Back to Journals » Cancer Management and Research » Volume 12
Clinical Study on Prelaryngeal Lymph Node Metastasis in Papillary Thyroid Carcinoma
Authors Gong JX, Gu JW, Ji F, Li K, Zhu Q, Gu FY, Chen Y, Ji QH
Received 29 September 2019
Accepted for publication 26 November 2019
Published 21 February 2020 Volume 2020:12 Pages 1323—1327
DOI https://doi.org/10.2147/CMAR.S232884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Jin-Xing Gong,1 Jian-Wei Gu,1 Feng Ji,1 Kun Li,1 Qi Zhu,1 Fang-Ying Gu,1 Yan Chen,1 Qing-Hai Ji2
1Department Four of Surgery, Kunshan Hospital of Traditional Chinese Medicine, Kunshan 215300, People’s Republic of China; 2Head & Neck Surgery, Fudan University Shanghai Cancer Center, Shanghai 200000, People’s Republic of China
Correspondence: Jian-Wei Gu
Department Four of Surgery, Kunshan Hospital of Traditional Chinese Medicine, No. 189 of Chaoyang Street, Yushan Town, Kunshan 215300, People’s Republic of China
Tel +86-051257310000-3698
Email [email protected]
Objective: This study aims to investigate the risk factors of prelaryngeal lymph node metastasis in papillary thyroid carcinoma and its clinical application value.
Methods: The clinical pathological features and metastatic risks were statistically analyzed by reviewing 254 patients with papillary thyroid carcinoma, who received their first operation and prelaryngeal lymph node dissection in our department.
Results: The detection of prelaryngeal lymph nodes, tumor size and any paratracheal lymph node metastasis were correlated with the number of paratracheal lymph node metastasis (P< 0.05), but these were not correlated with age, gender, multiple foci, tumor size, any paratracheal lymph node metastasis, metastatic location, or foci location (P> 0.05).
Conclusion: Paratracheal lymph node metastasis indicates a high possibility of prelaryngeal lymph node metastasis. Paratracheal lymph node dissection combined with prelaryngeal lymph node dissection should be simultaneously considered in operations for thyroid papilla carcinoma.
Keywords: papillary thyroid cancer, delphian lymph node, lymph node metastasis, lymph node dissection, tumor
Introduction
Delphian lymph nodes (DLN) are also known as the prelaryngeal lymph nodes. These are located in the fascia of the superior thyroid isthmus, in front of annular cartilage and thyroid cartilage, cricothyroid membrane and annular cartilage surface, and are also one of the most common local lymph nodes with metastasis in thyroid carcinoma.1–3 However, although this is one of the most common local lymph nodes with metastasis in thyroid carcinoma, few studies have been reported. Furthermore, paratracheal lymph node dissection is often ignored.4,5 Therefore, the present study aims to observe the metastasis of prelaryngeal lymph nodes in papillary thyroid carcinoma, and explore its related factors and clinical value, in order to further improve the surgical method of thyroid cancer, and reduce postoperative recurrence and metastasis.
Materials and Methods
General Data
A total of 378 patients, who were pathologically diagnosed with papillary thyroid carcinoma in our department from 2014 to 2018, were retrospectively analyzed. A total of 254 patients, who underwent paratracheal lymph node dissection and prelaryngeal lymph node dissection for the first time, were statistically analyzed. In our study, it was therapeutic central neck dissection. This study was conducted in accordance with the declaration of Helsinki and approved by the Ethics Committee of Kunshan Hospital of Traditional Chinese Medicine. All participants signed informed consent.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) patients confirmed with papillary thyroid carcinoma through pathological data; (2) patients who underwent paratracheal lymph node dissection in the first operation; (3) patients who underwent prelaryngeal lymph node dissection in the first operation; (4) patients above 18 years old. Exclusion criteria: (1) patients with thyroid tumors caused by the distant metastasis of other tumors; (2) patients who suffered from advanced tumors in the state of cachexia; (3) patients and their family who have given up further treatment.
