Back to Journals » Clinical Ophthalmology » Volume 13
Clinically relevant differences in the selection of toric intraocular lens power in normal eyes: preoperative measurement vs intraoperative aberrometry
Authors Davison JA, Makari S, Potvin R ![]()
Received 14 February 2019
Accepted for publication 7 May 2019
Published 30 May 2019 Volume 2019:13 Pages 913—920
DOI https://doi.org/10.2147/OPTH.S205352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
James A Davison,1 Sarah Makari,2 Richard Potvin2
1Wolfe Eye Clinic, Marshalltown, IA, USA; 2Science in Vision, Akron, NY, USA
Purpose: To assess the value of intraoperative aberrometry (IA) in determining toric intraocular lens (IOL) power in eyes with no previous ocular surgery.
Patients and methods: This was a retrospective data review at one US clinical site of eyes that underwent uncomplicated cataract surgery with toric IOL implantation where standard preoperative and IA measurements were available. Calculated IOL sphere and cylinder powers and orientation were compared based on the measurement method and the postoperative refraction, using both actual and simulated (back-calculated) results. Comparisons were between the surgeon’s preoperative calculations, IA measurements, the actual IOL implanted and results from the Barrett toric calculator.
Results: There was no significant difference (p>0.7) in the number of eyes expected to have, or having, a spherical equivalent refraction within 0.50D of the target between Actual (92%), IA (93%) or Preoperative calculation results (86%). The percentage of eyes with expected residual refractive astigmatism ≤0.50D was significantly higher for the IA vs Preoperative calculations (75% vs 53%, p<0.01). There was no significant difference in expected results between the Actual, IA and Barrett toric calculations (p>0.65).
Conclusion: Modern IOL calculations for sphere produced results comparable to those achieved with IA. The value of IA in determining IOL cylinder power and orientation was more evident when comparing expected results between IA and a preoperative method based on measured total corneal astigmatism than when comparing to expected results from the Barrett toric calculator.
Keywords: ORA, refraction, prediction error, IOL power calculation, astigmatism, toric IOL
Introduction
The goal of toric intraocular lens (IOL) implantation is to eliminate refractive astigmatism after cataract surgery, but this is not achieved in all cases. A 2012 review by Visser et al1 noted that about 30% of the eyes had more than 0.5D of residual refractive astigmatism after toric lens implantation. More recent studies have noted some improvement in outcomes, but still report about 20% of the eyes with more than 0.5D of residual refractive astigmatism.2–4 Further improving outcomes remains a challenge.
One source of variability in the prediction of refractive outcomes after toric lens implantation is preoperative measurement, primarily corneal power measurement. The most commonly used devices to measure corneal power are keratometers that measure only the anterior cornea. Ignoring the effects of the posterior cornea is likely to result in estimation errors5 and result in an increase in residual astigmatism after toric lens implantation.6,7 Formulas that take into account the astigmatic contribution of the posterior cornea, such as the Abulafia-Koch formula, have increased the likelihood of residual astigmatism less than 0.5D by nearly 50%.2 There are three methods in common use to account for posterior corneal astigmatism (PCA); one is to apply a formula to account for PCA,2 another is to directly measure the PCA preoperatively4 and the third is to directly measure astigmatism intraoperatively in the aphakic eye.
Several formulas have been introduced to account for PCA. One of the most commonly used is the Barrett toric calculator, which relies on a proprietary formula. Compared to other toric calculators the Barrett toric calculator has been shown to be as effective or more effective at increasing prediction accuracy of postoperative residual astigmatism.2,8–11 Reported results using the Barrett toric calculator show 7210–80%2 of the cases having a residual refractive astigmatism of 0.5D or less. This may indicate a limitation to the method, as formulas can rarely account for atypical eyes.
An accurate measurement of the posterior cornea, or the total corneal power, may further improve results. Several preoperative devices can now measure posterior corneal astigmatism directly and can incorporate that into a total corneal power calculation. One device in common use is the Pentacam® HR (OCULUS Optikgeräte GmbH, Wetzlar, Germany), which uses a rotating Scheimpflug camera to provide various corneal power measurements at different diameters from the center of the cornea; it is referred to in this manuscript as the Scheimpflug device. Park et al12 reported that using data from this device may improve results relative to the Barrett toric calculator, while Savini et al6 suggested that results to date were comparable to those obtained with the Barrett toric calculator. One of the measurements provided by the Scheimflug device is the total corneal refractive power (TCRP), a ray tracing technique that has been demonstrated in one study to show high repeatability,13 though was reported as less reliable in another.15 Davison and Potvin4 reported that 80% of the eyes had residual astigmatism within 0.5D using TCRP, while Reitblat et al14 reported a much lower percentage (25%). The large difference in results may be attributed to the fact that it is unclear at what diameter the TCRP value was measured in the Reitblat study. It may also be related to conflicting reports on the consistency of the Scheimpflug device readings, noted above.
