Back to Journals » Clinical Interventions in Aging » Volume 20
Clinical Value of Nutritional Assessment Tools in Older Adults with Chronic Obstructive Pulmonary Disease: An Integrative Review
Received 25 July 2025
Accepted for publication 2 December 2025
Published 24 December 2025 Volume 2025:20 Pages 2671—2683
DOI https://doi.org/10.2147/CIA.S556215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Maddalena Illario
Xiaoqin Hao, Tiansheng Bu
Department of Traditional Chinese Medicine, The Third Affiliated Hospital of Gansu University of Chinese Medicine, Baiyin, Gansu, People’s Republic of China
Correspondence: Tiansheng Bu, Department of Traditional Chinese Medicine, The Third Affiliated Hospital of Gansu University of Chinese Medicine, Baiyin, Gansu, People’s Republic of China, Email [email protected]
Abstract: Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory disorder frequently observed in older adults and is often accompanied by aging-related conditions such as sarcopenia, cognitive impairment, and immune dysfunction. Malnutrition is a major yet underrecognized contributor to poor outcomes in this population, accelerating disease progression and functional decline. This integrative review critically examines the clinical value of three widely used nutritional assessment tools—the Mini Nutritional Assessment (MNA), the Patient-Generated Subjective Global Assessment (PG-SGA), and the Nutritional Risk Screening 2002 (NRS-2002)—in identifying malnutrition and guiding targeted interventions for older adults with COPD. A systematic literature search was conducted in PubMed, Embase, and Web of Science databases for studies published between 2010 and 2025, using combinations of the keywords COPD, older adults, malnutrition, and nutritional assessment tools. Studies addressing both nutritional screening (risk detection) and nutritional assessment (comprehensive evaluation) were included to clarify their conceptual and practical distinctions. Findings indicate that while all three tools are useful for detecting nutritional risk, their sensitivity, specificity, and clinical applicability differ across settings. The MNA is most suitable for community and outpatient populations, the PG-SGA offers comprehensive evaluation for hospitalized or comorbid patients, and the NRS-2002 is effective for early inpatient screening and prognosis prediction. Integrating these tools into multidisciplinary COPD management enables early identification of malnutrition, sarcopenia, and immune dysfunction, supporting timely, personalized nutrition interventions. Future research should focus on standardizing tool selection, incorporating biomarkers and digital health technologies, and exploring AI-assisted assessments to enhance precision and applicability in diverse clinical contexts. This review underscores that routine nutritional assessment is not merely supportive care but an essential component of precision management for older adults with COPD.
Keywords: COPD, malnutrition, nutritional assessment tools, aging-related diseases, sarcopenia, cognitive decline
Introduction
COPD is one of the leading causes of morbidity and mortality globally, with an increasing prevalence in the older adult population. COPD is characterized by persistent airflow limitation, which is typically progressive and results from an abnormal inflammatory response of the lungs to harmful particles or gases. The older adult population is particularly vulnerable to COPD, as they often experience comorbid conditions, including sarcopenia, cognitive decline, and immune dysfunction, which can complicate the management and prognosis of the disease.1,2 These aging-related diseases are not only common in COPD patients but also exacerbate disease outcomes, leading to poorer health and quality of life.3
Aging itself is associated with several physiological changes that increase the risk of multiple diseases, including those affecting the musculoskeletal, cognitive, and immune systems. Sarcopenia, defined as the progressive loss of skeletal muscle mass and strength, is highly prevalent in older adult COPD patients, impairing their ability to perform daily activities and leading to worse clinical outcomes.4,5 Similarly, cognitive decline, which includes both mild cognitive impairment and more severe forms such as dementia, is frequently observed in this patient group and is associated with higher mortality and increased hospitalization.6,7 Additionally, immune aging, which manifests as a decline in immune function, significantly increases the vulnerability of older adult COPD patients to infections and delays their recovery from exacerbations.8,9 The role of nutrition in aging is critical, influencing both the progression of age-related diseases and the severity of COPD. Malnutrition, which is particularly common in older adult COPD patients, has been associated with worsened disease outcomes, including more frequent exacerbations, longer hospital stays, and increased mortality.10,11 Moreover, malnutrition can accelerate the aging process itself, exacerbating muscle wasting and immune dysfunction, and leading to a vicious cycle that worsens both aging and COPD progression.12 Hence, it is crucial to assess and monitor the nutritional status of older adult COPD patients to prevent further deterioration and optimize treatment outcomes.13
Despite extensive evidence linking malnutrition to poor COPD outcomes, the distinction between nutritional screening and nutritional assessment is often overlooked in the literature. Nutritional screening tools aim for rapid identification of patients at risk of malnutrition, whereas nutritional assessment tools provide a more comprehensive evaluation of nutritional status, etiology, and intervention needs.14,15 Failure to distinguish between these approaches may obscure their respective clinical roles and limit the precision of nutritional care in COPD management.
In clinical practice and research, several validated instruments are commonly used to evaluate nutrition in COPD, including the Mini Nutritional Assessment (MNA), the Patient-Generated Subjective Global Assessment (PG-SGA), and the Nutritional Risk Screening 2002 (NRS-2002).16–19 Each of these tools differs in structure, scoring system, and clinical applicability. For instance, the MNA is widely used in community-dwelling older adults; the PG-SGA offers a multidimensional clinical assessment suitable for hospitalized or multimorbid patients; and the NRS-2002 provides a standardized approach to identifying nutritional risk in acute care settings.20–23 However, previous reviews have primarily described the general relationship between COPD and nutrition, rather than comparing the diagnostic accuracy, strengths, and limitations of these tools in older adults.23–25
Therefore, this paper aims to conduct an integrative review of recent evidence to: (1) clarify the conceptual distinction between nutritional screening and assessment; (2) compare the clinical value, sensitivity, specificity, and limitations of major nutritional assessment tools (MNA, PG-SGA, NRS-2002) in COPD; and (3) explore how integrating these tools into multidisciplinary care can improve early detection, guide personalized nutrition interventions, and enhance outcomes for older adults with COPD.26–28 By synthesizing updated research, this review provides a structured framework for selecting appropriate nutritional tools and highlights their essential role in precision management of COPD in aging populations.
