Back to Journals » Drug Design, Development and Therapy » Volume 19
Clozapine Drug–Drug Interactions and Individualized Dosing in Bipolar Disorder: A Model-Informed Precision Dosing Approach
Authors Zhang Y, Wang J, Tian X, Zhang YJ, Li Y, He SM, Zhang C, Chen X, Wang DD ![]()
Received 1 August 2025
Accepted for publication 6 November 2025
Published 14 November 2025 Volume 2025:19 Pages 10119—10134
DOI https://doi.org/10.2147/DDDT.S557624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Yue Zhang,1,* Jie Wang,1,* Xue Tian,1,* Yi-Jia Zhang,1,* Ye Li,1,* Su-Mei He,2 Cun Zhang,3 Xiao Chen,4 Dong-Dong Wang1
1Jiangsu Key Laboratory of New Drug Research and Clinical Pharmacy and School of Pharmacy, Xuzhou Medical University, Xuzhou, Jiangsu, 221004, People’s Republic of China; 2Department of Pharmacy, Suzhou Research Center of Medical School, Suzhou Hospital, Affiliated Hospital of Medical School, Nanjing University, Suzhou, Jiangsu, 215153, People’s Republic of China; 3Department of Pharmacy, Xuzhou Oriental Hospital Affiliated to Xuzhou Medical University, Xuzhou, Jiangsu, 221004, People’s Republic of China; 4School of Nursing, Xuzhou Medical University, Xuzhou, Jiangsu, 221004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Su-Mei He, Department of Pharmacy, Suzhou Research Center of Medical School, Suzhou Hospital, Affiliated Hospital of Medical School, Nanjing University, Suzhou, Jiangsu, 215153, People’s Republic of China, Email [email protected] Dong-Dong Wang, Jiangsu Key Laboratory of New Drug Research and Clinical Pharmacy and School of Pharmacy, Xuzhou Medical University, Xuzhou, Jiangsu, 221004, People’s Republic of China, Email [email protected]
Objective: Clozapine is an effective treatment for bipolar disorder (BD), but its clinical use is complicated by drug–drug interactions (DDI), which may reduce efficacy or increase toxicity. This study aims to explore clozapine DDI and its individualized administration regimens for patients with BD based on model-informed precision dosing (MIPD) technology, and achieve clinical precision medication.
Methods: Data are collected from 51 patients with BD treated with clozapine, including all concomitant medications used in clinical practice. The MIPD technique is used to explore the potential DDI, and the Monte Carlo simulation is adopted to recommend the optimal administration regimen.
Results: It is ultimately found that zopiclone, zolpidem tartrate with clozapine have DDI. When patients with BD have no combined medication of zopiclone or zolpidem tartrate, the recommended doses of clozapine for patients at 40– 45 kg, 45– 60 kg, 60– 78 kg, 78– 106 kg, and 106– 120 kg are 10 mg/kg/day, 9 mg/kg/day, 8 mg/kg/day, 7 mg/kg/day, and 6 mg/kg/day, respectively. When patients with BD are combined with zopiclone, the recommended doses of clozapine for patients at 40– 60 kg and 60– 120 kg are 4 mg/kg/day and 3 mg/kg/day, respectively. When patients with BD are combined with zolpidem tartrate, the recommended doses of clozapine for patients at 40– 52 kg and 52– 120 kg are 5 mg/kg/day and 4 mg/kg/day, respectively.
Conclusion: This study explores the DDI of clozapine in patients with BD based on MIPD, and recommends the individualized dosing regimen of clozapine in patients with BD according to concomitant medication. These findings provide weight- and drug-specific dosing recommendations that may improve the safety and efficacy of clozapine in BD patients.
Keywords: clozapine, bipolar disorder, drug–drug interactions, zopiclone, zolpidem tartrate
Introduction
Bipolar disorder (BD) is a mental illness characterized by alternating episodes of mania (or hypomania) and depression. It is a highly recurrent and complex condition with diverse clinical manifestations. During the manic phase, individuals experience elevated mood, rapid thinking, increased activity, along with grandiose delusions, impulsive behaviors, or reduced need for sleep. In the depressive phase, symptoms include low mood, loss of interest, decreased energy, and in severe cases, suicidal tendencies.1–5 In terms of etiology, BD involves the interaction of multiple factors, mainly including genetic factors, neurobiological mechanisms, environmental and psychological factors, biological rhythm disorders, metabolic abnormalities, etc.6–10 According to data from the World Health Organization (WHO), the overall global incidence rate of BD has reached 2.4%.11 With the development of modern society, BD is showing an increasing trend.
The treatment methods for BD mainly include lifestyle adjustment, physical therapy, psychological therapy, drug therapy, etc, among which drug therapy is the main treatment method for BD.12,13 Clozapine is a dibenzodiazepine class. It has a strong blocking effect on the 5-hydroxytryptamine (5-HT2A) receptor and dopamine (DA1) receptor in the brain, and also has a blocking effect on the dopamine (DA4) receptor, but a weak blocking effect on the dopamine (DA2) receptor. In addition, it has anti-choline (M1), anti-histamine (H1) and anti-A-adrenergic receptor effects. Extrapyramidal reaction and delayed dyskinesia are mild, generally do not cause elevated prolactin in the blood, can directly inhibit the ascending activation system of the brainstem reticular structure, have a powerful sedative-hypnotic effect, indications include schizophrenia and bipolar disorder, including refractory schizophrenia that is ineffective to conventional antipsychotic drugs, additionally it significantly improves positive symptoms (such as hallucinations and delusions) and some negative symptoms (such as apainess), and can reduce the risk of suicide for patients with BD.14–18 More and more evidences indicate that clozapine can benefit patients with BD, especially for treatment-resistant cases or severe mood instability, and the frequency of its use in patients with BD is gradually increasing.19–24
However, clozapine has significant pharmacokinetic differences and large variations among individuals, making it difficult to treat an appropriate dose of clozapine. Clozapine is mainly metabolized by cytochrome P450 (CYP) enzymes in liver cells, among them CYP1A2 and CYP3A4 are the main metabolic enzymes, leading to an increased likelihood of CYP enzyme-mediated drug–drug interactions (DDI). A lower clozapine concentration can affect the efficacy of the drug, while a higher concentration often increases the risk of toxicity. Common adverse reactions of clozapine include weight gain, elevated fasting blood glucose, dyslipidemia, epileptic seizures, neutropenia, myocarditis, and pneumonia, etc, and therapeutic drug monitoring (TDM) is often used to detect the concentration of clozapine to formulate an appropriate dosing plan for the next dose of clozapine, clinically.25–30 However, since there is no reference TDM concentration when the first dose of clozapine is administered, it brings difficulties to the clinical individualized use of clozapine. Especially when there is potential DDI, it further increases the difficulty of individualized administration of clozapine in patients with BD. Thus, this study aims to explore clozapine DDI and its individualized administration regimens for patients with BD based on model-informed precision dosing (MIPD) technology, and achieve clinical precision medication.
Methods
Enrolled Patients
The BD patients included in this study are retrospectively collected from Xuzhou Oriental Hospital Affiliated to Xuzhou Medical University between July 2020 and January 2025 in electronic medical record, which is approved by the Research Ethics Committee of Xuzhou Oriental Hospital Affiliated to Xuzhou Medical University, where the requirement for written informed consent could be waived since the data are collected retrospectively without patient identifiers. This study adheres to the Declaration of Helsinki. Inclusion criteria: (1) BD patients, (2) clozapine treatment, (3) TDM for clozapine. Exclusion criteria: BD patients with missing clinical medical record data. The data included in this study mainly consist of the patients’ basic indicators, clinical test results, and medication information, etc.
Modeling
This study utilizes one of the main tools of MIPD, namely population pharmacokinetics (PPK) with non-linear mixed effect modeling (NONMEM, version 7, ICON Development Solutions, Ellicott City, MD, USA) software, to investigate the DDI of clozapine in patients with BD. Given trough concentration, we research the absorption phase with a one‐compartment model. During the modeling process, the main parameters included are CL/F, V/F, and Ka, where Ka is fixed at 1.3/h.31,32
Inter-individual variability is shown in Formula (a):

Ai is individual parameter. TV(A) is typical individual parameter. ηi is symmetrical distribution.
Random residual variability is shown in Formula (b):

Bi is observed concentration. Ci is individual predicted concentration. ε1 is symmetrical distribution.
Relationship between parameters and weight is shown in Formula (c):

Di is i-th individual parameter. Ei is i-th individual weight. Estd is standard weight of 70 kg and Dstd is typical individual parameter. F is the allometric coefficient: 0.75 for the CL/F and 1 for the V/F.33
Continuous or categorical covariates parameters are shown in Formulas (d) and (e), respectively:


Gi is individual parameter. TV(G) is typical individual parameter. Z is parameter to be estimated. Hi is covariate of the i-th individual. Hm is population median for the covariate.
Two-step method is used for constructing covariate model. Constructing covariate model uses two-step method. The objective function value (OFV) are decreased more than 3.84 (P<0.05) and increased more than 6.63 (P<0.01), being deemed to the inclusion and exclusion standard, respectively.
