Back to Journals » Clinical Ophthalmology » Volume 19
Clinical Tolerance to Induced Astigmatism in Eyes Implanted with a Single Extended Depth of Focus Intraocular Lens (AT LARA®)
Authors Hida WT ![]() , Moscovici BK
, Moscovici BK ![]() , Miziara PESC, Nogueira DC, Vilar C, Kniggendorf DV, Tzelikis PFDM
, Miziara PESC, Nogueira DC, Vilar C, Kniggendorf DV, Tzelikis PFDM ![]() , Mundim LP, Ribeiro de Melo Junior I, De Medeiros AL, Nose W, Carricondo PC
, Mundim LP, Ribeiro de Melo Junior I, De Medeiros AL, Nose W, Carricondo PC ![]()
Received 7 October 2025
Accepted for publication 1 December 2025
Published 5 December 2025 Volume 2025:19 Pages 4455—4462
DOI https://doi.org/10.2147/OPTH.S568747
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Wilson Takashi Hida,1 Bernardo Kaplan Moscovici,2– 4 Paulo Eduardo Souto Castro Miziara,1 Daniel Cruz Nogueira,1 Cesar Vilar,1,5 Danilo Varela Kniggendorf,1 Patrick Frensel De Moraes Tzelikis,1 Leandro P Mundim,1 Irineu Ribeiro de Melo Junior,1 André Lins De Medeiros,1 Walton Nose,2 Pedro C Carricondo6
1Department of Ophthalmology, Hospital Oftalmológico de Brasília, Brasília, DF, Brazil; 2Department of Ophthalmology, Federal University of São Paulo (UNIFESP), São Paulo, SP, Brazil; 3Department of Ophthalmology, Hospital Visão Laser, Santos, SP, Brazil; 4Postgraduate Program in Translational Medicine, Escola Paulista de Medicina, Federal University of São Paulo (UNIFESP), São Paulo, SP, Brazil; 5Vilar Hospital de Olhos, Teresina, PI, Brazil; 6Department of Ophthalmology, University of São Paulo, São Paulo, SP, Brazil
Correspondence: Bernardo Kaplan Moscovici, Department of Ophthalmology, Federal University of São Paulo (UNIFESP), Rua Cayowaa, 854, apt. 82, São Paulo, SP, 05018-001, Brazil, Email [email protected]
Purpose: To evaluate clinical tolerance to induced astigmatism in pseudophakic eyes bilaterally implanted with an extended depth of focus (EDOF) intraocular lens (AT LARA®, Carl Zeiss Meditec). We hypothesized that small amounts of induced astigmatism may be clinically well tolerated by patients implanted with this EDOF IOL.
Methods: Prospective study including 10 patients (20 eyes) bilaterally implanted with the same EDOF IOL. Monocular defocus curves were obtained under photopic conditions after introducing cylindrical lenses of +1.00 D, +2.00 D, and +3.00 D at with-the-rule (WTR) and against-the-rule (ATR) orientations.
Results: The IOL demonstrated good tolerance up to +1.00 D of induced astigmatism, with significant reductions in visual acuity at higher magnitudes of astigmatism. Tolerance was higher for ATR astigmatism compared to WTR, consistent with axis-dependent depth-of-focus effects.
Conclusion: The AT LARA® EDOF IOL maintained functional visual performance with up to +1.00 D of regular astigmatism, while higher magnitudes led to clinically meaningful degradation. Axis orientation modulated performance, with ATR preserving intermediate and near vision and WTR favoring distance.