The Relationship Between COPD and Aging
COPD is a progressive respiratory disorder that not only affects lung function but also accelerates the aging process in various physiological systems. Aging and COPD share multiple overlapping mechanisms, including chronic inflammation, oxidative stress, and cellular senescence, which together amplify systemic deterioration in older adults.16,29 This section discusses the specific aging features observed in older COPD patients, outlines the biological mechanisms of aging, and explores the bidirectional interaction between aging and COPD, demonstrating how aging exacerbates COPD and how COPD, in turn, accelerates aging.
Aging Features in COPD
Older adults with COPD exhibit several aging-related characteristics that contribute to the complexity of disease management. Sarcopenia—the age-related loss of muscle mass and function—is highly prevalent in COPD patients and significantly worsens outcomes. Studies have shown that sarcopenia is more severe in COPD than in age-matched healthy populations, largely due to systemic inflammation, hypoxia, and reduced physical activity induced by the disease.17–19,30 Sarcopenia not only impairs physical endurance but also weakens respiratory muscles, thereby intensifying dyspnea and functional decline. It is associated with reduced muscle strength, lower physical activity levels, and increased frailty, leading to poorer quality of life and greater mortality risk.21
In addition to musculoskeletal decline, cognitive dysfunction is another hallmark of aging in COPD. Cognitive impairment—including both mild cognitive impairment (MCI) and dementia—is more pronounced in COPD patients compared with individuals of similar age without pulmonary disease. Chronic hypoxemia, systemic inflammation, and cerebral microvascular injury have been identified as key contributors to this decline.22–24 As a result, cognitive deficits can interfere with treatment adherence and self-management, further worsening clinical prognosis.
Immune aging, or immunosenescence, is another crucial dimension of the aging phenotype in COPD. The combined effect of COPD-related inflammation and age-induced immune dysregulation increases susceptibility to infections, delays recovery from exacerbations, and contributes to chronic comorbidities. Impaired T-cell function, reduced B-cell responsiveness, and altered cytokine signaling all play roles in the heightened infection risk and delayed wound healing observed in older adults COPD populations.25,27,31
Biological Mechanisms of Aging
The biological mechanisms underlying the relationship between COPD and aging are multifactorial. Both conditions are characterized by sustained oxidative stress, mitochondrial dysfunction, and low-grade systemic inflammation, collectively known as “inflammaging”.28,32,33 In COPD, chronic exposure to cigarette smoke, pollutants, and inflammatory mediators leads to increased production of reactive oxygen species (ROS). These molecules damage lipids, proteins, and DNA, thereby accelerating cellular senescence and impairing tissue regeneration.34
Chronic inflammation serves as a central pathogenic bridge between COPD and aging. Proinflammatory cytokines such as IL-6, TNF-α, and CRP are persistently elevated in COPD and also represent key biomarkers of biological aging.35–37 This systemic inflammation extends beyond the lungs to affect skeletal muscle, cardiovascular, and neural tissues, thereby promoting sarcopenia, frailty, and neurodegeneration.38–40
Cellular senescence—the permanent arrest of cell division—further exacerbates tissue dysfunction in both COPD and aging. Senescent cells accumulate in the lungs and other organs, secreting proinflammatory and matrix-degrading factors known as the senescence-associated secretory phenotype (SASP). This creates a self-perpetuating cycle of inflammation, impaired repair capacity, and structural decline.41,42 The accumulation of senescent alveolar and epithelial cells also disrupts tissue homeostasis, accelerating lung remodeling and functional deterioration.
The Bidirectional Relationship Between Aging and COPD
The relationship between aging and COPD is bidirectional and synergistic. Aging accelerates COPD progression through cumulative exposure to environmental stressors, immune exhaustion, and diminished regenerative capacity. Age-related structural changes—such as loss of lung elastic recoil, decreased alveolar surface area, and impaired mucociliary clearance—reduce pulmonary resilience and predispose individuals to chronic airflow limitation.43,44
Conversely, COPD acts as a model of accelerated aging, as the chronic inflammatory burden and oxidative stress associated with the disease induce premature aging in multiple organ systems. COPD-related systemic inflammation increases circulating inflammatory mediators, which in turn amplify aging hallmarks in skeletal muscles, cardiovascular tissues, and the central nervous system.45–47 Additionally, physical inactivity caused by dyspnea and fatigue reinforces sarcopenia and frailty, perpetuating a vicious cycle of decline.48,49
This mutual reinforcement between aging and COPD highlights the need for comprehensive management strategies that integrate nutritional assessment, physical rehabilitation, and anti-inflammatory interventions. Understanding the shared biological mechanisms provides the foundation for targeted therapies that address both pulmonary dysfunction and systemic aging processes in older adults with COPD.
Nutritional Assessment Tools and Their Application in Aging-Related Diseases
Nutritional assessment tools play a pivotal role in identifying malnutrition and nutritional risks, particularly in older adults with chronic diseases such as COPD. These instruments are essential for detecting early signs of aging-related diseases, including sarcopenia, cognitive decline, and immune system deterioration. However, a clear conceptual distinction must be made between nutritional screening and nutritional assessment. Screening tools such as the NRS-2002 are used to rapidly detect individuals at risk of malnutrition, while assessment tools such as the MNA and PG-SGA provide a more comprehensive evaluation of nutritional status, etiology, and intervention needs.35–39
Accurate classification of these instruments is critical for clinical decision-making. Misuse or interchange of screening and assessment tools, as often seen in COPD studies, can lead to misinterpretation of patient needs and inappropriate nutritional interventions.40,41 Therefore, understanding the structure, scoring principles, and limitations of each tool is essential to optimize patient outcomes.
Major Nutritional Assessment Tools
Several standardized tools have been developed to assess the nutritional status of older adults. Among the most widely used are the Mini Nutritional Assessment (MNA), the Patient-Generated Subjective Global Assessment (PG-SGA), and the Nutritional Risk Screening 2002 (NRS-2002).
The MNA is one of the most widely applied and validated nutritional assessment instruments for older populations. It consists of 18 items evaluating BMI, recent weight loss, dietary intake, and functional capacity. The inclusion of psychosocial and mobility factors provides an advantage in identifying frail community-dwelling older adults with early signs of nutritional risk.35,36 However, it may overestimate malnutrition risk in acutely ill or hospitalized patients because it does not sufficiently account for disease-related metabolic stress.37
The PG-SGA offers a more comprehensive evaluation by combining subjective and objective parameters, including patient-reported weight loss, appetite, functional status, and clinical findings. Originally designed for oncology patients, it has since been validated in COPD and other chronic diseases.37,38 The PG-SGA provides greater clinical flexibility and can capture disease-specific metabolic alterations, but its complexity requires trained professionals and may limit use in high-volume clinical settings.