Model Evaluation
Observations vs population predictions, observations vs individual predictions, conditional weighted residuals (WRES) vs population predictions, conditional WRES vs time, observations/Predictions vs time, density vs weighted residuals, quantiles of weighted residuals vs quantiles of normal, visual predictive check (VPC) of model are used to evaluate the final clozapine PPK model in BD patients. In addition, bootstrap way is used to repeated random sampling with replacement from the raw data base with 1,000 repetitions with different random sampling. The medians and 2.5th–97.5th percentiles of the results from bootstrap are used for comparing with final model parameters.
Simulation
Monte Carlo simulation (number of interactions is 1000) is adopted to recommend the optimal administration regimen. The simulation scenarios are divided into three types: (i) Patients with BD who are not combined with zopiclone or zolpidem tartrate. (ii) Patients with BD who are combined with zopiclone. (iii) Patients with BD who are combined with zolpidem tartrate. Every type is simulated with 1000 virtual BD patients using 5 weight groups (40, 60, 80, 100, 120 kg) and 10 dose groups (1, 2, 3, 4, 5, 6, 7, 8, 9, 10 mg/kg/day), respectively. The therapeutic window is 350–800 ng/mL, and the toxicity threshold is set at 1000 ng/mL.34–37
Results
Patient Information
Fifty-one BD patients are included to analyze, among which 21 men and 30 women, aged 21.04–70.12 years old, and weighted 45.00–108.00 kg. Demographic data of BD patients and concomitant medication information are shown in Tables 1 and 2, respectively. Drug combination in BD patients include acarbose capsule, alprazolam tablet, amisulpride tablet, aripiprazole orally disintegrating tablet, aripiprazole tablet, atorvastatin calcium tablet, buspirone hydrochloride tablet, clonazepam tablet, diazepam injection, enteric-coated aspirin tablet, haloperidol injection, lamotrigine tablet, lithium carbonate extended-release tablet, lithium carbonate tablet, lorazepam tablet, magnesium valproate sustained-release tablet, metformin hydrochloride tablet, metoprolol succinate extended-release tablet, omeprazole enteric-coated capsule, perospirone hydrochloride tablet, phenhyxol hydrochloride tablet, propranolol hydrochloride tablet, risperidone tablet, sodium valproate sustained-release tablet, sodium valproate tablet, zolpidem tartrate, zopiclone tablet.
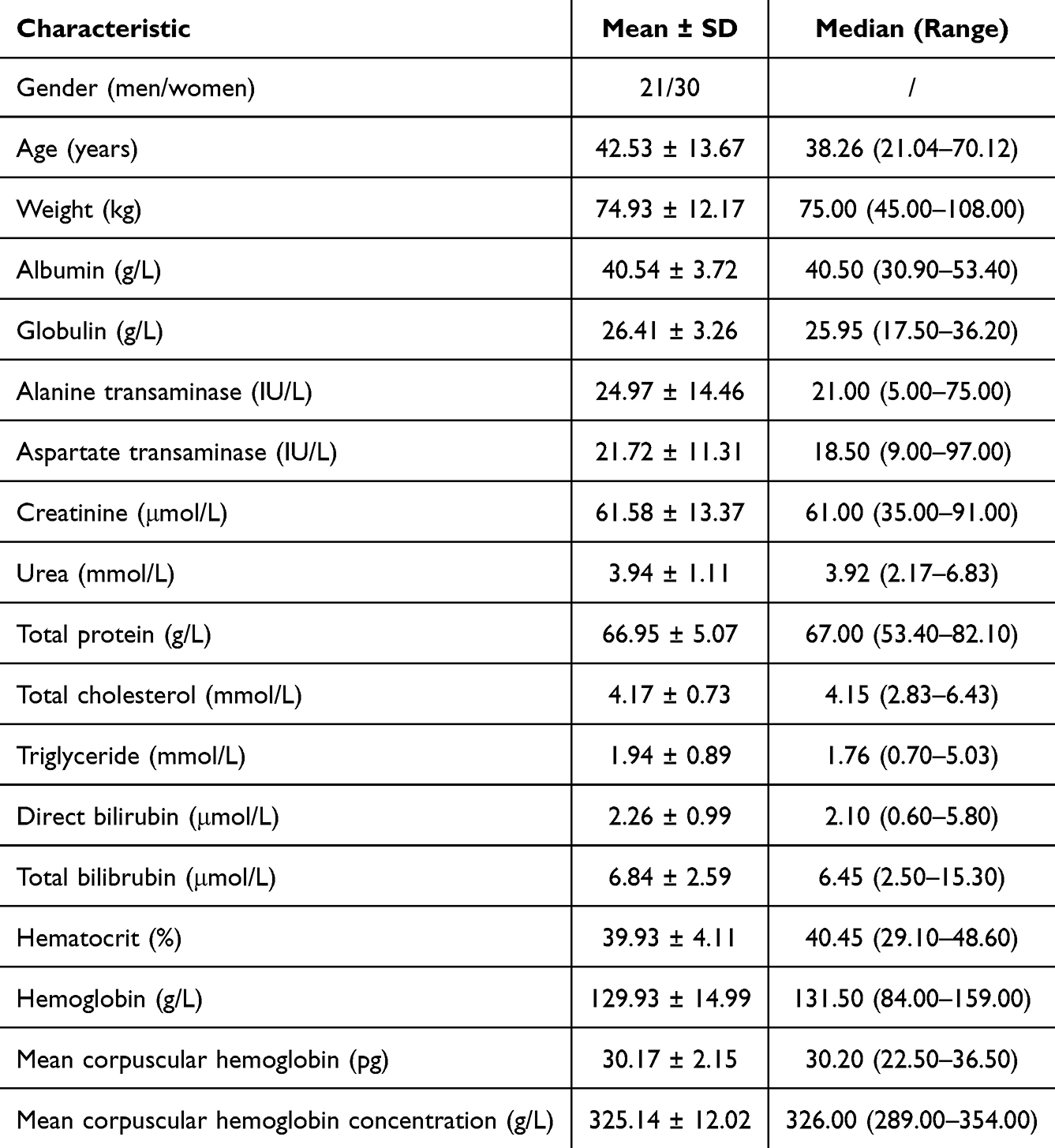 |
Table 1 Demographic Data of Bipolar Disorder Patients with Clozapine (n = 51) |
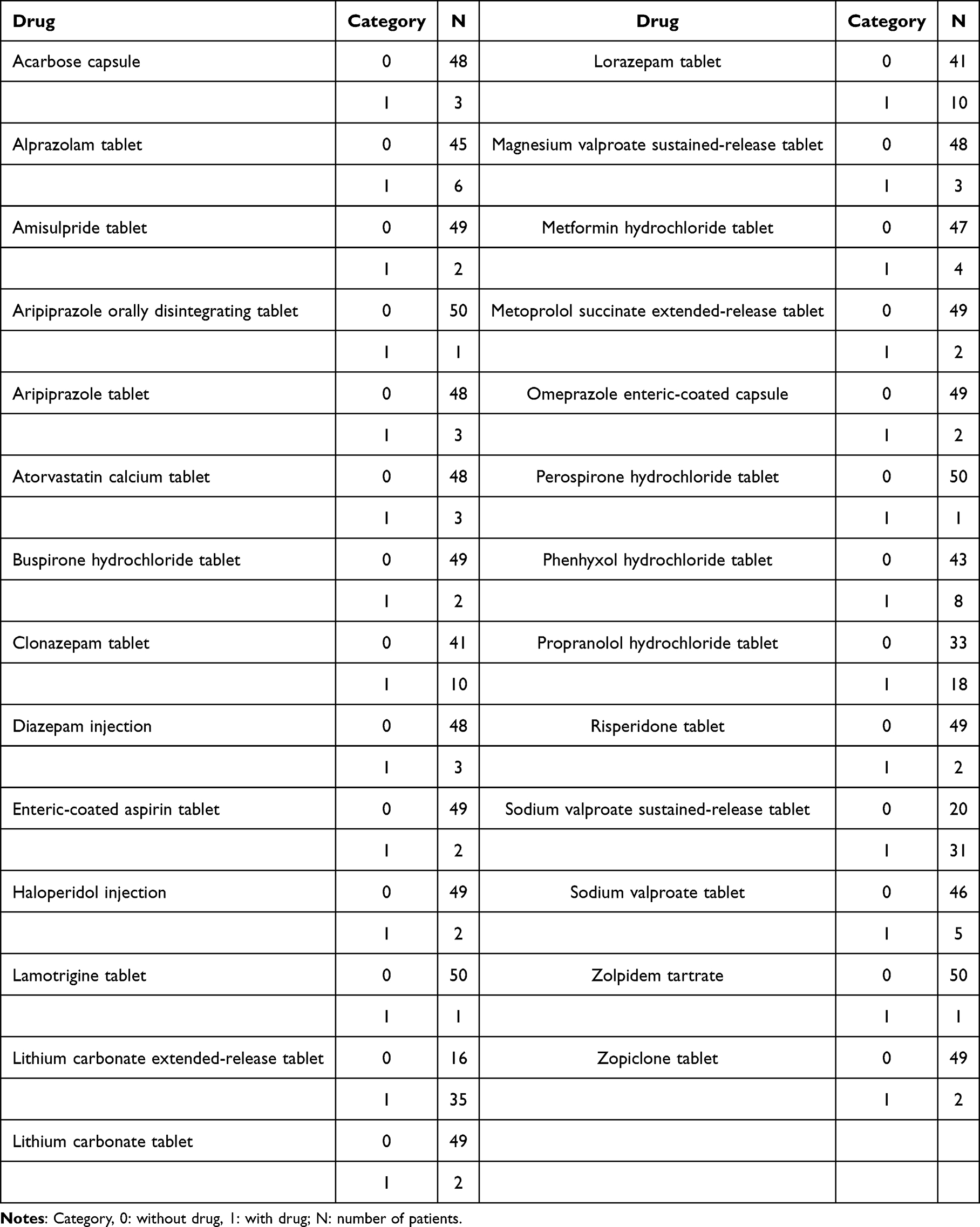 |
Table 2 Drug Combination in Bipolar Disorder Patients with Clozapine (n = 51) |
Modeling
In the final result, zopiclone, zolpidem tartrate with clozapine have DDI. Final clozapine MIPD model in BD patients is shown in Formulas (f) and (g):


ZOP, ZOL are zopiclone, and zolpidem tartrate, respectively. When BD patients take ZOP or ZOL, ZOP or ZOL is assigned the value of 1, otherwise ZOP or ZOL is 0.