Keywords: extended depth of focus intraocular lens, pseudophakia, astigmatism tolerance, defocus curve, with-the-rule, against-the-rule, toric intraocular lens
Introduction
Cataract surgery has evolved beyond its rehabilitative purpose of restoring lens transparency, becoming one of the most frequently performed and refined refractive procedures in ophthalmology. Advances in intraocular lens (IOL) design have expanded outcomes from simple visual rehabilitation to spectacle independence across distance, intermediate, and near ranges. Presbyopia-correcting IOLs, including diffractive multifocal, trifocal, and extended depth of focus (EDOF) lenses, have played a central role in this evolution.1–4
Residual refractive error, particularly astigmatism, remains one of the major factors influencing postoperative satisfaction. Even small amounts of uncorrected astigmatism, as low as 0.50 to 0.75 diopters, may compromise distance acuity and contrast sensitivity in diffractive optics. EDOF designs, by elongating the depth of focus without producing multiple foci, may confer better tolerance to small residual cylinders compared with bifocal or trifocal IOLs. Nonetheless, residual astigmatism above 1.00 D has been consistently associated with clinically relevant visual penalties.5–8
Astigmatism axis orientation adds another layer of complexity. With-the-rule (WTR) astigmatism, where the steeper meridian is vertical, tends to preserve distance acuity. In contrast, against-the-rule (ATR) astigmatism may extend the effective depth of focus, supporting tasks such as intermediate and near vision. Age-related corneal changes typically shift the corneal profile from WTR to ATR, influencing postoperative tolerance patterns and the relevance of axis-specific trade-offs.9–12
Recent studies from our group have validated methodologies based on defocus curves with induced astigmatism, demonstrating their reproducibility and clinical applicability. Although the optical behavior of multifocal IOLs under residual astigmatism has been previously investigated, few studies have analyzed this effect specifically in true extended-depth-of-focus (EDOF) lenses, leaving a gap in understanding how these designs respond to different magnitudes and axes of astigmatism. To address this gap, the present study focuses exclusively on a single EDOF model, the AT LARA® (Carl Zeiss Meditec AG, Jena, Germany), to characterize its clinical tolerance to induced astigmatism. We hypothesized that small, controlled amounts of induced astigmatism would be clinically well tolerated by eyes implanted with the AT LARA® EDOF IOL, maintaining functional visual acuity and patient comfort.1–20
Building upon this validated framework, the present study evaluates clinical tolerance to induced astigmatism of +1.00 D, +2.00 D, and +3.00 D at WTR and ATR axes in pseudophakic patients bilaterally implanted with an EDOF IOL, aiming to quantify thresholds and explore axis-specific differences with practical relevance for surgical planning.13–15
Methods
This was a prospective, non-randomized clinical study conducted at the Hospital Oftalmológico de Brasília (HOB), Brazil. The protocol adhered to the Declaration of Helsinki and was approved by the HOB Institutional Review Board (approval code: 42915320.3.0000.5667). Written informed consent was obtained from all participants. The study builds upon previously validated methodologies for induced astigmatism defocus testing.14,15 All assessments were performed monocularly under controlled photopic conditions using a single model of extended depth of focus IOL (AT LARA®).
Evaluation of IOL Position and Corneal Topography
Postoperative IOL centration and tilt were assessed at the slit lamp using coaxial retroillumination and by analyzing the symmetry of the Purkinje reflex. Eyes with visible decentration or tilt greater than 0.5 mm were excluded. Corneal regularity was confirmed by computerized corneal topography (Medmont E300, Medmont International, Melbourne, Australia) to exclude irregular astigmatism.
Sample Size and Power Analysis
A post hoc power analysis indicated that a sample of 20 eyes provided 80% power to detect a 0.10 logMAR difference in visual acuity between the induced astigmatism conditions, assuming a standard deviation of 0.08 and an α level of 0.05.
Application of Cylindrical Lenses
Astigmatism induction was performed using trial cylindrical lenses mounted in a standard trial frame to ensure reproducible vertex distance and axis alignment.
Participants
Ten patients (20 eyes) were enrolled between July and October 2019. The inclusion criteria were age 50–70 years, bilateral senile cataract, and bilateral implantation of the same extended depth of focus (EDOF) intraocular lens (AT LARA, Carl Zeiss Meditec, Jena, Germany). Preoperative corneal astigmatism had to be <1.00 D, and postoperative corrected distance visual acuity (CDVA) ≥20/30. Exclusion criteria were previous ocular surgery, irregular astigmatism, keratoconus, glaucoma, retinal disease, amblyopia, uveitis, intraoperative complications, IOL tilt/decentration >0.5 mm, or significant posterior capsular opacification.
Surgical Procedure
All surgeries were performed by the same experienced surgeon (DCN) using standard temporal clear-corneal phacoemulsification with a 2.2 mm incision. A 5.0–5.5 mm continuous curvilinear capsulorhexis was created, followed by hydrodissection, phacoemulsification, cortical cleanup, and in-the-bag implantation of the EDOF IOL. Postoperative regimen consisted of a topical antibiotic for one week and a corticosteroid tapered over four weeks.
