Back to Journals » Journal of Healthcare Leadership » Volume 18
Coaching as a Core Leadership Capability in Healthcare: A Framework for Embedding Adaptive Leadership Behavior in Complex Health Systems
Authors Kloek C ![]()
Received 5 April 2026
Accepted for publication 1 June 2026
Published 12 June 2026 Volume 2026:18 614661
DOI https://doi.org/10.2147/JHL.S614661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Russell Taichman
Carolyn Kloek1,2
1Department of Ophthalmology, University of Oklahoma College of Medicine, Oklahoma City, OK, USA; 2OU Health, Oklahoma City, OK, USA
Correspondence: Carolyn Kloek, OU Health, 700 NE 13th Street, Oklahoma City, OK, 73104, USA, Email [email protected]
Background: Healthcare systems face a persistent gap between the complexity of their adaptive challenges and the leadership behaviors applied to address them. Improvement efforts frequently plateau not for lack of commitment or tools, but because leadership behaviors remain primarily directive and technical in orientation.
Purpose: In this perspective, we synthesize current evidence and leadership theory to propose a practical framework for coaching as a core leadership behavior in complex health systems—applicable across clinical and operational domains, at every level of leadership.
Key Argument: Coaching in this context does not refer to professional executive coaching services. It refers to a learnable, observable set of leadership behaviors—a coaching stance, organizational listening, and coaching questions—that shift organizations from episodic problem-solving to sustained adaptive capacity. These behaviors are distinct from existing literature on physician coaching as a wellness or remediation intervention; the argument here is that coaching must be embedded as a leadership infrastructure capability across the enterprise.
Practice Implications: A practical framework—three core leadership behaviors and two organizational routines—is proposed to guide health system leaders in embedding coaching capability regardless of organizational size or maturity. Early implementation at an academic health system informs the framework and will be the subject of subsequent outcome reporting.
Keywords: coaching, leadership behavior, adaptive leadership, organizational learning, health systems, physician leadership, psychological safety, improvement science
Introduction
A hospitalist with twenty years of expertise in complex heart failure management watches the health system implement a standardized clinical pathway. Her accumulated clinical judgment—the nuanced pattern recognition that defines her practice—is reframed as “variation.” The pathway may be evidence-based and well-intentioned, but she experiences it as diminishment. Her resistance is not defiance; it is grief. And the leader who responds by tightening oversight will achieve compliance without understanding, and lose the signal embedded in that resistance.
This scenario captures a fundamental challenge in healthcare improvement: the mismatch between the nature of adaptive challenges and the leadership behaviors applied to address them.1,2 When improvement plateaus despite sustained effort, the issue is rarely commitment or discipline. More often, leaders are deploying technical responses to problems that require learning, interpretation, and behavior change.
A growing body of evidence illustrates this gap. Research from the Institute for Healthcare Improvement demonstrates that organizations achieving sustained improvement share common characteristics: psychological safety, distributed leadership, and learning behaviors.1,3 Leadership development research similarly identifies coaching behaviors as critical to cultures of sustained performance.4 A systematic review of coaching outcomes confirms sustained effects on8 leader development and performance, and a recent evidence review focused on physician leadership coaching came to the same conclusions.5,6 Recent scholarship in BMJ Leader has examined the health leader-as-coach role specifically, summarizing evidence that line managers who consciously deploy coaching skills benefit their teams, organizations, and the broader system.7
Most recently, Quiroga and Lee argued that healthcare’s most consequential challenges — burnout, workforce shortages, inequities, patient experience are complex rather than complicated, and that leadership approaches developed for complicated work have limited effectiveness in this terrain.8 Their commentary names the gap while this perspective defines leadership behaviors to close it and builds on this foundational work in two ways.
First, while existing literature has largely framed coaching as a professional service received by leaders or a wellness intervention for burnout, this paper argues that coaching must be understood as a leadership behavior—something leaders do, not something done to them. Second, this perspective proposes a concrete framework that health systems can implement regardless of size or maturity. Drawing on leadership theory, improvement science, and early implementation experience at an academic health system, we propose that embedding coaching as a core leadership behavior is not a developmental aspiration but a structural requirement for health systems navigating increasing complexity.
