Back to Journals » Clinical Ophthalmology » Volume 14
Clinical Results After Precision Pulse Capsulotomy
Authors Gundersen KG ![]() , Potvin R
, Potvin R ![]()
Received 24 November 2020
Accepted for publication 16 December 2020
Published 29 December 2020 Volume 2020:14 Pages 4533—4540
DOI https://doi.org/10.2147/OPTH.S293819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kjell G Gundersen,1 Richard Potvin2
1iFocus Øyeklinikk AS, Haugesund, Norway; 2Science in Vision, Bend, OR, USA
Correspondence: Kjell G Gundersen
iFocus Øyeklinikk AS, Sørhauggata 111, Haugesund 5527, Norway
Tel +47 52808902
Email [email protected]
Purpose: To compare residual refractive error and complication rates between eyes undergoing a manual capsulotomy and those receiving a precision pulse capsulotomy using an automated device.
Patients and Methods: This study was a non-interventional two-arm retrospective chart review of clinical results after bilateral cataract surgery or refractive lens exchange (RLE) surgery with a monofocal toric intraocular lens (IOL) or a trifocal IOL where a manual capsulorhexis (Manual) or automated precision pulse capsulotomy (PPC) was performed.
Results: Exams from 243 eyes (122 PPC, 121 Manual) from 124 patients were reviewed; about 75% of which had a trifocal IOL implanted. There was no statistically significant difference in the MRSE with either IOL type, or overall. The overall percentage of eyes with residual refractive cylinder ≤ 0.50 D was significantly higher in the PPC group (89% vs. 79% in the manual group, p = 0.03), primarily driven by results with the toric IOL. Best corrected distance visual acuity was not statistically significantly different by group. Capsulotomy-related complications were lower in the PPC group relative to the manual group (4.1% vs. 6.6%), but this result was not statistically significant (p = 0.38).
Conclusion: Significantly more eyes had refractive cylinder ≤ 0.50 D in the PPC group. For all other measures, the automated PPC device produced clinical results equivalent to those achieved with a manual capsulorhexis.
Keywords: precision pulse capsulotomy, cataract surgery, capsulorhexis, capsulotomy
Plain Language Summary
When surgeons perform cataract surgery, one of the most important procedures is creating an opening in the lens of the eye so that the contents can be removed and replaced with an intraocular lens (IOL). The surgeon can create this opening manually (with a pair of forceps) or with a femtosecond laser system. The former requires excellent surgical technique. The latter is more precise but requires a dedicated (and expensive) laser system. A third alternative is a relatively new hand-held device that allows for precision in the placement, size and circularity of the opening. The location, size and circularity of the opening are important to good clinical outcomes after surgery. This study was designed to determine if the results with the hand-held device were as good or better than those achieved using a manual technique.
Results indicated that visual acuity and the overall refractive error (the prescription in glasses after surgery) were similar with both techniques, though more eyes had low astigmatism after surgery with the hand-held device. The number of surgical complications was low in both groups. While complications were slightly lower with the hand-held device, the difference was not significant. This indicates that use of the hand-held device may have some slight advantages over a manual technique.
Introduction
A critical component of successful cataract surgery is the creation of the anterior capsulotomy. A properly sized, centered and circular capsulotomy ensures that the intraocular lens (IOL) optic is uniformly captured, increasing the likelihood of IOL stability post-surgery, a critical element in refractive stability.1 Precise edges reduce the likelihood of anterior capsule tears and increase the mechanical strength of the remaining capsule.2 Complete overlap of the intraocular lens (IOL) reduces the likelihood of future posterior capsule opacification (PCO).3
Continuous curvilinear capsulorhexis (CCC), a manual technique, is arguably the most common method of creating a capsulotomy at present. While generally effective, creating a good CCC is recognized as one of the most challenging aspects of cataract surgery.4 Associated complications can include anterior capsule tears, a non-circular shape and an off-center location, all of which may compromise clinical outcomes.5
Femtosecond laser systems can also be used to create a capsulotomy. Analyses of large data sets suggest that there are no significant advantages to using a femtosecond laser.6,7 Complication rates appear similar to those experienced with manual techniques.8 Some studies have shown a better ability to maintain centration and circularity with femtosecond laser systems, but at the cost of a more ragged edge from the laser pulses.9 Others have indicated that automated capsulotomy with femtosecond laser systems may be helpful in complicated cases such as white cataracts.10 Frequent concerns related to the use of femtosecond laser systems are related to the cost of the device and the increased procedure time.