The NRS-2002 is primarily a nutritional screening tool, developed for hospitalized patients. It assesses nutritional risk by integrating BMI, recent weight loss, and disease severity.39 NRS-2002 is particularly effective in identifying patients who would benefit from early nutritional support, especially during acute COPD exacerbations. Nonetheless, it focuses mainly on short-term risk detection rather than comprehensive nutritional evaluation, and its use in long-term care remains limited.40
In clinical research and practice, the combined application of screening and assessment instruments—using NRS-2002 for initial risk identification followed by MNA or PG-SGA for detailed assessment—provides a balanced strategy for both early detection and comprehensive evaluation.
Nutritional Assessment and Its Association with Aging-Related Diseases
Malnutrition and nutritional risk are closely associated with the development and progression of aging-related diseases, especially in older adults with COPD. As summarized in Table 1, nutritional assessment–guided interventions targeting sarcopenia, cognitive decline, and immune dysfunction are associated with distinct mechanistic pathways and clinically meaningful outcomes in older adults with COPD. As illustrated in Figure 1, malnutrition acts as a central driver linking sarcopenia, cognitive impairment, and immune dysfunction in older adults with COPD, while targeted nutritional interventions can interrupt these interconnected pathological pathways. Accurate nutritional assessment can predict the onset and severity of sarcopenia, cognitive impairment, and immune dysfunction.40–43
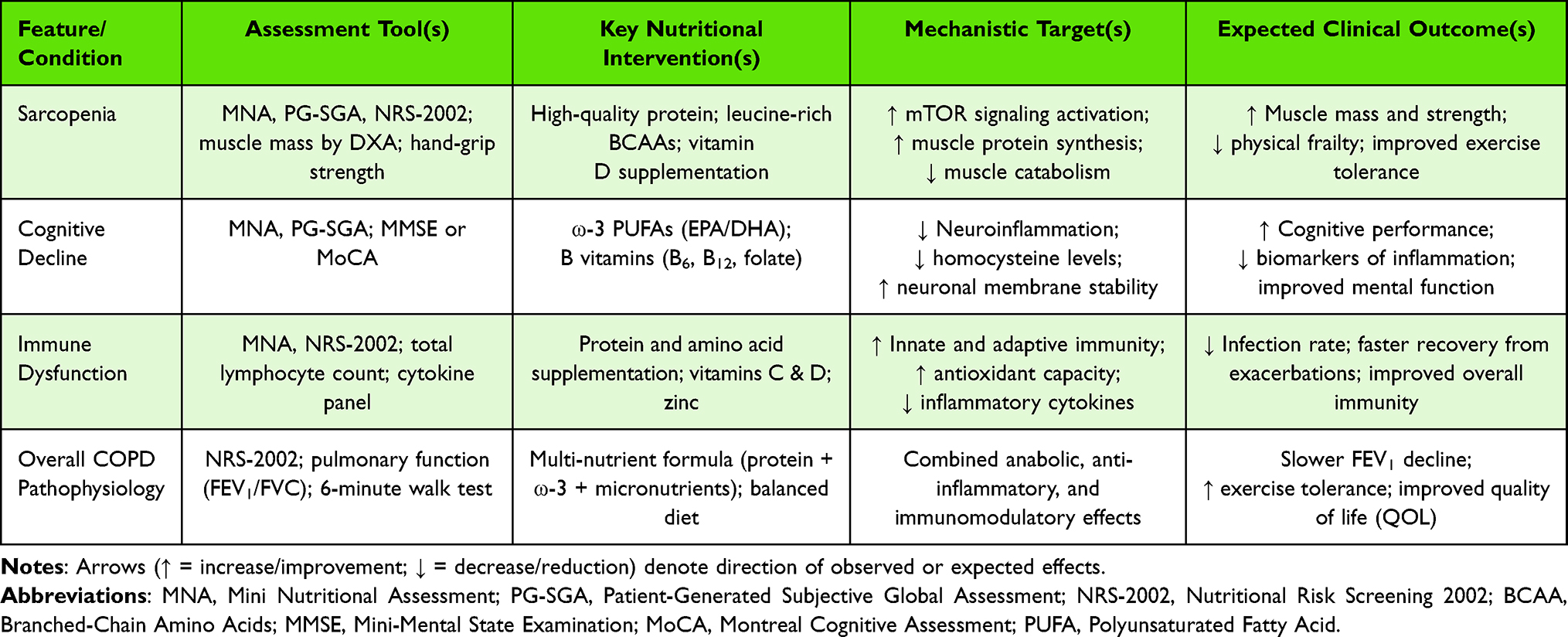 |
Table 1 Summary of Research Aims, Nutritional Interventions, Assessments, and Key Findings in Older Adults COPD Patients |
 |
Figure 1 Schematic of the interactions between malnutrition and age-related conditions in older adults with COPD, and the mechanisms of nutritional interventions. Malnutrition exacerbates sarcopenia, cognitive decline, and immune dysfunction. Supplementation with dietary protein, ω-3 fatty acids, and essential vitamins and minerals can improve muscle mass, enhance cognitive performance, and optimize immune responses, thereby mitigating COPD-related pathology. |
Sarcopenia represents one of the most clinically significant manifestations of nutritional deterioration. Nutritional deficiencies—particularly low protein and vitamin D intake—accelerate muscle loss in older adults. MNA and PG-SGA scores correlate strongly with muscle mass and grip strength, serving as early indicators of sarcopenia.44,50 In COPD, sarcopenia worsens respiratory muscle weakness and exercise intolerance, underscoring the importance of integrating nutrition-focused physical assessments into standard care.