Intraoperative aberrometry (IA) is a technique that allows for measurement of the power (sphere and cylinder) of the aphakic eye. One of the most commonly used intraoperative aberrometers is the ORA™ System (Alcon Laboratories, Inc., Fort Worth, TX, USA). Davison and Potvin16 showed comparable outcomes when IA was used relative to preoperative calculations for sphere power, with a possible benefit to considering IA when the difference between the IA and preoperative power calculations was high. Hill et al17 noted that when selecting sphere lens power, IA resulted in 80% of the cases within 0.5D, better than all other methods tested. A recent retrospective study of 30,000 cases noted that IA resulted in 82% of the cases within 0.5D of residual spherical equivalent refraction, while preoperative calculations resulted in 76% of the cases within 0.5D; the difference was greater when the lens power was different.18
Aphakic astigmatism can be directly measured using IA. In one study, compared to using a toric calculator that did not take into account posterior corneal astigmatism, results using aphakic astigmatism measurements from IA showed significantly more eyes with 0.5D or less of residual refractive astigmatism (78% with IA vs 33% without).19 Woodcock et al20 noted that 89% of the cases had residual astigmatism within 0.5D when they implanted toric lenses based on IA measurements, compared to 77% when using standard preoperative optical low coherence reflectometry and a calculator that did not take into account PCA. A large study (3,159 eyes) evaluating astigmatism outcomes from an online toric back calculator found that the use of IA was associated with less residual astigmatism.21 These data were limited to eyes exhibiting significant (>0.5D) residual refractive astigmatism after surgery.
The main concern with IA is that it is reliant on the assumption that the intraoperative measure is a reliable indicator of the postoperative state of the eye. Variables that may influence the accuracy of the IA measurement include eye position, intraocular pressure, effects of the speculum and the effect of ophthalmic viscosurgical devices.22,23
The purpose of the current study was to determine whether suggested IOL power and cylinder orientation from IA were superior to values from preoperative calculations for the purposes of toric IOL planning. IA sphere calculations were compared to the surgeon’s standard approach while IA cylinder calculations were compared to calculations from both the Barrett toric calculator and a toric calculation from a standard calculator using total corneal power as the input data.
Patients and methods
This retrospective data analysis was approved by the Wolfe Eye Clinic Institutional Review Board. A waiver of informed consent for the use of chart data was granted, as no protected health information was used for the analyses. Patient confidentiality was preserved, and data were treated consistent with the tenets of the Declaration of Helsinki. Operative records from 6/17 to 5/18 were reviewed to find eyes with no previous refractive surgery, no significant corneal pathology, for which an uncomplicated cataract surgery with toric IOL implantation was successfully completed; cases where a non-toric IOL was implanted but that included any calculation suggesting a toric IOL were also included. Cases had to include use of intraoperative aberrometry at the time of surgery and a manifest refraction performed 21 days or more after surgery. No eyes that had any secondary treatment (IOL reorientation or refractive procedure such as LASIK) were included.
For each eye, the preoperative biometry from the IOL Master 700 (Carl Zeiss Meditec AG, Jena, Germany), referred to in this manuscript as the biometer, and the Scheimpflug device were required. Sphere power was calculated using the biometer data and the Haigis and SRK/T formulas, with a given mean target between the two for the postoperative refraction. Long eye adjustments were made for eyes longer than 27.99 mm.24 The Haigis and Hoffer Q formulas were used in similar fashion for eyes with an axial length less than 22.0 mm. Results from the formula that yielded a value closest to plano were chosen when the other formula yielded a myopic result. Preoperative toric IOL calculations were made using the TCRP data from the 3 mm Apex Ring of the Scheimpflug device and a standard toric calculator. Additional calculations using the biometer data as input to the Barrett Toric calculator were subsequently made. During cataract surgery, intraoperative aberrometry was used for each eye to determine the recommended sphere power, toric power and orientation of the IOL to be implanted. This was done in the aphakic eye to determine the recommended cylinder power and orientation and then again in the pseudophakic eye to refine the orientation of the IOL. The actual IOL implanted and its final orientation (in the case of toric IOLs) were recorded at the time of surgery.
Back-vertex calculations were used to adjust the postoperative refraction based on differences in suggested sphere power from the preoperative and IA calculations. Results were rounded down (closer to plano) to the nearest 0.125D. After adjusting for the target refraction, this provided the expected (simulated) residual spherical equivalent refractive error for the IOL implanted (Actual), the preoperative calculation (Preop) and the IA calculation (IA).