An alternative to using forceps or a femtosecond laser system to create a capsulotomy is the Zepto® Precision Cataract Surgery device, referred to in this paper as the precision pulse capsulotomy (PPC) device. It is a small hand-held device designed to create an automated, strong, symmetrical, and circular anterior capsulotomy that can be precisely aligned to the patient’s visual axis. A clear suction cup securely fastens a nitinol ring to the anterior capsule, allowing delivery of several short bursts of electrical energy which cleave the capsule in about 4 ms.11 Patient fixation can be controlled to facilitate placement of the capsulotomy on the visual axis.12 The short time taken to create the entire capsulotomy reduces potential stress on the zonules and eliminates the shear stress associated with the tearing action of a manual capsulorhexis; both of these factors, and the mechanism of action, contribute to a higher edge tear strength post-capsulotomy.13 Previous clinical results have demonstrated the efficacy of the device.14–16 As with the femtosecond laser systems, there is some evidence that an automated capsulotomy that does not induce zonular stress may be helpful in complicated cases.15
The purpose of the current study was to retrospectively review refractive outcomes and complications in a high number of cases completed using the PPC device, comparing them to a similar set of cases completed using a manual CCC technique.
Patients and Methods
This study was a non-interventional two-arm retrospective review of clinical results after bilateral cataract surgery or refractive lens exchange (RLE) surgery with IOL implantation. As a retrospective review, there was no masking and no randomization. Results using manual (forceps) capsulotomy (Manual) were compared to those achieved using the PPC device. Regional ethics committee approval through the Regionale komiteer for medisinsk og helsefaglig forskningsetikk (REK), Norway was applied for and waived by the committee because the study was considered a quality control investigation. Patient data were deidentified for analysis. As the study was non-interventional there was no requirement to register it as a clinical trial. The study was conducted in accordance with the tenets of the Declaration of Helsinki and good clinical practice. Data are not available for sharing.
Except for the method of capsulotomy creation, all surgeries in both groups were completed in the same fashion by one surgeon (KGG) using the same optical biometry, incision size/location and surgical planning routine. The Verion™ Image Guided System (Alcon, Fort Worth, USA) was used for toric IOL alignment. Eyes included had to have undergone uncomplicated cataract surgery with no clinically significant preoperative pathology that might have affected the postoperative refraction, with clinical data available 90 to 180 days postoperative. Eyes with suboptimal outcomes unrelated to the method of capsulotomy used (e.g. cystoid macular edema) were excluded. Use of the precision pulse capsulotomy device in the practice was most common when single vision toric IOLs or trifocal IOLs were being implanted; data collected in both groups were restricted to those lens types. All toric IOLs were Acrysof® IQ toric lenses and all trifocal IOLs were Acrysof® Panoptix® lenses (both Alcon, Fort Worth, USA).
The measure of primary interest was the percentage of patients who had a postoperative refraction within 0.50 D of the intended spherical equivalent target. Other measures of interest included the rate of complications at the time of surgery (e.g. anterior capsular tears, posterior capsule rupture with vitreous loss). The correlation of results with anterior chamber depth (ACD), axial length or the presence of ocular pathology will also be examined where sufficient data are available.
