic system).47 In this study, the duration of COC use for more than 5 years was significantly associated with coagulopathy. This finding is in line with a study conducted by Abudegin O.48 However, a study conducted in Sudan by Elsayid et al reported that no significant changes were noticed in terms of the duration of oral contraceptive use.24
Strengths and Limitations of the Study
The study’s strength includes the comparison of coagulation profiles among groups in a large sample size, and associated factors were evaluated in detail. The first major limitation of this study was that the fibrinolytic assays were not studied, and a specific factor assay was not performed.
Conclusions
The present study verified that there is a high prevalence of coagulopathy among reproductive-age women who use COC. The use of hormonal contraceptives leads to a modified hemostatic profile characterized by increased procoagulant activity, which elevates the thrombogenic risk for users compared to nonusers. This study also found that COC users exhibited a greater tendency toward hypercoagulability, placing them at a higher risk of thromboembolic effects compared to those who do not use COC. Long-term usage of COC can lead to hypercoagulation and thrombotic abnormalities.
Abbreviations
AOR: Adjusted Odds Ratio; APC: Activated Protein C; APTT: Activated Partial Thromboplastin Time: BMI: Body Mass Index; CBC: Complete Blood Count; COC: Combined Oral Contraceptive; COR: Cruds Odds Ratio; CSA: Central Statistic Agency; EDTA: Ethylene Diamine Tetra Acetic acid; FGAE: Family Guidance Association of Ethiopia; FSH: Follicle-Stimulating Hormone; IQR: Inter-quartile Range; LH: Luteinizing Hormone; OC: Oral Contraceptives; PT: Prothrombin Time; SD: Standard Deviation; SOP: Standard Operating Procedure; SPSS: Statistical Package for Social Science; TG: Thrombin Generation; TM: Thrombin-Thrombomodulin.
Data Sharing Statement
All relevant data supporting the findings are within the manuscript.
Ethical Approval
This study complies with the Declaration of Helsinki. It study was conducted after ethical clearance was issued by the Ethical Review Committee of Jigjiga University (RERC/064/2024). A permission letter was obtained from the FGAE, Jigjiga Medium Clinic. Informed written consent was obtained from each study participant, and the findings were kept confidential. Informed assent and informed consent were obtained from participants aged 15 to 17 years and their parents or guardians, respectively. The confidentiality of the data was protected by using codes for specimens and results, and no personal identification was used. In case of abnormal results, it was informed to their doctors to get adequate treatment.
Acknowledgment
We would like to acknowledge Jigjiga University, the Institute of Health Sciences, Research Coordination Office for giving us the chance to conduct this study. Next, we would like to extend our warmest thanks to the Family Guidance Association of Ethiopia: Jigjiga Medium Clinic for permitting this study. Last but not least, we would like to thank all study participants who volunteered to participate in this study.
The authors affirm that this thesis is our original work, has not been submitted for a degree at this or any other university, and that all sources of materials utilized in the thesis have been properly acknowledged.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
For the research, writing, and/or publication of this article, the author(s) did not receive any funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Bansode OM, Sarao MS, Cooper DB. Contraception. In: StatPearls. Treasure Island (FL) ineligible companies StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC; 2025. Disclosure: Manbeer Sarao declares no relevant financial relationships with ineligible companies. Disclosure: Danielle Cooper declares no relevant financial relationships with ineligible companies.
2. Palmery M, Saraceno A, Vaiarelli A, Carlomagno G. Oral contraceptives and changes in nutritional requirements. Eur Rev Med Pharmacol Sci. 2013;17(13):1804–1813.
3. Use WC. United nations department of economic and social affairs. 2007.
4. Cooper DB, Patel P. Oral contraceptive pills. In: StatPearls. Treasure Island (FL) ineligible companies. StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC.; 2025. Disclosure: Preeti Patel declares no relevant financial relationships with ineligible companies.
5. Cable JK, Grider MH. Physiology, progesterone. In: StatPearls. Treasure Island (FL) ineligible companies, StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC.; 2025. Disclosure: Michael Grider declares no relevant financial relationships with ineligible companies.
6. Okigbo CC, Gill S, Hall JE. The Hypothalamic-Pituitary Axis in PCOS. Polycystic Ovary Syndrome: Current and Emerging Concepts. Springer; 2022:73–93.
7. Freeborn D, Burd I. Contraception/birth control. Nationwide Children’s Hospital. 2023.
8. Daniels K, Joyce C. Current contraceptive status among women aged 15–49: united States. Center for Disease Control and Prevention. 2015-2017.