To compare the cylinder results, four different measures were considered. For the Actual group, and for the IA/Preop group when the IOL implanted was the one suggested by IA/Preop, the postoperative refraction was the measure of interest. For the IA or Preop groups when the IOL suggested was not equal to the lens implanted, and for Barrett, the suggested IOL power and orientation were recorded. Then, a method first described by Hill et al to simulate clinical results from toric IOLs was used.25 In effect, the actual toric IOL implanted was mathematically removed from the eye and the IOL suggested by the results of the IA, Preop or Barrett calculation was mathematically inserted into the eye, yielding a simulated residual cylinder. The cylinder power at the corneal plane as determined from the Barrett toric IOL calculator was used for the remove/replace operation - the ratio between the IOL cylinder power at the IOL plane and the cylinder power at the corneal plane for the given eye was used.
Cylinder analysis consisted of considering the percentage of eyes within 0.50D, 0.75D and 1.00D of residual cylinder (actual or simulated) by calculation method. The IA cylinder power and orientation were compared to those from both the preoperative calculation and the Barrett Toric formula. Of primary interest was which method was expected to result in the highest percentage of eyes within 0.50D. Two other comparisons were made. First, calculation results were compared for those eyes with actual high postoperative cylinder, as these were considered refractive surprises. Second, calculation results for eyes where the vector difference between the Barrett or Preop expected refractive cylinder power and IA was more than 1.0D were analyzed, as these were cases where the cylinder power difference was considered significant. In these two specific comparisons, the intent was to determine if IA produced results consistently better than the other methods; this would suggest that IA might have a positive benefit in terms of reducing outliers.
The measured and calculated data were tabulated in Excel spreadsheets and then imported into an MS Access database for data checking and preliminary analyses (both Microsoft, Redmond, USA). Detailed statistical analysis was performed using the Statistica data analysis software system, version 12 (TIBCO Software Inc., Palo Alto, CA). Categorical comparisons were made using a Chi-squared test, and parametric data were evaluated using an analysis of variance (ANOVA). The level of statistical significance was set at p<0.05.
Results
The retrospective chart review identified 123 eyes in the specified time period with the relevant planning and postoperative refractive data available. Five of these eyes (4%) could not be measured with IA because of excessive movement and/or small pupils, leaving 118 eyes for analysis. Only two lens models were included in the data set; 100 eyes had a toric IOL implanted, while the remaining 18 eyes received a non-toric IOL (SN6ATx and SN60WF, respectively, both Alcon, Fort Worth, Texas, USA).
The expected spherical equivalent refractive error for each calculation method was determined as described in the methods. Table 1 summarizes the results, comparing the actual postoperative residual refractive error and the expected residual refractive errors from the preoperative and IA calculations. The number of eyes within 0.25D and within 0.50D of the intended spherical correction was higher for the IA calculation relative to the preoperative calculation; the difference was statistically significant for the 0.25D values (Chi-squared test, p=0.01) but not for the 0.50D values (Chi-squared test, p=0.08). The mean expected residual error differed overall by 0.13D, with the Preop group having a slightly more myopic mean; this is likely reflective of a more conservative Preop IOL selection (least minus). This was also apparent in the slightly higher likelihood of a hyperopic result (>+0.25D spherical equivalent) with the IA versus Preop calculations (13 vs 8), but the difference here was not statistically significant (Chi-squared test, p=0.25). The mean absolute expected residual error differed by a maximum of 0.08D between methods.
 | Table 1 Residual spherical equivalent refraction by method (n=118) |
The number of outliers for each method was low and similar. There were 9 eyes with Actual spherical equivalent refractive errors greater than 0.5D from intended. In only one of these cases did the IOL power determined by preoperative calculation produce an expected refraction less than or equal to 0.50D. This was similar to IA, where the IOL power determined also would have resulted in an expected refractive error less than or equal to 0.50D in only one case.
Table 2 shows the differences between the preoperative and IA calculated sphere powers, along with a comparison of the results by method. Note that in 42% of the eyes (50/118) there was no difference in the IOL sphere power determined by the preoperative and IA calculations. Where the difference in the expected residual refraction was less than or equal to 0.25D for the preoperative and IA methods, they were considered the same; this was observed in 92% of the eyes (108/118). For the 10 eyes where the expected residual refractive difference was >0.25D, there was no clear benefit seen for Preop or IA calculations.
 | Table 2 Best IOL sphere power by difference in suggested lens power |
Residual cylinder was available from the results of the actual IOL implanted, and from simulated results based on implanting the IOLs suggested by the preoperative calculation, the Barrett Toric calculation and IA. Table 3 summarizes the expected residual refractive errors by calculation method if the recommended IOL was implanted at the orientation determined by the different calculators. The expected percentage of eyes with residual cylinder ≤0.50D was significantly higher for the IA calculation relative to the Preop calculation (Chi-squared test, p<0.01). There was no statistically significant difference between the IA calculation and the other two methods (p>0.65 in both cases). Similarly, the percentage of eyes with residual cylinder ≤0.75D and ≤1.00D was also significantly higher for the IA calculation relative to Preop (p<0.01 and p=0.03, respectively), while there was no statistically significant difference between IA and the other two methods (Actual and Barrett, p>0.11 in all cases).
