Back to Journals » Clinical Ophthalmology » Volume 16
Clinical Performance of Extended Depth of Focus (EDOF) Intraocular Lenses – A Retrospective Comparative Study of Mini Well Ready and Symfony
Authors Nowik KE, Nowik K, Kanclerz P, Szaflik JP ![]()
Received 6 January 2022
Accepted for publication 14 April 2022
Published 26 May 2022 Volume 2022:16 Pages 1613—1621
DOI https://doi.org/10.2147/OPTH.S341698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Katarzyna Ewa Nowik,1 Kamil Nowik,1 Piotr Kanclerz,2,3 Jacek Paweł Szaflik1
1Department of Ophthalmology, Public Ophthalmic Clinical Hospital (SPKSO), Medical University of Warsaw, Warsaw, Poland; 2Department of Ophthalmology, Hygeia Clinic, Gdańsk, Poland; 3Helsinki Retina Research Group, University of Helsinki, Helsinki, Finland
Correspondence: Katarzyna Ewa Nowik, Tel +48 509 873 680, Email [email protected]
Purpose: Extended depth of focus intraocular (EDOF) IOLs form a bridge between single- and multifocal IOL design. This study aimed to compare clinical outcomes obtained after implanting two different optical designs of EDOF IOLs: the Mini Well Ready (SIFI Medtech, Catania, Italy) and Tecnis Symfony (Abbott Laboratories, Illinois, USA).
Methods: The retrospective observational study included 61 patients (122 eyes) who underwent bilateral implantation of the Mini Well Ready IOL (32 patients) or the Tecnis Symfony IOL (29 patients). The following preoperative and postoperative parameters were evaluated: spherical equivalent, anterior astigmatism, pupil size, monocular and binocular uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA), monocular and binocular uncorrected intermediate visual acuity (UIVA) and distance-corrected intermediate visual acuity (DCIVA), monocular and binocular uncorrected near visual acuity (UNVA) and distance-corrected near visual acuity (DCNVA). In the 6 months postoperative period, defocus curve, contrast sensitivity, photopic phenomena, and posterior capsule opacification were assessed.
Results: The patients receiving the Tecnis Symfony had slightly better monocular and binocular UDVA and CDVA than with the Mini Well Ready IOL, the differences were not statistically significant. Whereas the UIVA, DCIVA, UNVA, DCNVA, UNVA and DCNVA values were higher in the Mini Well Ready group, the differences were not significant. There were no significant between-group differences regarding the defocus curve for the vast majority of tested vergences. Dysphotopsias postoperatively were assessed at 6 months.
Conclusion: Patients receiving both the Mini Well Ready and Symfony IOLs had excellent visual acuity outcomes and spectacle independence.
Keywords: cataract, extended depth of focus, defocus curve, intraocular lens
Introduction
The extended-depth-of-focus (EDOF) intraocular lenses represent a modern lens technology that primarily improves intermediate visual acuity, useful for computer work, while providing good distance and near vision. Hence, EDOF lenses fill a gap between the monofocal and multifocal lenses, giving less unwanted optical phenomena, such as halo or glare, than the latter and offering improved contrast sensitivity.1,2 The EDOF lenses are based on the principle of producing a single focal point with an extended depth that offers clear distance to near vision. The design features a smoother transition between the individual focal lengths, which is achieved by introducing a small degree of optical aberration.3
This study aimed to analyse visual outcomes after bilateral implantation of two EDOF lenses, the Mini Well Ready (SIFI, Catania, Italy) and Tecnis Symfony (Abbott Medical Optics, Abbott Park, NY, USA).
Materials and Methods
Cataract surgery and all pre- and postoperative assessments were performed in the “Laser” Ophthalmology Clinic and the Independent Public University Eye Hospital in Warsaw between January 2017 and February 2020. All surgical procedures were performed by the same experienced surgeon (JPSz). The study was conducted according to the criteria set in the Declaration of Helsinki and all patients provided informed consent. The study protocol was approved by the Medical University of Warsaw Ethics Committee (reference number AKBE/202/2021).
