Back to Journals » Clinical Ophthalmology » Volume 19
Clinical Tolerance to Experimentally Induced with-the-Rule and Against-the-Rule Astigmatism After Implantation of an Extended Depth-of-Focus Intraocular Lens: A Defocus-Curve Study
Authors Hida WT ![]() , Mundim LP, Moscovici BK
, Mundim LP, Moscovici BK ![]() , Vilar CMC, Tzelikis PFDM
, Vilar CMC, Tzelikis PFDM ![]() , Nakano CT, de Melo Junior IR, de Medeiros AL, Lake JC, Chaves MAPD
, Nakano CT, de Melo Junior IR, de Medeiros AL, Lake JC, Chaves MAPD ![]() , Motta AFP, Nose W, Carricondo PC
, Motta AFP, Nose W, Carricondo PC ![]()
Received 7 October 2025
Accepted for publication 23 December 2025
Published 31 December 2025 Volume 2025:19 Pages 4967—4974
DOI https://doi.org/10.2147/OPTH.S569153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wilson Takashi Hida,1 Leandro Pessoa Mundim,1 Bernardo Kaplan Moscovici,2– 4 César Martins Cortez Vilar,1,5 Patrick Frensel De Moraes Tzelikis,1 Celso Takashi Nakano,6 Irineu Ribeiro de Melo Junior,1 André Lins de Medeiros,1 Jonathan Clive Lake,1 Mario Augusto Pereira Dias Chaves,1 Antonio Francisco Pimenta Motta,1 Walton Nose,2 Pedro C Carricondo6
1Department of Ophthalmology, Hospital Oftalmológico de Brasília, Brasília, DF, Brazil; 2Department of Ophthalmology, Federal University of São Paulo (UNIFESP), São Paulo, SP, Brazil; 3Department of Ophthalmology, Hospital Visão Laser, Santos, SP, Brazil; 4Postgraduate Program in Translational Medicine, Escola Paulista de Medicina, Federal University of São Paulo, São Paulo, SP, Brazil; 5Department of Ophtalmology, Vilar Hospital de Olhos, Teresina, PI, Brazil; 6Department of Ophthalmology, University of São Paulo, São Paulo, SP, Brazil
Correspondence: Bernardo Kaplan Moscovici, Email [email protected]
Purpose: To quantify the clinical tolerance to induced with-the-rule (WTR, 90°) and against-the-rule (ATR, 0°/180°) astigmatism after implantation of an extended depth-of-focus (EDOF) intraocular lens (IOL), and to identify axis-specific trade-offs across the defocus curve.
Methods: In this non-randomized, comparative, cross-sectional study, nine pseudophakic patients (nine dominant eyes) implanted with a Tecnis Symfony® EDOF IOL underwent monocular photopic testing (85 cd/m2) at 4 m using Early Treatment Diabetic Retinopathy Study (ETDRS) charts. Defocus curves were acquired from − 5.00 D to +2.50 D in 0.50-D steps over best subjective refraction. Regular myopic astigmatism was optically induced with +1.00 D, +2.00 D, and +3.00 D positive cylindrical lenses at canonical axes (0°, 45°, 90°, 135°); analyses focused on WTR (90°) and ATR (0°/180°). Visual acuity (VA) was converted to logMAR. Repeated-measures ANOVA with Tukey post hoc testing assessed effects of cylinder magnitude, axis, and vergence (α=0.05).
Results: Distance VA remained functionally preserved with +1.00 D, while +2.00 D produced clinically meaningful deterioration and +3.00 D caused broad loss of acuity across vergences. Axis orientation modulated performance: WTR preserved distance acuity around plano, whereas ATR relatively favored intermediate and very near vergences (approximately − 2.00 D to − 3.50 D). ANOVA confirmed significant effects of cylinder magnitude and vergence (both p< 0.01) and a significant axis-by-vergence interaction near plano and +0.50 D (p< 0.05). These findings support a practical tolerance envelope of about +1.00 D for EDOF recipients, beyond which functional penalties become evident.