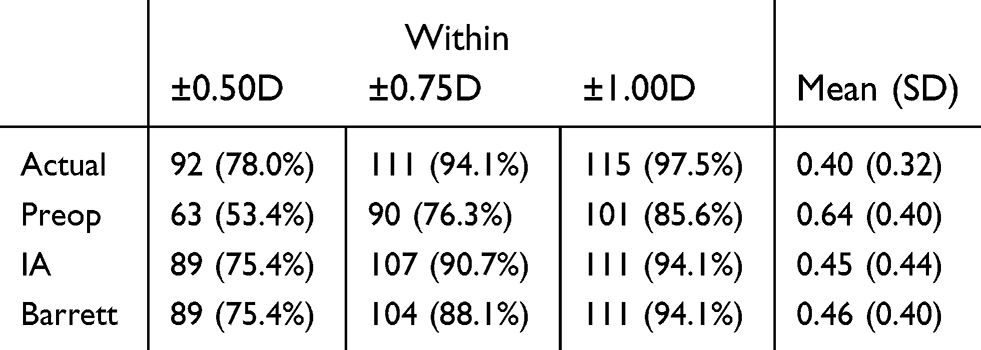 | Table 3 Residual cylinder by method (n=118) |
The differences between IA and the three other methods were considered as follows. The choice of lens cylinder power was either the same or different. If the planned orientation angle for any two methods differed by less than 5 degrees, then the orientation was considered the same; otherwise it was considered different. Table 4 shows the results of comparing the IA suggested cylinder and orientation to the Preop, Barrett and Actual cylinder and orientation. Note that the close match between IA and Actual (70% of the eyes with the same IOL power at the same orientation) was a function of the fact that IA was the primary method used to determine the implanted cylinder power and orientation at the time of surgery.
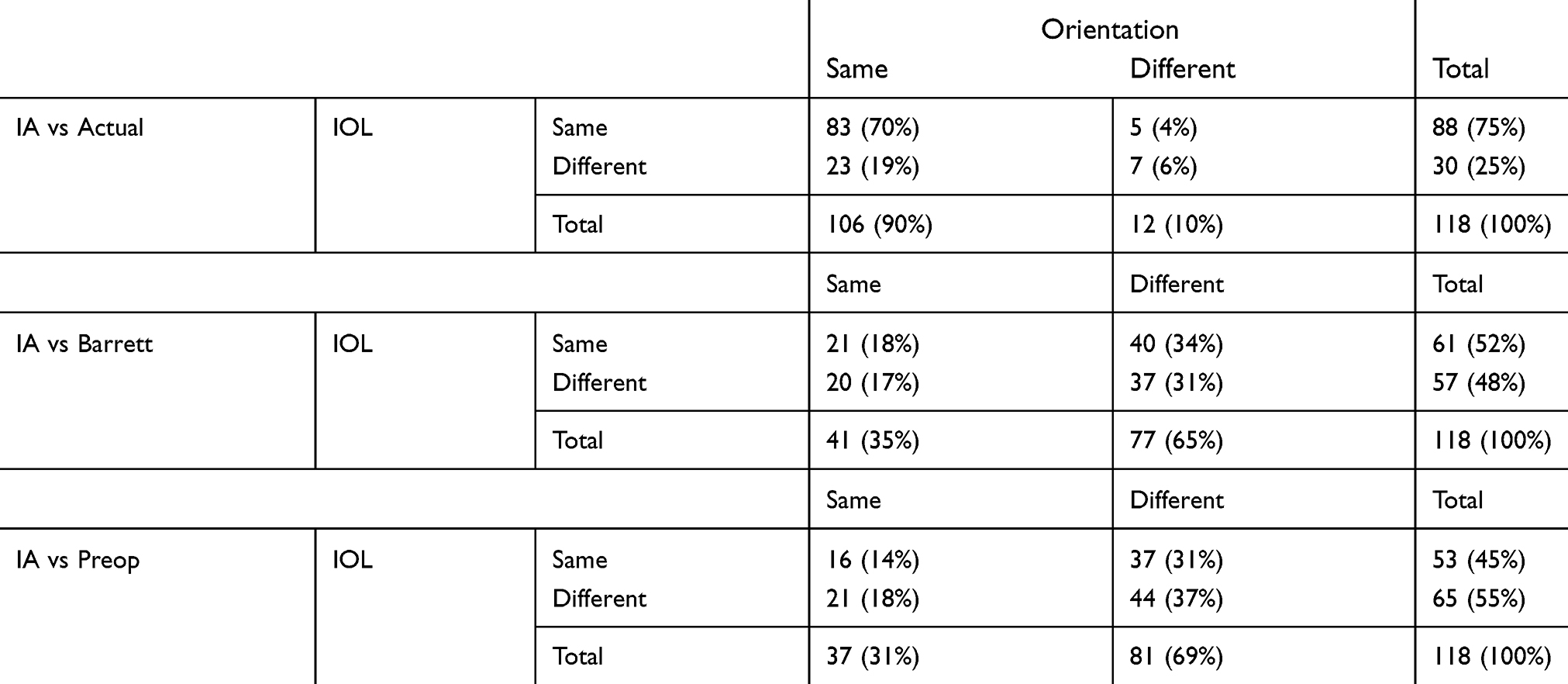 | Table 4 Differences in IOL cylinder power and/or orientation |
From a practical standpoint, the degree to which these changes in IOL cylinder power and orientation were likely to affect clinical outcomes was of interest. The magnitude of simulated or actual residual cylinder was considered for this purpose. If any two methods compared in Table 4 resulted in a difference in cylinder magnitude of 0.25D or less, they were considered the same; test–retest variability in refractive cylinder is higher than this. Otherwise, the method that resulted in the lowest residual cylinder was considered the better choice. Table 5 summarizes the results of this analysis; each line in this table corresponds to an individual cell in Table 4. As can be seen, in 93% of the cases (110/118), the results for IA and the actual lens implanted were expected to be the same. In the remaining 8 cases, there was no clear bias towards one method