Observation Indicator
The age, gender, number of lesions, tumor size, paratracheal lymph node metastasis and lesion location were recorded for grouping and statistical analysis. The sum of the diameters of all lesions on the ipsilateral side was considered as the final tumor size.
Statistical Analysis
The SPSS 20.0 statistical software was used to process the data in the present study. Measurement data were expressed as mean ± standard deviation (x ± SD). Enumeration data were expressed in percentage (%). W-test was used for the normality test, F-test was used for the homogeneity test of variances, and t-test was used for comparison between the two groups. The nonparametric test was used to compare the mean of multiple samples that were non-normally distributed, or normally distributed, but had an uneven variance. Counting data were used for the chi-square test. P<0.05 was considered statistically significant.
Results
General Condition
Among the 254 patients in the present study, 63 patients were males and 191 patients were females, and the male-to-female ratio was 1.00:3.03. The mean age of these patients was 43.88 years old. Prelaryngeal lymph nodes were detected in 147 patients, with a detection rate of 57.9%. Among these patients, 25 patients had metastases, with a metastatic rate of 17.0%. The average metastases were 1.32 (1–4) lymph nodes. In 16 patients, the paratracheal lymph node metastases occurred at the same time, accounting for 64%. Furthermore, paratracheal lymph nodes were detected in 235 patients, with a detection rate of 92.5%. Among these patients, 99 patients had metastasis, with a metastatic rate of 42.1%.