The inclusion and exclusion criteria were identical for both groups. The inclusion criteria for the EDOF IOL implantation included: age of 18 years or older at the time of surgery, bilateral cataract, elective cataract removal by phacoemulsification, preoperative total corneal astigmatism < 0.75D measured by the corneal tomography in both eyes, willingness and ability to attend all postoperative appointments, clear intraocular media other than cataract. The exclusion criteria included: irregular or asymmetrical astigmatism, presence of corneal abnormalities such as keratoconus, keratoglobus, keratolysis, keratomalacia, cornea plana, capsular or zonular abnormalities that may affect postoperative lens centration or tilt (eg, pseudoexfoliation syndrome, chronic uveitis, Marfan’s syndrome), pupillary abnormalities such as non-reactive, tonic pupils that do not dilatate under mesopic or scotopic conditions, abnormally shaped or positioned pupils, pupil size < 3 mm under photopic conditions and > 6 mm under mesopic conditions. Furthermore, individuals with known psychiatric disorders that could confound the outcomes, those dissatisfied with their progressive spectacle correction and those whose mental or physical health may make postoperative neurological adaptation to new visual conditions particularly difficult were excluded. All patients presented no retinal or optic nerve pathologies. Both groups were analysed in reference to their occupation. The results are presented in Table 1. The chi-square test was used to evaluate similarity of the two groups. The Early Treatment of Diabetic Retinopathy Study (ETDRS) charts (Precision Vision, Woodstock, IL) with the visual acuity logMAR scale were used to measure monocular and binocular uncorrected distance visual acuity and corrected distance visual acuity at a distance of 4 m, uncorrected intermediate visual acuity and corrected intermediate visual acuity at a distance of 60 cm, and uncorrected near visual acuity and corrected near visual acuity at a distance of 40 cm. Preoperative biometric measurements were made using an IOL Master® 700 (Carl Zeiss Meditec AG, Jena, Germany). For IOL calculation SRK/T, Barrett Universal II and Hoffer Q formulas were applied. These formulas were used to achieve emmetropic IOL power. Halo and glare were evaluated using the Halo and Glare Simulator which imitated night-driving scene (Eyeland-Design Network GmbH, Vreden, Germany).4 Patient satisfaction levels were determined using the VF-14 questionnaire which the patients were requested to complete during the follow-up visit.5 The measure consists of 14 items relative do activities of daily life, such as reading, writing, completing document forms, preparing meals, physical activity, driving, watching TV. The raw scores are translated into standard scores using a specific formula. The higher the score, the greater patient satisfaction level. The degree of spectacle independence after the EDOF lens implantation was also determined. The questionnaire the patients completed included a question about the need to wear glasses for better distance, near and intermediate vision (computer work). The indicated frequency of using spectacle correction for a given activity of daily life was translated into the percentage score as follows:
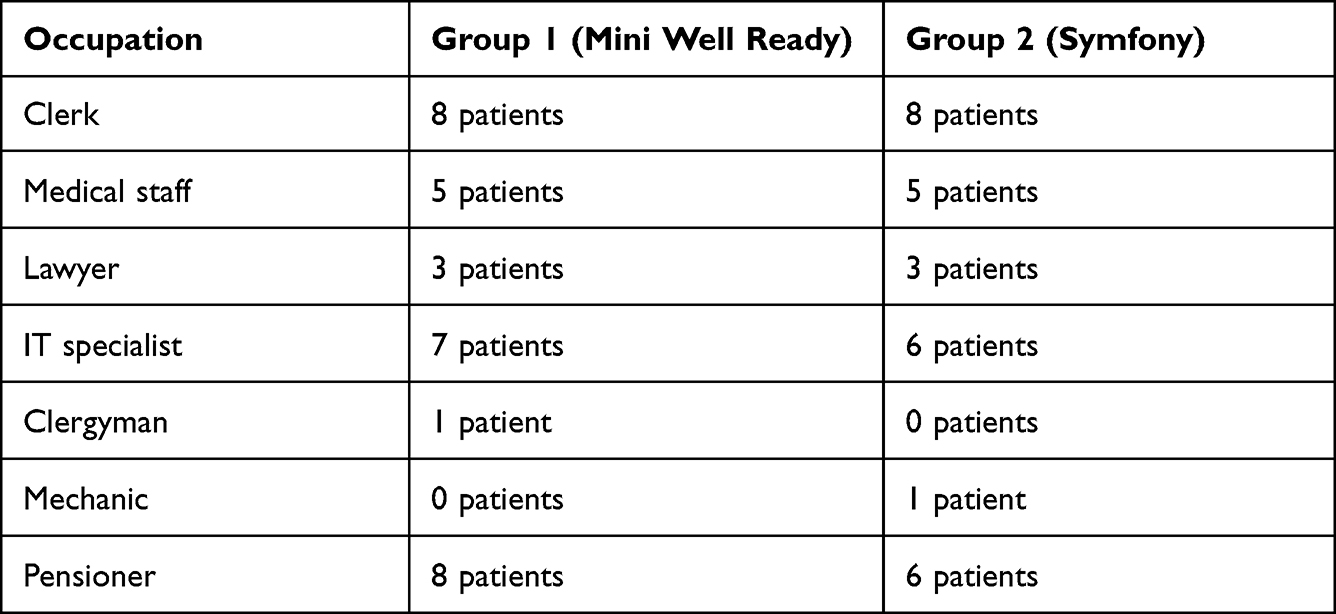 |
Table 1 Patients’ Occupation in Both Groups |
1. always (100%)
2. most of the time (75%)
3. sometimes (50%)
4. rarely (25%)
5. never (0%).
Statistical Analysis
All statistical analyses were carried out using the R software bundle, version 3.6.0. The repeated measures one-way analysis of variance (ANOVA) was used, with Friedman test used as the non-parametric alternative when the distributions differed from normal. The distribution of selected population traits was verified using the Shapiro–Wilk test. The normality of distribution criterion was violated for all variables but K2(D) in both groups. Where the distribution differed from normal, the Mann–Whitney U-test was used whereas the t-test was used for traits that showed normal distribution. There were no significant between-group differences in demographic and occupational parameters, so the baseline group similarity was assumed. The between-group differences in visual outcomes were ascertained in a post hoc analysis using a conservative Bonferroni test or a moderately liberal Tukey’s test, and a Wilcoxon test with Bonferroni correction, for parametric ANOVA and non-parametric Friedman test, respectively. P values smaller than 0.05, were considered significant for all comparisons.