Sample size calculations suggested that 120 eyes in each group would be sufficient to detect clinical differences in the outcomes measured. At one point in time, the PPC device was adopted to treat all eyes receiving toric monofocal and trifocal IOLs. Clinical data were extracted by working backward from that point for the manual results and forward from that point for PPC results to reach the desired number of cases. As a single practice in a restricted geographical area loss to follow up is rarely observed.
Clinical data were extracted from the patient files and collated in an Excel file, then imported into MS Access for data checking and preliminary analysis (both Microsoft Corp., Redmond, WA, USA). The STATISTICA data analysis software system, version 12 (TIBCO Software Inc., Palo Alto, CA, USA) was used to perform between-group comparisons. Subgroup analysis was based on IOL type. Continuous variables were compared using an analysis of variance (ANOVA) while the Chi-squared test was used to compare non-parametric variables. In both cases statistical significance was based on p ≤ 0.05.
Results
A total of 243 eyes from 124 patients were eligible for inclusion (5 subjects had only one eye included). About 75% of subjects in both groups were implanted with the same trifocal IOL, with the remaining 25% implanted with the same monofocal toric IOL. There was no statistically significant difference in the ratio of multifocal to toric IOLs between the Manual and PPC groups (p = 0.69). Table 1 summarizes the demographic characteristics of the study population. There were no statistically significant