Visual Testing and Defocus Protocol
Assessments were performed monocularly between 30 and 90 days postoperatively. Corrected distance visual acuity was measured under photopic conditions (85 cd/m2) at 4 m using retroilluminated ETDRS charts (CSV-1000, Vector Vision, Greenville, USA).
A control defocus curve was first obtained by adding spherical trial lenses from +2.50 to –2.50 D in 0.50-D steps over the manifest refraction (cylinder = 0). To simulate residual astigmatism, cylindrical trial lenses of +1.00, +2.00, and +3.00 D were introduced at two orientations: 90° (with-the-rule, WTR) and 180° (against-the-rule, ATR). For each magnitude and axis, the full spherical defocus series was repeated in randomized order. A two-minute rest interval was maintained between sequences. The vertex distance was standardized at 12–14 mm, and ambient illumination was kept at a constant level. The same examiner conducted all testing.
Statistical Analysis
Visual acuity values were converted to logMAR. Normality was assessed with the Shapiro–Wilk test. One-way ANOVA with Tukey’s HSD was performed at each vergence to compare control versus induced cylinders (WTR and ATR). A two-way ANOVA was used to evaluate the main effects of cylinder magnitude and axis, as well as their interaction. Statistical significance was set at p < 0.05.
Results
Demographics
Twenty eyes from ten patients were analyzed. Mean age was 59.3 ± 5.1 years; seven were male (70%) and three female (30%). All surgeries were uneventful, and all eyes demonstrated centered-in-the-bag AT LARA IOLs and clear visual axes at the time of testing (Table 1).
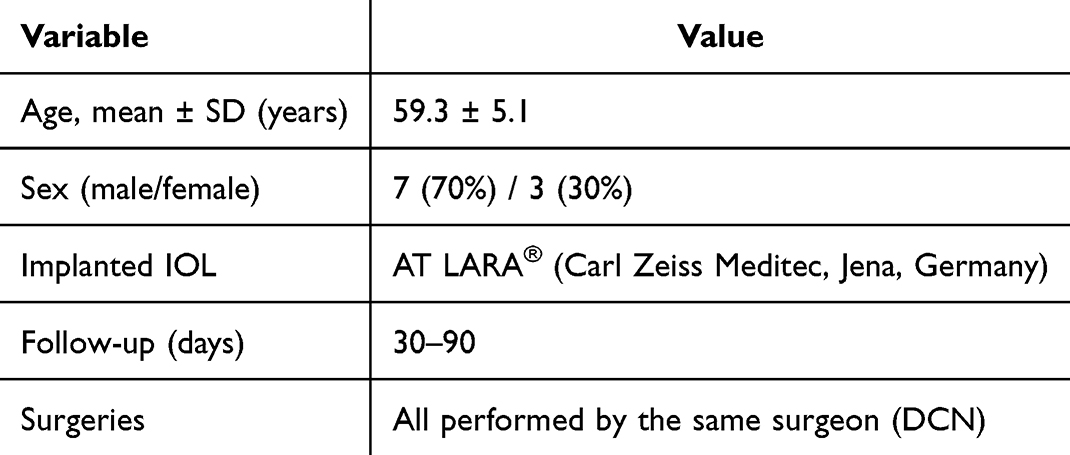 |
Table 1 Demographic Characteristics of the Study Cohort (n=10 Patients, 20 Eyes) |
Control Defocus Curves
The control defocus curve (0 D cylinder) exhibited the expected EDOF profile, with optimal acuity at plano and maintained performance through −1.50 D. A gradual decline occurred under hyperopic vergences beyond +1.00 D (Figure 1, with error bars representing ±1 standard deviation).
