Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
CO2 Laser Resection of Giant Rhinophyma Under Local Anesthesia: A Case Report
Authors Zhao QK
Received 5 February 2026
Accepted for publication 19 March 2026
Published 26 March 2026 Volume 2026:19 597723
DOI https://doi.org/10.2147/CCID.S597723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Qian-Kun Zhao
Department of Dermatology and Aesthetic Plastic Surgery, Xi’an No.3 Hospital, Xi’an, Shaanxi 710018, People’s Republic of China
Correspondence: Qian-Kun Zhao, Email [email protected]
Introduction and Importance: Phymatous rosacea (PhR), also known as “rhinophyma”, refers to a benign condition characterized by the excessive proliferation of sebaceous glands and fibrosis in the facial skin due to rosacea, leading to thickening and hardening of the nasal skin, ultimately developing into rhinophyma. This disease’s pathophysiology remains unclear but is seen as an advanced stage of rosacea.
Presentation of Case: The patient is a 67-year-old male and has hypertrophy of nasal tip and an enlarged nodule measuring approximately 7 cm × 6.1 cm × 4.5 cm in size of dark red color, uneven surface, clear dilation of follicular orifices, presence of white pustules and yellowish-white comedone-like secretions on light touch. Compression causes deformity of the nostrils that influences the quality of life and breathing. A total excision of the rhinophyma under local anesthesia by means of the CO2 laser surgery was agreed upon. The dressing changes were used to treat the wound after surgery and full healing took place after 30 days. The patient had satisfactory results, both in a functional and aesthetic sense, with the result having no recurrence in 1 year after surgery.
Clinical Discussion: The CO2 laser therapy with local anesthesia is an extension of traditional general anesthesia surgery when it comes to the removal of rhinophyma because it is easy to perform the surgery, with minimal trauma, bleeding, and no follow-up surgical operation, which leads to the development of a personal approach to the treatment. In our case, reconstructing the nasal area is complicated by the decision on anesthesia and management of nasal wound, which does not interfere with its functionality and beauty.
Conclusion: In this report, we emphasize the surgical value of local anesthesia with CO2 laser for rhinophyma, reducing blood loss, operation time, and the need for secondary surgery. Follow-up for 1 year.
Plain Language Summary: ① We report a case of giant rhinophyma treatment, supplementing clinical data for this type of disease; ② We propose performing the surgery under local anesthesia, which shortens the operation time and hospitalization time compared to traditional general anesthesia; ③ The clinical practicality of CO2 laser in the treatment of rhinophyma is provided as a reference.
Keywords: rosacea, rhinophyma, local anesthesia, CO2 laser
Introduction
PhR, also known as “rhinophyma”, refers to a disease caused by the excessive proliferation of sebaceous glands and fibrosis in the face due to rosacea, leading to thickening and hardening of the nasal skin, developing into rhinophyma. From a histopathological perspective, rhinovegetation is characterized by hypertrophic sebaceous glands, a fibrovascular mucinous matrix, and dermal lymphocyte infiltration.1 In advanced cases, fibrosis may destroy sebaceous glands,2 though the exact etiology and pathogenesis remain unclear.3 Rhinophyma is more common in elderly males4 and is one of the most severe manifestations of rosacea. The large mass of rhinophyma can cause collapse of the external nasal valve, affecting the patient’s normal breathing and eating, reducing the patient’s quality of life,5 and having a significant negative impact on mental health, especially in social aspects.6,7 Early-stage rosacea can be treated with CO2 fractional laser, while surgical treatment is the preferred method for rhinophyma once the condition progresses.7,8 Depending on the state of the patient and the dimensions of the rhinophyma, the selection of a method to be applied surgically can be fully understandable, and some of the most frequently used procedures, such as excision, ablation, laser techniques, and their combinations, may be used.6 In this case, we provide an account of a successful surgical procedure that utilizes local anesthesia to excise the rhinophyma of a 67-year-old male patient, since the rhinophyma was penetrating into the patient’s breathing, eating, and social interactions. It is an article that includes a case (written following the Surgical Case Report (SCARE) guidelines).