Why Technical Approaches Fall Short
Healthcare improvement has been shaped by methods designed for complicated work, domains where cause and effect are knowable, concrete steps can be followed, and standardization produces reliable results. The WHO surgical safety checklist is an example: a brief structured set of pre-surgical steps that, when reliably executed, reduces surgical complications and mortality.9
Other challenges are complex, shaped by assumptions, relationships and interpretation, with no predetermined right answer that expertise or a series of executed steps can solve.10 A health system with OR staff that are reluctant to speak up about unsafe conditions or near-miss events is one such case: the reporting system exists and policy mandates its use, yet the behavior the system depends on to support patient safety does not follow.3
A recent commentary extends this distinction directly to healthcare leadership, arguing that defaulting to complicated-system tools such as committees, multiyear plans, ROI gates when problems are complex stalls progress and suppresses learning.8,11
Complicated and complex problems call for different kinds of leadership response. Technical responses, best suited for complicated problems, apply existing knowledge and authority. They can be executed by experts who share and disseminate knowledge and tools and enforced through policy. Adaptive responses, most effective for complex problems, ask people in the system to change how they think, act, or what they value; no expert or policy can do that work on their behalf.2
Complex healthcare problems characteristically generate adaptive work; complicated ones, technical work, but the mapping is not automatic. The persistent failure in healthcare improvement is responding to adaptive work as if it were technical.
These directive methods remain essential: in cardiac arrest management, clear role assignment is lifesaving; in infection prevention, evidence-based bundles reduce preventable harm.
Consider a hospitalist team rounding after a weekend of admissions. The discharge checklist is at 95% completion, teach-back is documented in every note, the post-discharge call goes out within 48 hours. Yet patients keep coming back and the readmitted patients often went home with a prescription they could not fill: the pharmacist thought the case manager was confirming access, the case manager thought the resident had asked at the bedside, and no one on the team had confirmed the patient could obtain and afford the medication. The discharge protocol is intact but the shared accountability and communication that makes the protocol work is not.
Leadership responses suited to complicated problems such as clear directives, tighter controls, rapid problem-solving can unintentionally suppress learning when the challenge is adaptive. When leaders default to enforcing compliance, systems lose the capacity to surface emerging risks and test assumptions. Improvement stalls not for lack of discipline, but for lack of adaptive learning.
Figure 1 summarizes this logic by showing how a challenge is diagnosed and how the appropriate leadership response is determined. Furthermore, a coaching response converts an adaptive challenge into a sustainable system capability instead of compliance.
 |
Figure 1 Coaching as a leadership behavior in complex health systems. This framework is intended as a diagnostic for healthcare system leaders when evidence-based practices do not sustain, metrics plateau, or change initiatives stall despite sound design. The figure asks the prior question: is the problem complicated, where cause and effect are knowable and standardization produces reliable results, or complex, where the problem is shaped by assumptions, relationships, and interpretation, and no predetermined solution applies? Complicated problems generate technical work, appropriately met with directive leadership. Complex problems generate adaptive work; when leaders respond to that work as if it were technical, systems achieve compliance with gains that do not sustain (red dashed path). When leaders meet adaptive work with coaching as a leadership behavior, three capabilities and two organizational routines build durable adaptive capacity that sustains improvement and feeds readiness for the next challenge (green dashed path). The framework integrates established constructs including adaptive leadership theory,2 the complicated/complex distinction,10 organizational listening as a leadership capability,12 the leader-as-coach,7,13 and improvement science as a learning system14 into an operational diagnostic for healthcare system leaders. Color coding in Figure 1 distinguishes elements of the framework: beige boxes indicate diagnostic and problem identification; blue boxes represent directive leadership applied to complicated problems; purple boxes represent coaching as a leadership behavior applied to complex problems; Orange represents the two organizational routines; green boxes represent the durable adaptive capacity that coaching produces; and the red box represents the failure mode that occurs when adaptive work is treated as if it were technical. This perspective does not propose new leadership constructs; its contribution is the synthesis of established constructs into an operational framework, and the distinction between coaching as a leadership behavior and the substantial existing literature on coaching as a service or wellness intervention. |
Coaching as Leadership Behavior: Defining the Distinction
Who practices coaching behaviors in healthcare leadership? In the framework presented here, coaching behaviors can be applied by any individual who is leading in a healthcare system. The physician role appears most often in the illustrative examples, though the framework applies to leaders in any critical healthcare role.
Who receives coaching? Again, this can apply to individuals in any role across the system, most typically a leader interacting with a direct report, but equally a leader working with a team.