Conclusion: After EDOF implantation, regular astigmatism of ~+1.00 D is generally tolerated, while +2.00 D and +3.00 D compromise function across the defocus curve. Axis matters: WTR preferentially preserves distance VA and ATR relatively supports intermediate/near performance. These data provide actionable thresholds and axis-aware guidance for toric planning, residual-targeting, and patient counseling.
Keywords: astigmatism, lenses, intraocular, cataract extraction, visual acuity, refraction, ocular
Introduction
Cataract surgery has evolved from a rehabilitative procedure into one of the most frequently performed refractive surgeries worldwide. The introduction of presbyopia-correcting intraocular lenses (IOLs), including multifocal, trifocal, and extended depth-of-focus (EDOF) designs, has broadened patient expectations from simple visual restoration to functional spectacle independence across distance, intermediate, and near ranges.1,2 Despite these advances, residual refractive errors, particularly astigmatism, remain among the most important limiting factors affecting postoperative visual outcomes and patient satisfaction.3–5
Residual astigmatism of 0.50 to 0.75 diopters (D) has been shown to reduce distance visual acuity (VA), contrast sensitivity, and overall visual quality in eyes implanted with monofocal, EDOF, and multifocal IOLs.6–8 This effect is especially pronounced in diffractive multifocal and trifocal optics, which exhibit higher sensitivity to optical aberrations.9,10 In contrast, EDOF IOLs are designed to elongate the depth of focus without generating multiple foci, thereby demonstrating slightly greater tolerance to low levels of astigmatism than bifocal and trifocal lenses.11,12 However, clinically relevant deterioration in VA has been consistently reported when residual cylinders exceed 1.00 D.13,14
Astigmatism orientation also plays a crucial role in functional outcomes. With-the-rule (WTR) astigmatism, in which the vertical meridian is steeper, tends to preserve distance vision. In contrast, against-the-rule (ATR) astigmatism, with a steeper horizontal meridian, may provide an extended depth of focus, favoring intermediate and near visual tasks.15–17 Age-related corneal remodeling, with a gradual shift from WTR to ATR profiles, further emphasizes the importance of axis-specific tolerance when planning refractive targets and surgical strategies.18,19 Recent clinical studies have confirmed that ATR induction may preserve intermediate vision more effectively, whereas WTR maintains sharper contours for distance.20–22
Validated experimental protocols have employed induced astigmatism through defocus curves to quantify tolerance thresholds in pseudophakic eyes.22–24 These methodologies have been applied to various lens platforms, demonstrating reproducibility and clinical applicability for evaluating the functional impact of both the magnitude and axis of residual astigmatism. Within this context, the diffractive echelette-design EDOF IOL has shown favorable intermediate and near performance. Still, data remain limited regarding its tolerance to induced astigmatism across different orientations.
This study adds to previous literature by quantifying axis-specific effects of induced astigmatism on defocus curves and clarifying how these patterns may influence clinical decision-making.
The present study aims to evaluate the clinical tolerance of pseudophakic patients implanted with an EDOF IOL with induced cylindrical defocus of +1.00, +2.00, and +3.00 D, oriented along WTR and ATR axes. By integrating validated methodologies and focusing on axis-specific differences, this study seeks to provide clinically relevant thresholds to guide toric planning, residual refractive targeting, and patient counseling in EDOF cataract surgery.
Methods
Study Design and Ethics
This was a prospective, non-randomized clinical study conducted at the Hospital Oftalmológico de Brasília (HOB), Brazil. The protocol adhered to the Declaration of Helsinki and was approved by the HOB Institutional Review Board (approval code: 42915320.3.0000.5667). Written informed consent was obtained from all participants.
Patients
Nine pseudophakic patients (nine dominant eyes) aged 18 years or older were included. All had undergone uneventful phacoemulsification with implantation of a Tecnis Symfony® extended depth-of-focus (EDOF) intraocular lens (Johnson & Johnson Vision, Santa Ana, CA, USA) in the dominant eye. Exclusion criteria were: inability to perform standardized visual acuity testing; corrected distance visual acuity (CDVA) worse than 20/25; optic nerve, macular or corneal pathology; media opacities beyond minimal posterior capsule opacification; ocular inflammation; or any prior intraocular surgery other than cataract extraction.
Preoperative corneal astigmatism was not systematically recorded, as the study evaluated optically induced astigmatism rather than relying on preoperative corneal values.