Among the 254 patients, 234 received unilateral radical thyroidectomy and 20 received bilateral radical thyroidectomy, and the lymph nodes were dissected into ipsilateral or bilateral tracheal lymph nodes and anterior laryngeal lymph nodes (six cervical lymph nodes). The total number of prelaryngeal lymph nodes was 256.
Factors Correlated to the Detection of Prelaryngeal Lymph Nodes
The detection of prelaryngeal lymph nodes was correlated to the number of paratracheal lymph node metastases (P<0.05), but this was not correlated to age, gender, multiple foci, tumor size, any paratracheal lymph node metastasis, metastatic location and foci location (P>0.05, Table 1).
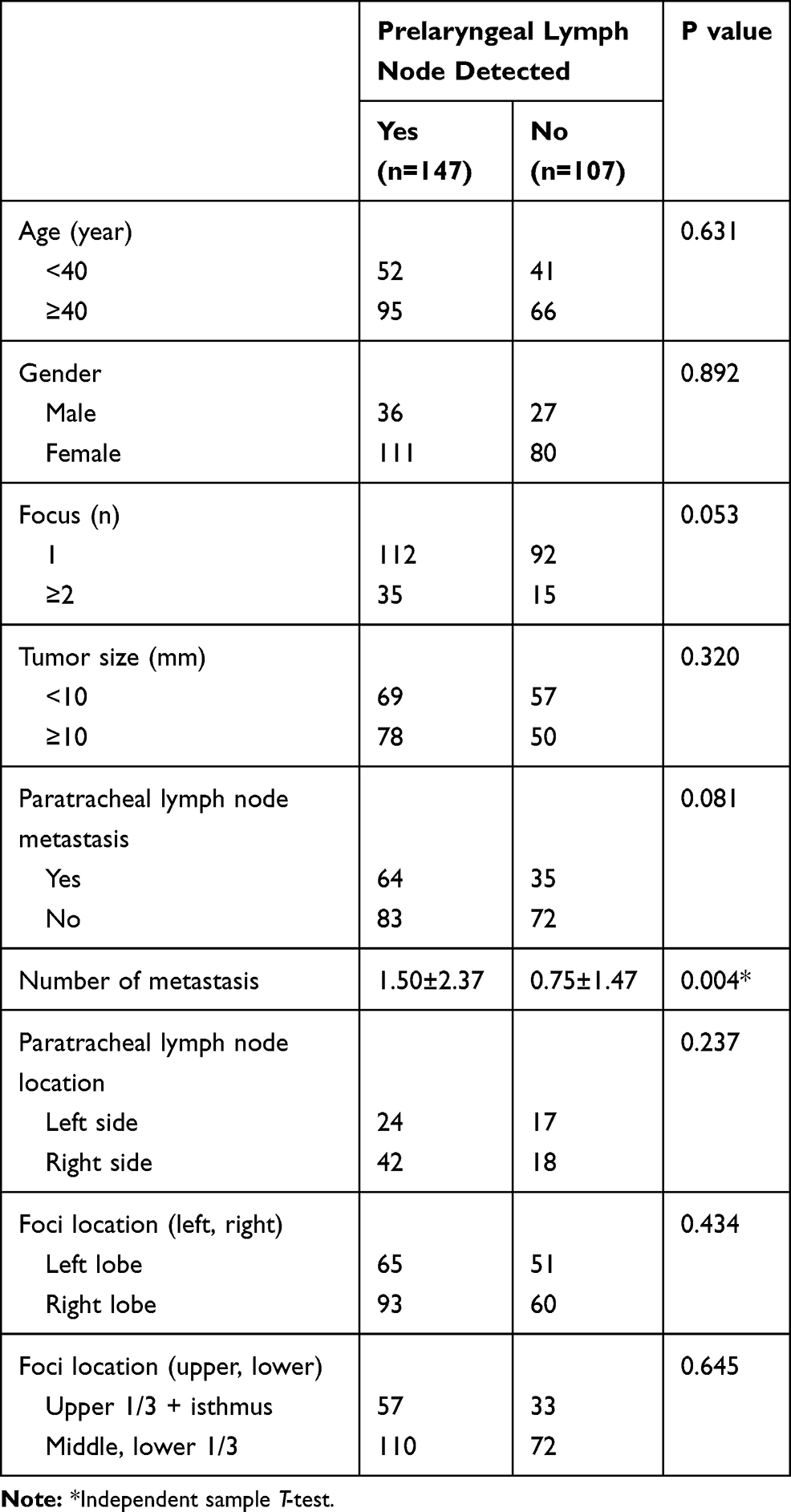 |
Table 1 Analysis of the Factors Correlated to Prelaryngeal Lymph Node Detection |
Risk Factors for Prelaryngeal Lymph Node Metastasis
The detection of prelaryngeal lymph nodes, tumor size and any paratracheal lymph node metastasis was correlated with the number of paratracheal lymph node metastases (P<0.05), but was not correlated with age, gender, multiple foci, tumor size, any paratracheal lymph node metastasis, metastatic location and foci location (P>0.05, Table 2).
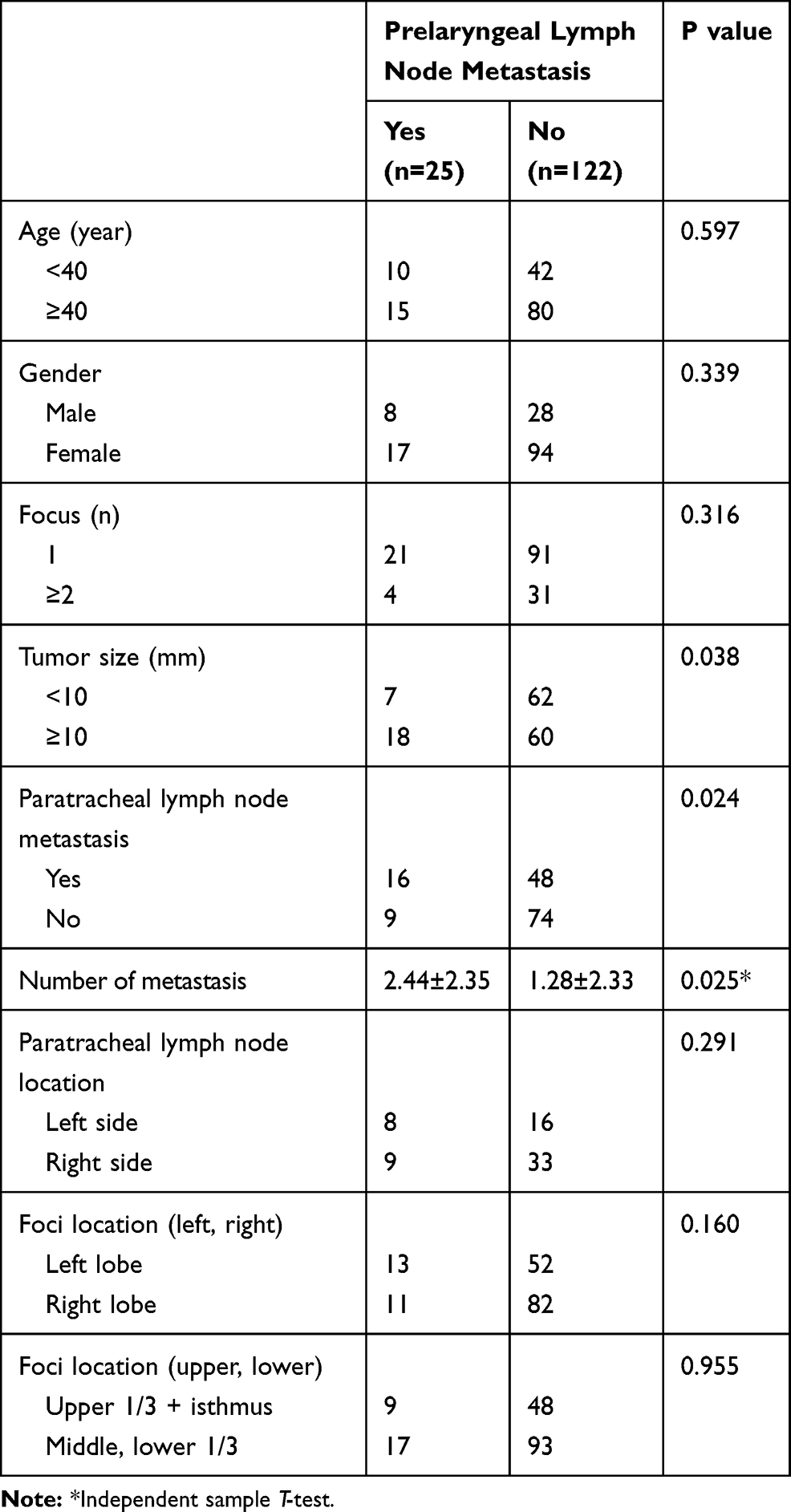 |
Table 2 Analysis of the Factors Correlated to Prelaryngeal Lymph Node Metastasis |
Multivariate Analysis of the Risk Factors Associated with Prelaryngeal Lymph Node Metastasis
Multivariate analysis of the risk factors associated with prelaryngeal lymph node metastasis showed that the metastasis of prelaryngeal lymph node was correlated with the metastasis of parastatal lymph node (p<0.05, Table 3).
 |
Table 3 Multivariate Analysis of the Risk Factors Associated with Prelaryngeal Lymph Node Metastasis |
Discussion