In healthcare, the term coaching is used imprecisely.7 It frequently refers to hiring external executive coaches, providing individualized support during underperformance, or—as a growing body of literature describes—professional coaching interventions to address burnout and promote physician well-being.15,16 These approaches carry real value. But they are not what this perspective addresses.
The focus here is coaching as a core leadership competency: a learnable, observable set of behaviors that leaders at every level can practice in daily interactions. This framing aligns with Ibarra and Scoular’s influential Harvard Business Review analysis of the leader-as-coach, which argues that effective leaders must shift from being directive problem-solvers to enabling the problem-solving capability of others.13 It extends Day’s BMJ Leader synthesis of the health leader-as-coach literature, which summarizes benefits while noting that no consistent academic definition or specific competencies yet exist for this role in healthcare contexts.7 Competencies have since been defined for professional coaches who work with physicians, but these address external coaching relationships rather than coaching as a behavior integrated into leadership practice, which is the position of this perspective.17
Coaching as a leadership behavior does not replace decisiveness or accountability. It shapes when leaders direct and when they listen; when they intervene and when they allow learning to unfold.
Enforcing infection prevention protocols is a technical leadership task requiring clarity and authority. Helping a team explore why workarounds persist despite clear expectations and repeated reinforcement is a complex challenge requiring an adaptive approach. Both are essential. They are not interchangeable and applying a technical response to an adaptive problem reliably produces short-term compliance with risk of long-term slide.
Coaching as a leadership behavior is key to addressing complex problems in healthcare that require adaptive responses. In practice, coaching as a leadership behavior shows up through three interrelated capabilities: a coaching stance, organizational listening, and coaching questions. Together, these create the conditions in which teams can reflect, surface early signals, test assumptions, and adapt.
The Three Capabilities: A Practical Framework
Coaching Stance
A coaching stance is a deliberate orientation toward curiosity rather than certainty and a posture that treats the knowledge and perspective of those a leader leads as critical inputs rather than obstacles to a predetermined solution. Leaders who hold a coaching stance ask before they tell, probe beneath the presenting concern, and treat resistance and skepticism as information rather than defiance.18 They seek to understand before determining the next action.
Clinical training, particularly in medicine, is built to install a cognitive framework that lets clinicians process large volumes of information, recognize patterns under time pressure, and apply evidence-based protocols to deliver care. This training works as it produces the diagnostic and therapeutic competence that good clinical care depends on. This formation builds specific instincts. Clinical decisions are often time-sensitive, sometimes life-or-death, and the clinician is trained to act under uncertainty rather than wait for it to resolve.
Trainees learn early that hesitation can harm and that the team and the patient need a leader who appears sure of the next step so projected certainty becomes part of the role, often beyond what the underlying evidence strictly supports. The academic hierarchy reinforces this pattern: the resident who answers crisply, the attending who decides decisively, the senior leader who closes meetings with clear next steps each earns trust and advancement through the same set of habits.
Yet adaptive work asks for the opposite. It requires sitting with uncertainty rather than acting through it, slowing down when the trained instinct is to move, staying with a question long enough to surface what is actually beneath it. The instincts that make a clinician effective in running a code are the instincts that, applied to adaptive work, shut down the very inquiry on which adaptive work depends.
Mature healthcare leadership requires both modes. Directive leadership remains essential when the problem is complicated and a clear next step exists while a coaching stance is an alternative mode, available when the work is adaptive and the next step must be surfaced rather than supplied. The key healthcare leadership skill is recognizing which the situation calls for, and choosing the leadership approach the work requires.
This second mode is not foreign to clinicians. They are trained to begin patient encounters with open-ended questions to better understand and explore the patient’s experience before narrowing toward diagnosis. The same logic applies when the work is adaptive: understanding how the work is being experienced by those a leader leads is the equivalent prerequisite — the leadership history before the leadership intervention.
Table 1 illustrates the language shift involved, contrasting the directive responses to which leaders default under pressure with coaching-oriented alternatives that create space for adaptive learning. This is not a call to abandon directiveness rather it is a call to deploy it deliberately, reserving it for situations that genuinely require it.