Surgical Procedure
All surgeries were performed by the same experienced surgeon using a standardized technique. A 2.2 mm clear corneal incision was created on the steepest meridian, followed by a ~5.0 mm continuous curvilinear capsulorhexis, hydrodissection, phacoemulsification, cortical cleanup, and in-the-bag implantation of a diffractive echelette-design EDOF IOL using the manufacturer’s injector. No intraoperative complications occurred.
Visual Acuity Testing
Monocular visual performance was assessed under photopic conditions (85 cd/m2) at 4 m with Early Treatment Diabetic Retinopathy Study (ETDRS) charts using the CSV-1000 system (VectorVision, Greenville, OH, USA). Testing included uncorrected distance visual acuity, manifest refraction, and CDVA. Visual acuity values were recorded and converted to logarithm of the minimum angle of resolution (logMAR) for analysis.
Before each defocus and cylinder-induction measurement, the cylindrical axis was carefully aligned and reconfirmed through repeated verification in the trial frame to ensure consistent vertex distance and axis stability throughout all measurements.
Defocus Curves and Cylinder Induction
Defocus curves were obtained by adding spherical trial lenses from −5.00 D to +2.50 D in 0.50-D steps over the patient’s best subjective refraction (cylinder neutralized). Regular myopic astigmatism was then optically induced with positive cylindrical lenses of +1.00 D, +2.00 D, and +3.00 D at canonical axes (0°, 45°, 90°, and 135°). For analytical purposes, 90° was treated as with-the-rule (WTR) and 0°/180° as against-the-rule (ATR); oblique axes (45° and 135°) were recorded and may be reported separately.
Axis convention note: in plus-cylinder notation, WTR corresponds to +cyl at 90° (≡ −cyl at 180° in minus-cyl notation) and ATR corresponds to +cyl at 180° (≡ −cyl at 90°).
Outcomes
The primary outcome was the change in logMAR visual acuity across defocus vergences for each induced cylinder magnitude, relative to the control (no cylinder). Secondary outcomes included the effect of axis orientation (WTR vs ATR) at each vergence and the interaction between cylinder magnitude and axis orientation. For clinical interpretation in figures, the 0.3 logMAR reference line (≈20/40) was annotated but not used as a statistical decision threshold.
Statistical Analysis
Repeated-measures analysis of variance (ANOVA) was used to assess the effects of vergence and cylinder magnitude/axis on logMAR acuity, with Tukey post hoc testing for pairwise comparisons (α=0.05). Demographic homogeneity (sex, age distribution, laterality) was explored with Kruskal–Wallis tests. Analyses were performed with Microsoft® R Open 3.5.1 and RStudio 1.1.456, and Microsoft® Excel 2007.
Results
Patient Demographics
Nine eyes from nine patients were analyzed. The mean age was 60.9 ± 5.6 years; three patients (33%) were 50–59 years and six (67%) 60–69 years. Five patients were female (56%) and four male (44%). Six eyes (67%) were left and three (33%) right. Kruskal–Wallis testing confirmed homogeneity for sex (p=0.323) and laterality (p=0.602), while age distribution was significant (p=0.019). Full demographics are shown in Table 1.
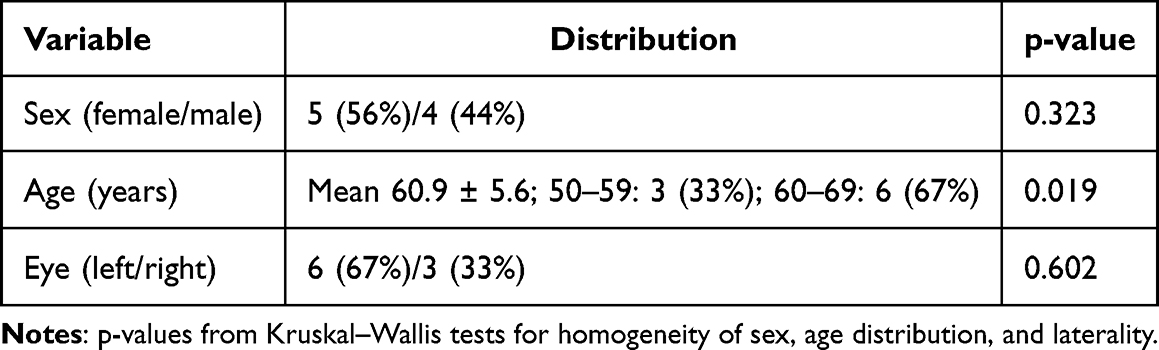 |
Table 1 Patient Demographics and Baseline Characteristics |
Visual Acuity with Induced Astigmatism (Magnitude Effect)
Distance visual acuity remained functionally preserved with +1.00 D of induced regular astigmatism, whereas +2.00 D produced clinically meaningful deterioration and +3.00 D caused widespread loss of acuity across most vergences. A qualitative summary by cylinder magnitude is presented in Table 2.