Patient Information
The patient, a 67-year-old male, reported having a rhinophyma as a result of rosacea over the past 12 years. According to the patient, 12 years ago, The patient had a history of hypertension. He had continuous localized redness in the nasal region with telangiectasia, followed by a pustule, which could resolve after self-extraction. The skin became thickened with increased follicular orifices, to varying degrees after subsiding. He had already visited a local hospital, where he was diagnosed with rosacea but was not treated regularly. Five years ago, the nasal tip began to grow slowly outward without pain and was not treated. In the past year, the nasal growth enlarged to affect breathing, eating, and normal social interactions, leading to a clinic visit on July 1, 2024, with an outpatient diagnosis of “PhR” (See Table 1).
 |
Table 1 The Duration of Disease Progression, Any Previous Treatments, Relevant Comorbidities |
Clinical Findings
Nasal tip growth, measuring approximately 7 cm × 6.1 cm × 4.5 cm, with a dark red color, uneven surface, obvious dilation of follicular orifices, visible white pustules, and yellowish-white comedone-like secretions upon light touch. The nostrils are deformed due to compression, but the patient did not experience pain. Based on these prior findings, the patient had to undergo surgical excision of the mass (See Figure 1).
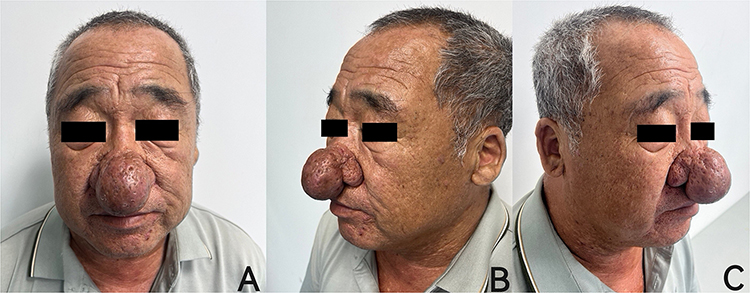 |
Figure 1 (A) Preoperative anteroposterior view; (B) Preoperative left lateral view; (C) Preoperative right lateral view. |
Diagnostic Assessment
Diagnosis: Medical history and clinical presentation: Giant nasal tip growth, compressed and deformed nasal apertures, thickened nasal skin, uneven surface, extremely dilated sebaceous gland openings, excessive secretion, shiny oily surface, dark red color, gradually formed on the basis of long-term rosacea (nasal flushing, erythema, telangiectasia, papulopustules), commonly seen in elderly males. Differential diagnosis: Basal cell carcinoma: Especially the nodular ulcerative type, which may be misdiagnosed. Cancer typically presents as an ulcer with rolled edges, growing differently. Sarcoidosis: A systemic granulomatous disease that can sometimes affect the nasal skin. Lymphoma: Cutaneous lymphoma may present as nodules and swelling.
Therapeutic Intervention
The surgery was performed under local anesthesia, using a CO2 laser for layer-by-layer excision: Preoperatively, the surgical excision range was designed with reference to the normal tissue plane and marked with a marking pen. The local anesthetic was prepared as follows: 10 mL of lidocaine (1%~2%) mixed with 0.1 mg of epinephrine (1:1000 concentration), resulting in a final epinephrine concentration of 1:100,000~1:200,000. The patient was in a supine position, and after routine povidone-iodine disinfection, local infiltrative anesthesia was administered according to the surgical area. Anesthetic was supplemented in a timely manner based on the patient’s pain response. After the drug took effect, the CO2 laser was used for layer-by-layer excision of the proliferative mass, with the Lumenis CO2 laser set to continuous pulse mode, power adjusted to 5–8 W depending on the depth of the wound, cutting to a level about 1 mm below the surrounding normal tissue. The wound was covered with one layer of sterile paraffin gauze, one layer of saline gauze, and three layers of sterile dry gauze for bandaging. The patient did not experience significant pain 1–2 hours postoperatively, with good intraoperative anesthesia effect and long postoperative analgesia duration. Through careful planning and execution, the team successfully achieved the excision of the nasal tumor, The patient declined histopathological examination during treatment. With the surgical area dressing changed daily with sterile gauze, and the surgical team meticulously managed the postoperative wound, resulting in complete wound healing after 30 days (See Figure 2).