or the other. A similar comparison showed that 65% (77/118) of the results for the IA and Barrett calculations were expected to be the same. The remaining cases were equally distributed between the IA and Barrett calculations. It is apparent from the table that IA appeared to provide a slightly better result than Barrett when only the lens orientation differed (10 cases to 4), but this was not a statistically significant difference (p=0.25). The differences between IA and Preop were more pronounced. Only 52% (61/118) of the results for the IA and Preop calculations were expected to be the same. When they were different, the IA calculation was statistically significantly more likely to produce a better outcome (Chi-squared test, 41:16 vs 29:29, p=0.02).
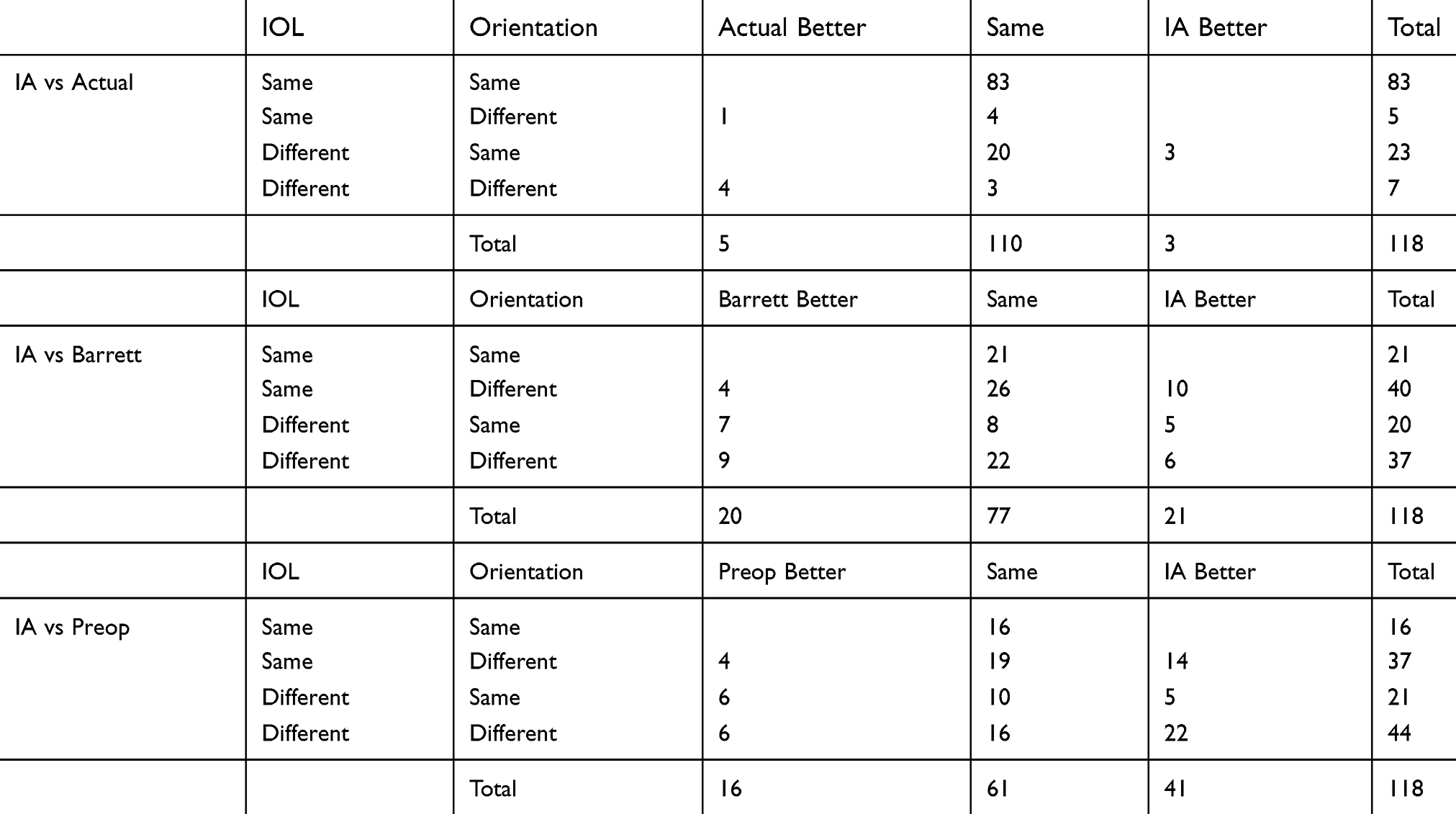 | Table 5 Relatively lower expected residual cylinder by IOL calculation method |
The potential for preventing refractive cylinder outliers was another practical consideration of interest. Three eyes of the 118 (2.5%) had an actual residual refractive astigmatism of 1.0D or higher after toric IOL implantation. In 2 cases, the IA calculation was used to select the IOL implanted. In the other case, the IA calculation would have been expected to produce a slightly better result (1.00 D residual cylinder instead of 1.25 D).
Finally, all cases where the difference in the calculated residual cylinder magnitude between IA and the other two methods (Preop or Barrett) was 1.0D or more were identified. In 7 cases, the IA calculation differed from Preop by 1.0D or more; the IA calculation appeared better for 6 of these. In 5 cases, the IA calculation differed from Barrett by 1.0D or more; the IA calculation appeared better for 4 of these. The numbers show a trend but are too small for reliable statistical analysis.