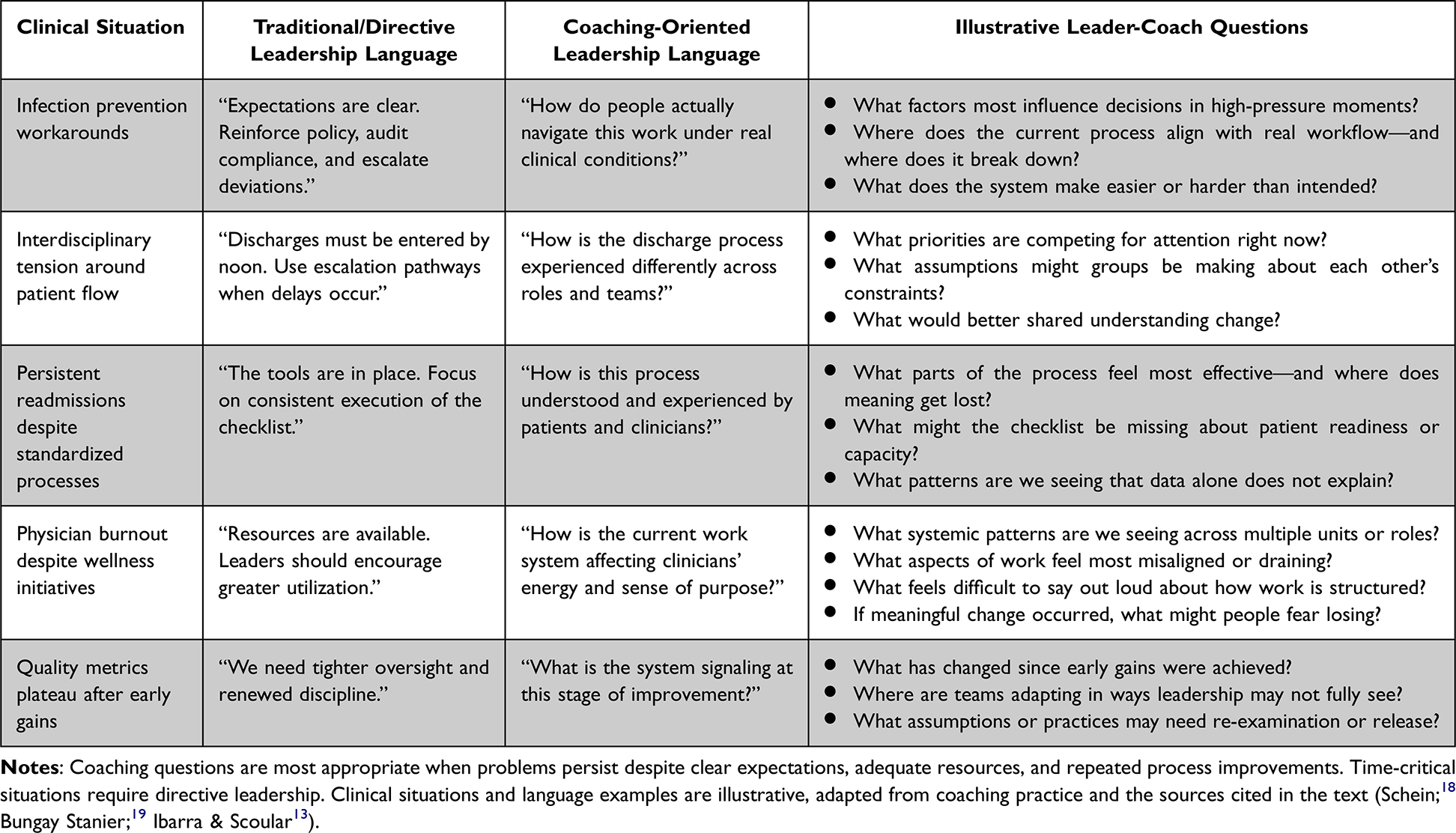 |
Table 1 From Directive to Coaching: A Shift in Leadership Language |
Organizational Listening
Organizational listening is frequently misunderstood. Surveys, town halls, and focus groups are useful tools—but they do not, by themselves, constitute organizational listening. Organizational listening is a leadership capability: the disciplined practice of noticing, interpreting, and acting on signals that emerge from across the system.12 These signals are often qualitative, early, and uncomfortable, surfacing through workarounds, hesitation, or silence rather than dashboards and formal reports.20
This capability requires judgment: attending to patterns that recur across settings and time; triangulating across multiple sources; and resisting the impulse to react to the loudest or most recent concern.12 Adaptive leaders listen not for isolated complaints, but for what those concerns reveal about underlying assumptions or misalignments in the system.