Evaluation
Visual evaluation of final clozapine MIPD model in BD patients is shown in Figure 1, individual plots are shown in Figure 2, and bootstrap validation is shown in Table 3, indicating that clozapine model is accurate and reliable. Figure 3 is the clearance rate of clozapine in patients with BD. Meanwhile, when patients with BD are combined with zopiclone or zolpidem tartrate, the clearance rates of clozapine in patients with BD decrease by 44.9% or 35%, respectively.
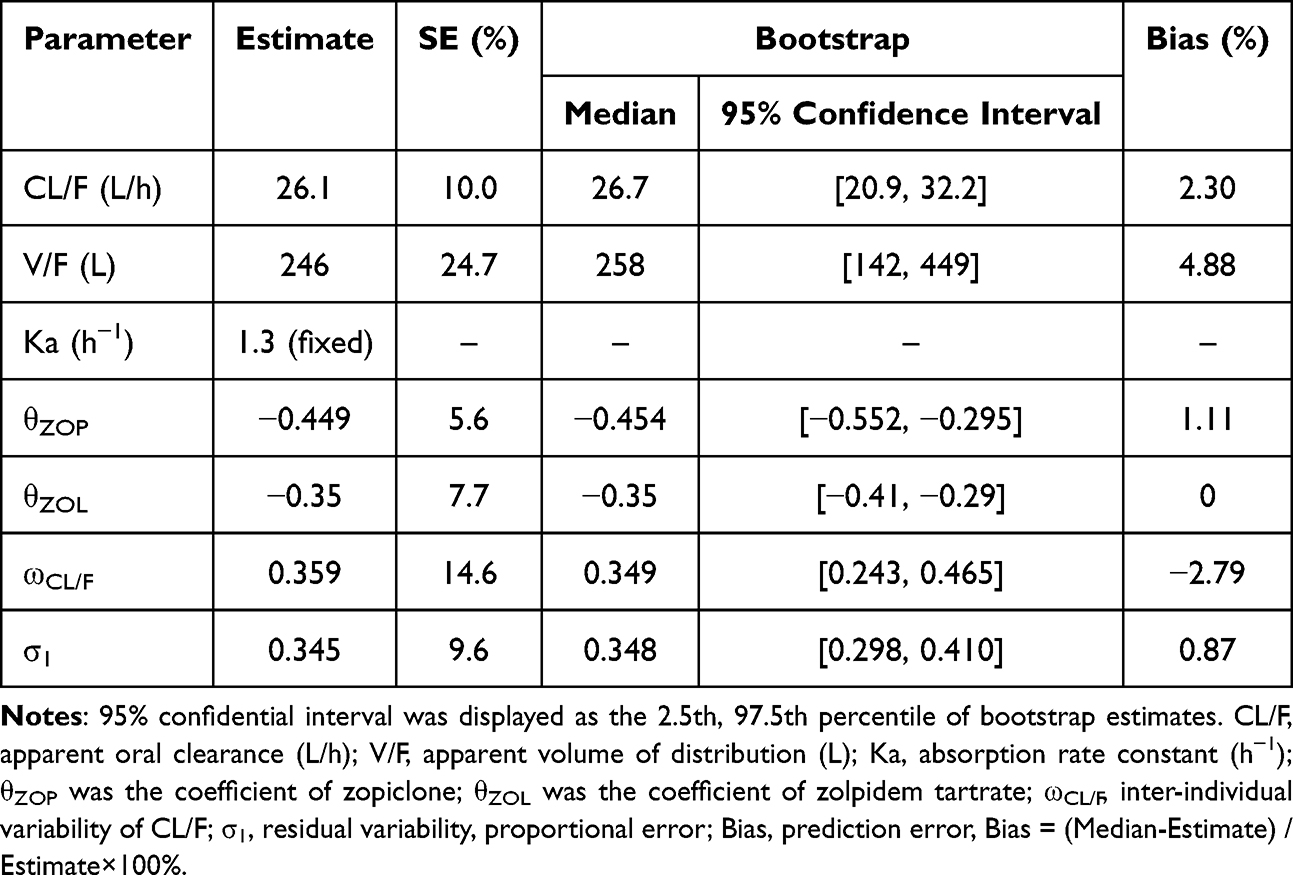 |
Table 3 Parameter Estimates of Clozapine Final Model and Bootstrap Validation in Bipolar Disorder Patients |
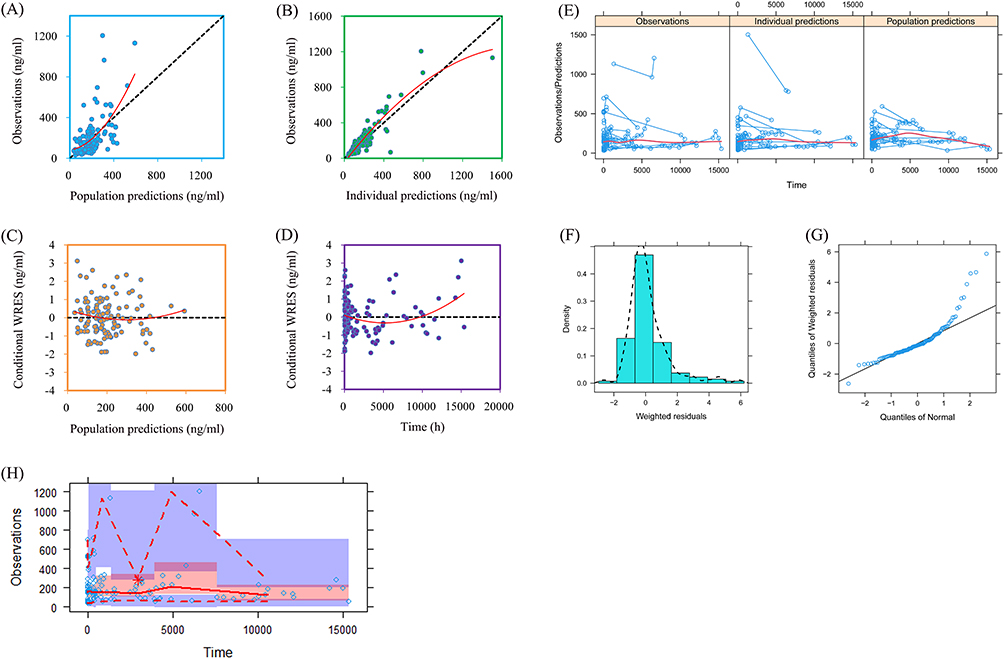 |
Figure 1 Model evaluation. (A) Observations vs population predictions. (B) Observations vs individual predictions. (C) Conditional weighted residuals (WRES) vs population predictions. (D) Conditional WRES vs time. (E) Observations/Predictions vs time. (F) Density vs weighted residuals. (G) Quantiles of weighted residuals vs quantiles of normal. (H) Visual predictive check (VPC) of model. |
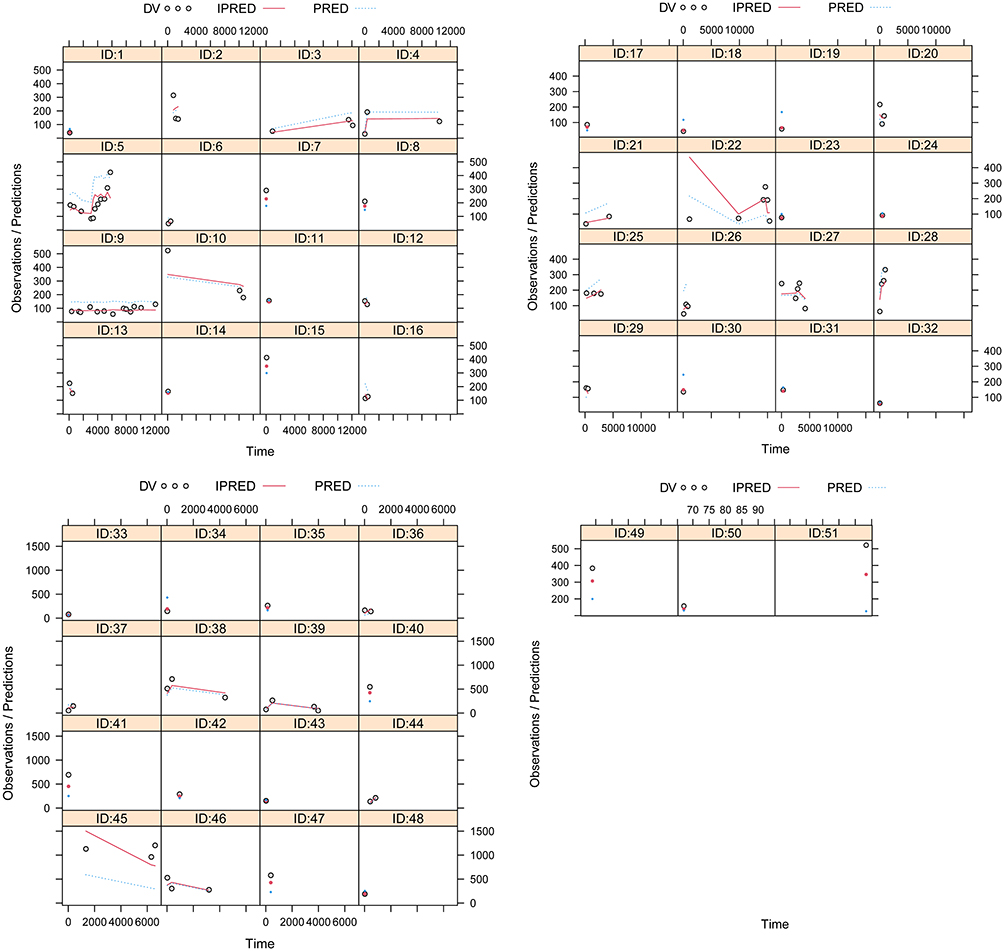 |
Figure 2 Individual plots. Abbreviations: ID, patient ID number; DV, measured concentration values; IPRED, individual predictive values; PRED, population predictive values. |
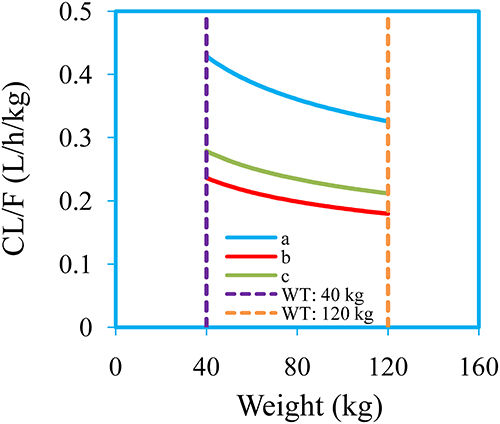 |
Figure 3 The clearance rates of clozapine in patients with bipolar disorder. a: patients with bipolar disorder are not combined with zopiclone or zolpidem tartrate. b: patients with bipolar disorder are combined with zopiclone. c: patients with bipolar disorder are combined with zolpidem tartrate. |
Recommended Dose
The simulated clozapine concentrations in patients with BD who are not combined with zopiclone or zolpidem tartrate, the simulated clozapine concentrations in patients with BD who are combined with zopiclone, and the simulated clozapine concentrations in patients with BD who are combined with zolpidem tartrate are shown in Figures 4–6, respectively. The probability for achieving the target concentrations of clozapine in patients with BD is shown in Figure 7, where Figure 7A–C are patients with BD who are not combined with zopiclone or zolpidem tartrate, patients with BD who are combined with zopiclone, patients with BD who are combined with zolpidem tartrate, respectively. When patients with BD have no combined medication of zopiclone or zolpidem tartrate, the recommended doses of clozapine for patients at 40–45 kg, 45–60 kg, 60–78 kg, 78–106 kg, and 106–120 kg are 10 