Results
The baseline demographic data of all patients is presented in Table 2. A total of 61 patients (122 eyes), including 39 women and 22 men, divided into 2 groups according to the type of EDOF IOL, were included in the retrospective analysis. Group 1 comprised of 32 patients (64 eyes) after a bilateral implantation of Mini Well Ready lens, while group 2 comprised of 29 patients (58 eyes) after a bilateral implantation of Tecnis Symfony lens.
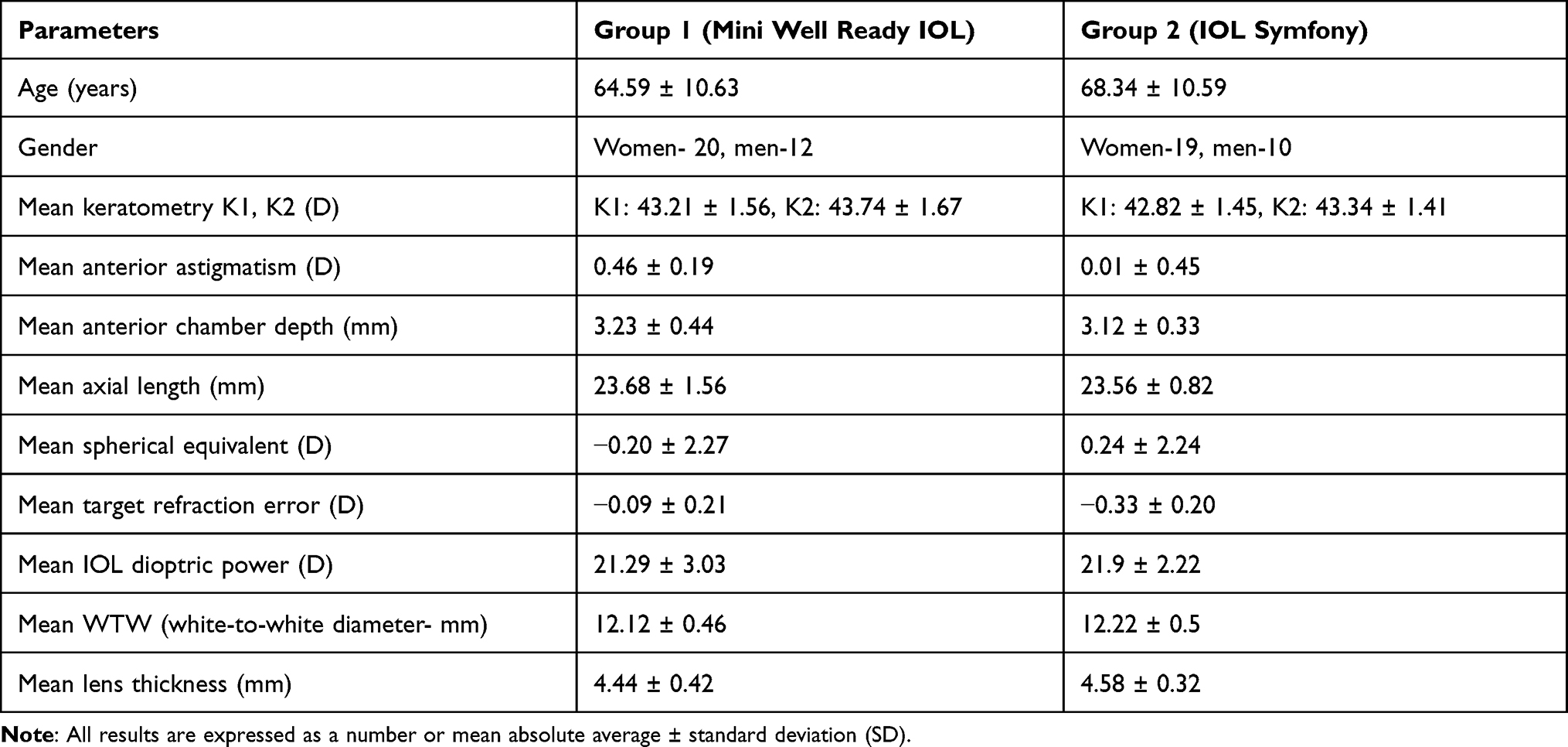 |
Table 2 Demographic Data of Patients Before Surgery |
Visual Outcomes
The visual outcomes were reassessed at 6 months. In both groups, there was a significant UDVA improvement from baseline (0.77±0.48 to 0.065±0.049, P < 0.05 in the Mini Well Ready group vs 0.66±0.34 to 0.01±0.06, P < 0.05 in the Tecnis Symfony group), which did not differ significantly between the groups (P = 0.074). Surgically induced astigmatism was 0.09 Dcyl ± 0.25 Dcyl in the Mini Well Ready group vs 0.07 Dcyl ±0.21 Dcyl in the Tecnis Symfony group.
The postoperative monocular CDVA improved significantly from baseline in both groups (0.43±0.38 to 0.0098±0.029, P < 0.05 in the Mini Well Ready group vs 0.33±0.20 to −0.02±0.07, P < 0.05 in the Tecnis Symfony group) and the improvement was not different between the groups (P = 0.303).