Multiple national bodies have converged on the same conclusion: collecting feedback without disciplined interpretation and visible response erodes trust, while organizational listening, understood as a leadership capability, is essential to safety, well-being, and sustained improvement.1,21–24 Listening conveys respect most powerfully when paired with transparent response: we heard; here is what we will do and what we will not do, and why.
Table 2 outlines common listening methods alongside the leadership capabilities required to transform each from a data-collection exercise into organizational insight.
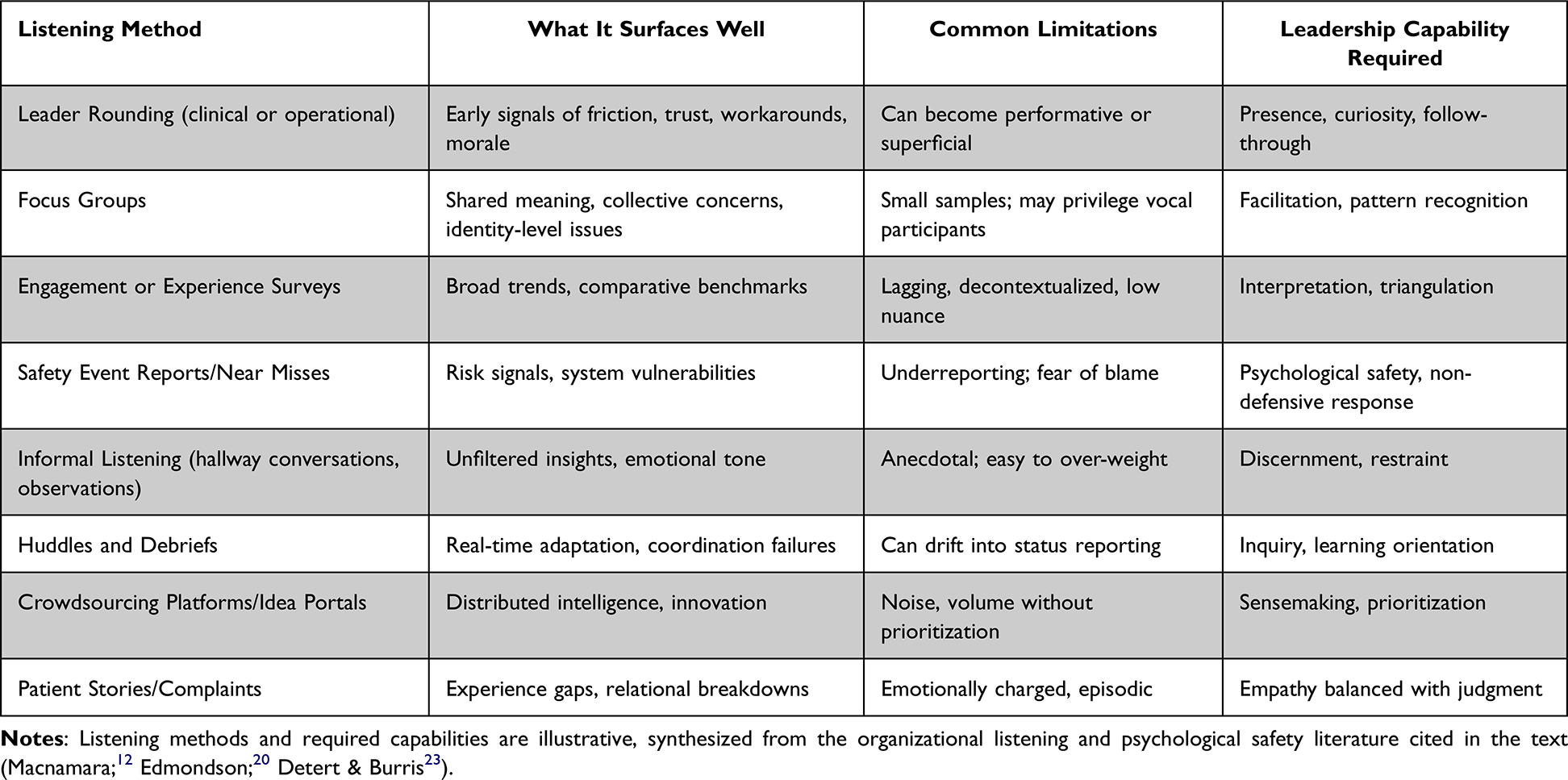 |
Table 2 From Listening Tools to Listening Capability: Required Leadership Practices |
Coaching Questions
Coaching questions operationalize the coaching stance and organizational listening.19 They are deliberately open-ended and non-directive—designed not to signal the right answer but to create space for reflection, surface assumptions, and deepen shared understanding. Effective coaching questions do not assign blame or rush toward resolution; they slow the conversation just enough to enable insight.