mg/kg/day, 9 mg/kg/day, 8 mg/kg/day, 7 mg/kg/day, and 6 mg/kg/day, respectively. When patients with BD are combined with zopiclone, the recommended doses of clozapine for patients at 40–60 kg and 60–120 kg are 4 mg/kg/day and 3 mg/kg/day, respectively. When patients with BD are combined with zolpidem tartrate, the recommended doses of clozapine for patients at 40–52 kg and 52–120 kg are 5 mg/kg/day and 4 mg/kg/day, respectively. The recommended doses are shown in Table 4. Furthermore, this study simulates the probability to exceed the upper limit of the safe concentrations, which is shown in Figure 8A–C are patients with BD who are not combined with zopiclone or zolpidem tartrate, patients with BD who are combined with zopiclone, patients with BD who are combined with zolpidem tartrate, respectively. The detailed probability to exceed the upper limit of the safe concentrations can be seen in Table 4.
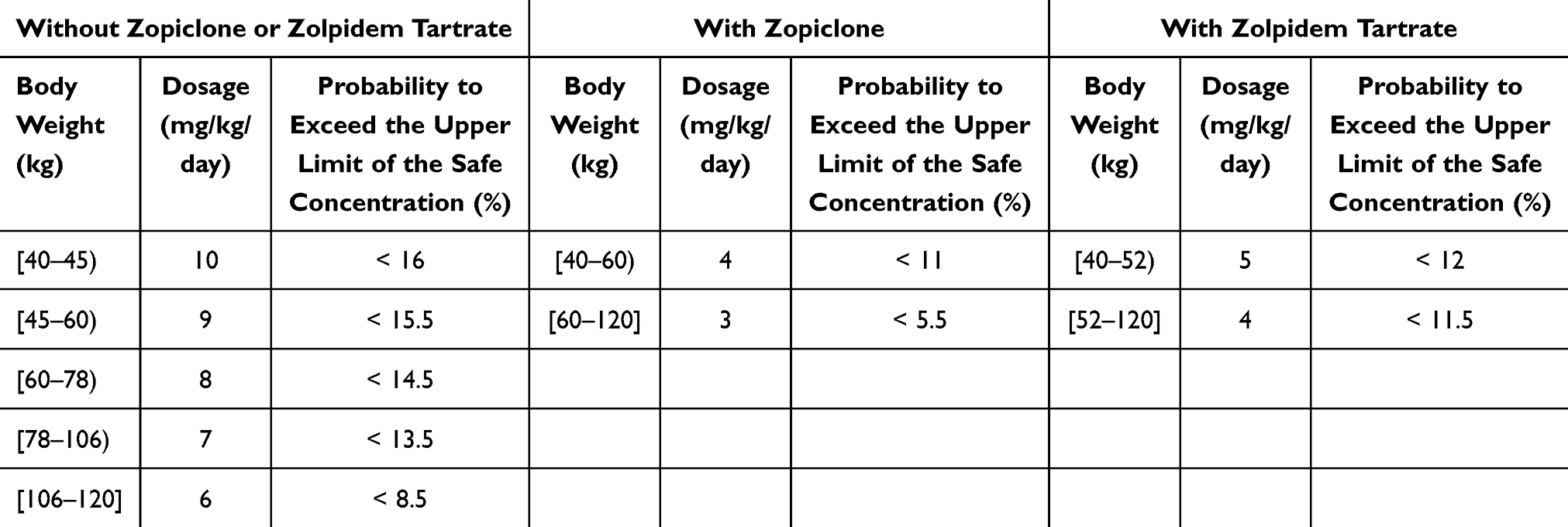 |
Table 4 Initial Dosage Recommendation of Clozapine in Patients with Bipolar Disorder |
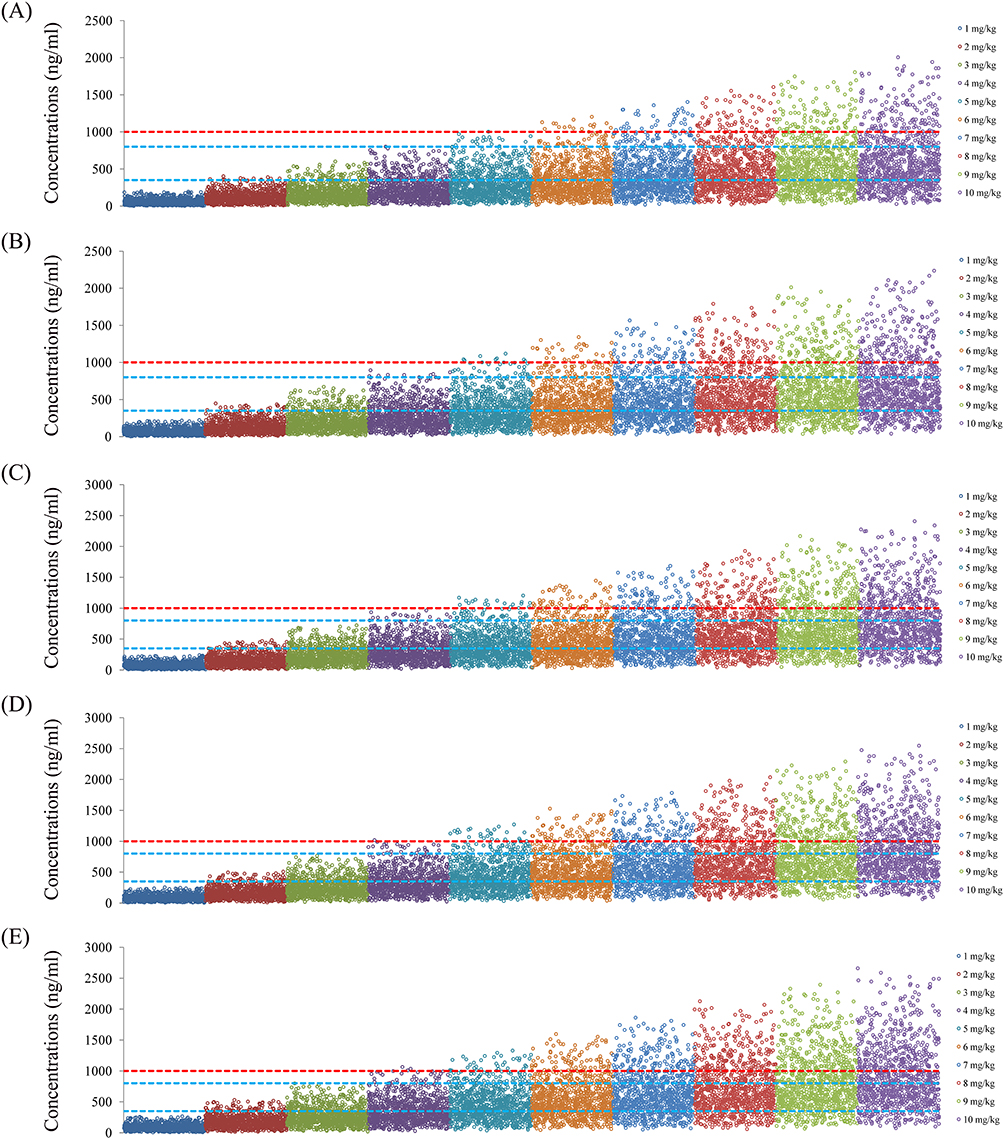 |
Figure 4 The simulated clozapine concentrations in patients with bipolar disorder who are not combined with zopiclone or zolpidem tartrate. (A) Bipolar disorder patients with 40 kg. (B) Bipolar disorder patients with 60 kg. (C) Bipolar disorder patients with 80 kg. (D) Bipolar disorder patients with 100 kg. (E) Bipolar disorder patients with 120 kg. |
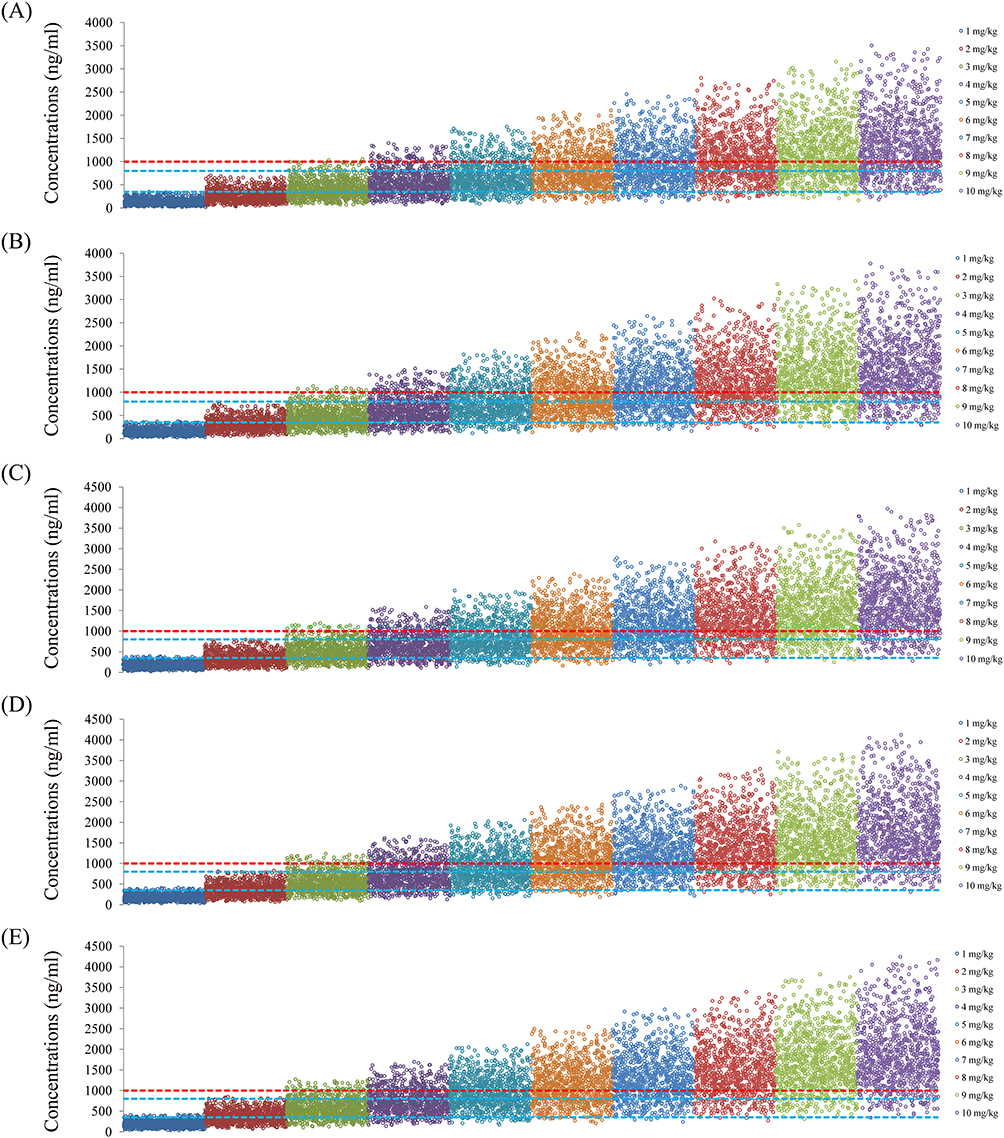 |
Figure 5 The simulated clozapine concentrations in patients with bipolar disorder who are combined with zopiclone. (A) Bipolar disorder patients with 40 kg. (B) Bipolar disorder patients with 60 kg. (C) Bipolar disorder patients with 80 kg. (D) Bipolar disorder patients with 100 kg. (E) Bipolar disorder patients with 120 kg. |
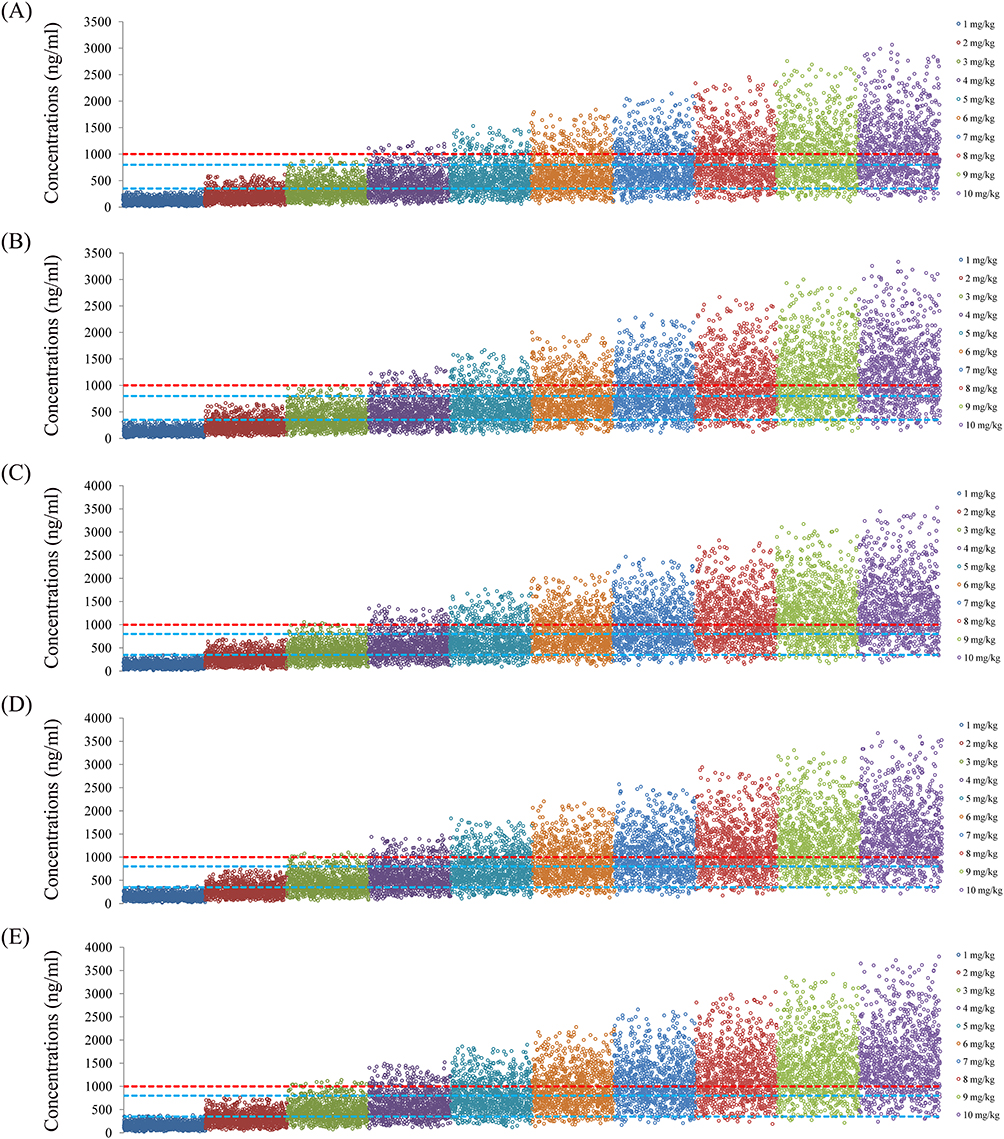 |
Figure 6 The simulated clozapine concentrations in patients with bipolar disorder who are combined with zolpidem tartrate. (A) Bipolar disorder patients with 40 kg. (B) Bipolar disorder patients with 60 kg. (C) Bipolar disorder patients with 80 kg. (D) Bipolar disorder patients with 100 kg. (E) Bipolar disorder patients with 120 kg. |
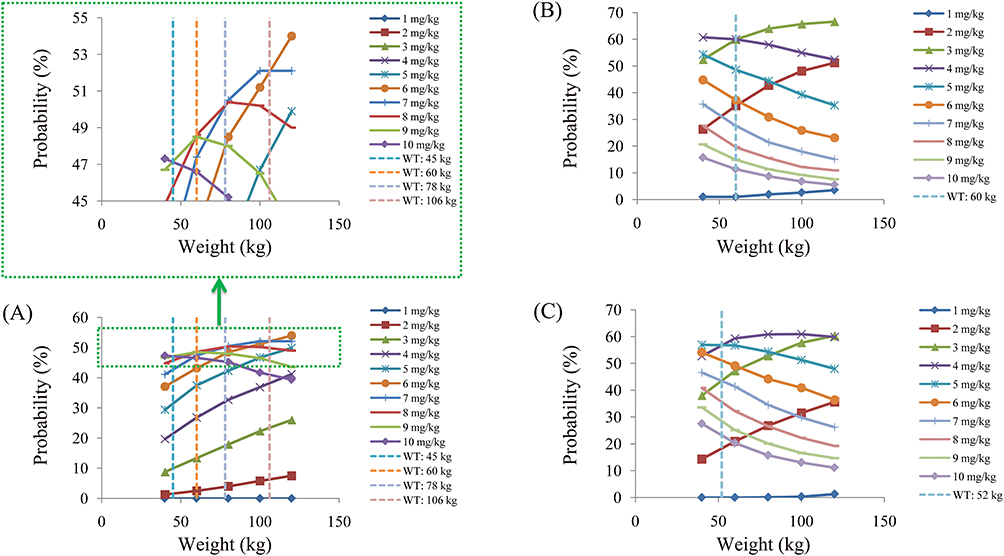 |
Figure 7 Probability for achieving the target concentrations of clozapine in patients with bipolar disorder. (A) Patients with bipolar disorder who are not combined with zopiclone or zolpidem tartrate. (B) Patients with bipolar disorder who are combined with zopiclone. (C) Patients with bipolar disorder who are combined with zolpidem tartrate. |