9. Ethiopian public health Institute (EPHI)[Ethiopia] and ICF. Ethiopia Mini Demographic Health Survey: Key Indicators 2019.
10. Rosendaal F, Van Hylckama Vlieg A, Tanis B, Helmerhorst F. Estrogens, progestogens and thrombosis. J Thromb Haemost. 2003;1(7):1371–1380. doi:10.1046/j.1538-7836.2003.00264.x
11. Lichota A, Szewczyk EM, Gwozdzinski K. Factors affecting the formation and treatment of thrombosis by natural and synthetic compounds. Int J Mol Sci. 2020;21(21):7975. doi:10.3390/ijms21217975
12. Dahlbäck B, Villoutreix BO. Regulation of blood coagulation by the protein C anticoagulant pathway: novel insights into structure-function relationships and molecular recognition. Arterioscler Thromb Vasc Biol. 2005;25(7):1311–1320. doi:10.1161/01.ATV.0000168421.13467.82
13. Akhter QS, Akhter N, Begum UN, Rahman F. Assessment of coagulation disorder in women taking oral contraceptives. J Bangladesh Soc Physiol. 2014;9(1):1–5.
14. Owaidah T, Saleh M, Alzahrani H, et al. Prevalence of bleeding symptoms among adolescents and young adults in the capital city of Saudi Arabia. Advances in Hematology. 2018;2018:1–8. doi:10.1155/2018/1858241
15. Mellins CA, Tassiopoulos K, Malee K, et al. Behavioral health risks in perinatally HIV-exposed youth: co-occurrence of sexual and drug use behavior, mental health problems, and nonadherence to antiretroviral treatment. AIDS Patient Care and STDs. 2011;25(7):413–422. doi:10.1089/apc.2011.0025
16. Lidegaard Ø, Løkkegaard E, Svendsen AL, Agger C. Hormonal contraception and risk of venous thromboembolism: national follow-up study. BMJ. 2009;339.
17. van Hylckama Vlieg A, Middeldorp S. Hormone therapies and venous thromboembolism: where are we now? J Thromb Haemost. 2011;9(2):257–266. doi:10.1111/j.1538-7836.2010.04148.x
18. Mohamed AB, Kelchtermans H, Konings J, et al. The effects of oral contraceptive usage on thrombin generation and activated protein C resistance in Saudi women, with a possible impact of the body mass index. PLoS One. 2018;13(10):e0206376. doi:10.1371/journal.pone.0206376
19. Brandy KR, Meyer RM, Luo X, Rao GH, Datta YH, Divani AA. Evaluation of the coagulation profile among oral and vaginal combined hormonal contraceptive users using sonoclot coagulation analyzer. Clin Appl Throm/Hemostasis. 2012;18(6):576–581. doi:10.1177/1076029611434526
20. Abdulrahaman Y. Dallatu MJNjob, sciences a. Evaluation of prothrombin time and activated partial thromboplastin in patients with diabetes mellitus. Nig J Basic Appl Sci. 2012;20(1):60–63.
21. Sapkota B, Shrestha SK, Poudel S. Association of activated partial thromboplastin time and fibrinogen level in patients with type II diabetes mellitus. BMC Res Notes. 2013;6(1):485. doi:10.1186/1756-0500-6-485
22. Population Census Commission. Summary and Statistical Report of the 2007 Population and Housing Census. Population Size by Age and Sex. 2008:314
23. Jigjig woreda health department office Annual health service report, jigjig 2002.
24. Elsayid M, Elbasheer MAM, Elgari MM, Elfaki TEM. The effect of contraceptive pills on coagulation tests among sudanese women in Khartoum State-Sudan. IJSR. 2016.
25. Em O, Ee M, E-Ab S, Jz A. Isolated effect of progestogen-only contraceptives on some coagulation parameters of women attending family planning clinics In Kaduna State, Nigeria. Eur J Biomed Pharm Sci. 2019;6(1):01–10.
26. Mega JL, Simon T. Pharmacology of antithrombotic drugs: an assessment of oral antiplatelet and anticoagulant treatments. Lancet. 2015;386(9990):281–291. doi:10.1016/S0140-6736(15)60243-4
27. Ek A. Promoting public health by Physical activity on Prescription, with focus on organized exercise [Internet] [Dissertation]. Master of Public Health, MPH: 2011.