Discussion
The current study was designed to provide a clinically relevant examination of differences in IOL sphere power, cylinder power and orientation when using IA versus standard preoperative calculation methods.
The percent of eyes with an expected residual spherical equivalent refraction within 0.5D was 93% using IA; this is higher than reported by Hill et al (80%)17 and Cionni et al (82%).18 The mean absolute expected residual error difference between Preop and IA was 0.07D, similar to the value reported by Cionni et al.18 The slightly higher number of eyes within 0.25D with the IA calculation appears to be a function of targeting emmetropia with IA relative to a least-minus target with the Preop calculation, evident in the slightly higher number of hyperopic outcomes with IA. The current study did not observe a notable reduction in outliers (>0.5D absolute error) in spherical equivalent results with IA vs Preop calculations.
There was no clinically significant difference between the sphere power suggested by the Preop calculation and IA (Table 2). This is consistent with results reported by Davison and Potvin.16 The current study found that the number of eyes within 0.50D of the intended spherical equivalent refraction was not significantly different between the Preop and IA groups, though 7% more eyes in the IA group had an expected spherical equivalent refraction within 0.5D. This appears consistent with Cionni et al18, where a 6%18 increase in the number of cases with residual spherical equivalent refraction within 0.5D was found in the IA group when compared with preoperative methods; the larger data set in that study resulted in the observed difference being statistically significant.