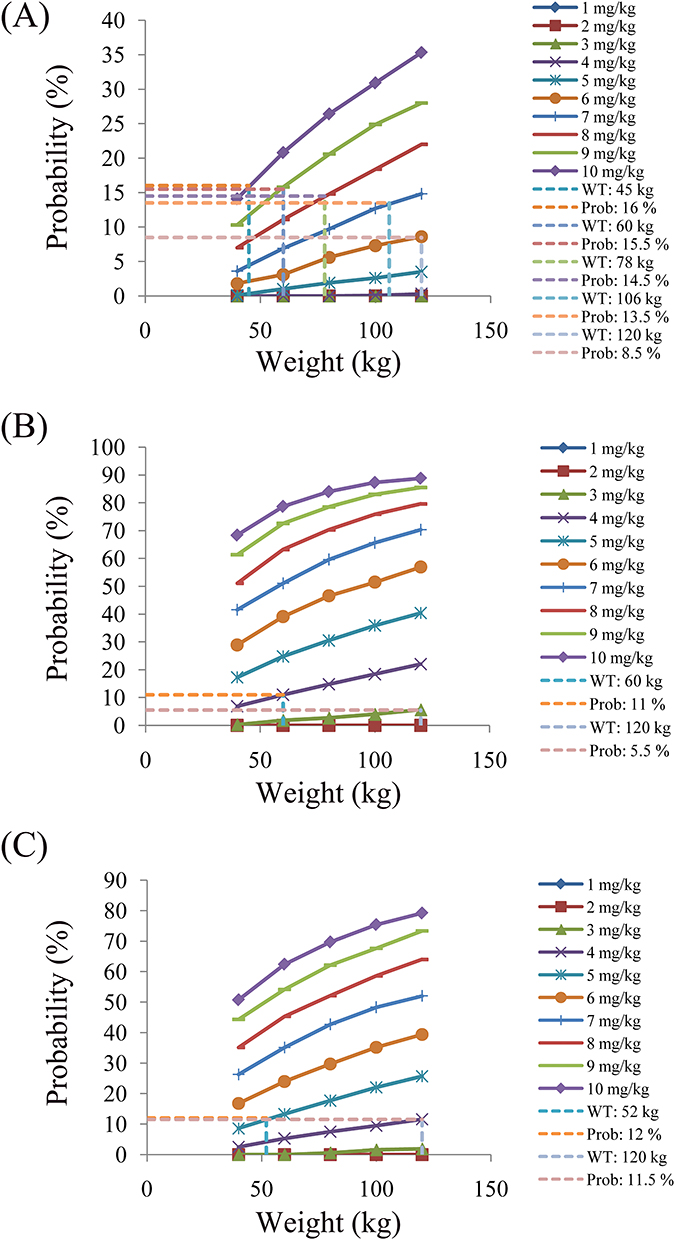 |
Figure 8 Probability for exceeding the upper limit of safe concentrations in patients with bipolar disorder. (A) Patients with bipolar disorder who are not combined with zopiclone or zolpidem tartrate. (B) Patients with bipolar disorder who are combined with zopiclone. (C) Patients with bipolar disorder who are combined with zolpidem tartrate. |
Discussion
DDI refers to the synergistic effect produced when patients use multiple drugs simultaneously or sequentially. It may enhance the therapeutic effect or alleviate adverse reactions, or it may reduce the therapeutic effect or cause unexpected toxicity.38 This interaction can be divided into two categories: enhanced efficacy (including improved therapeutic effect and increased toxicity) and weakened efficacy (including decreased therapeutic effect and reduced toxicity). In terms of mechanism, it can be divided into pharmacokinetic and/or pharmacodynamic interactions. The pharmacokinetic interactions of medicine mainly result from the mutual interference of drugs in the absorption, distribution, metabolism and excretion links. Recent studies have confirmed that pharmacokinetic DDI can significantly alter the administration process of antipsychotic drugs in patients,39–44 which affects the clinical therapeutic effect. Therefore, individualized drug administration regimens need to be considered in clinical drug administration. To explore the pharmacokinetic effects of combined medication on clozapine in patients with BD and further screen for potential DDI factors, this study conducts relevant explorations using MIPD.
MIPD integrates individual differences of patients, drug characteristics and disease information through mathematical modeling to guide personalized dose adjustment, so as to improve therapeutic effect and reduce adverse reactions.45,46 Especially in the exploration of drug-related effects, MIPD has significant advantages. MIPD overcomes the limitations of traditional DDI clinical trials in terms of sample size, cost control, and coverage of special populations through sparse data modeling, multi-dimensional covariate integration, and dynamic simulation techniques. It is particularly suitable for interaction analysis and precise medication intervention in complex medication scenarios. Among them, the PPK model is one of the mainstream research methods of MIPD and is currently an important tool used in clinical research for DDI.47–51 Based on this, we explore clozapine DDI and its individualized administration regimens for patients with BD based on MIPD technology, and achieve clinical precision medication.