Cognitive decline in older COPD patients is influenced by both hypoxia and nutritional insufficiency. Deficiencies in B vitamins and omega-3 fatty acids contribute to neuronal damage and cognitive impairment. MNA and PG-SGA can indirectly capture this risk through appetite, dietary intake, and weight change indicators.46,47 Malnourished COPD patients show a higher prevalence of cognitive dysfunction, suggesting that timely nutritional assessment may also serve as a preventive approach against neurodegeneration.48
Immune dysfunction is another critical concern. Aging and COPD both impair immune response, a process exacerbated by micronutrient deficiencies such as zinc, vitamin D, and antioxidants. Nutritional assessment tools enable clinicians to detect these deficiencies early and introduce targeted supplementation, thereby reducing infection risk and COPD exacerbations.49
Clinical Implications and Future Perspectives
The choice of nutritional assessment tool should depend on the clinical context and patient condition. For community or outpatient settings, the MNA offers a holistic and practical approach. For hospitalized or multimorbid patients, the PG-SGA provides a detailed evaluation that integrates disease-specific parameters. In acute or short-stay units, the NRS-2002 allows rapid identification of patients requiring early nutritional support.
Incorporating structured nutritional assessment into multidisciplinary COPD care—alongside pulmonary rehabilitation, exercise therapy, and pharmacological management—can substantially improve patient survival, physical performance, and quality of life.40,41,48
Despite these advantages, several limitations remain. The predictive accuracy of existing tools varies across populations, comorbidities, and cultural dietary patterns. Most tools were developed and validated in Western settings, limiting their cross-cultural applicability.51 Moreover, inconsistent administration and subjective scoring can lead to variability among assessors, particularly with the PG-SGA. The absence of standardized guidelines specifying when and how to use these instruments in COPD pathways also restricts their integration into routine practice.
Future studies should aim to validate these tools in diverse clinical and demographic settings and incorporate emerging technologies for precision assessment. Biomarker-based and imaging-supported indicators such as inflammatory profiles and muscle mass scanning could enhance diagnostic accuracy.52 The integration of artificial intelligence (AI) and electronic health records (EHRs) offers promising opportunities for automated nutritional screening, personalized interventions, and continuous monitoring.53 Establishing standardized clinical protocols that link nutritional assessment outcomes with actionable treatment pathways will help ensure the full clinical utility of these tools.
By combining evidence-based nutritional evaluation with technological innovation, clinicians can move toward more personalized, preventive, and effective COPD management for older adults.
The Impact of Nutritional Intervention on Aging in Older Adults COPD Patients
Nutritional interventions are increasingly recognized for their potential to mitigate the effects of aging-related diseases in older adults with COPD. Because malnutrition and nutritional deficiencies are highly prevalent in this population, timely and targeted interventions can significantly improve outcomes and slow the progression of sarcopenia, cognitive decline, and immune dysfunction. Importantly, these interventions should be guided by validated nutritional assessment tools (eg: MNA, PG-SGA, NRS-2002), rather than simple screening checklists, to ensure precise identification of patients’ needs and to individualize treatment plans.39,54
Nutritional Intervention and Sarcopenia
Sarcopenia, characterized by progressive loss of muscle mass and function, is one of the most debilitating age-related conditions among older COPD patients. It leads to frailty, decreased physical performance, and higher mortality rates. Nutritional interventions—especially high-protein diets and vitamin D supplementation—have demonstrated strong benefits in alleviating sarcopenia symptoms in this group. High-protein intake supports muscle protein synthesis and enhances respiratory muscle strength, which is often compromised in COPD.48,55 Combined with resistance training, protein supplementation helps preserve lean body mass and improve exercise capacity.49,50
Vitamin D supplementation also plays a critical role by improving calcium metabolism, reducing inflammatory cytokine expression, and enhancing muscle contractility.49 Studies have shown that restoring vitamin D levels improves muscle strength and physical performance, while simultaneously mitigating the chronic inflammation associated with COPD.28,48
Nutritional Intervention and Cognitive Function
Cognitive decline is a common comorbidity in older COPD patients, leading to poor treatment adherence and diminished quality of life. Specific nutrients such as omega-3 fatty acids and B vitamins have been shown to improve or preserve cognitive performance. Omega-3 polyunsaturated fatty acids (PUFAs) exert anti-inflammatory and neuroprotective effects, which help reduce systemic and neural inflammation in COPD.56,57 Clinical studies indicate that omega-3 supplementation enhances brain function and mood while slowing cognitive deterioration.58
Similarly, B-vitamin supplementation—particularly folate, B6, and B12—has been found to reduce homocysteine levels, a key biomarker linked to cognitive impairment and dementia.47,59,60 Maintaining adequate B-vitamin levels in older adults with COPD may therefore help attenuate cognitive decline and improve daily functioning.60
Nutritional Intervention and Immune Aging
Immune dysfunction, or immune senescence, is another hallmark of aging that is particularly prominent in COPD. Nutritional deficiencies weaken immune responses and increase vulnerability to infections. Protein and amino acid supplementation—especially arginine, glutamine, and branched-chain amino acids (BCAAs)—enhances immune cell activity and promotes recovery from infection.56,61
Micronutrients such as vitamins A, C, D, and zinc are also crucial for maintaining innate and adaptive immunity. Vitamin D modulates immune signaling pathways, while zinc supports cytokine production and antioxidant defense mechanisms.44,54 Recent studies have confirmed that optimizing micronutrient intake improves immune resilience, reduces infection rates, and shortens hospitalization among older adults with COPD.43,62
Furthermore, emerging evidence supports the use of probiotics and prebiotics to regulate gut microbiota, thereby improving systemic immunity and reducing COPD-related inflammation. These findings collectively highlight that effective nutritional interventions—guided by structured assessment tools—can substantially reduce the burden of aging-related complications in COPD.
Emerging Research and Clinical Applications of Nutritional Assessment Tools
Nutritional assessment tools have gained increasing attention for their ability to improve health outcomes in older adults with COPD. These tools provide a systematic approach to identifying malnutrition and its associated risks, including aging-related complications such as sarcopenia, cognitive decline, and immune dysfunction. Importantly, recent evidence emphasizes that effective nutritional intervention depends not only on screening for risk but also on conducting comprehensive nutritional assessments to guide individualized treatment plans.35,37,39
Recent Research Findings
Several recent studies have underscored the importance of nutritional assessment in the management of older COPD patients. Early identification of malnutrition using validated instruments—such as the MNA, the PG-SGA, and the NRS-2002—can substantially enhance patient outcomes by allowing for early, targeted interventions.
For example, Kaiser et al demonstrated that MNA scores are closely correlated with the risk of hospitalization, exacerbations, and mortality among older adults with COPD.35 The PG-SGA, combining subjective symptoms with objective anthropometric and clinical data, has proven especially valuable for detecting malnutrition in patients with multiple chronic conditions, including COPD.63 Meanwhile, the NRS-2002 effectively predicts poor outcomes and prolonged hospital stays by integrating disease severity and nutritional risk.