The binocular UDVA and CDVA changed significantly from baseline in both groups (0.60±0.15 and 0.38±0.14 to 0.02±0.04 and −0.01±0.07, P < 0.05 in the Mini Well Ready group vs 0.65±0.16 and 0.39±0.18 to −0.02±0.04 and −0.05±0.05, P < 0.05 in the Tecnis Symfony group). Both between-group differences were non-significant, though (P = 0.089 and P = 0.255 for the binocular UDVA and CDVA, respectively).
The monocular postoperative UIVA and DCIVA were −0.01±0.04 and −0.01±0.04 in the Mini Well Ready group vs 0.03±0.06 and 0.00±0.02 logMAR in the Tecnis Symfony group. Both between-group differences were non-significant, though (P = 0.784 and P = 0.240 for the monocular UIVA and DCIVA, respectively).
The binocular postoperative UIVA and DCIVA were −0.01±0.05 and −0.02±0.05 in the Mini Well Ready group vs 0.01±0.05 and −0.01±0.05 logMAR in the Tecnis Symfony group postoperatively. Both between-group differences were non-significant, though (P = 0.090 and P = 0.240 for the binocular UIVA and DCIVA, respectively).
The monocular postoperative UNVA and DCNVA was 0.00±0.05 and 0.00±0.04 in the Mini Well Ready group, whereas the binocular postoperative UNVA and DCNVA 0.01±0.05 and −0.01±0.05 logMAR. In the Tecnis Symfony group, the monocular postoperative UNVA and DCNVA was 0.11±0.09 and 0.02±0.12 logMAR, whereas the postoperative binocular UNVA and DCNVA was 0.05±0.06, 0.00±0.02 logMAR. Although the patients from the Mini Well Ready group had better near vision, the between-group difference was non-significant (P > 0.05). All visual acuity outcomes are shown in Table 3.
 |
Table 3 Pre- and Post-Operative Visual Acuity Results in Patients with Mini Well and Symfony Implanted Lenses |
All patients in the Mini Well Ready group achieved both monocular and binocular UDVA and CDVA of 0.1 logMAR or better. All patients in the Tecnis Symfony group achieved a monocular UDVA and CDVA of 0.1 logMAR or better, and a binocular UDVA and CDVA improved of 0.1 logMAR. All patients in the Mini Well Ready group achieved both monocular and binocular UIVA and DCIVA of 0.1 logMAR or better. In the Tecnis Symfony group, 88% of patients achieved the monocular UIVA of 0.1 logMAR or better, whereas all patients achieved monocular DCIVA as well as both binocular UIVA and DCIVA of 0.1 logMAR or better. In the Mini Well Ready group, 97% of patients achieved the monocular UNVA of 0.1 logMAR, whereas all patients achieved the monocular DCNVA as well as both binocular UNVA and DCNVA of 0.1 logMAR or better. In the Tecnis Symfony group, 88% of patients achieved the monocular UNVA of 0.1 logMAR or better, whereas 95% of patients achieved the binocular UNVA of 0.1 logMAR. All patients in that group achieved both monocular and binocular DCNVA of 0.1 logMAR or better.
Defocus Curve
The binocular defocus curve data was ascertained by obtaining best-corrected distance (4 m) visual acuity (VA). Visual acuity was measured in logMAR scale, and the optotype was used ETDRS (Precision Vision, Illinois, USA). Using the 0.50 D increments, the defocus curve measured the patients’ binocular VA from −4.00 to +1.50 D with the target luminance set at 85 cd/m2 and the ambient luminance at 21.25 lux.6 The chi-squared test was used for data analysis. As shown in Figure 1, there were no significant differences between the Mini Well Ready and Tecnis Symfony groups at the tested vergences. Subjective DOF was obtained from those vergences (in D) which provided VA values of 0.1 logMAR. The Mini Well Ready group outperformed the Tecnis Symfony group in a plateau curve ranging from −1 D (0.66 m) to −2.5 D (corresponding to 0.4 m), with a mean visual acuity of 0.12 logMAR at −1.5 D or 0.66 m, 0.14 logMAR at −2.0 D or 0.5 m and 0.17 logMAR at −2.5 D or 0.4 m, respectively. In the Tecnis Symfony group, the mean visual acuity was 0.17 logMAR at −1.5 D or 0.66 m (P < 0.001), 0.24 logMAR at −2.0 D or 0.5 m (P < 0.001) and 0.34 logMAR at −2.5 D or 0.4 m (P < 0.001), respectively. Both groups obtained a plateau curve from 0 D (infinite) to −1.5 D (corresponding to 0.66 m). Hence, both groups had a similar intermediate distance vision, in regard to the defocus curve. Subjective DOF measures for 0.1 logMAR criterion did not differ significantly for the following comparisons: Mini Well Ready vs Tecnis Symfony (P = 0.999).