The present study collects 51 patients with BD treated with clozapine and all the concomitant medication information used in the clinical practice of the patients are included and analyzed. Although the current number of 51 patients included is not very large, this methodological approach for PPK is fully adequate. Many studies with a similar sample size have already been reported. For example, in the study of population pharmacokinetics and dosing optimisation of polymyxin B in patients with severe burns, the sample size is 53.52 In the study of population pharmacokinetics and dosing optimization of cefoselis in paediatric patients with haematological malignancies, the sample size is 53.53 In the study of levetiracetam dosing optimization in neurocritical care population: neuro-ARC study, the sample size is 50.54 In the study of population pharmacokinetics and pharmacodynamics of meropenem in critically ill patients with renal impairment or on continuous renal replacement therapy, the sample size is 54.55 In the study of impact of body weight on mycophenolic acid population pharmacokinetics in paediatric lupus nephritis: a pharmacogenomic integration study, the sample size is 51.56 In the study of population pharmacokinetics of pyrazinamide and isoniazid in plasma and cerebrospinal fluid from South African adults with tuberculous meningitis, the sample size is 49.57 That is to say, the current sample size of 51 patients is sufficient.
In the final result of present study, zopiclone, zolpidem tartrate with clozapine have DDI. Meanwhile, when patients with BD are combined with zopiclone or zolpidem tartrate, the clearance rates of clozapine in patients with BD decrease by 44.9% or 35%, respectively. Zopiclone and zolpidem tartrate are both commonly used non-benzodiazepine sedative-hypnotic drugs in clinical practice, mainly used to treat insomnia. In the treatment of BD, they are mainly used to improve sleep disorders. Of course, this research result can also be explained. As everyone knows, clozapine is mainly metabolized in the liver through CYP3A4 and CYP1A2.58–60 In addition, zopiclone and zolpidem tartrate are mainly metabolized by the CYP3A4 enzyme.61–64 Therefore, zopiclone and zolpidem tartrate may compete CYP3A4 metabolic enzymes, influence clozapine in the clearance rate of patients with BD.