Beyond these traditional measures, recent studies advocate for a comparative use of multiple assessment tools to improve accuracy and clinical applicability. For instance, integrating NRS-2002 with biomarkers such as C-reactive protein (CRP) enhances predictive capacity for systemic inflammation—a major driver of both COPD progression and aging-related comorbidities.64 This aligns with the view that malnutrition, inflammation, and aging are interdependent processes requiring multidimensional diagnostic frameworks.34
Clinical Application and Challenges
Despite the strong evidence supporting these tools, their implementation in everyday clinical practice remains inconsistent. Common barriers include limited clinician training, time constraints, and the absence of standardized protocols across healthcare systems.51,63 The PG-SGA, for example, requires professional judgment to interpret subjective components, which may lead to inter-observer variability. Similarly, while the MNA is simple to administer, it may not capture disease-specific risks relevant to COPD populations.65
To address these issues, recent guidelines encourage interdisciplinary integration, bringing together dietitians, pulmonologists, and geriatricians to ensure consistent nutritional evaluation and intervention.37,66 Digital innovations are also reshaping clinical applications: embedding nutritional assessment modules into electronic health records (EHRs) or mobile platforms has been shown to improve accessibility and reduce time burden for clinicians.53,67 Such digitalization not only facilitates real-time data monitoring but also supports longitudinal tracking of patient outcomes.
Discussion and Future Directions
Nutritional assessment tools have become an integral component of managing older adults with COPD. They provide valuable insights into nutritional risks and aging-related comorbidities, such as sarcopenia, cognitive impairment, and immune dysfunction. However, despite growing recognition of their value, several conceptual and practical limitations persist, constraining their clinical utility. This section outlines current challenges, proposes targeted improvements, and highlights future research directions aimed at enhancing the precision, applicability, and technological integration of these tools.
Limitations and Challenges of Nutritional Assessment Tools
Current nutritional assessment tools—such as MNA, PG-SGA, and NRS-2002—were primarily developed for general older adults or hospitalized populations rather than disease-specific cohorts. Consequently, their cultural adaptability and disease specificity remain limited.51,52 For example, dietary patterns in Eastern populations, which often emphasize plant-based or herbal diets, are not fully reflected in Western-developed instruments. This may lead to misclassification of nutritional risk in older adults with COPD from non-Western contexts.66
In addition, individual variability complicates interpretation. COPD patients commonly present with multiple comorbidities (eg, diabetes, cardiovascular disease) that alter nutritional requirements and metabolism.19,67 Existing tools do not account for such dynamic, disease-specific needs, nor for the interactions between malnutrition, systemic inflammation, and physical deconditioning.34,65 Moreover, many assessment instruments rely on subjective measures (eg, appetite, weight change), which are susceptible to recall bias or inconsistent reporting by patients.37,51,63
Practical barriers also hinder implementation. Some tools, such as the PG-SGA, demand trained personnel for accurate scoring and interpretation—resources not always available in high-volume clinical settings.63 Furthermore, absence of standardized clinical pathways leads to inconsistent usage across institutions, undermining comparability and reproducibility of results.65
Future Research Directions
To overcome these limitations, technological innovation and personalized medicine approaches represent key avenues for advancement.
First, AI and machine learning (ML) offer promising solutions for automating nutritional risk prediction. By integrating large-scale datasets—spanning demographics, comorbidities, biomarker profiles, and lifestyle factors—AI systems can identify subtle patterns not captured by conventional assessment methods.53,67 These predictive algorithms could generate personalized nutrition risk scores, providing clinicians with real-time, evidence-based decision support.
Second, future research should focus on integrating multiple complementary tools into unified diagnostic frameworks. Combining subjective assessments (eg, MNA, PG-SGA) with objective indicators such as bioelectrical impedance analysis (BIA) or computed tomography-based muscle quantification can improve the sensitivity and specificity of malnutrition and sarcopenia detection.19,59 This multimodal approach will provide a more holistic picture of nutritional health, capturing both biological and behavioral dimensions.
Third, digital health platforms hold great potential for enhancing accessibility and adherence. Embedding assessment tools into electronic health records (EHRs) or mobile applications allows longitudinal monitoring of patient nutrition status, dietary adherence, and treatment outcomes. Remote tracking through wearable devices may further support early intervention, especially for patients with limited mobility or those in long-term home care.
Finally, the integration of nutritional assessment into multidisciplinary care teams—including dietitians, pulmonologists, geriatricians, and rehabilitation specialists—will be crucial for ensuring continuity of care. Such models enable coordinated interventions that address both physiological and psychosocial aspects of malnutrition, thereby improving clinical outcomes and quality of life for older COPD patients.66
Clinical Significance and Intervention Strategies
In clinical practice, comprehensive nutritional assessment provides more than diagnostic information—it serves as a strategic intervention point for personalized care. Identifying patients at early risk of malnutrition allows clinicians to initiate targeted therapies, such as high-protein supplementation, micronutrient replacement, and anti-inflammatory dietary interventions.43,47,49 These strategies can delay disease progression, reduce exacerbation frequency, and enhance independence and daily functioning.
Future development should prioritize standardization, personalization, and integration. Establishing COPD-specific nutritional assessment criteria based on international consensus52 will enhance diagnostic consistency. Personalized intervention algorithms that leverage AI-driven insights could then translate these assessments into adaptive treatment plans.
Ultimately, advancing the field requires bridging the gap between nutritional science, gerontology, and digital health. By uniting these domains, clinicians will be better equipped to deliver precision nutrition care that mitigates the dual burden of COPD and aging, promoting longevity and functional resilience in older adults.19,67
Conclusion
The significance of nutritional assessment tools in the management of older adults with COPD is increasingly recognized in both clinical research and practice. These tools provide valuable insights into the nutritional status of patients, offering an effective means of identifying those at risk of malnutrition and aging-related diseases, such as sarcopenia, cognitive decline, and immune dysfunction. Importantly, a clear distinction should be maintained between nutritional screening—a rapid identification of risk—and nutritional assessment, which provides a comprehensive evaluation of nutritional status and guides intervention planning. As highlighted throughout this paper, early detection and timely intervention, driven by accurate nutritional assessments, can profoundly improve outcomes for older COPD patients by addressing both disease progression and aging-related comorbidities.