 |
Figure 1 Binocular defocus curve in patients implanted with the Mini Well and Symfony EDOF-IOL. The vertical bars represent the standard deviation of defocus. Abbreviation: CDVA, corrected distance visual acuity. |
Dysphotopsia
In the Mini Well Ready group, 13 patients (40%) reported postoperative halo effect, including 7 patients with the H1 type, 3 patients with the H2 type and 3 patients with the H3 type. Only 1 patient reported postoperative glare (G1). The size and intensity of both phenomena were scored on a scale of 0–100. The mean halo size was 9.5 ± 14.51 with the mean intensity of 7.87 ± 14.11, whereas the mean glare size was 0.06 ± 0.35, with the mean intensity of 0.06 ± 0.35. These results translate into 19 patients (60%) free of halo effect, 31 patients (96.9%) free of glare and the entire group (100%) free of starburst effect. In the Tecnis Symfony group, 19 patients reported postoperative halo effect, including 9 patients with the H1 type, 7 patients with the H2 type and 2 patients with both H1 and H2 types. Furthermore, 7 patients reported glare, including 5 patients with the G1 glare and 2 patients with the G2 glare. The mean halo size was 14.79 ± 16.01, with the mean intensity of 12.92 ± 1.33 whereas the mean glare size was 2.62 ± 5.65, with the mean intensity of 5.65 ± 20.57. These results translate into 11 patients (38%) free of halo effect, 22 patients (76%) free of glare and the entire group (100%) free of starburst effect. Whereas dysphotopsia was more common in the Tecnis Symfony group, the only significant between-group differences were those in mean glare size and intensity (P = 0.013 and P = 0.028, respectively). All patients had no negative dysphotopsia recorded.
Contrast Sensitivity
In the Mini Well Ready group, the monocular contrast sensitivity was 1.67 ± 0.12 logCS and 1.7 ± 0.125 logCS at 1 m and 40 cm, respectively. The binocular contrast sensitivity was 1.85 ± 0.12 logCS and 1.86 ± 0.09 logCS at 1 m and 40 cm, respectively. In the Tecnis Symfony group, the monocular contrast sensitivity was 1.56 ± 0.14 logCS and 1.54 ± 0.15 logCS at 1 m and 40 cm, respectively. The binocular contrast sensitivity was 1.73 ± 0.12 log CS and 1.71 ± 0.13 at 1 m and 40 cm, respectively. Thus, Mini Well Ready outperformed Tecnis Symfony in both monocular and binocular contrast sensitivity at both 1 m and 40 cm. All differences were statistically significant (P = 0.001).
Posterior Capsule Opacification (PCO)
In the Mini Well Ready group, 13 patients (40.6%) had PCO with all cases assessed to be grade 1 after 6 months. In the Tecnis Symfony group, 3 patients (10%) had PCO, also all cases assessed to be grade 1 after 6 months. All patients with PCO were offered and performed a YAG-capsulotomy. Patients in both groups with PCO (Tecnis Symfony group and Mini Well Ready group) had visual acuity examined following a YAG-capsulotomy.
Patient Satisfaction
The postoperative VF-14 questionnaire scores were 92.9 ± 13.8 (range: 72 to 100) and 85.9 ± 17.3 (range: 68 to 98.2) in the Mini Well Ready and Tecnis Symfony groups, respectively. The difference was not statistically significant (P = 0.15).
Discussion
The visual outcomes obtained with bilateral implantation of both (Symfony and Mini Well Ready) EDOF lenses are promising as both groups achieved a significant postoperative improvement of distance, intermediate and near visual acuity. In recent years, several studies evaluating Tecnis Symfony and Mini Well Ready EDOF IOLs in terms of their distance, intermediate and near visual acuity have been published. Their findings are summarised in Supplementary Table 1.7–24
The defocus curves have been used to determine the subjective depth of focus, assess visual outcomes and measure the amplitude of pseudoaccommodation in pseudophakic eyes.23 This concept may apply to patients with EDOF IOLs to some extent, as these remain unaffected by residual accommodation. Hence, we suggest replacing the term “amplitude of pseudoaccommodation” with “defocus (blur) tolerance of the IOL”, which is measured using an additional lens rather than native accommodation.
Despite a slight defocus curve deflection at a myopic defocus, the Tecnis Symfony curve remained steeper nevertheless. A similar trend was observed for the hyperopic defocus, and the observed differences were significant. We adopted the blur tolerance criterion at 0.2 logMAR. In our comparison, the Mini Well Ready EDOF IOLs covered a broader range of subjective depth of focus than the Tecnis Symfony EDOF IOLs and the difference was significant. This stems from the differences in the design and intended use of those IOLs. This implies that despite fairly slight difference in visual outcomes between the studies, the blur tolerance of IOL, if properly assessed and described, will translate into the depth of focus measurements, as shown by different authors.