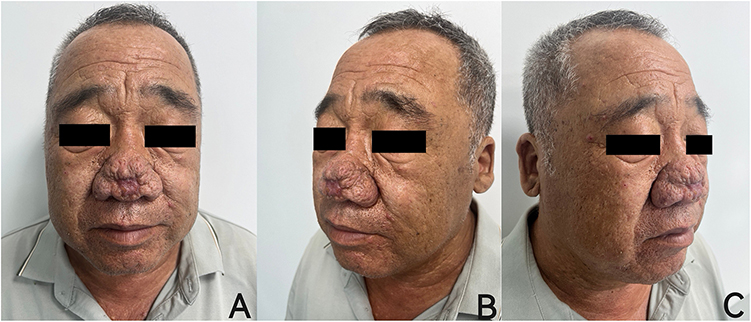 |
Figure 2 (A) Postoperative anteroposterior view; (B) Postoperative left lateral view; (C) Postoperative right lateral view. |
Follow-Up and Outcomes
Follow-up for 1 year. No local recurrence was observed, no scar hypertrophy, and the patient was satisfied with the nasal appearance. Achieved good cosmetic and functional results.
Discussion
Compared to other nasal masses, PhR is a benign and non-invasive tumor. In 2017, the Global Rosacea Consensus Expert Panel (ROSCO) proposed a classification system with six major phenotypes centered on “flushing”, “persistent erythema”, “telangiectasia”, “papules/pustules”, “phymatous changes”, and “ocular manifestations”.9 There is no specific immunological diagnosis for rhinophyma. Therefore, the diagnosis of rhinophyma is usually clinical,10 and it typically occurs in elderly patients, with a significant male predominance.4,8 If there are underlying diseases such as heart disease, emphysema, renal insufficiency, or cirrhotic ascites, these are contraindications for general anesthesia. Local anesthesia can broaden the surgical indications11 and can be performed in an outpatient surgical setting. Postoperatively, patients can resume normal activities, which aids recovery and avoids complications associated with traditional anesthesia, such as aspiration pneumonia and lower limb venous thrombosis, with minimal impact on elderly bodies and low treatment costs. This case involves a 67-year-old male patient with a history of hypertension, presenting with giant rhinophyma causing nasal aperture deformity, compressing the upper lip, and affecting normal breathing. Intubation under general anesthesia was not conducive to the surgical operation, so local anesthesia was chosen for the direct excision of the hypertrophic rhinophyma tissue, reducing the patient’s general anesthesia surgical risks, with satisfactory effects in the operative procedure and anesthesia time.
PhR also lacks a standardized treatment protocol. Multiple studies recommend surgical excision as treatment.7,8 The traditional surgical method involves excising the lesional tissue, followed by skin grafts or flaps. However, skin grafts have a high postoperative contracture rate, and flap repairs require multiple surgeries for reshaping.10 The skin in the PhR is subject to long-term chronic infection, and direct grafting or flap transplantation on infected wounds carries a high postoperative infection risk and may also alter the nasal skin color and texture. Dermabrasion has poor hemostatic effects, while electrosurgery risks cartilage necrosis or imprecise resection depth.6 Given the patient’s preference for outpatient treatment, refusal of hospitalization, and the history of hypertension, We adopted a personalized surgical plan for the patient,9 using the CO2 laser for direct excision combined with moist dressing and bandaging treatment, achieving good therapeutic results.6 This method has advantages such as simple operation, minimal trauma, less bleeding, and no need for secondary surgery,3,12–14 There is a risk of post-surgical pigmentation or scarring. Intraoperative excision of lesional tissue should not be excessive.3 If excision reaches the cartilage layer of the nasal wing, the wound cannot heal through epithelialization and requires flap transfer for repair or the use of expensive artificial materials to cover the wound.15 Careful preoperative patient assessment, accurate intraoperative surgical techniques, and appropriate postoperative care can reduce the risk of complications after rhinophyma surgery. Postoperative moist dressing changes without pressure bandaging led to wound healing after 30 days of routine dressing changes. The patient’s nasal appearance and quality of life improved markedly, with high satisfaction and no complications or cosmetic issues after one year of follow-up.