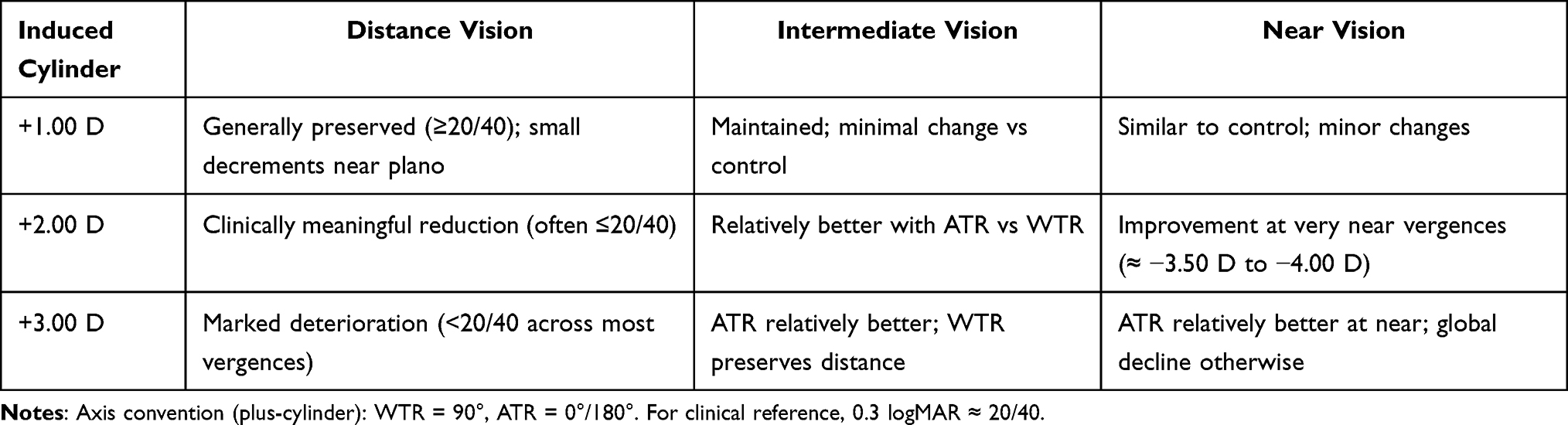 |
Table 2 Summary of Visual Acuity Outcomes with Induced Regular Astigmatism |
Defocus Curves (Overall)
Figure 1 depicts the defocus curves for control (no cylinder) versus +1.00 D, +2.00 D, and +3.00 D across vergences from −5.00 D to +2.50 D. With +1.00 D, the curve remained close to control, with minor decrements near plano and in low hyperopic vergences. With +2.00 D, acuity worsened at multiple vergences along the curve, and with +3.00 D the deterioration was broad, sparing essentially only the most myopic defocus points (very near). The dashed line at 0.3 logMAR marks the 20/40 functional threshold and illustrates the transition from acceptable to impaired distance function as cylinder increases.