Although we identified some studies to evaluate the subjective depth of focus of bifocal or trifocal IOLs, there is still insufficient research to investigate subjective the depth of focus in eyes with EDOF IOLs using defocus curves, so the results of those studies cannot be directly compared to ours.13,16 Firstly, we adopted the blur tolerance criterion at 0.2 logMAR, other studies used more subjective criteria. Assessing the subjective depth of focus of AT LISA tri IOLs, Barisic reported the mean depth of focus of 2.59 D, having assumed the blur tolerance criterion of 20/30.25 Buckhurst adopted the blur tolerance criterion at 0.3 logMAR and found the depth of focus of 3 D for multifocal IOLs.26 The depth of focus amplitude in our study is smaller than in other published papers. Other authors indicated an association between the VA threshold values and DOF outcomes, ie, the larger the VA threshold value, the bigger the DOF amplitude.18,27
The information of adverse photic phenomena (dysphotopsias) rates, such as halo, glare or starburst, is crucial for many patients when choosing the most suitable IOL. The majority of published data suggests that dysphotopsias are more common with multifocal IOLs. According to Tchah, 55.8% of patients report halo and glare after multifocal IOL implantation.27 Comparing dysphotopsias in patients after AT LISA tri 839MP and Tecnis Symfony IOL implantation, Lubiński also reported a higher incidence of halo and glare in those with AT LISA tri 839MP IOLs.18 In our study, 38% of patients in the Tecnis Symfony group were halo-free and 76% were glare-free. There was no case of starbursts. Other published in the literature results vary. Hyeck-Soo Son demonstrated that 37% of patients with Tecnis Symfony lenses reported halo and 13% had glare.7 In the study by Rodov, 14% of patients with Tecnis Symfony lenses reported any dysphotopsia whereas in the study by Mencucci, the halo and glare rates were as high as 70% and 30%, respectively.10,28 To our best knowledge no negative dysphotopsia was recorded in other peer reviewed papers investigating EDOF intraocular lenses.
The Mini Well Ready IOLs are thought to cause less dysphotopsia than other multifocal IOL as they do not use diffractive optics.22 This is in line with our findings of better outcomes in the Mini Well Ready group, where 60% of patients were halo-free and 96.9% were glare-free. Again, there were no cases of starbursts in this group, either. The mean halo size was 9.5 ± 14.51 while halo intensity was 7.87 ± 14.11. The mean glare size was 0.06 ± 0.35, and glare intensity was 0.06 ± 0.35. The patients in our study used the Halo & Glare Simulator for assessments. The study by Giers suggests worse results with 54% and 30% of patients with Mini Well Ready IOLs remaining halo- and glare-free, respectively.22 However, 23% of patients reported starburst.22 In the study by Savini, 5% of patients reported halo, 10% reported glare and 27% reported starburst.23 The mean halo size and intensity, as well as glare size and intensity values were significantly higher in that study than in ours (34.8 ± 22.08, 38.50 ± 16.47, 4.40 ± 8.69, and 15.70 ± 26.33, respectively).20 Auffarth found that following Mini Well Ready EDOF IOL implantation, halo was reported by 25% patients (less than in our study), whereas 19% of patients reported glare, more than in our study.19 The mean halo size, halo intensity, glare size and glare intensity were higher than in our study (33.06 ± 14.25, 38.00 ± 10.43, 23.85 ± 10.43 and 42.23 ± 13.22, respectively).19 Furthermore, their patients made it clear that the visual disturbances in question had little to no impact on their daily functioning.19 This corresponds to other studies where halo sizes differed ranging from 35 of 100 to 51 of 100.20,27,30
In our study, both groups achieved close distance high spectacle independence (88% vs 86.2% in the Mini Well Ready and Tecnis Symfony groups, respectively). All patients were intermediate distance spectacle independent. In the literature spectacle independence in the patients with Mini Well Ready IOL implanted is reported to be 78.6%–90%, whereas in the patients with Tecnis Symfony IOL is 28.57%–88.57%.15,18,22,27,29–31 It is assumed that differences in the close distance outcome in the Tan paper is associated with different population parameters (eg, race and height) and different reading distance requirementsfor example, the reading distance is greater in Europe and in the USA (40 cm) than in China (33 cm).27
Although contrast sensitivity measured under photopic conditions monocularly and binocularly at a distance of 40 cm and 1 m in both groups was satisfactory, the Mini Well Ready group achieved better contrast sensitivity and the between-group difference was significant. The finding of high contrast sensitivity is most likely related to a single focal length rather than light dispersion into two or three focal lengths which is the case with multifocal lenses.20 As the test was carried out under photopic conditions, its value may be limited. However, there is no data on mesopic and scotopic contrast sensitivity tests.
Posterior capsule opacity (PCO) was more common in the Mini Well Ready group than in the Tecnis Symfony group (40.6% vs 10%). In the study by Pedrotti, the incidence of PCO was 30% after Mini Well Ready IOL implantation.21 Their follow-up period, however, was shorter than ours (3 months vs 6 months) which may have resulted in a lower PCO incidence. In a study with a follow-up comparable to ours (6 months), Cochener showed the presence of PCO in 4.4% of patients after the Tecnis Symfony IOL implantation.32 Such big difference in PCO could be partially explained by material design of both intraocular lens. The Mini Well Ready intraocular lens is manufactured of hydrophilic acrylic material with hydrophobic surface whereas the Symfony intraocular lens is totally hydrophobic material design. The Zhao et al meta analysis found that hydrophobic lenses had lower rate Nd:YAG laser capsulotomy than hydrophilic treatment (OR = 0.38; P = 0.029).33 Hydrophobic lenses compared with hydrophilic lenses were also associated with better subjective and estimated PCO score (P ≤ 0.015).33 In our study, the Tecnis Symfony group had lower rate of Nd:YAG laser capsulotomy than the Mini Well Ready group (OR = 0.17; P = 0.01). The haptic design might be also a cause of easier migration of lens epithelial cells in this region, which may result in a more frequent PCO occurrence.34,35 However, further studies should be performed to check the impact of haptic design on PCO inhibition. All measurements in our study were taken with no PCO present.