Conclusion
In this report, we emphasize the surgical value of local anesthesia with CO2 laser for rhinophyma, reducing blood loss, operation time, and the need for secondary surgery. We will conduct long-term follow-up on the patient, but single-case studies on rhinovegetation have limitations. Future comparative studies will be conducted to enhance the scientific rigor and balance of the research.
Artificial Intelligence Usage Statement
No AI tools were involved.
Ethics Statement
The studies involving humans were approved by Ethics Committee of Xi’an No.3 Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent was obtained from the patient for the publication of the case details and accompanying images. Institutional approval is not required for publication of this case study.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Weber L, Thaller SR, Kassira WM. Rhinophyma: diagnosis and management. In: Thaller SR, Cohen MN, editors. A Comprehensive Guide to Male Aesthetic and Reconstructive Plastic Surgery. Cham: Springer International Publishing; 2024:567–5.
2. Plewig G, Melnik B, Chen W. Rosacea clinic and classification. In: Plewig and Kligman’s Acne and Rosacea. Cham: Springer International Publishing; 2019:517–557.
3. Nganzeu CG, Lopez A, Brennan TE. Ablative CO2 laser treatment of rhinophyma in people of color: a case series. Plast Reconstr Surg Glob Open. 2025;13(3):e6616. PMID: 40061169; PMCID: PMC11888977. doi:10.1097/GOX.0000000000006616
4. Ismail D, Asfour L, Madan V. Rhinophyma in women: a case series. Lasers Med Sci. 2021;36:1283–1287. doi:10.1007/s10103-020-03183-z
5. van Zuuren EJ. Rosacea. N Engl J Med. 2017;377(18):1754–1764. doi:10.1056/NEJMcp1506630
6. Benyo S, Saadi RA, Walen S, Lighthall JG. A systematic review of surgical techniques for management of severe rhinophyma. Craniomaxillofac Trauma Reconstr. 2021;14(4):299–307. doi:10.1177/1943387520983117
7. Dick MK, Patel BC. Rhinophyma. [Updated August 8, 2023]. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544373/.
8. Faenza M, Molle M, Ronchi A, et al. Multiple Foci of Basal cell carcinoma arising in rhinophyma: a case report and literature review. JPRAS Open. 2023;38:186–192. doi:10.1016/j.jpra.2023.10.001
9. Tan J, M AL, Bewley A, et al. Updating the diagnosis,classification and assessment of rosacea:recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017;176(2):431–438. doi:10.1111/bjd.15122
10. Ezra N, Greco JF, Haley JC, Chiu MW. Gnathophyma and otophyma. J Cutan Med Surg. 2009;13(5):266–272. doi:10.2310/7750.2008.08051
11. Balentine CJ, Meier J, Berger M, et al. Using local anesthesia for inguinal hernia repair reduces complications in older patients. J Surg Res. 2021;258:64–72. doi:10.1016/J.JSS.2020.08.054
12. Barolet AC, Barolet D. Fully ablative CO2 laser therapy for rhinophyma: long-term efficacy, safety and insights from an artificial intelligence-assisted predictive model in a large cohort. Skin Health Dis. 2025;5(5):357–367. doi:10.1093/skinhd/vzaf042
13. Volk K, Ulfers A, Yi RC, Feldman S, Taylor SL. Treatment management for rosacea: current pharmacological and non-pharmacological options. Expert Rev Clin Pharmacol. 2025;18(8):589–605. PMID: 40836652. doi:10.1080/17512433.2025.2550727
14. Kishchuk V, Bartsikhovskyi A, Isnyuk A, et al. Rhinophyma. Clinical course and the step-by-step treatment modern reviews. Surgical treatment methods efficiency comparison (bibliographic review, own experience). Sci Collection «interconf+». 2025;59(256):210–230.
15. Plewig G, Kligman AM, Jansen T. Acne and Rosacea. Springer; 2011:758.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.