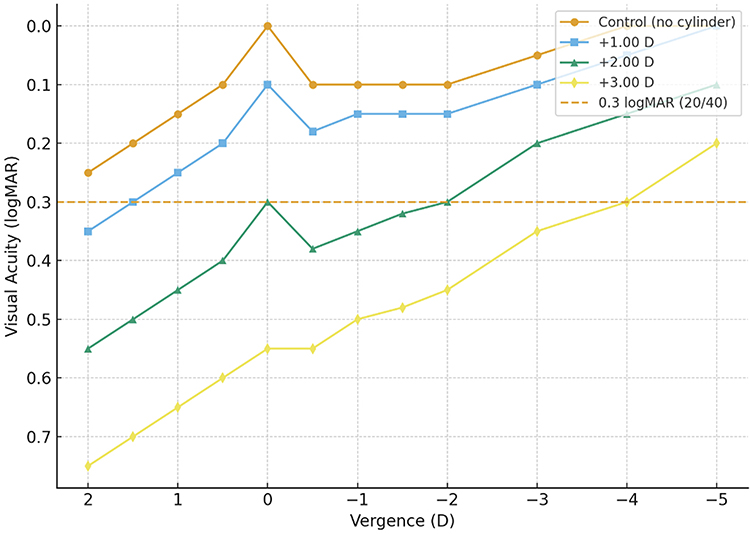 |
Figure 1 Defocus curves under control and induced cylinders (+1.00 D, +2.00 D, +3.00 D). Monocular logMAR visual acuity across vergences from −5.00 D to +2.50 D under photopic conditions; dashed line indicates 0.3 logMAR (20/40). |
Axis-Specific Tolerance (WTR = 90° vs ATR = 0°/180°)
Axis orientation significantly modulated functional performance (Figure 2). At +1.00 D, both WTR (90°) and ATR (0°/180°) maintained functional acuity with minimal differences across vergences. At +2.00 D, ATR preserved intermediate and very near performance more effectively (approximately −2.00 D to −3.50 D), whereas WTR tended to preserve sharper distance acuity near plano. At +3.00 D, the same pattern persisted—ATR relatively superior at intermediate/near and WTR relatively superior at distance—although both orientations resulted in clinically meaningful deterioration overall due to the higher cylinder magnitude.
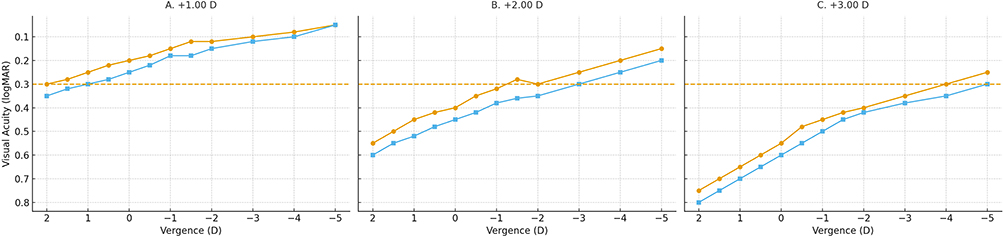 |
Figure 2 Defocus curves comparing ATR and WTR at +1.00 D (A), +2.00 D (B), and +3.00 D (C). Axis convention (plus-cylinder): WTR = 90°, ATR = 0°/180°. Dashed line indicates 0.3 logMAR (20/40). |
Statistical Analysis
Repeated-measures ANOVA showed significant main effects for cylinder magnitude (p<0.01) and vergence (p<0.01), and a significant interaction between axis and vergence near plano and +0.50 D (p<0.05). Tukey post hoc comparisons confirmed that +2.00 D and +3.00 D differed from control across most vergences, while +1.00 D generally did not. These analyses support a practical tolerance envelope of approximately +1.00 D for EDOF IOL recipients; beyond this level, functional penalties become evident and expand across the defocus curve.
Discussion
This study quantified the functional impact of optically induced regular astigmatism after implantation of an extended depth-of-focus (EDOF) intraocular lens by combining defocus curves with explicit axis analysis. Three consistent observations emerged across the dataset. First, distance visual acuity remained largely functional under +1.00 D, whereas +2.00 D produced clinically relevant decrements and +3.00 D caused broad deterioration along the defocus curve. Second, axis orientation modulated performance: with-the-rule (WTR, 90°) tended to preserve distance acuity near plano, while against-the-rule (ATR, 0°/180°) relatively favored intermediate and very near vergences. Third, these axis-dependent differences were present at all cylinder levels but were most evident at +2.00 D, where clinical trade-offs are easiest to appreciate.