The main limitation of the study is a limited group size; the American Academy of Ophthalmology recommends that for EDOF IOL studies a group should consist of a minimum of 100 patients.6 Nevertheless, this criterion is difficult to fulfill, and the minority of the EDOF studies published in recent years had such a group size.7–24 Secondly, the study was carried out using the artificial, standardized simulator which only resembles real-life conditions of, eg, night driving. Contrast sensitivity was measured only under photopic conditions but not under mesopic and scotopic conditions. The study is, therefore, only an approximation of the real-life conditions.
Conclusion
Both EDOF IOLs are very good solutions for those who strive to remain spectacle-independent. The lens model can be selected considering the patient’s profession, as well as their activity level and preferences. The Mini Well Ready group had better near and intermediate visual acuity than the Tecnis Symfony group, while the latter achieved better distance visual acuity.
Acknowledgments
The authors thank the clinicians, support staff and administrators.
Funding
This work was supported by funding from Independent Public Ophthalmic Hospital in Warsaw.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pacific J Ophthalmol. 2020;9(3):194–202. doi:10.1097/APO.0000000000000296
2. Kohnen T, Suryakumar R. Extended depth-of-focus technology in intraocular lenses. J Cataract Refract Surg. 2020;46(2):298–304. doi:10.1097/j.jcrs.0000000000000109
3. Akella SS, Juthani VV. Extended depth of focus intraocular lenses for presbyopia. Curr Opin Ophthalmol. 2018;29(4):318–322. doi:10.1097/ICU.0000000000000490
4. El Naggar F, Alnassar A, Tarib I, Breyer DR, Gerl M, Kretz FT. Enhancing intermediate vision in different working distances with a novel enhanced depth of focus intraocular lens (EDOF). ECOP. 2018;9(3):94–99.
5. Steinberg EP, Tielsch JM, Schein OD, et al. The VF-14. An index of functional impairment in patients with cataract. Arch Ophthalmol. 1994;112(5):630–638. doi:10.1001/archopht.1994.01090170074026
6. MacRae S, Holladay JT, Glasser A, et al. Special report: American Academy Of Ophthalmology Task Force consensus statement for extended depth of focus intraocular lenses. Ophthalmology. 2017;124(1):139–141. doi:10.1016/j.ophtha.2016.09.039
7. Son HS, Kim SH, Auffarth A, Choi CH. Prospective comparative study of tolerance to refractive errors after implantation of extended depth of focus and monofocal intraocular lenses with identical aspheric platform in Korean population. BMC Ophthalmol. 2019;19(1):19. doi:10.1186/s12886-019-1032-2
8. Kohnen T, Böhm M, Hemkeppler E, et al. Visual performance of an extended depth of focus intraocular lens for treatment selection. Eye. 2019;33(10):1556–1563. doi:10.1038/s41433-019-0443-x
9. Medeiros AL, Saraiva FJ, Iguma CI, et al. Comparison of visual outcomes after bilateral implantation of two intraocular lenses with distinct diffractive optics. Clin Ophthalmol. 2019;13:1657–1663. doi:10.2147/OPTH.S202895
10. Mencucci R, Favuzza E, Caporossi O, Savastano A, Rizzo S. Comparative analysis of visual outcomes, reading skills, contrast sensitivity and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2018;256(10):1913–1922. doi:10.1007/s00417-018-4052-3
11. Łabuz G, Auffarth GU, Özen A, et al. The effect of a spectral filter on visual quality in patients with an extended-depth-of-focus intraocular lens. Am J Ophthalmol. 2019;208:56–63. doi:10.1016/j.ajo.2019.07.001
12. Pedrotti E, Carones F, Aiello F, et al. Comparative analysis of visual outcomes with 4 intraocular lenses: monofocal, multifocal, and extended range of vision. J Cataract Refract Surg. 2018;44(2):156–167. doi:10.1016/j.jcrs.2017.11.011
13. Attia MSA, Auffarth GU, Kretz FTA, et al. Clinical evaluation of an extended depth of focus intraocular lens with the Salzburg reading desk. J Refract Surg. 2017;33(10):664–669. doi:10.3928/1081597X-20170621-08
14. Rementería-Capelo LA, García-Pérez JL, Gros-Otero J, Carillo V, Pérez-Lanzac J, Contreras I. Real-world evaluation of visual results and patient satisfaction for extended range of focus intraocular lenses compared to trifocal lenses. Int Ophthalmol. 2021;41(1):163–172. doi:10.1007/s10792-020-01563-6
15. Xu J, Zheng T, Ly Y. Comparative analysis of visual performance and astigmatism tolerance with monofocal, bifocal, and extended depth-of-focus intraocular lenses targeting slight myopia. J Ophthalmol. 2020;24. doi:10.1155/2020/9283021