The results of the present study revealed that the detection of prelaryngeal lymph nodes was correlated with the number of paratracheal lymph node metastases, but was not correlated with age, gender, multiple foci, tumor size, any paratracheal lymph node metastasis, metastatic location and foci location. The prelaryngeal lymph node metastases were correlated with tumor size, any paratracheal lymph node metastasis, and the number of paratracheal lymph node metastasis, but were not correlated with age, gender, multiple foci, location of the paratracheal lymph node metastasis, and foci location.
Prelaryngeal lymph nodes were officially cited in the James Means textbook – Thyroid and Its Related Diseases, which particularly referred to prelaryngeal lymph nodes. This was later widely cited and accepted.6 However, as one of the most common local lymph nodes with metastasis in thyroid carcinoma, few studies have been reported. Furthermore, paratracheal lymph node dissection is often ignored.7,8 The present study revealed that prelaryngeal lymph node metastasis is correlated with the tumor size of the papillary thyroid carcinoma, any metastasis of the paratracheal lymph nodes, and the number of paratracheal lymph node metastases (P<0.05). This is basically consistent with the reports of other studies.3,9–11 It has been suggested that prelaryngeal lymph node metastasis predicts the possibility of paratracheal lymph node metastasis and the increase in the number of metastases.12,13 In addition, nine of 25 patients with prelaryngeal lymph node metastasis were not accompanied by paratracheal lymph node metastasis at the same time. This suggests that attention should be given to the metastasis of prelaryngeal lymph nodes and the choice of surgical methods in the treatment of papillary thyroid carcinoma.