differences between the Manual and PPC groups for any of the measured variables. Patients receiving trifocal IOLs were statistically significantly younger than those receiving the toric monofocal (p < 0.001), but this was the case in both the Manual and PPC groups. Average keratometry was statistically significantly higher in eyes receiving the toric IOL (p < 0.001), as expected, but again this was the case in both the Manual and PPC groups.
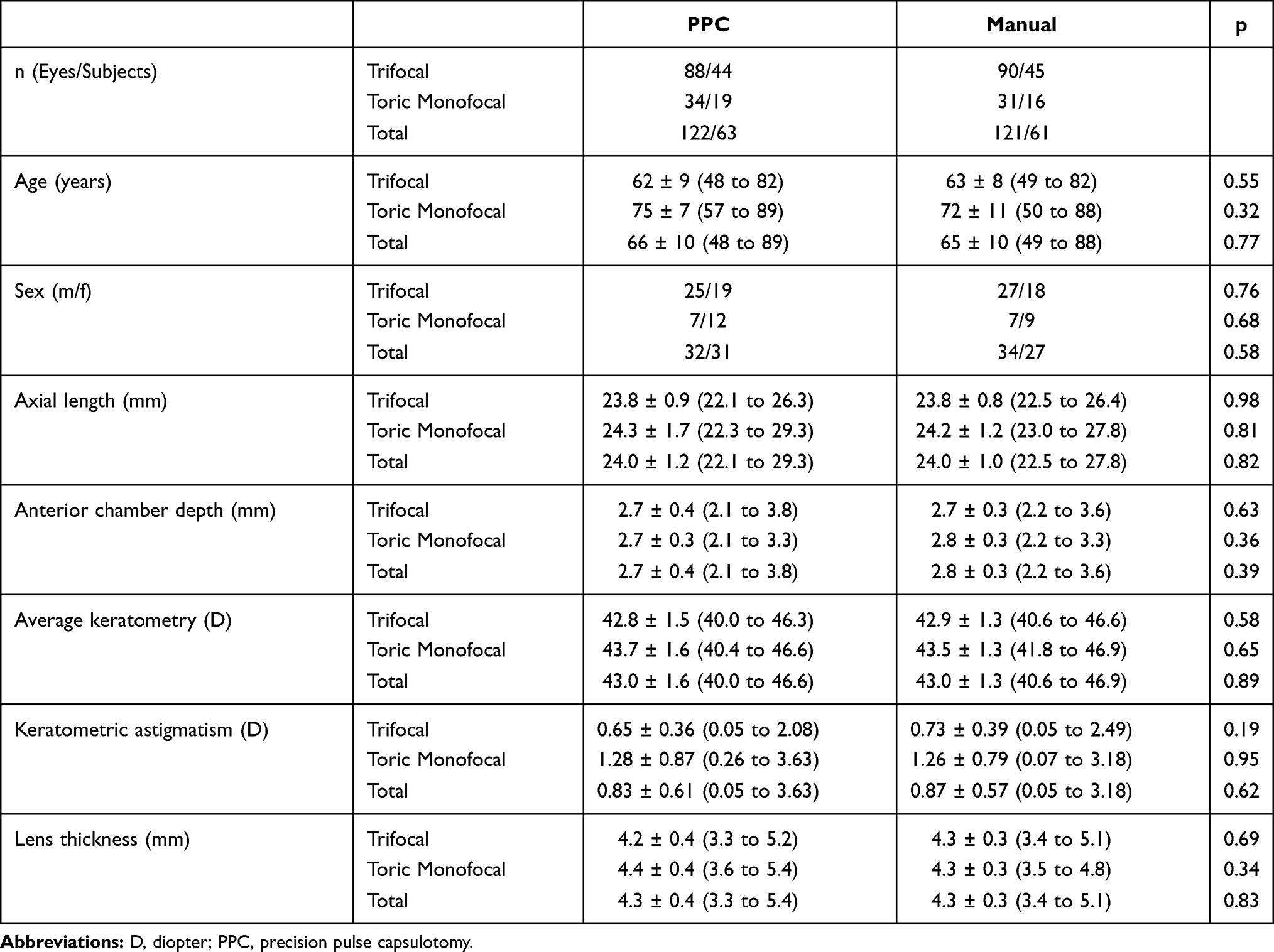 |
Table 1 Demographics and Biometry |
Figure 1 shows the results of an analysis of variance of the difference between the expected and actual residual mean spherical equivalent refractions by IOL type and capsulotomy type, adjusted to account for monovision targets in some eyes. There was a statistically significant difference in results by IOL type (p < 0.001), but not by capsulotomy type (p = 0.37); there was also no interaction effect (p = 0.84).
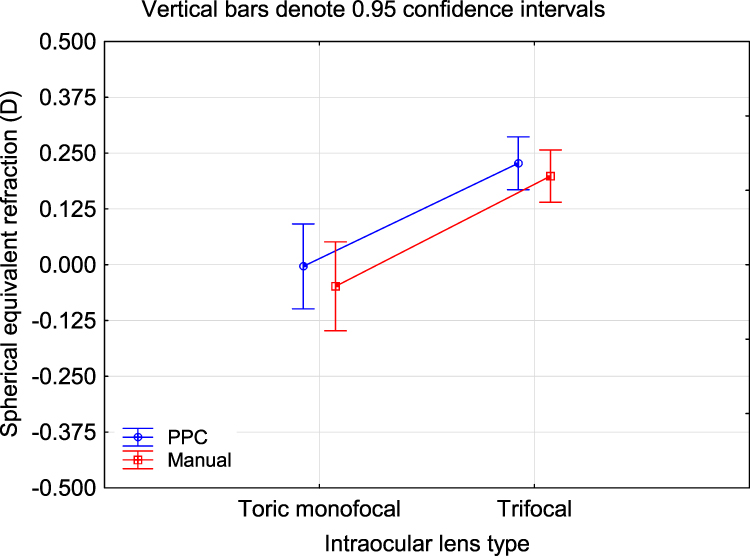 |
Figure 1 Mean spherical equivalent refraction by IOL type and rhexis method (adjusted by the target refraction for monovision eyes). Abbreviations: D, diopter; PPC, precision pulse capsulotomy. |
Figure 2 shows the results of an analysis of variance for the residual refractive cylinder by IOL type and capsulotomy group. There was a statistically significant difference in the results by capsulotomy type (p = 0.011), with this result primarily driven by differences in the eyes implanted with toric IOLs. The mean residual refractive cylinder of the PPC group was about 0.15D lower than for the Manual group in this subset of eyes.