In practice, coaching questions shift attention from what should be done to how work is actually experienced across roles, pressures, and time:
What pressures are shaping decisions in this moment?
What feels hardest to let go of if we try something different?
What would success look like from another team’s perspective
What assumptions might we be making that deserve testing?
The goal is not consensus or immediate closure. It is to deepen understanding, strengthen collective judgment, and build the capacity to adapt by shifting attention from solving the current problem to developing the capability to solve the next one.
An ED wait time example illustrates the potential impact of coaching questions. A directive approach measures door-to-triage time, sets a five-minute target, monitors compliance, and escalates when nurses fall behind. Metrics improve. Wait times do not. Leadership initially interprets this as a staff compliance problem.
Coaching questions reframe it: What happens at triage when multiple ambulances arrive simultaneously? What trade-offs are nurses forced to make to meet the metric? How does the workaround play out downstream for patients and handoffs? These questions surface that nurses face an impossible choice between meeting the metric and completing thorough assessments—a system design problem invisible in the compliance data.
The problem was never staff behavior; it was surge capacity workflow. Coaching questions are, in this sense, a quality and safety tool. They surface what metrics miss.
Adaptive Change, Identity, and the Leader’s Role
The opening vignette of this perspective illustrates a broader pattern: adaptive change almost always involves loss—of familiar roles, professional autonomy, identity, or ways of working.2,25,26 Resistance in these situations is rarely about disagreement with the goal. It is more often about what must be relinquished to achieve it.
When leaders treat this resistance as a compliance problem, they escalate control often by tightening oversight, reinforcing mandates, doubling down on accountability. These responses may achieve short-term adherence while suppressing learning and deepening disengagement.
A coaching stance enables a different response. Rather than arguing for the change, leaders help teams surface what feels at risk, name what is being lost, and examine whether those losses are real, assumed, or negotiable. By acknowledging the identity dimensions of change, leaders create space for adaptation rather than forcing compliance. Adaptive leadership does not eliminate loss. It helps people work through it.
Building coaching into leadership is itself an adaptive challenge. Many clinical leaders move into leadership roles on the strength of their clinical performance and technical mastery, and are expected to already possess the core skills leadership requires, skills often quite different from the ones that earned them the role.27
The difficulty is not simply learning a new technique. Coaching asks leaders to lead in a way that can feel at odds with what made them successful as clinicians: drawing out others’ judgment rather than supplying the answer themselves.28 In Rooke’s framework of leadership development, this represents a shift from the expert action logic — which centers technical mastery and being the source of answers — toward higher-order action logics in which the leader’s effectiveness depends on developing capability in others.29,30 This capability must be deliberately developed; medical leaders are often left to acquire it on their own.
Alignment with Improvement Science
These principles are consistent with Lean as originally conceived—not primarily as a set of tools, but as a learning system grounded in humility, curiosity, and respect for people.14,31,32 The sensei role in Lean practice is instructive: the sensei does not solve problems for the organization but helps leaders and teams see more clearly, challenge assumptions, and build learning capability from the work itself. This is a coaching orientation, applied systematically.33
Research on relational coordination reinforces this framing. Organizations sustaining improvement demonstrate consistently higher relational coordination—characterized by frequent, timely, accurate communication and shared problem-solving.34 Virginia Mason Medical Center’s attribution of 75% of their improvement gains to cultural change rather than tools alone reflects the operationalization of exactly these behaviors.35
Practical Implications for Health System Leaders
If coaching and organizational listening are to function as leadership infrastructure, they cannot be reserved for senior leaders, remediation contexts, or high-potential development programs. The following framework—three core leadership behaviors and two organizational routines—offers a practical starting point that health systems can adopt regardless of size or current maturity.
Three Core Leadership Behaviors
- Coaching stance in daily interactions: Leaders at all levels shift from telling to asking when problems persist despite technical fixes. The questions in Table 1 serve as practical starting points, particularly at the moment when a leader’s instinct is to solve—because that is precisely when an adaptive problem is most likely to be missed.