Some studies suggest that most of the prelaryngeal lymph nodes are drained from tumors in the thyroid lobe, thyroid isthmus, and anterior superior pyramidal lobe. In addition, the prelaryngeal lymph node metastasis is closely correlated with the location of the lesions, especially in the thyroid isthmus and upper 1/3 of the thyroid gland.14,15 However, the results of the present study revealed that the difference in the location of the lesions was not significant (including the left and right, and superior and inferior) in prelaryngeal lymph node metastasis, and this is consistent with the results reported by Zheng et al.16 This may be correlated to the sample size, which needs to be further investigated and discussed.
In addition, in the comparison between detected prelaryngeal lymph nodes and the undetected group, it was found that the detection of prelaryngeal lymph nodes was correlated with the number of paratracheal lymph node metastases (P<0.05). That is, the greater the number of paratracheal lymph node metastases, the easier it would be to detect the prelaryngeal lymph nodes. Therefore, there is a reason to consider that this can reflect the relationship between prelaryngeal lymph node metastasis and paratracheal lymph node metastasis from the other side.
The investigators consider that paratracheal lymph node dissection should be considered in the operation of papillary thyroid carcinoma, especially when the tumor is ≥10 mm. Furthermore, although the prognosis of papillary thyroid carcinoma is relatively good, there is a lack of long-term follow-up data.17–20 More and more studies have revealed the importance of prelaryngeal lymph nodes in the metastasis of papillary thyroid carcinoma. Therefore, there is a need to carry out follow-up studies, in order to determine whether the postoperative recurrence and metastasis of papillary thyroid carcinoma can be reduced after prelaryngeal lymph node dissection.
The present study has the following limitations. First, the present study is an observational study, and not a randomized controlled trial. Therefore, there is still a certain risk of bias. Second, the present study was a single-center clinical study, and the sample size is small. Thus, there is a need to further increase the sample size and conduct multicenter clinical research. Finally, the correlation between prelaryngeal lymph node metastasis and thyroid papilla carcinoma in the present study needs to be further investigated.
Conclusion
Paratracheal lymph node metastasis indicates a high possibility of prelaryngeal lymph node metastasis. Paratracheal lymph node dissection combined with prelaryngeal lymph node dissection should be simultaneously considered in the operation of thyroid papilla carcinoma.
Disclosure
The authors declared that there is no conflict of interest in this work.
References
1. Chen Q, Wei T, Wang XL, Li ZH, Du ZH, Zhu JQ. The total number of prelaryngeal and pretracheal lymph node metastases: is it a reliable predictor of contralateral central lymph node metastasis in papillary thyroid carcinoma? J Surg Res. 2017;214:162–167. doi:10.1016/j.jss.2015.02.056
2. Lee YC, Shin SY, Kwon KH, Eun YG. Incidence and clinical characteristics of prelaryngeal lymph node metastasis in papillary thyroid cancer. Eur Arch Otorhinolaryngol. 2013;270(9):2547–2550. doi:10.1007/s00405-013-2471-7
3. Kim WW, Yang SI, Kim JH, Choi YS, Park YH, Kwon SK. Experience and analysis of Delphian lymph node metastasis in patients with papillary thyroid carcinoma. World J Surg Oncol. 2012;10:226–232. doi:10.1186/1477-7819-10-226
4. Lee YC, Na SY, Park GC, Han JH, Kim SW, Eun YG. Occult lymph node metastasis and risk of regional recurrence in papillary thyroid cancer after bilateral prophylactic central neck dissection: a multi-institutional study. Surgery. 2017;161(2):465–471. doi:10.1016/j.surg.2016.07.031
5. Dai W, Jiang B, Chen W, Han L. The significance of lymph node dissection in the VI area of cN0 thyroid papillary carcinoma. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016;30(4):319–321.