Furthermore, the present study recommends the dose of clozapine in patients with BD in the presence of DDI through Monte Carlo simulation. When patients with BD have no combined medication of zopiclone or zolpidem tartrate, the recommended doses of clozapine for patients at 40–45 kg, 45–60 kg, 60–78 kg, 78–106 kg, and 106–120 kg are 10 mg/kg/day, 9 mg/kg/day, 8 mg/kg/day, 7 mg/kg/day, and 6 mg/kg/day, respectively. When patients with BD are combined with zopiclone, the recommended doses of clozapine for patients at 40–60 kg and 60–120 kg are 4 mg/kg/day and 3 mg/kg/day, respectively. When patients with BD are combined with zolpidem tartrate, the recommended doses of clozapine for patients at 40–52 kg and 52–120 kg are 5 mg/kg/day and 4 mg/kg/day, respectively.
Currently, the research mainly focuses on the DDI in pharmacokinetics. In the future, it is necessary to further explore the DDI impact on symptom control and adverse reactions. Additionally, the TDM data from external validation needs to be further verified to support our conclusions.
Conclusion
The present study explores the DDI of clozapine in patients with BD based on MIPD, and recommends the individualized dosing regimen of clozapine in patients with BD according to concomitant medication. The TDM data from external validation need to be further verified to support our conclusions in the future.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Science and Technology Program of Xuzhou (No. KC23217), The Basic Science (Natural Science) Project of Higher Education Institutions in Jiangsu Province (No. 25KJD310004), The Medical Research Project of Jiangsu Provincial Health Commission (No. Z2023010), Jiangsu Province Education Science Planning Project (No. C/2022/01/36), Xuzhou Medical University Labor Education Special Project (No. X1d202209), Jiangsu Province Higher Education Informatization Research Topic (No. 2023JSETKT136), Xuzhou Medical University Research Topic of Higher Education Teaching Reform (No. Xjyzrd202304). Xuzhou Medical University Research Project on Reform of Postgraduate Education and Teaching (No. XYJGKT202506). Xuzhou Medical University Teaching Academic Research Topics (No. 2024ZDKT02-Y03). Suzhou Applied Basic Research Science and Technology Innovation Project (No. SYWD2024258).
Disclosure
Yue Zhang, Jie Wang, Xue Tian, Yi-Jia Zhang, and Ye Li are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Uzman Ozbek S, Verim B, Kucukakdag A. et al. Clinical high risk for psychosis in bipolar disorder: clinical features, cognition and functioning. Psychiatry Res. 2025;348:116478. doi:10.1016/j.psychres.2025.116478
2. Chan JMT, Lo HKY, Chau AKC, et al. Cognitive and affective theory-of-mind impairment in people with early-stage bipolar disorder. BMC Psychiatry. 2025;25(1):526. doi:10.1186/s12888-025-06808-1
3. Huang Y, Zhou S, Feng S, et al. Differential relationships among homocysteine levels, cognitive deficits, and low-frequency fluctuation in brain activity in bipolar disorder with suicidal ideation. BMC Psychiatry. 2025;25(1):514. doi:10.1186/s12888-025-06925-x
4. Liu S, Xu JJ, Zhu XQ, et al. Factors associated with the frequency of manic and depressive episodes in bipolar disorder: a multicenter study in China. BMC Psychiatry. 2025;25(1):507. doi:10.1186/s12888-025-06863-8
5. Warner A, Holland C, Lobban F, Bentley L, Tyler E, Palmier-Claus J. Quality of life in older adults with mood states associated with bipolar disorder: a secondary analysis of the English longitudinal study of ageing data. Br J Clin Psychol. 2025;64(2):188–202. doi:10.1111/bjc.12495
6. Du J, Baranova A, Zhang F. Bidirectional causal effects between bipolar disorder and immune cell traits. J Affect Disord. 2025;383:179–186. doi:10.1016/j.jad.2025.04.146
7. Liu J, Chen Z, Teng Z, et al. Chronic inflammation response as a key factor in polycystic ovary syndrome among patients with bipolar disorder. J Affect Disord. 2025;377:264–274. doi:10.1016/j.jad.2025.02.072
8. Geoffroy PA, Maruani J. Chronobiology of mood disorders: the role of the biological clock in depression and bipolar disorder. Biol Psychiatry. 2025;98:830–841. doi:10.1016/j.biopsych.2025.05.005
9. McQuillin A, Ophoff RA. Genomics of Bipolar Disorder: what the Clinician Needs to Know. Psychiatr Clin North Am. 2025;48(2):331–341. doi:10.1016/j.psc.2025.01.009
10. Khayachi A, Nunes A, Alda M, Rouleau GA. The overlooked role of metabolic disorders in bipolar disorder. Neurosci Biobehav Rev. 2025;174:106203. doi:10.1016/j.neubiorev.2025.106203
11. Jain A, Mitra P. Bipolar Disorder. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Paroma Mitra declares no relevant financial relationships with ineligible companies; 2025.
12. Lin J, Hong L, Wang Z, et al. Analysis of maintenance pharmacotherapy in Chinese bipolar disorder patients: guideline concordance and adjunctive medication use. J Affect Disord. 2025;381:560–572. doi:10.1016/j.jad.2025.03.096
13. Prajapati AR, Scott S, Dima AL, et al. A qualitative investigation of the modifiable determinants of medication adherence in bipolar disorder (BD): views of patients and their family and friends. J Affect Disord. 2025;382:462–470. doi:10.1016/j.jad.2025.04.149
14. Clozapine. Drugs and Lactation Database (LactMed(R)). Bethesda (MD); 2006.
15. Fanshawe JB, Kabir T, Lennox BR. Clozapine: old drugs require efforts to improve patient experience and access. Lancet. 2025;405:2259–2261. doi:10.1016/S0140-6736(25)00774-3
16. Correll CU. Clozapine: past, present and future. World Psychiatry. 2025;24(2):153–154. doi:10.1002/wps.21335
17. Wilkowska A, Wiglusz MS, Cubala WJ. Clozapine: promising treatment for suicidality in bipolar disorder. Psychiatry Danub. 2019;31(Suppl 3):574–578.
18. Morrison PD, Jauhar S, Young AH. The mechanism of action of clozapine. J Psychopharmacol. 2025;39(4):297–300. doi:10.1177/02698811251319458
19. Tabrisi R, Harun-Rashid MD, Montero J, Venizelos N, Msghina M. Clozapine but not lithium reverses aberrant tyrosine uptake in patients with bipolar disorder. Psychopharmacology. 2023;240(8):1667–1676. doi:10.1007/s00213-023-06397-5
20. Kapczinski F, Pfaffenseller B, Dursun SM, de Azevedo Cardoso T. Clozapine for bipolar disorder: what do we know so far and what next? Bipolar Disord. 2021;23(2):115–116. doi:10.1111/bdi.13050
21. Delgado A, Velosa J, Zhang J, Dursun SM, Kapczinski F, de Azevedo Cardoso T. Clozapine in bipolar disorder: a systematic review and meta-analysis. J Psychiatr Res. 2020;125:21–27. doi:10.1016/j.jpsychires.2020.02.026
22. Wilkowska A, Wiglusz MS, Cubala WJ. Clozapine in treatment-resistant bipolar disorder with suicidality. three case reports. Front Psychiatry. 2019;10:520. doi:10.3389/fpsyt.2019.00520
23. Loo LWJ, Chew QH, Lin SK, et al. Clozapine use for bipolar disorder: an Asian Psychotropic Prescription Patterns Consortium Study. J Clin Psychopharmacol. 2023;43(3):278–282. doi:10.1097/JCP.0000000000001693
24. Forte A, Pompili M, Imbastaro B, et al. Effects on suicidal risk: comparison of clozapine to other newer medicines indicated to treat schizophrenia or bipolar disorder. J Psychopharmacol. 2021;35(9):1074–1080. doi:10.1177/02698811211029738
25. Sherazi AW. Challenges in validating population pharmacokinetic models for clozapine dosage prediction and therapeutic drug monitoring. Ther Drug Monit. 2025;47(2):313–315. doi:10.1097/FTD.0000000000001280
26. Lind PA, Parker RK, Northwood K, Siskind DJ, Medland SE. Clozapine efficacy and adverse drug reactions among a Nationwide Study of 1021 Australians prescribed clozapine: the ClozaGene Study. Schizophr Bull. 2025;51(2):458–469. doi:10.1093/schbul/sbae065
27. Flanagan RJ, Handley SA, James C, Wells L, Every-Palmer S. Clozapine-induced gastrointestinal hypomotility: UK pharmacovigilance reports, 2018–2022. BJPsych Open. 2025;11(3):e79. doi:10.1192/bjo.2025.29
28. Zheng P, Semancik S, Barman I. Deep learning-assisted SERS for therapeutic drug monitoring of clozapine in serum on plasmonic metasurfaces. Nano Lett. 2025;25(13):5342–5349. doi:10.1021/acs.nanolett.5c00391
29. Jogi L, Praveen P, Shibu A, et al. The impact of therapeutic drug monitoring on clozapine dosing and clinical outcome in a Tertiary Care Center in India: a retrospective study. J Clin Psychopharmacol. 2025;45(3):251–257. doi:10.1097/JCP.0000000000001980