- Organizational listening as discipline: Leaders distinguish signal from noise by attending to patterns across roles and time. The methods in Table 2 become useful when paired with visible, documented response: what was heard, what will change, and what will not change, and why.
- Acknowledging loss in change: Leaders explicitly name what is being relinquished—autonomy, professional identity, familiar ways of working—rather than treating resistance as disengagement. This requires leaders to hold the emotional dimensions of change alongside the operational ones.
Two Organizational Routines
- Assess leaders for learning, not just results: Performance reviews should include questions such as “How are you building your team’s capacity to adapt?” alongside “Did you meet targets?” This shifts accountability from outputs alone to the capability that produces sustainable outputs.
- Close the listening loop visibly: Document systematically what was heard, what will change as a result, and what will not change, and why. This transparency builds trust even when all requests cannot be accommodated—and signals that organizational listening is a practice, not a performance.
Boards and senior leaders accelerate this shift by asking not only “Are targets being met?” but “How is the organization learning?”—and by treating the second question as equally consequential.
Limitations and Future Directions
This perspective builds on and synthesizes existing evidence and proposes a practical framework for healthcare system leaders with real-world examples; it does not present primary outcome data. The empirical literature on coaching specifically as a leadership behavior in healthcare systems, as distinct from coaching as a professional service or wellness intervention, is still emerging, and the evidence base draws on adjacent constructs including psychological safety, relational coordination, and adaptive leadership research.2,15,16
At OU Health, an academic health system in Oklahoma, the framework described here is in early implementation within a broader organizational operating initiative. Elements under active development include coaching stance training for leaders, organizational listening infrastructure with closed-loop response protocols, and integration of coaching question frameworks into leadership development programming. Outcome data, including measures of psychological safety, improvement culture, and leadership effectiveness, will be reported in a subsequent publication.
Future research should examine which leadership behaviors and contextual factors most reliably enable the transition from directive to coaching-oriented leadership, particularly in academic health systems where professional hierarchy and identity are especially pronounced. Studies examining which populations of leaders respond most to coaching behavior development, and which organizational conditions enable or inhibit embedding, would substantially advance the field.
Conclusion
Healthcare does not lack improvement tools. What remains scarce is leadership capability matched to system complexity.
The next era of healthcare improvement will not fail for lack of methods. It will falter if leaders continue to rely on control when learning is required, or on efficiency when adaptation is needed. Coaching—understood as a leadership behavior and embedded as practice—enables organizational listening, adaptive learning, and the deliberate building of relational capacity. Listening is not a courtesy; it is a core operating capability. Coaching is not the soft edge of transformation. It is what allows improvement to endure.
Acknowledgments
The author used Claude (Anthropic) to assist with manuscript preparation. All intellectual content, clinical framework, and conclusions are the author’s own, and the author takes full responsibility for the final manuscript.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; has agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Funding
The author received no funding for this work.
Disclosure
The author reports no conflicts of interest.
References
1. Hilton K, Anderson A. IHI Pyschology of change framework to advance and sustain improvement. An IHI Resource. 2018
2. Heifetz RA. Leadership Without Easy Answers. Harvard University Press; 1994. doi:10.4159/9780674038479
3. Edmondson A. Psychological safety and learning behavior in work teams. Administ Sci Quart. 1999;44(2):350–10. doi:10.2307/2666999
4. Center for creative leadership: how to have a coaching conversation. Center for Creative Leadership; 2025. Available from: https://www.ccl.org/articles/leading-effectively-articles/how-to-have-a-coaching-conversation/.
5. Martin W, Heroman M. The evidence and impact of coaching: focusing on physician leadership coaching for improved outcomes. HALMJ. 2025;3(5):249–252. doi:10.55834/halmj.2432524134
6. Athanasopoulou A, Dopson S. A systematic review of executive coaching outcomes: is it the journey or the destination that matters the most? The Leadership Quarterly. 2018;29(1):70–88. doi:10.1016/j.leaqua.2017.11.004
7. Day FJ. How the “Health Leader-as-Coach” benefits health leaders, their teams, peers, organisation and the system. BMJ Lead. 2025;9(1):11–15. doi:10.1136/leader-2023-000870
8. Quiroga A, Lee TH. Why clinicians hold the key to fixing health care’s complexity problem. NEJM Catalyst. 2025;7(1). doi:10.1056/CAT.25.0310
9. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360(5):491–499. doi:10.1056/NEJMsa0810119
10. Snowden DJ, Boone ME. A leader’s framework for decision making. Harvard Business Review. Available from: https://hbr.org/2007/11/a-leaders-framework-for-decision-making.