6. Santrac N, Besic N, Buta M, et al. Lymphatic drainage, regional metastases and surgical management of papillary thyroid carcinoma arising in pyramidal lobe – a single institution experience. Endocr J. 2014;61(1):55–59. doi:10.1507/endocrj.EJ13-0316
7. lyer NG, Shaha AR, Ferlito A. Delphian node metastasis in head and neck cancers – oracle or myth? J Surg Oncol. 2010;102(4):354–358. doi:10.1002/jso.21640
8. Hao SL, Song XC, Jiang LX, Zheng HT. Significance and research progress of delphian lymph node in thyroid cancer. Chin J Gen Surg. 2016;31(12):1067–1068.
9. Iyer NG, Kumar A, Nixon IJ, et al. Incidence and significance of Delphian node metastasis in papillary thyroid cancer. Ann Surg. 2011;253(5):988–991. doi:10.1097/SLA.0b013e31821219ca
10. Isaacs JD, Lundgren CI, Sidhu SB, Sywak MS, Edhouse PJ, Delbridge LW. The Delphian lymph node in thyroid cancer. Ann Surg. 2008;247(3):477–482. doi:10.1097/SLA.0b013e31815efdc4
11. Oh EM, Chung YS, Lee YD. Clinical significance of Delphia lymph node metastasis in papillary thyroid carcinoma. World J Surg. 2013;37(11):2594–2599. doi:10.1007/s00268-013-2157-8
12. Lee YC, Na SY, Chung H, Kim SI, Eun YG. Clinicopathologic characteristics and pattern of central lymph node metastasis in papillary thyroid cancer located in the isthmus. Laryngoscope. 2016;126(10):2419–2421. doi:10.1002/lary.25926
13. Ji YB, Yoo HS, Song CM, Park CW, Lee CB, Tae K. Predictive factors and pattern of central lymph node metastasis in unilateral papillary thyroid carcinoma. Auris Nasus Larynx. 2016;43(1):79–83. doi:10.1016/j.anl.2015.09.005
14. Hunt JP, Buchmann LO, Wang L, Abraham D. An analysis of factors predicting lateral cervical nodal metastasis in papillary carcinoma of the thyroid. Arch Otolaryngol Head Neck Surg. 2011;137(11):1141–1145. doi:10.1001/archoto.2011.174
15. Chai YJ, Kim SJ, Choi JY, Koo Do H, Lee KE, Youn YK. Papillary thyroid carcinoma located in the isthmus or upper third is associated with Delphian lymph node metastasis. World J Surg. 2014;38(6):1306–1311. doi:10.1007/s00268-013-2406-x
16. Zheng GB, Hao SL, Liu XC, et al. The clinical significance of Delphian lymph node metastasis in papillary thyroid cancer. Chin J Otorhinolaryngol Head Neck Surg. 2016;51(11):842–845.
17. Guleria P, Agarwal S, Iyer VK, Jain D, Mathur SR, Yadav D. Subcategorisation of AUS/FLUS thyroid lesions as per the 2017 Bethesda system for reporting thyroid cytopathology: a retrospective study from a tertiary care centre analysing risk of malignancy (ROM) of the different subcategories. J Clin Pathol. 2019;
18. Jat MA. Comparison of surgeon-performed ultrasound-guided fine needle aspiration cytology with histopathological diagnosis of thyroid nodules. Pak J Med Sci. 2019;35(4):1003–1007. doi:10.12669/pjms.35.4.537
19. Cheng X, Xu S, Pan J, et al. MKL1 overexpression predicts poor prognosis in patients with papillary thyroid cancer and promotes nodal metastasis. J Cell Sci. 2019;132(16):jcs231399. doi:10.1242/jcs.231399
20. Ma LJ, Wang SX, Zhu GQ. Multiple papillary carcinoma of thyroid with extensive metastasis of the lateral neck and parapharyngeal: a case report. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019;33(7):675–676. doi:10.13201/j.issn.1001-1781.2019.07.025
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.