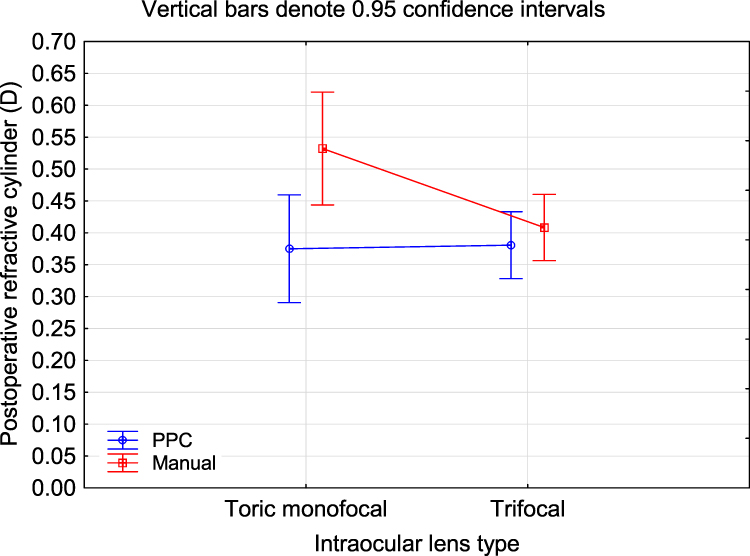 |
Figure 2 Residual refractive cylinder by IOL type and rhexis method. Abbreviations: D, diopter; PPC, precision pulse capsulotomy. |
Table 2 shows the number of eyes with a spherical equivalent refraction within 0.50 D of intended, and the number of eyes with residual refractive cylinder ≤0.50 D. While there was a trend evident for the number of eyes with an MRSE within 0.50 D of intended, there was no statistically significant difference in the MRSE with either IOL type or overall. The residual refractive cylinder was statistically significantly lower in the PPC group for the toric IOL type and overall.
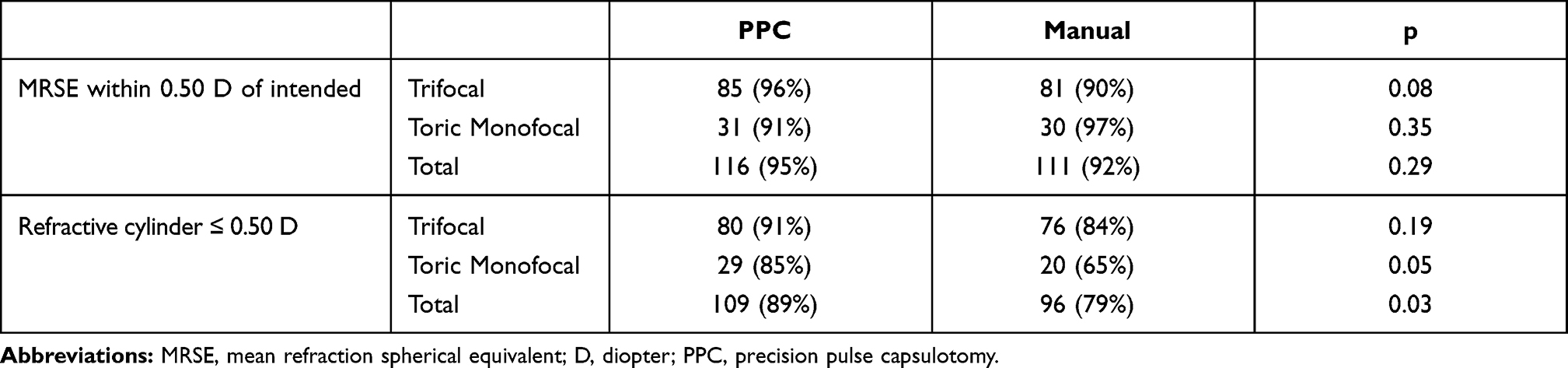 |
Table 2 Residual Refractive Data |
Figure 3 shows the best corrected distance visual acuity by IOL type and Group. There was a statistically significant difference by IOL type (about 2 logMAR letters, p < 0.001), but no statistically significant difference by capsulotomy type for either IOL type, or overall.