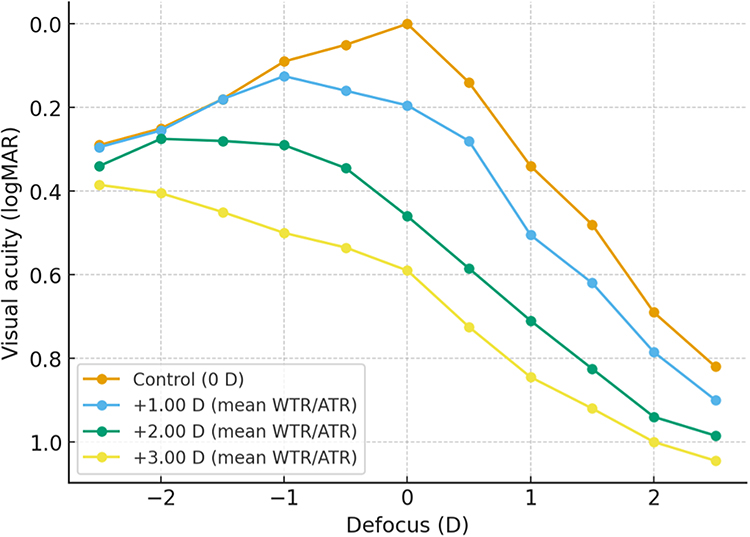 |
Figure 1 Pooled defocus curves (Control vs +1.00 D, +2.00 D, +3.00 D). |
+1.00 D Induced Astigmatism
With +1.00 D induction, visual acuity was largely preserved compared with the control. Statistically significant decrements were observed at plano and low hyperopic vergences—specifically plano (p = 0.002), +1.00 D (p = 0.009), and +1.50 D (p = 0.012) for WTR, and plano (p < 0.001), +0.50 D (p = 0.007), +1.00 D (p = 0.001), and –0.50 D (p = 0.026) for ATR (Table 2). Defocus curves showed that the myopic side (–0.50 to –1.50 D) remained close to the control.
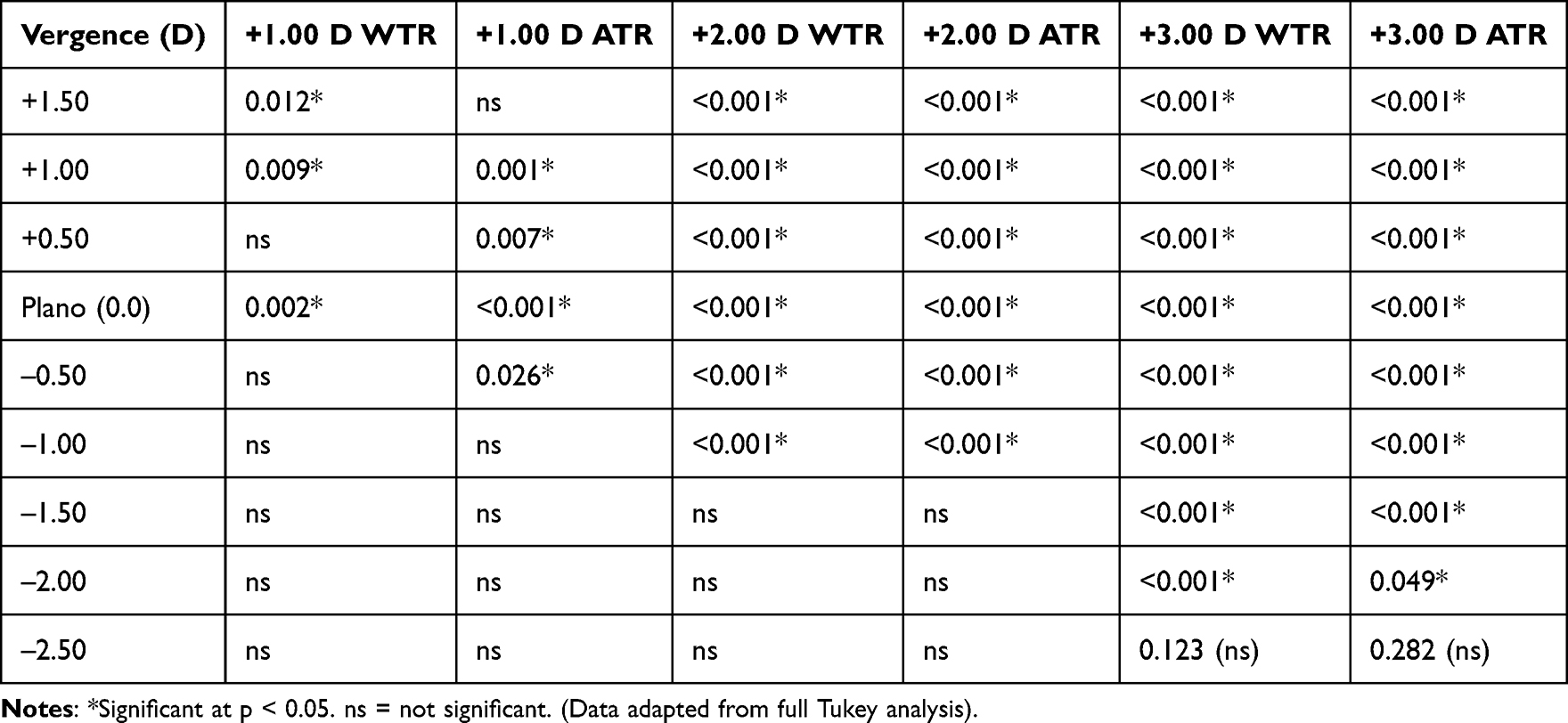 |
Table 2 Summary of Significant Tukey Comparisons vs Control (p-values at Key Vergences) |
+2.00 D Induced Astigmatism
At +2.00 D, acuity decreased significantly across most vergences for both axes, sparing only −1.50, −2.00, and −2.50 D. ATR orientation preserved intermediate vergences (−0.50 to −1.50 D) better than WTR. At the same time, WTR favored distance acuity at plano (Table 2 and Figure 2).