Summary of Findings
This review has highlighted the critical role of nutritional assessment tools in managing the health of older COPD patients. Tools such as the MNA, PG-SGA, and NRS-2002 provide reliable means of detecting malnutrition, sarcopenia, and other aging-related conditions, allowing for early intervention. Current evidence indicates that these instruments—when applied appropriately—can guide personalized nutritional interventions that mitigate the impact of aging-related diseases. Specifically, interventions such as high-protein diets, vitamin D supplementation, omega-3 fatty acids, and B vitamins have been shown to improve muscle strength, cognitive function, and immune health, thereby enhancing overall quality of life and reducing the burden of COPD exacerbations. Furthermore, integrating these tools into clinical practice, especially when combined with biomarkers and functional indicators, enhances their predictive accuracy and clinical utility.19,66,67
Clinical Implications
The practical implications of these findings are significant for clinical care. Incorporating nutritional screening and assessment tools into routine COPD management allows healthcare providers to detect nutritional deficiencies and aging-related risks that may not be apparent through standard clinical evaluation. Early identification enables targeted and evidence-based nutritional interventions that address both malnutrition and the underlying aging mechanisms contributing to disease progression. This approach improves patient outcomes by not only enhancing nutritional status but also slowing the progression of sarcopenia, cognitive decline, and immune dysfunction.
Moreover, personalized, tool-guided interventions enable clinicians to tailor treatment plans to the specific needs of each patient. This personalized care approach is particularly important in older COPD patients with complex comorbidities. The integration of multidisciplinary care teams—including dietitians, pulmonologists, and geriatricians—ensures that nutritional assessments lead to actionable interventions. In practice, this can help reduce hospitalization rates, improve functional independence, and enhance overall patient satisfaction.41,68
Future Outlook
Looking ahead, the future development of nutritional assessment tools and personalized interventions in aging and COPD management holds significant promise. One of the most exciting prospects is the integration of AI and machine learning into nutritional assessment tools. AI has the potential to analyze vast amounts of patient data, such as demographics, clinical history, and biomarkers, to predict individualized nutritional risks with greater precision. This would enable healthcare providers to deliver even more personalized and effective interventions, particularly for older adults COPD patients who may be at risk for multiple comorbidities and aging-related diseases.69
Furthermore, there is potential for digital health technologies to enhance the implementation and accessibility of nutritional assessments. Mobile health applications and wearable devices could be used to track patients’ nutritional intake, physical activity, and other relevant metrics in real time. These technologies can provide both patients and healthcare providers with continuous feedback, improving patient engagement and adherence to nutritional interventions.70
In addition to technological advancements, future research should focus on multi-dimensional approaches that integrate several assessment tools, biomarkers, and imaging techniques. This would create a more comprehensive picture of a patient’s nutritional status and aging-related diseases, allowing for even earlier and more accurate interventions. Moreover, the inclusion of patient-reported outcomes and subjective measures alongside objective data can improve the overall effectiveness of these assessments, leading to better clinical decision-making.52
Overall, the future of nutritional assessment tools in older adults COPD management looks promising. By advancing these tools and integrating them with personalized and technology-driven approaches, healthcare providers will be better equipped to manage the complex needs of older adults patients, improving both their longevity and quality of life.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li N, Wang W, Lv Y, et al. The impact of case management on elderly patients with chronic obstructive pulmonary disease. Int J Chronic Obstr. 2025;20:1407–1417. doi:10.2147/COPD.S517564
2. Atchley W, Montgomery A, Seth R, et al. Navigating COPD in aging populations: insights into pathophysiology and comprehensive care. Semin Resp Crit Care Med. 2024;45(5):560–573. doi:10.1055/s-0044-1792112
3. Zhong S, Yang L, Liu N, et al. Identification and validation of aging-related genes in COPD based on bioinformatics analysis. Aging. 2022;14(10):4336–4356. doi:10.18632/aging.204064
4. Mollica M, Aronne L, Paoli G, et al. Elderly with COPD: comoborbitidies and systemic consequences. J Gerontol Geriatrics. 2020;69(1):32–44. doi:10.36150/2499-6564-434
5. Xia S, Zhou C, Kalionis B, et al. Combined antioxidant, anti-inflammaging and mesenchymal stem cell treatment: a possible therapeutic direction in elderly patients with chronic obstructive pulmonary disease. Aging Dis. 2020;11(1):129–140. doi:10.14336/AD.2019.0508
6. Wang T, Mao L, Wang J, et al. Influencing factors and exercise intervention of cognitive impairment in elderly patients with chronic obstructive pulmonary disease. Clin Interventions Aging. 2020;15:557–566. doi:10.2147/CIA.S245147
7. Wei Y, Giunta S, Xia S. Hypoxia in aging and aging-related diseases: mechanism and therapeutic strategies. Int J Mol Sci. 2022;23:8165.
8. Divo M, Celli B, Poblador-Plou B, et al. Chronic obstructive pulmonary disease (COPD) as a disease of early aging: evidence from the EpiChron cohort. PLoS One. 2018;13(2). doi:10.1371/journal.pone.0193143
9. Valério M, Sá PC, Rodrigues D, et al. Accelerated aging mechanisms in chronic obstructive pulmonary disease. Front Med Technol. 2021;3. doi:10.3389/fmedt.2021.649506
10. Gao H, Cheng X, Zuo X, et al. Exploring the impact of adequate energy supply on nutrition, immunity, and inflammation in elderly patients with chronic obstructive pulmonary disease. Int J Chronic Obstr. 2024;19:1391–1402. doi:10.2147/COPD.S450209
11. Bodrug N. Clinical features of chronic obstructive pulmonary disease in the elderly. Bulletin Acad Sci Moldova Med Sci. 2022;71(3):72–77. doi:10.52692/1857-0011.2021.3-71.33
12. Tayutina T, Bagmet A, Lysenko A, et al. The risk factors studying for chronic obstructive pulmonary disease development in non-smoking elderly patients. Adv Gerontol. 2022;35(3):361–367.