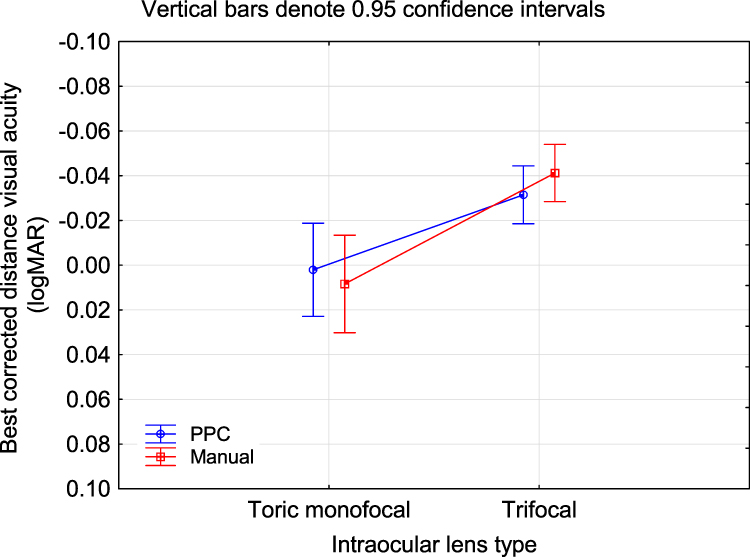 |
Figure 3 Best corrected distance visual acuity by IOL type and rhexis method. Abbreviations: logMAR, log of the minimum angle of resolution; PPC, precision pulse capsulotomy. |
There were eight patients (15 eyes) with preoperative co-morbidity, 5 patients with glaucoma and 3 with diabetes, too few eyes for reliable statistical analysis. There was no evident correlation between these co-morbidities and the clinical results reported above.
During surgery, there were 5 reported anterior capsule tears in the PPC group (4.1%) and 8 in the Manual group (6.6%). While lower in the PPC group, the difference was not statistically significant (p = 0.38). Of these, two eyes in the PPC group (1.6%) and 3 eyes in the Manual group (2.5%) experienced vitreous loss with anterior vitrectomy performed; again, the incidence was lower in the PPC group, but the difference was not statistically significant (p = 0.64).
Discussion
The current study demonstrated that, in a large sample from one site with a single, very experienced surgeon, the PPC device produced clinical results as good as manual continuous curvilinear capsulorhexis, with slightly, but statistically significantly better results in terms of residual refractive astigmatism after surgery.
The lack of a difference in mean spherical equivalent refraction, as found here, appears consistent with the findings of Bang et al,17 though they reported more variability in the effective lens position for the manual capsulorhexis group relative to their PPC group. Effective lens position was not directly measured in the current study.
A higher percentage of eyes with residual refractive astigmatism ≤0.50 D with the toric IOLs, and overall, appears driven by the toric results, as is apparent in Table 2. Accurate biometry, predictable placement and rotational stability are well-established criteria critical to the success of toric IOLs in correcting astigmatism.18 Given that planning, biometry and surgery were completed by one surgeon at one clinic, the findings here suggest that the PPC group had a higher level of rotational stability. This may be a function of the optimized size, circularity and location of the capsulotomy; the PPC capsulotomy has been reported to be more consistent in these regards than a manual capsulorhexis.17 A more uniform capsulorhexis may reduce rotational stress on the IOL.