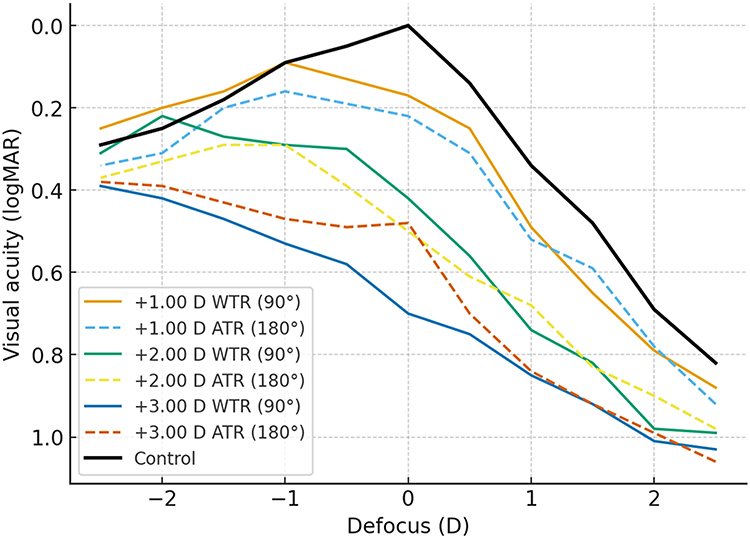 |
Figure 2 Axis-specific defocus curves (WTR vs ATR). |
+3.00 D Induced Astigmatism
Induction of +3.00 D produced marked deterioration across nearly the entire defocus curve, sparing only –2.50 D (p = 0.123 for WTR; p = 0.282 for ATR). ATR maintained slightly better intermediate acuity, while WTR preserved distance performance (Table 2 and Figure 2).
Two-Way ANOVA
Two-way analysis confirmed significant main effects of cylinder magnitude at most vergences (partial η2 = 0.18–0.41, p < 0.01). Axis effects were smaller but significant near plano and intermediate vergences (partial η2 = 0.06–0.12, p < 0.05). Significant magnitude–axis interactions were observed at plano and ±0.50 D, consistent with the axis-dependent trade-offs (Table 2).
Discussion
The present prospective clinical study investigated tolerance to induced astigmatism in pseudophakic patients bilaterally implanted with an EDOF IOL. By employing an induced defocus-with-cylinder protocol validated in prior work,14,15 we systematically evaluated the impact of +1.00 D, +2.00 D, and +3.00 D cylinders, oriented at the WTR and ATR axes, on defocus curves. Our initial hypothesis was that EDOF optics would maintain functional visual acuity under small amounts of induced astigmatism, particularly up to +1.00 D. The findings revealed three principal observations. First, the AT LARA® EDOF IOL demonstrated good tolerance to approximately +1.00 D of induced astigmatism, with significant decrements confined to plano and low hyperopic vergences. Second, +2.00 D and especially +3.00 D cylinders produced widespread and clinically relevant loss of acuity across the curve, sparing only extreme myopic vergences. Third, axis orientation modulated visual performance, with ATR astigmatism relatively preserving intermediate and near ranges, while WTR maintained distance acuity at plano.