16. Paik DW, Park JS, Yang CM, Lim DH, Chung TY. Comparing the visual outcome, visual quality and satisfaction among three types of multifocal intraocular lenses. Sci Rep. 2020;10. doi:10.1038/s41598-020-69318-y
17. Ruiz-Mesa R, Abengózar-Vela A, Ruiz-Santos M. A comparative study of the visual outcomes between a new trifocal and an extended depth of focus intraocular lens. EUR J Ophthalmol. 2018;28(2):182–187. doi:10.5301/ejo.5001029
18. Lubiński W, Podboraczyńka-Jodko K, Kirkiewicz M, Mularczyk M, Post M. Comparison of visual outcomes after implantation of At Lisa tri 839 MP and Symfony intraocular lenses. Int Ophthalmol. 2020;40(10):2553–2562. doi:10.1007/s10792-020-01435-z
19. Auffarth GU, Moraru O, Munteanu M, et al. European, multicenter, prospective, non-comparative clinical evaluation of an extended depth of focus intraocular lens. J Refract Surg. 2020;36(7):426–434. doi:10.3928/1081597X-20200603-01
20. Savini G, Schiano-Lomoriello D, Balducci N, Barboni P. Visual performance of a new extended depth-of-focus intraocular lens compared to a distance-dominant diffractive multifocal intraocular lens. J Refract Surg. 2018;34(4):228–235. doi:10.3928/1081597X-20180125-01
21. Pedrotti E, Chierego CH, Talli PM, et al. Extended depth of focus versus monofocal IOLs: objective and subjective visual outcomes. J Refract Surg. 2020;36(4):214–222. doi:10.3928/1081597X-20200212-01
22. Giers BU, Khoramnia R, Varadi D, et al. Functional results and photic phenomena with new extended-depth-of-focus intraocular lens. BMC Ophthalmol. 2019;19(1):197. doi:10.1186/s12886-019-1201-3
23. Savini G, Balducci N, Carbonara C, et al. Functional assessment of a new extended depth-of-focus intraocular lens. Eye. 2019;33(3):404–410. doi:10.1038/s41433-018-0221-1
24. Escandón-García S, Ribeiro FJ, McAlinden C, Queirós A, González-Méijome JM. Through-focus vision performance and light disturbances of 3 new intraocular lenses for presbyopia correction. J Ophthalmol. 2018;2018:1–8. doi:10.1155/2018/6165493
25. Barisic A, Patel S, Gabric N, Feinbaum CG. The clinical depth of field achievable with trifocal and monofocal intraocular lenses: theoretical considerations and proof of concept clinical results. Graefes Arch Clin Exp Ophthalmol. 2017;255(2):367–373. doi:10.1007/s00417-016-3566-9
26. Buckhurst PJ, Wolffsohn JS, Naroo SA, et al. Multifocal intraocular lens differentiation using defocus curves. Invest Ophthalmol Vis Sci. 2012;53(7):3920–3926. doi:10.1167/iovs.11-9234
27. Tan J, Qin Y, Wang CH, Yuan S, Ye J. Visual quality and performance following bilateral implantation of TECNIS Symfony intraocular lenses with or without micro-monovision. Clin Ophthalmol. 2019;Volume 13(13):1071–1077. doi:10.2147/OPTH.S202380
28. Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg. 2019;35(7):434–440. doi:10.3928/1081597X-20190618-01
29. Tchah H, Nam K, Yoo A. Predictive factors for photic phenomena after refractive, rotationally asymmetric, multifocal intraocular lens implantation. Int J Ophthalmol. 2017;10(2):241–245. doi:10.18240/ijo.2017.02.10
30. Chang DH, Janakiraman DP, Smith PJ, et al. Visual outcomes and safety of the Tecnis Symfony intraocular lens: results of a pivotal clinical trial. J Cataract Refract Surg. 2022;48(3):288–297. doi:10.1097/j.jcrs.0000000000000747
31. Sevik MU, Turhan SA, Toker E. Clinical outcomes with a low add multifocal and an extended depth of focus intraocular lenses both implanted with mini-monovision. Eye. 2021. doi:10.1038/s41433-021-01600-3
32. Cochener B; Concerto Study Group. Clinical outcomes of a new extended range of vision intraocular lens: International Multicenter Concerto Study. J Cataract Refract Surg. 2016;42(9):1268–1275. doi:10.1016/j.jcrs.2016.06.033
33. Zhao Y, Yang K, Li J, Huang Y, Zhu S. Comparison of hydrophobic and hydrophilic intraocular lens in preventing posterior capsule opacification after cataract surgery: an updated meta-analysis. Medicine. 2017;96(44):e8301. doi:10.1097/MD.0000000000008301
34. Ursell PG, Dhariwal M, Majirska K, et al. Three-year incidence of Nd: YAGcapsulotomy and posterior capsule opacification and its relationship to monofocal acrylic IOL biomaterial: a UK Real World Evidence study. Eye. 2018;32(10):1579–1589. doi:10.1038/s41433-018-0131-2
35. Mylonas G, Prskavec M, Baradaran-Dilmaghani R, Karnik N, Buehl W, Wirtitsch M. Effect of a single-piece and a three-piece acrylic sharp-edged IOL on posterior capsule opacification. Curr Eye Res. 2013;38(1):86–90. doi:10.3109/02713683.2012.717242
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.