28. Naif HM. Pathogenesis of HIV infection. Infect Dis Rep. 2013;5(Suppl 1):e6. doi:10.4081/idr.2013.s1.e6
29. Weir CB, Jan A. BMI classification percentile and cut off points. In: StatPearls. StatPearls Publishing; 2019:1–10.
30. Manual AP. Anthropometry Procedures Manual for National Health and Nutrition Examination Survey. Atlanta: CDC; 2007.
31. Sultan A. Five-minute preparation of platelet-poor plasma for routine coagulation testing. East Mediterr Health J. 2010;16(2):233–236. doi:10.26719/2010.16.2.233
32. Adinew T. Performance Evaluation of Cell-Dyn 1800 and Sysmex KX-21 Hematology Analyzers at St. Addis Ababa, Ethiopia: Paul’s Hospital Millennium Medical College, Addis Ababa University; 2015.
33. Ignjatovic V. Prothrombin time/international normalized ratio. Meth Mol Biol. 2013;992:121–129.
34. Ignjatovic V. Activated partial thromboplastin time. Meth Mol Biol. 2013;992:111–120.
35. Aynalem M, Shiferaw E, Gelaw Y, Enawgaw B. Coagulopathy and its associated factors among patients with a bleeding diathesis at the University of Gondar Specialized Referral Hospital, Northwest Ethiopia. Thrombosis J. 2021;19(1):36. doi:10.1186/s12959-021-00287-6
36. United Nations Department of Economic and Social Affairs Population Division. Contraceptive Use by Method 2019: Data Booklet. United Nations; 2019.
37. Christin-Maitre S. History of oral contraceptive drugs and their use worldwide. Best Pract Res Clin Endocrinol Metab. 2013;27(1):3–12. doi:10.1016/j.beem.2012.11.004
38. Morimont L, Haguet H, Dogné JM, Gaspard U, Douxfils J. Combined oral contraceptives and venous thromboembolism: review and perspective to mitigate the risk. Front Endocrinol. 2021;12:769187. doi:10.3389/fendo.2021.769187
39. Kolovou G, Giannakopoulou V, Vasiliadis Y, Bilianou H. Effects of estrogens on atherogenesis. Curr Vasc Pharmacol. 2011;9(2):244–257. doi:10.2174/157016111794519327
40. Tekle E, Gelaw Y, Asrie F. Hematological profile changes among oral contraceptive users: a narrative review. J Blood Med. 2022;13:525–536. doi:10.2147/JBM.S379841
41. Tsakok FH, Koh S, Ratnam SS. Effects of oral contraceptives containing 50 microgram estrogen on blood coagulation in non-Caucasian women. Contraception. 1980;21(5):505–527. doi:10.1016/0010-7824(80)90015-3
42. Zia A, Callaghan MU, Callaghan JH, et al. Hypercoagulability in adolescent girls on oral contraceptives‐global coagulation profile and estrogen receptor polymorphisms. Am J Hematol. 2015;90(8):725–731. doi:10.1002/ajh.24064
43. Salman ST, Hussein AA, Saadi RK. Effect of combined oral contraception on coagulation profiles in women attending fertility control clinic in Baqubah City-Iraq. J Fac Med Baghdad. 2018;60(1):47–51. doi:10.32007/jfacmedbagdad.v60i1.44
44. Kashmoola MA, AL-Husaynee AJ. Effect of combined oral contraceptive pills on some haemostatic parameters. Ann Coll Med Mosul. 2007;33(1):66–69. doi:10.33899/mmed.2007.8834
45. Babatunde AS, Olatunji PO. Short-term effect of oral contraceptive pills on some haemostatic parameters in healthy Nigerian women. Niger Postgrad Med J. 2004;11(4):246–250. doi:10.4103/1117-1936.175164
46. Osaro E, Isaac I, Kaoji A, John R, Suleiman S. Assessment of some coagulation parameters among clients on hormonal contraceptive in a tertiary health facility in Sokoto, north western, Nigeria. Hematol Thrombo Dis. 2014;2(139):2.
47. Kuhl H, März W, Jung-Hoffmann C, Heidt F, Gross W. Time-dependent alterations in lipid metabolism during treatment with low-dose oral contraceptives. Am J Clin Exp Obstet Gynecol. 1990;163(1 Pt 2):363–369. doi:10.1016/0002-9378(90)90583-S
48. Abudegin O, Elsigar L, Ali M, Khalifa E. Evaluation the effect of oral contraceptive pills on coagulation profile in Sudanese women in Shendi -Sudan. World J Biol Pharm Health Sci. 2022;12:028–33. doi:10.30574/wjbphs.2022.12.1.0098
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.