These results align with and extend prior evidence that the tolerance thresholds of presbyopia-correcting IOLs depend on their optical design. Hayashi et al demonstrated that diffractive bifocal and trifocal lenses are sensitive to residual astigmatism as small as 0.50–0.75 D, resulting in significant loss of acuity across various distances.5,6 In contrast, EDOF and enhanced monofocal designs have been reported to preserve functional acuity up to about +1.00 D.7,8 Rocha et al confirmed that an enhanced monofocal IOL designed to extend depth of focus tolerated approximately +1.00 D of induced cylinder before showing significant losses, a threshold echoed in the present findings.7 Pérez-Sanz et al also emphasized axis-specific differences in tolerance, with ATR orientation better preserving image quality at intermediate vergences compared to WTR.8 Our clinical data support these bench and optical analyses, demonstrating that ATR induction mitigated losses at intermediate vergences, whereas WTR provides sharper distance contours.
The optical underpinnings of these axis-dependent effects are consistent with classical theory. In WTR astigmatism, the vertical meridian is steeper, and the circle of least confusion tends to maintain sharper vertical contours at distance, thereby preserving high-contrast optotypes near plano. Conversely, ATR astigmatism elongates the blur ellipse horizontally, effectively extending the depth of focus and allowing better tolerance to defocus at intermediate and near ranges.9,10 Rhim et al confirmed these differences experimentally, showing that eyelid squinting preferentially enhances near vision in ATR and distance vision in WTR pseudophakic eyes.10 These biomechanical interactions add to the optical explanation of why ATR orientation preserved intermediate vergences better in our study.
Age-related corneal changes also contextualize our findings. Population studies, such as the Reykjavik Eye Study, have demonstrated a natural shift from WTR to ATR with advancing age, due to the flattening of the vertical meridian and the relative steepening of the horizontal meridian.12 This physiologic drift implies that a large proportion of older cataract patients will naturally present ATR orientation preoperatively. Our data suggest that small amounts of residual ATR may be more tolerable in EDOF optics, potentially even advantageous for intermediate tasks, whereas residual WTR may better support distance vision. These insights underscore the importance of individualizing refractive targets not only by cylinder magnitude but also by axis orientation, particularly in elderly populations.
The tolerance observed at +1.00 D is clinically significant. In practice, approximately 35–45% of cataract patients present with corneal astigmatism of 0.75 D or greater preoperatively, and about 15–20% present with astigmatism of 1.50 D or greater.12 While toric IOLs, arcuate keratotomy, and femtosecond-assisted corneal incisions provide means to address astigmatism, surgical variability and biometric limitations frequently leave residual cylinder. The present results, combined with prior validation studies,14,15 indicate that EDOF IOLs maintain functional acuity up to about +1.00 D, but beyond this threshold, clinically meaningful penalties occur. These findings justify correcting astigmatism ≥1.00 D in EDOF recipients, consistent with current expert consensus.11
Recent comparative studies further highlight that tolerance thresholds are design-dependent. Campos et al demonstrated that dual-technology diffractive IOLs combined with enhanced monofocals showed different tolerance profiles, with ATR orientation consistently preserving intermediate performance better than WTR.18 Likewise, Hida et al reported that blended strategies with dual-technology and EDOF optics may mitigate losses by distributing visual priorities across distance ranges.19 These findings extend the clinical applicability of induced astigmatism protocols, supporting their role not only in single-platform evaluation but also in comparative refractive planning.
The magnitude-dependent results further illustrate the nonlinear relationship between astigmatism and visual acuity. With a +1.00 D induction, decrements were small and localized, while with a +2.00 D induction, acuity decreased across most vergences, and with a +3.00 D induction, deterioration was nearly global. Importantly, at higher magnitudes, axis effects became more pronounced: ATR continued to preserve intermediate vergences better, while WTR favored distance. This interaction was confirmed in the two-way ANOVA, which demonstrated significant magnitude–axis interactions at plano and ±0.50 D. These observations reinforce that surgical decisions should not only consider the magnitude of preoperative astigmatism but also its axis orientation.