The percentage of eyes with ≤0.50 D or less of residual refractive astigmatism with the manual capsulorhexis is higher in this group than was reported by Lai et al when comparing manual results to a femtosecond laser system.19 More importantly, perhaps, is that the difference they found between the results with the manual and femto procedures was about 10%, similar to the difference observed here between manual and PPC. Both non-manual procedures appear to provide a similar benefit.
The rate of anterior capsular tears seen with the PPC system in the current study appears consistent with that reported by Hooshmand et al for the same device,20 and slightly higher than was observed in a multicenter US clinical trial performed to support FDA approval.21 As noted by one surgeon participant in that trial, there is a learning curve with the PPC device.22 The results reported here were from the first cases performed by the surgeon author (KGG). Prior experience reported in the literature suggests that complications in early cases are primarily related to not ensuring complete capsule contact or a failure to fully retract the push rod used to insert the device, which can interfere with suction.15
There are limitations to the current study. While numbers were relatively high, the retrospective nature of the data collected reduced the level of detail that could be extracted from the clinical records. Uncorrected visual acuity was not available, for instance. Capsulotomy imaging was also not available, either immediately after surgery or at the postoperative visit. The number of eyes in each group, with the low number of associated complications, made it difficult to make any definitive statements regarding relative complication rates. The data collection was also restricted to one site and one surgeon, so corroboration of the findings at other sites would be useful. Finally, retrospective data related to results with a femtosecond laser system were not available, precluding any direct comparisons.
Conclusion
The use of a hand-held device to create the capsulotomy at the time of cataract surgery increased the likelihood of residual refractive astigmatism ≤0.50 D relative to results with a manual technique. Other clinical results (best-corrected visual acuity, spherical equivalent refraction and complication rates) were similar between the two methods.
Funding
This study was supported with an unrestricted research grant from Centricity Vision Inc.
Disclosure
Dr. Gundersen is a consultant to Alcon, Staar, 1stQ and Glaukos. Dr. Potvin is a consultant to Alcon and Carl Zeiss Meditec. The authors report no other conflicts of interest in this work.
References
1. Li S, Hu Y, Guo R, et al. The effects of different shapes of capsulorrhexis on postoperative refractive outcomes and the effective position of the intraocular lens in cataract surgery. BMC Ophthalmol. 2019;19(1):59. doi:10.1186/s12886-019-1068-3
2. Packer M, Teuma EV, Glasser A, Bott S. Defining the ideal femtosecond laser capsulotomy. Br J Ophthalmol. 2015;99(8):1137–1142. doi:10.1136/bjophthalmol-2014-306065
3. Langwińska-Wośko E, Broniek-Kowalik K, Szulborski K. The impact of capsulorhexis diameter, localization and shape on posterior capsule opacification. Med Sci Monit. 2011;17(10):CR577–CR582. doi:10.12659/msm.881984
4. Dooley IJ, O’Brien PD. Subjective difficulty of each stage of phacoemulsification cataract surgery performed by basic surgical trainees. J Cataract Refract Surg. 2006;32(4):604–608. doi:10.1016/j.jcrs.2006.01.045
5. Sharma B, Abell RG, Arora T, Antony T, Vajpayee RB. Techniques of anterior capsulotomy in cataract surgery. Indian J Ophthalmol. 2019;67(4):450–460. doi:10.4103/ijo.IJO_1728_18