30. Bye KN, Leloux MR, Cole KC, et al. Improving result turnaround time as a crucial factor to increasing clozapine therapeutic drug monitoring in hospitalized patients. J Clin Psychopharmacol. 2025;45(3):225–230. doi:10.1097/JCP.0000000000001982
31. Shang DW, Li LJ, Wang XP, et al. Population pharmacokinetic/pharmacodynamic model of clozapine for characterizing the relationship between accumulated exposure and PANSS scores in patients with schizophrenia. Ther Drug Monit. 2014;36(3):378–386. doi:10.1097/FTD.0000000000000014
32. Li LJ, Shang DW, Li WB, et al. Population pharmacokinetics of clozapine and its primary metabolite norclozapine in Chinese patients with schizophrenia. Acta Pharmacol Sin. 2012;33(11):1409–1416. doi:10.1038/aps.2012.71
33. Anderson BJ, Holford NH. Mechanism-based concepts of size and maturity in pharmacokinetics. Ann Rev Pharmacol Toxicol. 2008;48:303–332. doi:10.1146/annurev.pharmtox.48.113006.094708
34. Wills KH, Behan SJ, Nance MJ, et al. Combining Therapeutic Drug Monitoring and Pharmacokinetic Modelling Deconvolutes Physiological and Environmental Sources of Variability in Clozapine Exposure. Pharmaceutics. 2021;14(1):47. doi:10.3390/pharmaceutics14010047
35. Liu HC, Chang WH, Wei FC, Lin SK, Lin SK, Jann MW. Monitoring of plasma clozapine levels and its metabolites in refractory schizophrenic patients. Ther Drug Monit. 1996;18(2):200–207. doi:10.1097/00007691-199604000-00015
36. Stark A, Scott J. A review of the use of clozapine levels to guide treatment and determine cause of death. Aust N Z J Psychiatry. 2012;46(9):816–825. doi:10.1177/0004867412438871
37. Schulte P. What is an adequate trial with clozapine?: therapeutic drug monitoring and time to response in treatment-refractory schizophrenia. Clin Pharmacokinet. 2003;42(7):607–618. doi:10.2165/00003088-200342070-00001
38. Cheng J, Zhang Y, Zhang H, Lu M. Fuzzy-DDI: a robust fuzzy logic query model for complex drug-drug interaction prediction. Artif Intell Med. 2025;164:103125. doi:10.1016/j.artmed.2025.103125
39. Ngo LT, Yun HY, Chae JW. Application of the population pharmacokinetics model-based approach to the prediction of drug-drug interaction between rivaroxaban and carbamazepine in humans. Pharmaceuticals. 2023;16(5):684. doi:10.3390/ph16050684
40. Zhang C, Chen L, Duan YY, et al. Drug-drug interaction of paroxetine on olanzapine and initial dosage optimization in patients with major depressive disorder based on population pharmacokinetics. Front Psychiatry. 2025;16:1538996. doi:10.3389/fpsyt.2025.1538996
41. Zhang C, Jiang L, Hu K, et al. Effects of aripiprazole on olanzapine population pharmacokinetics and initial dosage optimization in schizophrenia patients. Neuropsychiatr Dis Treat. 2024;20:479–490. doi:10.2147/NDT.S455183
42. Vella T, Mifsud J. Interactions between valproic acid and quetiapine/olanzapine in the treatment of bipolar disorder and the role of therapeutic drug monitoring. J Pharm Pharmacol. 2014;66(6):747–759. doi:10.1111/jphp.12209
43. Liu H, Yu Y, Qin Y, Han B. PBPK modelling for the evaluation of drug-drug interaction between meropenem and valproic acid. Br J Clin Pharmacol. 2025;91(4):1198–1207. doi:10.1111/bcp.16350
44. Liu Z, Shao W, Wang X, et al. Physiologically based pharmacokinetic models for predicting lamotrigine exposure and dose optimization in pediatric patients receiving combination therapy with carbamazepine or valproic acid. Pharmacotherapy. 2024;44(9):711–721. doi:10.1002/phar.4603
45. Falkenhagen U, Cavallari LH, Duarte JD, Kloft C, Schmidt S, Huisinga W. Leveraging QSP models for MIPD: a case study for Warfarin/INR. Clin Pharmacol Ther. 2024;116(3):795–806. doi:10.1002/cpt.3274
46. Perez-Blanco JS, Lanao JM. Model-Informed Precision Dosing (MIPD). Pharmaceutics. 2022;14(12):2731. doi:10.3390/pharmaceutics14122731
47. Wu Y, Niu LL, Ling YY, et al. Drug-drug interaction of phenytoin sodium and methylprednisolone on voriconazole: a population pharmacokinetic model in children with thalassemia undergoing allogeneic hematopoietic stem cell transplantation. Eur J Clin Pharmacol. 2025;81(3):365–374. doi:10.1007/s00228-024-03795-2
48. Tolbert D, Bekersky I, Chu HM, Ette EI. Drug-metabolism mechanism: knowledge-based population pharmacokinetic approach for characterizing clobazam drug-drug interactions. J Clin Pharmacol. 2016;56(3):365–374. doi:10.1002/jcph.603
49. Cleary Y, Kletzl H, Grimsey P, et al. Estimation of FMO3 ontogeny by mechanistic population pharmacokinetic modelling of Risdiplam and its impact on drug-drug interactions in children. Clin Pharmacokinet. 2023;62(6):891–904. doi:10.1007/s40262-023-01241-7
50. Wang DD, Chen X, Fu M, Zheng QS, Xu H, Li ZP. Model extrapolation to a real-world dataset: evaluation of tacrolimus population pharmacokinetics and drug interaction in pediatric liver transplantation patients. Xenobiotica. 2020;50(4):371–379. doi:10.1080/00498254.2019.1631505
51. Zhou D, Lu Z, Sunzel M, Xu H, Al-Huniti N. Population pharmacokinetic modelling to assess clinical drug-drug interaction between AZD7325 and midazolam. J Clin Pharm Therap. 2014;39(4):404–410. doi:10.1111/jcpt.12152
52. Yang J, Liu F, Zhao Y, et al. Population pharmacokinetics and dosing optimisation of polymyxin B in patients with severe burns. Burns. 2025;51(9):107696. doi:10.1016/j.burns.2025.107696
53. Liu JR, Fu SM, Jirasomprasert T, et al. Population pharmacokinetics and dosing optimization of cefoselis in paediatric patients with haematological malignancies. J Antimicrob Chemother. 2025. doi:10.1093/jac/dkaf363
54. Kharouba M, Cook AM, Bastin MLT, Kutsogiannis DJ, Mahmoud SH. Levetiracetam dosing optimization in neurocritical care population: neuro-ARC study. Neurocrit Care. 2025. doi:10.1007/s12028-025-02347-5
55. Feng C, Bian J, Qu Y, et al. Population pharmacokinetics and pharmacodynamics of meropenem in critically ill patients with renal impairment or on continuous renal replacement therapy. Eur J Clin Pharmacol. 2025;81(11):1689–1698. doi:10.1007/s00228-025-03910-x
56. Ye C, Liu B, Chen L, et al. Impact of body weight on mycophenolic acid population pharmacokinetics in paediatric lupus nephritis: a pharmacogenomic integration study. Lupus Sci Med. 2025;12(2):e001535. doi:10.1136/lupus-2025-001535
57. Calderin JM, Wasserman S, Resendiz-Galvan JE, et al. Population pharmacokinetics of pyrazinamide and isoniazid in plasma and cerebrospinal fluid from South African adults with tuberculous meningitis. Antimicrob Agents Chemother. 2025;69(8):e0009925. doi:10.1128/aac.00099-25
58. Wysokinski A, Dreczka J. Clozapine Toxicity Predictor: deep neural network model predicting clozapine toxicity and its therapeutic dose range. Psychiatry Res. 2024;342:116256. doi:10.1016/j.psychres.2024.116256
59. Rafizadeh R, Sooch A, Risi A, et al. Impact of patient-specific factors on clozapine metabolism in individuals with treatment-resistant schizophrenia or schizoaffective disorder. J Psychopharmacol. 2024;38(6):526–531. doi:10.1177/02698811241241394
60. Kuhn AK, Determan ML, Wright JA, Matey E, Leung JG. The potential influence of estrogen-containing oral contraception on clozapine metabolism in a patient with known pharmacogenomic status. Ment Health Clin. 2024;14(3):220–223. doi:10.9740/mhc.2024.06.220
61. Tornio A, Neuvonen PJ, Backman JT. The CYP2C8 inhibitor gemfibrozil does not increase the plasma concentrations of zopiclone. Eur J Clin Pharmacol. 2006;62(8):645–651. doi:10.1007/s00228-006-0155-6
62. Yoon S, Jeong S, Jung E, et al. Effect of CYP3A4 metabolism on sex differences in the pharmacokinetics and pharmacodynamics of zolpidem. Sci Rep. 2021;11(1):19150. doi:10.1038/s41598-021-98689-z
63. Alderman CP, Gebauer MG, Gilbert AL, Condon JT. Possible interaction of zopiclone and nefazodone. Ann Pharmacother. 2001;35(11):1378–1380. doi:10.1345/aph.1A074
64. Jung EH, Lee CM, Byeon JY, et al. Relationship between plasma exposure of zolpidem and CYP2D6 genotype in healthy Korean subjects. Arch Pharm Res. 2020;43(9):976–981. doi:10.1007/s12272-020-01250-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.