In the current study, residual refractive astigmatism of 0.50D or less was expected in 75% of the eyes based on IA, 75% of the eyes based on the Barrett toric calculator and 53% of the eyes using the Preop method (Table 3). The IA and Barrett results reported here are consistent with results reported in the literature, with 78%19 and 72%10 of eyes having residual astigmatism within 0.5D for IA and Barrett, respectively. The percentage for the Preop method is lower than was reported by the same authors in a previous study,4 but higher than has been reported for the Scheimpflug device in a second study.14 Variability remains a concern with the Scheimpflug device,15 which may explain some of the larger differences between the IA and Preop calculations in the current study. The IA calculations produced a statistically significantly higher percentage of eyes with an expected residual cylinder of 0.50D or less relative to the Preop calculations, though the percentage of eyes with an expected residual cylinder of 0.50D or less was equivalent to that calculated for the Barrett Toric Calculator. Where Barrett and IA differed with regard to orientation angle, the IA measurement appeared more likely to be correct, though again this was not statistically significant. The use of IA in the pseudophakic eye to refine final orientation of the toric IOL may have been important in this regard. Finally, there was no evidence that IA could consistently prevent outliers (refractive surprises), but it did appear that there was a greater likelihood that IA was correct when IA and the other methods produced largely different calculations.
There are limitations to the current study. It was noted in the paper by Hill et al25 that the simulated calculation was always slightly worse than actual calculations; simulated results were systematically about 0.2D higher than the actual residual cylinder. This “remove and replace” technique appears to slightly favor the actual method used to determine the cylinder power. The current study included eyes where the majority of IOL implants were based on IA. This may result in an overstatement of the advantages of IA. One alternative to this approach is to conduct a prospective randomized study using contralateral eyes, but such a study would also have limitations. Other limitations include the fact that the study was retrospective in nature, and postoperative IOL orientation was not available to compare intended IOL orientation to actual orientation at the time of the refraction. For the latter comment, it can be stated that the literature indicates significant toric IOL misorientation is relatively rare.1
It is worth noting that for both sphere and cylinder, the highest percentage of eyes within 0.5D of the target was achieved with the Actual IOL implanted. This may be a result of the limitations in using a “remove and replace” methodology for analysis. However, it seems more likely that it reflects the fact that surgeon judgment related to the inputs from various devices remains an important deciding factor when choosing a toric IOL for surgery. Balanced against the use of measurements/calculations from various devices is the cost and time associated with collecting them from each device, and the cost of the devices.
Conclusion
In conclusion, modern IOL calculation formulas for sphere appear to produce results comparable to those achieved with IA. However, there may be some value in using IA to determine IOL cylinder power and orientation. This is most apparent when comparing results between IA and a preoperative method based on measured total corneal astigmatism. The relative benefit of IA is less apparent when results from the IA calculation are compared to those expected with the Barrett toric calculator. The consideration of both preoperative and IA toric IOL planning produced the best overall results in astigmatic eyes.
Acknowledgments
This research was supported with an investigator-initiated study grant (IIT#36913981) from Alcon (Ft. Worth, Texas, USA).
Disclosure
Dr James A Davison reports grants from Alcon, during the conduct of the study. Dr Sarah Makari reports grants from Alcon, during the conduct of the study and outside the submitted work. Dr Richard Potvin reports grants from Alcon, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Visser N, Bauer NJ, Nuijts RM. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg. 2013;39(4):624–637. doi:10.1016/j.jcrs.2013.02.020
2. Abulafia A, Koch DD, Wang L, et al. New regression formula for toric intraocular lens calculations. J Cataract Refract Surg. 2016;42(5):663–671. doi:10.1016/j.jcrs.2016.02.038
3. Gundersen KG, Potvin R. Clinical outcomes with toric intraocular lenses planned using an optical low coherence reflectometry ocular biometer with a new toric calculator. Clin Ophthalmol. 2016;10:2141–2147. doi:10.2147/OPTH.S120414