11. Petropanagos A, Oliver J, Chidwick P. How adaptive leadership can enhance healthcare ethics. Healthc Manage Forum. 2025;38(4):290–294. doi:10.1177/08404704251327667
12. Macnamara J. Toward a Theory and practice of organizational listening. Int J Listen. 2018;32(1):1–23. doi:10.1080/10904018.2017.1375076
13. Ibarra H, Scoular A. The leader as coach. Harvard Business Review. Available from: https://hbr.org/2019/11/the-leader-as-coach.
14. Spear SJ. Learning to lead at Toyota. Harv Bus Rev. 2004;82(5):78–86,151.
15. Gazelle G, Liebschutz JM, Riess H. Physician burnout: coaching a way out. J Gen Intern Med. 2015;30(4):508–513. doi:10.1007/s11606-014-3144-y
16. Boet S, Etherington C, Dion PM, et al. Impact of coaching on physician wellness: a systematic review. Lau Y ed. PLoS One. 2023;18(2):e0281406. doi:10.1371/journal.pone.0281406
17. Passarelli AM, Gazelle G, Schwab LE, et al. Competencies for those who coach physicians: a Modified Delphi Study. Mayo Clinic Proceedings. 2024;99(5):782–794. doi:10.1016/j.mayocp.2024.01.002
18. Schein EH. Humble Inquiry: The Gentle Art of Asking Instead of Telling. Berrett-Koehler Publishers; 2013.
19. Bungay Stanier M. The Coaching Habit: Say Less, Ask More & Change the Way You Lead Forever. Box of Crayons Press; 2016.
20. Edmondson AC. The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and Growth. Wiley; 2019.
21. Agency for Healthcare Reseach and Quality. Hospital Survey on Patient Safety Culture. 2019. Available from: https://ahrq.gov/sops/surveys/hospital/index.html.
22. Committee on Systems Approaches to Improve Patient Care by Supporting Clinician Well-Being, National Academy of Medicine, National Academies of Sciences, Engineering, and Medicine. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. National Academies Press; 2019:25521. doi:10.17226/25521
23. Detert JR, Burris ER. Leadership behavior and employee voice: is the door really open? AMJ. 2007;50(4):869–884. doi:10.5465/amj.2007.26279183
24. A framework for safe, reliable, and effective care. IHI white paper. Institute for Healthcare Improvement; 2017.
25. Kegan R, Lahey LL. Immunity to Change: How to Overcome It and Unlock the Potential in Yourself and Your Organization. Harvard Business School Publishing Corporation; 2009.
26. Risse M. The moral architecture of adaptive leadership. SSRN. 2026. doi:10.2139/ssrn.6278081
27. Sullivan EE, Stephenson AL, Hoffman AR. Engaging physicians in leadership: motivations, challenges, and identity-based considerations. J Healthc Manage. 2022;67(4):254–265. doi:10.1097/JHM-D-21-00224
28. Huikko-Tarvainen S, Sajasalo P, Auvinen T. Just a leader? Leadership work challenges and identity contradiction experienced by Finnish physician leaders. JHOM. 2021;35(9):195–210. doi:10.1108/JHOM-10-2020-0421
29. Rooke D, Torbert WR. 7 transformations of leadership. Harv Bus Rev. 2005;83(4):66–76,133.
30. Rooke D. Transformational leadership capabilities for medical leaders. leader. 2018;2(1):3–6. doi:10.1136/leader-2017-000041
31. Toussaint JS, Berry LL. The promise of lean in health care. Mayo Clin Proc. 2013;88(1):74–82. doi:10.1016/j.mayocp.2012.07.025
32. Spear S. Learning from Toyota’s Stumble. Harvard Business Review. https://hbr.org/2010/01/learning-from-toyotas-stumble.
33. Rother M. Toyota Kata: Managing People for Improvement, Adaptiveness, and Superior Results. McGraw Hill Education; 2010.
34. Gittell JH, Godfrey M, Thistlethwaite J. Interprofessional collaborative practice and relational coordination: improving healthcare through relationships. J Interprof Care. 2013;27(3):210–213. doi:10.3109/13561820.2012.730564
35. Kenney C. Transforming Health Care; Virginia Mason Medical Center’s Pursuit of the Perfect Patient Experience. Productivity Press; 2010.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.