The magnitude-dependent pattern aligns with current knowledge about presbyopia-correcting optics. Diffractive multifocal and trifocal lenses are more sensitive to residual ametropia and show decrements in visual performance even with modest cylinders, reflecting the penalty of splitting light into multiple foci.9,10 In contrast, EDOF designs, which elongate the focal zone rather than create discrete focal points, generally show slightly greater tolerance to low residual cylinders, often up to about 0.50–1.00 D, while values beyond ~1.00 D consistently produce clinically meaningful losses, especially at distance.11–14 Our finding that +1.00 D was broadly tolerated, whereas +2.00 D and +3.00 D produced progressively larger penalties, is therefore congruent with prior clinical and psychophysical evidence indicating that small cylinders (≈0.50–0.75 D) can already reduce visual quality and that ≥1.00 D frequently crosses a pragmatic threshold of functional impact in eyes with presbyopia-correcting optics.6–8,11,12,14
Axis orientation behaved as predicted by optical theory and empirical work. With a steeper vertical meridian, WTR tends to maintain sharper distance contours. In contrast, ATR shifts the circle of least confusion, effectively extending the depth of focus toward intermediate and near tasks.15–17 In the present series, the ATR advantage was most evident at vergences that map to common working distances, approximately −1.50 D to −2.50 D (about 66 to 40 cm), which correspond to computer and reading ranges. At the same time, WTR preserved distance around plano, a priority for activities such as driving. These axis-resolved results are clinically relevant in the context of age-related corneal remodeling, which shows a well-documented shift from WTR to ATR with aging; such remodeling can alter how residual astigmatism is perceived postoperatively and should be factored into lens selection and counseling.18,19 Recent clinical studies further support the idea that ATR may preserve intermediate performance more effectively, whereas WTR tends to maintain distance clarity, a pattern that closely mirrors our defocus curves.20–22
Methodologically, induced-defocus paradigms provide within-subject, lens-specific characterization of functional performance across vergences and have become a standard framework to benchmark presbyopia-correcting IOLs [23,24.25]. Using a photopic, high-contrast ETDRS protocol reduces ceiling effects and supports reproducibility. In this context, separating cylinder magnitude from axis orientation clarifies which component drives losses at each vergence. The present analysis focuses on WTR (90°) and ATR (0°/180°) because these orientations are the most clinically actionable and best represented in the literature; oblique axes were collected but intentionally not emphasized here to maintain clarity and because their functional profile commonly falls between the WTR and ATR extremes in everyday tasks. Nonetheless, the absence of a dedicated analysis of oblique astigmatism constitutes a limitation, as oblique axes (45° and 135°) may present intermediate behavior that could refine axis-specific interpretation.
The interaction between magnitude and axis has direct practical implications. For patients implanted with EDOF IOLs, residual cylinders around +1.00 D were generally tolerated, while +2.00 D and +3.00 D produced broad functional penalties along the defocus curve. When small residuals are unavoidable, tailoring the axis to visual priorities can be helpful: ATR tends to favor intermediate/near tasks (eg, office work, reading, smartphone use), whereas WTR better supports distance acuity. This does not imply that leaving the cylinder is desirable; rather, it provides a framework for risk-benefit discussions when perfect neutrality is uncertain, and it emphasizes that the magnitude should remain low to avoid global degradation.6–8,11–17,20–22 These principles should be integrated with careful preoperative planning and counseling that acknowledge the natural WTR-to-ATR corneal evolution with age and the patient’s visual demands.18,19 However, patient-reported outcomes (such as visual satisfaction, photic phenomena, and functional complaints) were not collected, which limits the ability to correlate objective findings with subjective experience.