13. Zhao Y, Wu Z. TROP2 promotes PINK1-mediated mitophagy and apoptosis to accelerate the progression of senile chronic obstructive pulmonary disease by up-regulating DRP1 expression. Exp Gerontology. 2024;191:112441. doi:10.1016/j.exger.2024.112441
14. Fotokian Z, Mohammadi Shahboulaghi F, Fallahi-Khoshknab M, et al. The empowerment of elderly patients with chronic obstructive pulmonary disease: managing life with the disease. PLoS One. 2017;12(4):e0174028. doi:10.1371/journal.pone.0174028
15. Lopes AJ, Vigário PS, Hora AL, et al. Ventilation distribution, pulmonary diffusion and peripheral muscle endurance as determinants of exercise intolerance in elderly patients with chronic obstructive pulmonary disease. Physiol Res. 2018;67(6):863–874. doi:10.33549/physiolres.933867
16. Wang CJ, Leung JM, Sin DD. A tale as old as time - the importance of accelerated lung aging in chronic obstructive pulmonary disease. Expert Rev Respiratory Med. 2025;19(6):597–608. doi:10.1080/17476348.2025.2492800
17. Montesi SB, Rao R, Liang LL, et al. Gadofosveset-enhanced lung magnetic resonance imaging to detect ongoing vascular leak in pulmonary fibrosis. Europ Resp J. 2018;51(5). doi:10.1183/13993003.00171-2018
18. Widjanantie SC, Lestari F, Nusdwinuringtyas N, et al. Rehabilitation management for sarcopenia in chronic obstructive pulmonary disease: a literature review. Respiratory Sci. 2024;4(3):232–250.
19. Benz E, Trajanoska K, Lahousse L, et al. Sarcopenia in COPD: a systematic review and meta-analysis. European Respiratory Rev. 2019;28(154). doi:10.1183/16000617.0049-2019
20. Jain D, Atochina-Vasserman EN, Tomer Y, et al. Surfactant protein D protects against acute hyperoxic lung injury. Am J Respir Crit Care Med. 2008;178(8):805–813. doi:10.1164/rccm.200804-582OC
21. Tsutsumi T, Nakano D, Kawaguchi M, et al. MAFLD associated with COPD via systemic inflammation independent of aging and smoking in men. Diabetol Metab Syndrome. 2022;14(1):115. doi:10.1186/s13098-022-00887-w
22. Meier HCS, Mitchell C, Karadimas T, et al. Systemic inflammation and biological aging in the health and retirement study. GeroScience. 2023;45(6):3257–3265. doi:10.1007/s11357-023-00880-9
23. Magnussen H, Watz H. Systemic inflammation in chronic obstructive pulmonary disease and asthma: relation with comorbidities. Proc Am Thorac Soc. 2009;6(8):648–651. doi:10.1513/pats.200906-053DP
24. Joppa P, Petrasova D, Stancak B, et al. Systemic inflammation in patients with COPD and pulmonary hypertension. Chest. 2006;130(2):326–333. doi:10.1378/chest.130.2.326
25. Fu JJ, McDonald VM, Gibson PG, et al. Systemic inflammation in older adults with asthma-COPD overlap syndrome. Allergy Asthma Immunol Res. 2014;6(4):316–324. doi:10.4168/aair.2014.6.4.316
26. Wang J, Wen CK. Cryptic role of the ETHYLENE INSENSITIVE2 nuclear localization signal in ethylene signaling. Mol Plant. 2015;8(8):1129–1130. doi:10.1016/j.molp.2015.06.007
27. Bridevaux PO, Gerbase MW, Schindler C, et al. Sex-specific effect of body weight gain on systemic inflammation in subjects with COPD: results from the SAPALDIA cohort study 2. Europ Resp J. 2009;34(2):332–339. doi:10.1183/09031936.00162608
28. Bolton CE, Evans M, Ionescu AA, et al. Insulin resistance and inflammation - A further systemic complication of COPD. COPD. 2007;4(2):121–126. doi:10.1080/15412550701341053
29. Sin DD, Yoon YS, Jin M. Chronic obstructive pulmonary disease—a disease of accelerated aging. Aging and Disease. 2018;9(1):95–104.
30. Sanina N, Panina S. Features of systemic inflammation in patients with stable COPD. European Respiratory Journal. 2014;44(Suppl 58):3631.
31. Ellingsen J, Bröms K, Hårdstedt M, et al. Biomarkers of systemic inflammation are not associated with the risk of COPD exacerbations. 2023.
32. Pertseva ТО, Konopkina L, Basina BО. Peculiarities of response of systemic inflammation markers in patients with chronic obstructive pulmonary disease under their long-term follow-up. Pharma Innovation. 2013;2.
33. Obling N, Backer V, Hurst JR, et al. Nasal and systemic inflammation in chronic obstructive pulmonary disease (COPD). Respir Med. 2022;195:106774. doi:10.1016/j.rmed.2022.106774
34. Gea J, Barreiro E, Orozco-Levi M. Systemic Inflammation in COPD. Clin Pulmonary Med. 2009;16(5):233–242.
35. Kaiser MJ, Bauer JM, Rämsch C. Frequency of malnutrition in older adults: a multinational perspective using the mini nutritional assessment. J Am Geriatr Soc. 2010;58(9):1734–1738. doi:10.1111/j.1532-5415.2010.03016.x
36. Guigoz Y, Vellas B, Garry PJ. Assessing the nutritional status of the elderly: the mini nutritional assessment as part of the geriatric evaluation. Nutr Rev. 1996;54(1):S59. doi:10.1111/j.1753-4887.1996.tb03793.x
37. Detsky AS, McLaughlin JR, Baker JP, et al. What is subjective global assessment of nutritional status? J Parenteral Enteral Nutr. 1987;11(1):8–13. doi:10.1177/014860718701100108
38. Ottery FD. Definition of standardized nutritional assessment and interventional pathways in oncology. Nutrition. 1996;12(Supplement):S15–S19. doi:10.1016/0899-9007(96)90011-8
39. Kondrup J, Rasmussen HH, Hamberg OLE, et al. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutrition. 2003;22(3):321–336. doi:10.1016/s0261-5614(02)00214-5
40. Kwang BM, Na CE, Joon C, et al. Sarcopenia correlates with systemic inflammation in COPD. Int J Chronic Obstructive Pulmonary Dis. 2017;12:669–675.