Clinical applicability is clear. For patients implanted with EDOF IOLs, leaving residual ATR of up to +1.00 D may be less disruptive than leaving WTR. In borderline cases (~1.00 D), surgeons may tailor refractive targets based on visual priorities: preserving small ATR for patients prioritizing intermediate/near tasks, while preserving small WTR for those emphasizing distance. Moreover, toric IOL planning must account for the precision of alignment. Misalignment reduces effective cylinder correction by approximately 3.3% per degree, with substantial degradation beyond 10°.17 Misalignment may also inadvertently convert WTR to ATR or vice versa, altering the expected tolerance profile. Alpins’ vector analysis emphasizes the importance of considering flattening, steepening, and torque components of astigmatic correction, particularly in relation to axis.16 Precision in alignment is therefore essential to preserve the axis-dependent advantages identified in this study.20–22
The broader consequences of residual astigmatism go beyond high-contrast acuity. Residual cylinders have been associated with loss of contrast sensitivity, dysphotopsia, and increased retreatment rates in multifocal IOL recipients.13 While EDOF designs mitigate these risks, the present findings confirm that tolerance is not unlimited. Incorporating tolerance thresholds and axis trade-offs into preoperative planning can help reduce dissatisfaction and the need for retreatments. Recent studies by Hida, Moscovici et al, compared blended IOL strategies, showing that combinations of enhanced monofocal or EDOF with diffractive multifocals may balance contrast and spectacle independence.14–19 Understanding astigmatism tolerance is relevant to such strategies, as residual astigmatism may interact with different optics in complex ways.
Limitations of the present study should be acknowledged. The sample size was modest and derived from a single center, which may limit the generalizability of the findings. Only one EDOF platform was evaluated; tolerance may differ across models due to variations in optical design. Testing was performed monocularly under photopic luminance and with high-contrast optotypes; thus, binocular summation, mesopic conditions, and contrast sensitivity were not assessed. Furthermore, induced astigmatism under experimental conditions may not perfectly replicate the multifactorial nature of real-world residual cylinder, which can include irregular components and neural adaptation effects. Nevertheless, induced-defocus protocols provide valuable within-subject comparisons under controlled conditions and have been increasingly adopted to benchmark presbyopia-correcting optics.7,8,14–18 Future studies with larger, multicenter cohorts and inclusion of different EDOF platforms, binocular assessments, and contrast sensitivity measures are warranted to validate and expand these findings.
In conclusion, the present study demonstrates that pseudophakic eyes implanted with an EDOF IOL tolerated approximately +1.00 D of regular astigmatism with minimal impact across defocus curves. In contrast, cylinders of +2.00 D and +3.00 D produced widespread and clinically meaningful deterioration. Axis orientation modulated outcomes, with ATR preserving intermediate and near performance and WTR favoring distance. These results support the hypothesis that EDOF optics offer increased tolerance to small residual astigmatism compared with multifocal designs, reinforcing their suitability for patients with limited astigmatic correction potential. These findings confirm validated induced-astigmatism protocols, align with contemporary evidence from optical and clinical studies,5–8,15–19 and provide practical thresholds for toric planning, residual targeting, and patient counseling in cataract surgery with EDOF implantation.
Funding
No specific funding was received for this work.
Disclosure
The authors declare no conflicts of interest.