The present findings are also consistent with broader differences among presbyopia-correcting platforms. Compared with diffractive multifocal and trifocal lenses—which can show clear penalties with relatively small cylinders9,10—EDOF optics typically provide a slightly wider tolerance window at low cylinder levels.11–14 Even within non-diffractive presbyopia-oriented designs, tolerance is not uniform and depends on the specific optical design; some designs deliver tolerance closer to that of conventional monofocals, while others confer modest but clinically meaningful robustness under ATR at intermediate vergences.11,12,23–25 Because real-world performance depends on multiple interacting factors, biometry accuracy, posterior corneal power, surgically induced astigmatism, ocular surface stability, and individual neural adaptation, these lens-specific characteristics should be interpreted within the context of comprehensive surgical planning and postoperative optimization.3–8,11–14,18–25 Additionally, as all measurements were performed monocularly, the study does not capture potential binocular summation effects, which in clinical practice often enhance contrast and improve distance performance compared to monocular viewing. Furthermore, only photopic and high-contrast acuity were assessed; mesopic conditions, glare/halo perception, and contrast sensitivity, which are clinically relevant, especially for EDOF lenses, were not evaluated.26
This study has limitations, including a modest sample size and a single-center design, which limit precision for small effect sizes and generalizability. The use of optically induced regular astigmatism provides a controlled model but does not fully replicate postoperative irregular astigmatism or neural adaptation dynamics.
In summary, the study met its objective by defining clinically relevant tolerance limits to induced astigmatism after EDOF implantation and by demonstrating that axis orientation meaningfully modulates functional performance. In practical terms, about +1.00 D represents a reasonable upper bound for tolerance, +2.00 D and +3.00 D produce progressive losses across the defocus curve, WTR better preserves distance, and ATR relatively supports intermediate and near. These findings provide actionable thresholds and axis-aware guidance for toric planning, residual-targeting, and patient counseling in EDOF cataract surgery.
Ethics
Approved by the Research Ethics Committee of the Hospital Oftalmológico de Brasília; written informed consent obtained from all participants.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Davidson RS, Dhaliwal D, Hamilton DR. et al. Surgical correction of presbyopia. J Cataract Refract Surg. 2016;42(7):920–930. doi:10.1016/j.jcrs.2016.05.003
2. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol (Phila). 2020;9(3):194–202. doi:10.1097/APO.0000000000000296
3. de Vries NE, Webers CAB, Touwslager WRH, et al. Dissatisfaction after implantation of multifocal intraocular lens. J Cataract Refract Surg. 2011;37(5):859–865. doi:10.1016/j.jcrs.2010.11.032
4. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992–997. doi:10.1016/j.jcrs.2009.01.031
5. Gundersen KG, Makari S, Ostenstad S, Potvin R. Retreatments after multifocal intraocular lens implantation: an analysis. Clin Ophthalmol. 2016;10:365–371. doi:10.2147/OPTH.S100840
6. Berdahl JP, Hardten DR, Kramer BA, Potvin R. Effect of astigmatism on visual acuity after multifocal versus monofocal intraocular lens implantation. J Cataract Refract Surg. 2018;44(10):1192–1197. doi:10.1016/j.jcrs.2018.06.048
7. Villegas EA, Alcón E, Artal P. Minimum amount of astigmatism that should be corrected. J Cataract Refract Surg. 2014;40(1):13–19. doi:10.1016/j.jcrs.2013.09.010
8. Lehmann RP, Houtman DM. Visual performance in cataract patients with low levels of postoperative astigmatism: full correction versus spherical-equivalent correction. Clin Ophthalmol. 2012;6:333–338. doi:10.2147/OPTH.S28241
9. Hayashi K, Manabe SI, Yoshida M, Hayashi H. Effect of astigmatism on visual acuity in eyes with a diffractive multifocal intraocular lens. J Cataract Refract Surg. 2010;36(8):1323–1329. doi:10.1016/j.jcrs.2010.02.016