4. Davison JA, Potvin R. Refractive cylinder outcomes after calculating toric intraocular lens cylinder power using total corneal refractive power. Clin Ophthalmol. 2015;9:1511–1517. doi:10.2147/OPTH.S88693
5. Tonn B, Klaproth OK, Kohnen T. Anterior surface-based keratometry compared with Scheimpflug tomography-based total corneal astigmatism. Invest Ophthalmol Vis Sci. 2014;56(1):291–298. doi:10.1167/iovs.14-15659
6. Savini G, Næser K, Schiano-Lomoriello D, Ducoli P. Optimized keratometry and total corneal astigmatism for toric intraocular lens calculation. J Cataract Refract Surg. 2017;43(9):1140–1148. doi:10.1016/j.jcrs.2017.06.040
7. Klijn S, Reus NJ, van der Sommen CM, Sicam VA. Accuracy of total corneal astigmatism measurements with a Scheimpflug imager and a color light-emitting diode corneal topographer. Am J Ophthalmol. 2016;167:72–78. doi:10.1016/j.ajo.2016.04.011
8. Abulafia A, Hill WE, Franchina M, Barrett GD. Comparison of methods to predict residual astigmatism after intraocular lens implantation. J Refract Surg. 2015;31(10):699–707. doi:10.3928/1081597X-20150928-03
9. Ferreira TB, Ribeiro P, Ribeiro FJ, O’Neill JG. Comparison of astigmatic prediction errors associated with new calculation methods for toric intraocular lenses. J Cataract Refract Surg. 2017;43(3):340–347. doi:10.1016/j.jcrs.2016.12.031
10. Ferreira TB, Ribeiro P, Ribeiro FJ, O’Neill JG. Comparison of methodologies using estimated or measured values of total corneal astigmatism for toric intraocular lens power calculation. J Refract Surg. 2017;33(12):794–800. doi:10.3928/1081597X-20171004-03
11. Kern C, Kortüm K, Müller M, Kampik A, Priglinger S, Mayer WJ. Comparison of two toric IOL calculation methods. J Ophthalmol. 2018;2018:2840246. doi:10.1155/2018/2840246
12. Park DY, Lim DH, Hwang S, Hyun J, Chung TY. Comparison of astigmatism prediction error taken with the Pentacam measurements, Baylor nomogram, and Barrett formula for toric intraocular lens implantation. BMC Ophthalmol. 2017;17(1):156. doi:10.1186/s12886-017-0550-z
13. Fityo S, Bühren J, Shajari M, Kohnen T. Keratometry versus total corneal refractive power: analysis of measurement repeatability with 5 different devices in normal eyes with low astigmatism. J Cataract Refract Surg. 2016;42(4):569–576. doi:10.1016/j.jcrs.2015.11.046
14. Reitblat O, Levy A, Kleinmann G, Abulafia A, Assia EI. Effect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: comparison of methodologies. J Cataract Refract Surg. 2016;42(2):217–225. doi:10.1016/j.jcrs.2015.11.036
15. Galvis V, Tello A, Niño CA, Parra MM. Total corneal astigmatism measurement precision. Invest Ophthalmol Vis Sci. 2015;56(10):5912. doi:10.1167/iovs.15-17735
16. Davison JA, Potvin R. Preoperative measurement vs intraoperative aberrometry for the selection of intraocular lens sphere power in normal eyes. Clin Ophthalmol. 2017;11:923–929. doi:10.2147/OPTH.S135659
17. Hill DC, Sudhakar S, Hill CS, et al. Intraoperative aberrometry versus preoperative biometry for intraocular lens power selection in axial myopia. J Cataract Refract Surg. 2017;43(4):505–510. doi:10.1016/j.jcrs.2017.01.014
18. Cionni RJ, Dimalanta R, Breen M, Hamilton C. A large retrospective database analysis comparing outcomes of intraoperative aberrometry with conventional preoperative planning. J Cataract Refract Surg. 2018;44(10):1230–1235. doi:10.1016/j.jcrs.2018.07.016
19. Hatch KM, Woodcock EC, Talamo JH. Intraocular lens power selection and positioning with and without intraoperative aberrometry. J Refract Surg. 2015;31(4):237–242. doi:10.3928/1081597X-20150319-03
20. Woodcock MG, Lehmann R, Cionni RJ, Breen M, Scott MC. Intraoperative aberrometry versus standard preoperative biometry and a toric IOL calculator for bilateral toric IOL implantation with a femtosecond laser: one-month results. J Cataract Refract Surg. 2016;42(6):817–825. doi:10.1016/j.jcrs.2016.02.048
21. Potvin R, Kramer BA, Hardten DR, Berdahl JP. Factors associated with residual astigmatism after toric intraocular lens implantation reported in an online toric intraocular lens back-calculator. J Refract Surg. 2018;34(6):366–371. doi:10.3928/1081597X-20180327-01
22. Stringham J, Pettey J, Olson RJ. Evaluation of variables affecting intraoperative aberrometry. J Cataract Refract Surg. 2012;38(3):470–474. doi:10.1016/j.jcrs.2011.09.039
23. Masket S, Fram NR, Holladay JT. Influence of ophthalmic viscosurgical devices on intraoperative aberrometry. J Cataract Refract Surg. 2016;42(7):990–994. doi:10.1016/j.jcrs.2016.04.022
24. Hoffer KJ, Savini G. IOL power calculation in short and long eyes. Asia Pac J Ophthalmol (Phila). 2017;6(4):330–331. doi:10.22608/APO.2017338
25. Hill W, Osher R, Cooke D, et al. Simulation of toric intraocular lens results: manual keratometry versus dual-zone automated keratometry from an integrated biometer. J Cataract Refract Surg. 2011;37(12):2181–2187. doi:10.1016/j.jcrs.2011.06.028
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.