References
1. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–618. doi:10.1136/bjophthalmol-2011-300539
2. Lundström M, Dickman M, Henry Y, et al. Changing practice patterns in European cataract surgery as reflected in the European registry of quality outcomes for cataract and refractive surgery 2008 to 2017. J Cataract Refract Surg. 2021;47(3):373–378. doi:10.1097/j.jcrs.0000000000000457
3. Gatinel D, Loicq J. Clinically relevant optical properties of bifocal, trifocal and extended depth of focus intraocular lenses. J Refract Surg. 2016;32(4):273–280. doi:10.3928/1081597X-20160121-07
4. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth of focus versus trifocal for intraocular lens implantation: systematic review and meta-analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
5. Hayashi K, Manabe S, Yoshida M, Hayashi H. Effect of astigmatism on visual acuity in eyes with a diffractive multifocal intraocular lens. J Cataract Refract Surg. 2010;36(8):1323–1329. doi:10.1016/j.jcrs.2010.02.016
6. Hayashi K, Yoshida M, Igarashi C, Hirata A. Effect of refractive astigmatism on all-distance visual acuity in eyes with a trifocal intraocular lens. Am J Ophthalmol. 2021;221:279–286. doi:10.1016/j.ajo.2020.07.051
7. Rocha KM, Costa ED, Dodhia M, Waring GO. Tolerance to induced astigmatism with a monofocal intraocular lens designed to extend the depth of focus. J Refract Surg. 2023;39(4):222–228. doi:10.3928/1081597X-20230126-02
8. Pérez-Sanz L, Vega F, Azor-Morón JA, Cuellar F, Millán MS, Garzón N. Tolerance to residual astigmatism of an isofocal intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2024;262(4):1169–1180. doi:10.1007/s00417-023-06305-9
9. Sawusch MR, Guyton DL. Optimal astigmatism to enhance depth of focus after cataract surgery. Ophthalmology. 1991;98(7):1025–1029. doi:10.1016/S0161-6420(91)32182-1
10. Rhim JW, Eom Y, Park SY, et al. Eyelid squinting improves near vision in against-the-rule and distance vision in with-the-rule astigmatism in pseudophakic eyes: an eye model experimental study. BMC Ophthalmol. 2020;20(1):4. doi:10.1186/s12886-019-1297-5
11. Villegas EA, Alcon E, Artal P. Minimum amount of astigmatism that should be corrected. J Cataract Refract Surg. 2014;40(1):13–19. doi:10.1016/j.jcrs.2013.09.010
12. Ferrer-Blasco T, Montés-Micó R, Peixoto-de-Matos SC, González-Méijome JM, Cerviño A. Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35(1):70–75. doi:10.1016/j.jcrs.2008.09.027
13. Gundersen KG, Makari S, Ostenstad S, Potvin R. Retreatments after multifocal intraocular lens implantation: an analysis. Clin Ophthalmol. 2016;10:365–371.
14. Hida WT, Vilar CM, Moscovici BK, Motta AFP, Carricondo PC. A new methodology for evaluating the potential impact of residual refractive astigmatism in pseudophakic patients. Clin Ophthalmol. 2024;18:1909–1914. doi:10.2147/OPTH.S453340
15. De Melo IR, Hida WT, Moscovici BK, et al. Validation of clinical protocol of astigmatism induction in pseudophakic patients. Clin Ophthalmol. 2024;18:3375–3387. doi:10.2147/OPTH.S472752
16. Alpins NA. Vector analysis of astigmatism changes by flattening, steepening, and torque. J Cataract Refract Surg. 1997;23(10):1503–1514. doi:10.1016/S0886-3350(97)80021-1
17. Tognetto D, Perrotta AA, Bauci F, et al. Quality of images with toric intraocular lenses: effect of misalignment. J Cataract Refract Surg. 2018;44(3):376–381. doi:10.1016/j.jcrs.2017.10.053
18. Campos PTS, Hida WT, Moscovici BK, et al. Comparison of tolerance to induced astigmatism in pseudophakic eyes implanted with dual-technology diffractive IOL and enhanced monofocal IOL. Indian J Ophthalmol. 2025;73(9):1302–1306. doi:10.4103/IJO.IJO_2224_24
19. Hida WT, Moscovici BK, Cortez CM, et al. Comparison of visual outcomes of bilateral dual-technology diffractive intraocular lens vs blended enhanced monofocal with dual-technology intraocular lens. J Cataract Refract Surg. 2024;50(4):401–406. doi:10.1097/j.jcrs.0000000000001374
20. Rodrigues PF, Moscovici BK, Lamazales L, et al. Measurement of the visual axis through two different methods: quantification and differences for measuring chord μ. Arq Bras Oftalmol. 2023;87(4):e2022–0035. doi:10.5935/0004-2749.2022-0035
21. Rios LC, Silva PGD, Canamary Junior AM, et al. Centration in refractive surgery. Arq Bras Oftalmol. 2020;83(1):76–81. doi:10.5935/0004-2749.20200014
22. de Miranda AP, Silva CB, Mimica LM, Moscovici BK, Malavazzi GR, Hida RY. In vitro antimicrobial analysis of aqueous humor after topical application of moxifloxacin hydrochloride 0.5%. J Cataract Refract Surg. 2015;41(1):135–139. doi:10.1016/j.jcrs.2014.11.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.