10. Hayashi K, Yoshida M, Igarashi C, Hirata A. Effect of refractive astigmatism on all-distance visual acuity in eyes with a trifocal intraocular lens. Am J Ophthalmol. 2021;221:279–286. doi:10.1016/j.ajo.2020.07.051
11. Rocha KM, Costa ED, Dodhia M, Waring GO. Tolerance to induced astigmatism with a monofocal intraocular lens designed to extend the depth of focus. J Refract Surg. 2023;39(4):222–228. doi:10.3928/1081597X-20230126-02
12. Wan KH, Au ACK, Kua WN, et al. Enhanced monofocal versus conventional monofocal intraocular lens in cataract surgery: a meta-analysis. J Refract Surg. 2022;38(8):538–546. doi:10.3928/1081597X-20220707-01
13. Carones F. Residual astigmatism threshold and patient satisfaction with bifocal, trifocal, and extended range of vision intraocular lenses. Open J Ophthalmol. 2017;7(01):1–7. doi:10.4236/ojoph.2017.71001
14. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth-of-focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
15. Remón L, Monsoriu JA, Furlan WD. Influence of different types of astigmatism on visual acuity. J Optom. 2017;10(3):141–148. doi:10.1016/j.optom.2016.07.003
16. Sawusch MR, Guyton DL. Optimal astigmatism to enhance depth of focus after cataract surgery. Ophthalmology. 1991;98(7):1025–1029. doi:10.1016/S0161-6420(91)32182-1
17. Rhim JW, Eom Y, Park SY, Kang SY, Song JS, Kim HM. Eyelid squinting improves near vision in against-the-rule and distance vision in with-the-rule astigmatism in pseudophakic eyes: an eye model experimental study. BMC Ophthalmol. 2020;20(1):4. doi:10.1186/s12886-019-1297-5
18. Ferrer-Blasco T, Montés-Micó R, Peixoto-de-Matos SC, González-Méijome JM, Cerviño A. Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35(1):70–75. doi:10.1016/j.jcrs.2008.09.027
19. Visser N, Bauer NJC, Nuijts RMMA. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg. 2013;39(4):624–637. doi:10.1016/j.jcrs.2013.02.020
20. Campos PT, Hida WT, Moscovici BK, et al. Comparison of tolerance to induced astigmatism in pseudophakic eyes implanted with dual-technology diffractive IOL and enhanced monofocal IOL. Indian J Ophthalmol. 2025;73(9):1302–1306. doi:10.4103/IJO.IJO_2224_24
21. Hida WT, Moscovici BK, Cortez CM, et al. Comparison of visual outcomes of bilateral dual-technology diffractive intraocular lens vs blended enhanced monofocal with dual-technology intraocular lens. J Cataract Refract Surg. 2024;50(4):401–406. doi:10.1097/j.jcrs.0000000000001374
22. De Melo IR, Hida WT, Moscovici BK, et al. Validation of clinical protocol of astigmatism induction in pseudophakic patients. Clin Ophthalmol. 2024;18:3375–3387. doi:10.2147/OPTH.S472752
23. Ang RE. Comparison of tolerance to induced astigmatism in pseudophakic eyes implanted with small-aperture, trifocal, or monofocal intraocular lenses. Clin Ophthalmol. 2019;13:905–911. doi:10.2147/OPTH.S208651
24. Pérez-Sanz L, Vega F, Azor-Morón JA, Cuellar F, Millán MS, Garzón N. Tolerance to residual astigmatism of an isofocal intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2024;262(4):1169–1180. doi:10.1007/s00417-023-06305-9
25. Hida WT, Vilar C, Moscovici BK, Motta AFP, Carricondo PC. A new methodology for evaluating the potential impact of residual refractive astigmatism in pseudophakic patients. Clin Ophthalmol. 2024;18:1909–1914. doi:10.2147/OPTH.S453340
26. Hida WT, Moscovici BK, Miziara PESC, et al. Clinical Tolerance to Induced Astigmatism in Eyes Implanted with a Single Extended Depth of Focus Intraocular Lens (AT LARA®). Clin Ophthalmol. 2019;19:4455–4462. PMID: 41377133; PMCID: PMC12687617. doi:10.2147/OPTH.S568747
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fluctuations of Anterior Chamber Depth and Astigmatism in Pseudophakic Eyes
Tutchenko L, Patel S, Skovron M, Voytsekhivskyy OV, Gilevska F
Clinical Ophthalmology 2024, 18:3739-3752
Published Date: 13 December 2024
Refractive Outcomes of a Low-Addition Refractive, Rotationally Asymmetric Bifocal IOL and Its Toric Version: A Comparative Cohort Study of 316 Eyes
Lognon A, Matagrin B, Agard E, El Chehab H, Verrecchia S, Levron A, Chudzinski R, Billant J, Goissaud-Mignard A, Fenniri I, Dot C
Clinical Ophthalmology 2026, 20:583057
Published Date: 1 May 2026