6. Chen X, Xiao W, Ye S, Chen W, Liu Y. Efficacy and safety of femtosecond laser-assisted cataract surgery versus conventional phacoemulsification for cataract: a meta-analysis of randomized controlled trials. Sci Rep. 2015;5:13123. doi:10.1038/srep13123
7. Day AC, Gore DM, Bunce C, Evans JR. Laser-assisted cataract surgery versus standard ultrasound phacoemulsification cataract surgery. Cochrane Database Syst Rev. 2016;7(7):CD010735. doi:10.1002/14651858.CD010735.pub2
8. Day AC, Burr JM, Bennett K, et al., FACT group. Femtosecond Laser-Assisted Cataract Surgery Versus Phacoemulsification Cataract Surgery (FACT): a randomized noninferiority trial. Ophthalmology. 2020;127(8):1012–1019. doi:10.1016/j.ophtha.2020.02.028
9. Tognetto D, De Giacinto C, Perrotta AA, et al. Scanning electron microscopy analysis of the anterior capsulotomy edge: a comparative study between femtosecond laser-assisted capsulotomy and manual capsulorhexis. J Ophthalmol. 2018;2018:8620150. doi:10.1155/2018/8620150
10. Zhu Y, Chen X, Chen P, et al. Lens capsule-related complications of femtosecond laser-assisted capsulotomy versus manual capsulorhexis for white cataracts. J Cataract Refract Surg. 2019;45(3):337–342. doi:10.1016/j.jcrs.2018.10.037
11. Chang DF, Mamalis N, Werner L. Precision pulse capsulotomy: preclinical safety and performance of a new capsulotomy technology. Ophthalmology. 2016;123(2):255–264. doi:10.1016/j.ophtha.2015.10.008
12. Thompson V. Streamlined method for anchoring cataract surgery and intraocular lens centration on the patient’s visual axis. J Cataract Refract Surg. 2018;44(5):528–533. doi:10.1016/j.jcrs.2018.02.013
13. Thompson VM, Berdahl JP, Solano JM, Chang DF. Comparison of manual, femtosecond laser, and precision pulse capsulotomy edge tear strength in paired human cadaver eyes. Ophthalmology. 2016;123(2):265–274. doi:10.1016/j.ophtha.2015.10.019
14. Waltz KL, Thompson VM, Quesada G. Precision pulse capsulotomy: initial clinical experience in simple and challenging cataract surgery cases. J Cataract Refract Surg. 2017;43(5):606–614. doi:10.1016/j.jcrs.2017.01.023
15. Ifantides C, Lee J, Rouweyha R, Vital M, Sretavan D. Precision pulse capsulotomy: performance metrics and utility in routine and complex cases. J Cataract Refract Surg. 2020;46(11):1522–1529. doi:10.1097/j.jcrs.0000000000000318
16. Park MJ, Bang CW, Han SY. Precision pulse capsulotomy in challenging cataract surgery cases. Clin Ophthalmol. 2019;13:1361–1368. doi:10.2147/OPTH.S217919
17. Bang SP, Jun JH. Comparison of postoperative axial stability of intraocular lens and capsulotomy parameters between precision pulse capsulotomy and continuous curvilinear capsulotomy: a prospective cohort study. Medicine (Baltimore). 2019;98(48):e18224. doi:10.1097/MD.0000000000018224
18. Hirnschall N, Findl O, Bayer N, et al. Sources of error in toric intraocular lens power calculation. J Refract Surg. 2020;36(10):646–652. doi:10.3928/1081597X-20200729-03
19. Lai KR, Zhang XB, Yu YH, Yao K. Comparative clinical outcomes of Tecnis toric IOL implantation in femtosecond laser-assisted cataract surgery and conventional phacoemulsification surgery. Int J Ophthalmol. 2020;13(1):49–53. doi:10.18240/ijo.2020.01.07
20. Hooshmand J, Abell RG, Allen P, Goemann K, Vote BJ. Intraoperative performance and ultrastructural integrity of human capsulotomies created by the improved precision pulse capsulotomy device. J Cataract Refract Surg. 2018;44(11):1333–1335. doi:10.1016/j.jcrs.2018.07.041
21. U.S. National Institutes of Health Clinical Trials. A prospective multi-center study of anterior lens capsulotomy using the mynosys zepto system. NCT02890303. Available from: https://clinicaltrials.gov/ct2/show/NCT02890303.
22. Thompson VM. MD rate of complete capsulotomies from precision pulse technology. J Cataract Refract Surg. 2018;44(8):1055. doi:10.1016/j.jcrs.2018.07.001
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.