41. Sepúlveda-Loyola W, Osadnik C, Phu S, et al. Diagnosis, prevalence, and clinical impact of sarcopenia in COPD: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2020;11(5):1164–1176. doi:10.1002/jcsm.12600
42. Bateman R, Sharpe M, Jagger JE, et al. 36th international symposium on intensive care and emergency medicine: Brussels, Belgium. 15-18 March 2016. Crit Care. 2016;20(Suppl 2):94. doi:10.1186/s13054-016-1208-6
43. Pae M, Meydani SN, Wu D. The role of nutrition in enhancing immunity in aging. Aging Dis. 2012;3(1):91.
44. Marcos A, Nova E, Montero A. Changes in the immune system are conditioned by nutrition. Eur J Clin Nutr. 2003;57 Suppl 1:S66. doi:10.1038/sj.ejcn.1601819
45. Shi Z, Taylor AW, Riley M, et al. Association between dietary patterns, cadmium intake and chronic kidney disease among adults. Clin Nutrition. 2017;37:S0261561416313668.
46. Cadranel J, Canellas A, Matton L, et al. Pulmonary complications of immune checkpoint inhibitors in patients with nonsmall cell lung cancer. European Respiratory Rev. 2019;28(153):190058. doi:10.1183/16000617.0058-2019
47. Tieland M, Dirks ML, van der Zwaluw N, et al. Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: a randomized, double-blind, placebo-controlled trial. J Am Med Directors Assoc. 2012;13(8):713–719. doi:10.1016/j.jamda.2012.05.020
48. Hornikx M, Van Remoortel H, Lehouck A, et al. Vitamin D supplementation during rehabilitation in COPD: a secondary analysis of a randomized trial. Respir Res. 2012;13(1):84. doi:10.1186/1465-9921-13-84
49. Beaudart C, Buckinx F, Rabenda V, et al. The effects of vitamin D on skeletal muscle strength, muscle mass, and muscle power: a systematic review and meta-analysis of randomized controlled trials. J Clin Endocrinol Metab. 2014;99(11):4336–4345. doi:10.1210/jc.2014-1742
50. Shi Z, Taylor AW, Riley M, et al. Association between dietary patterns, cadmium intake and chronic kidney disease among adults. Clin Nutrition. 2018;37(1):276–284. doi:10.1016/j.clnu.2016.12.025
51. Green SM, James EP, Latter S, et al. Barriers and facilitators to screening for malnutrition by community nurses: a qualitative study. J Human Nutrition Dietetics. 2014;27(1):88–95. doi:10.1111/jhn.12104
52. Jensen GL, Cederholm T, Correia M, et al. GLIM criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community. JPEN J Parenter Enteral Nutr. 2019;43(1):32–40. doi:10.1002/jpen.1440
53. Côté M, Lamarche B. Artificial intelligence in nutrition research: perspectives on current and future applications. Appl Physiol Nutr Metab. 2022;47(1):1–8. doi:10.1139/apnm-2021-0448
54. Kirkil G, Hamdi Muz M, Seçkin D, et al. Antioxidant effect of zinc picolinate in patients with chronic obstructive pulmonary disease. Respir Med. 2008;102(6):840–844. doi:10.1016/j.rmed.2008.01.010
55. van de Rest O, Berendsen AA, Haveman-Nies A, et al. Dietary patterns, cognitive decline, and dementia: a systematic review. Adv Nutrition. 2015;6(2):154–168. doi:10.3945/an.114.007617
56. Calder PC. Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochem Soc Trans. 2017;45(5):1105–1115. doi:10.1042/BST20160474
57. Dyall SC. Long-chain omega-3 fatty acids and the brain: a review of the independent and shared effects of EPA, DPA and DHA. Front Aging Neurosci. 2015;7:52. doi:10.3389/fnagi.2015.00052
58. Shoaib M, Shehzad A, Omar M, et al. Inulin: properties, health benefits and food applications. Carbohydr Polym. 2016;147:444–454. doi:10.1016/j.carbpol.2016.04.020
59. Ford AH, Almeida OP. Effect of homocysteine lowering treatment on cognitive function: a systematic review and meta-analysis of randomized controlled trials. J Alzheimer’s Dis. 2012;29(1):133–149. doi:10.3233/JAD-2012-111739
60. Dodd JW. Lung disease as a determinant of cognitive decline and dementia. Alzheimer’s Res Ther. 2015;7(1):32. doi:10.1186/s13195-015-0116-3
61. Aquilani R, Boselli M, Boschi F, et al. Branched-chain amino acids may improve recovery from a vegetative or minimally conscious state in patients with traumatic brain injury: a pilot study. Arch Phys Med Rehabil. 2008;89(9):1642–1647. doi:10.1016/j.apmr.2008.02.023
62. Gonçalinho GHF, Sampaio GR, Soares-Freitas RAM, et al. Omega-3 fatty acids in erythrocyte membranes as predictors of lower cardiovascular risk in adults without previous cardiovascular events. Nutrients. 2021;13(6). doi:10.3390/nu13061919
63. Jager-Wittenaar H, Ottery FD. Assessing nutritional status in cancer: role of the patient-generated subjective global assessment. Curr Opin Clin Nutr Metab Care. 2017;20(5):322–329. doi:10.1097/MCO.0000000000000389
64. Agustí A, Noell G, Brugada J, et al. Lung function in early adulthood and health in later life: a transgenerational cohort analysis. Lancet Respir Med. 2017;5(12):935–945. doi:10.1016/S2213-2600(17)30434-4
65. Schols A. Nutrition as a metabolic modulator in COPD. Chest. 2013;144(4):1340–1345. doi:10.1378/chest.13-0326
66. Norman K, Pichard C, Lochs H, et al. Prognostic impact of disease-related malnutrition. Clin Nutrition. 2008;27(1):5–15. doi:10.1016/j.clnu.2007.10.007
67. MacNee W. Is chronic obstructive pulmonary disease an accelerated aging disease? Ann Am Thoracic Soc. 2016;13 Suppl 5:S429–s437. doi:10.1513/AnnalsATS.201602-124AW
68. Dodd JW, Getov SV, Jones PW. Cognitive function in COPD. Europ Resp J. 2010;35(4):913–922. doi:10.1183/09031936.00125109
69. Côté M, Lamarche B. Artificial intelligence in nutrition research: perspectives on current and future applications. Applied Physiol Nutrition Metabol. 2021;47:1–8.
70. Glynn L, Moloney E, Lane S, et al. A smartphone app self-management program for chronic obstructive pulmonary disease: randomized controlled trial of clinical outcomes. JMIR mHealth uHealth. 2025;13:e56318. doi:10.2196/56318
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.