Back to Journals » Clinical Ophthalmology » Volume 8
Clinical performance of a new aspheric dual-optic accommodating intraocular lens
Authors Marques EF, Castanheira-Dinis A
Received 17 August 2014
Accepted for publication 3 September 2014
Published 19 November 2014 Volume 2014:8 Pages 2289—2295
DOI https://doi.org/10.2147/OPTH.S72804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eduardo F Marques,1 António Castanheira-Dinis2
1Department of Ophthalmology, Hospital da Cruz Vermelha, Lisboa, Portugal; 2Visual Sciences Research Centre, Universidade de Lisboa, Portugal
Purpose: To describe the clinical performance of a new dual-optic intraocular lens (IOL) with an enhanced optic profile designed to mimic natural accommodation.
Patients and methods: Prospective multicenter clinical study with the new dual-optic aspheric accommodating IOL (Synchrony Vu) in 74 patients (148 eyes) undergoing cataract surgery. Refractive target was emmetropia. Examinations at 1 month and 6 months included subjective refractions; visual acuities at near, intermediate, and far; mesopic contrast sensitivity with and without glare; safety data; and subjective survey on dysphotopsia (halos and glare).
Results: Clinical data at 6 months showed 89% of the eyes within ±1.0 D spherical equivalent refraction. Mean binocular uncorrected and distance-corrected visual acuity was 20/20 at far (0.00±0.11 logMAR and -0.06±0.08 logMAR, respectively), 20/20 at intermediate (0.01±0.13 logMAR and -0.01±0.10 logMAR, respectively), and 20/25 at near (0.10±0.14 logMAR and 0.14±0.15 logMAR, respectively). Mesopic contrast sensitivity was within normal limits. Seventy-eight percent of the patients had no spectacles and 70% had no dysphotopsia. One eye had IOL repositioning within 1 month of surgery.
Conclusion: The new aspheric Synchrony Vu accommodating IOL provided good visual performance at a range of distances without affecting quality of vision and with minimal safety considerations.
Keywords: accommodating IOL, cataract surgery, intraocular lens, presbyopia
Introduction
Accommodating intraocular lenses (IOLs) are dynamic devices that need to optimally interact with the capsular bag and ciliary muscle to effect a change in optical power during near viewing.1,2 The equilibrium between the IOL and the intraocular accommodative plant (capsular bag, zonular fibers, and ciliary muscle) may ultimately impact performance of the accommodating IOL. In addition, the dynamic nature of accommodating IOLs may also impact refractive outcomes, depending on the baseline state of the IOL in the eye.
The dual-optic Synchrony accommodating IOL (Abbott Medical Optics Inc., Santa Ana, CA, USA) was specifically designed to fill the entire capsular bag and benefit from the accommodative capacity of the lens capsule during near vision.3,4 The three-dimensional, single-piece, foldable silicone lens has a high plus-powered moving optic attached to a variable minus-powered optic through spring haptics. A preloaded injector facilitates implantation through a small incision. The IOL is designed to provide a single, clear focus over a wide range of viewing distances through active accommodation. When implanted within the capsular bag, the capsular tension exerts a compressive force and decreases the interoptic separation of the IOL to a minimum. This compressed state is the emmetropic state of the IOL. With accommodative action, the zonules relax, releasing the tension on the capsular bag, which results in a forward displacement of the anterior optic. Design and clinical performance of the parent dual-optic accommodating IOL (Synchrony) have been discussed in detail in previous publications, including improved near vision, reading ability, and long-term performance.4–7
A next generation, aspheric version of the dual-optic IOL (Synchrony Vu; Abbott Medical Optics Inc.) was developed to further mimic the optical changes in the eye during natural accommodation. During natural accommodation, the optical power of the crystalline lens increases along with an increase in negative spherical aberration.8,9 The central region of the natural lens exhibits greater change in optical power compared to more peripheral regions.8,9 The new generation dual-optic IOL is designed to mimic the spatially variant characteristics of natural accommodation and to further improve the near benefit provided by the dual-optic IOL. It incorporates a blended aspheric design with a central zone of negative spherical aberration smoothly transitioning into a spherical periphery. The purpose of this design is to achieve a selective increase in negative spherical aberration during near viewing associated with pupil constriction, while maintaining good optical quality during mesopic conditions with larger pupil diameter.
The objective of the current multicenter clinical study is to evaluate outcomes following primary implantation of this new aspheric dual-optic accommodating IOL for the visual correction of patients undergoing cataract extraction.
Materials and methods
Clinical study design
A multicenter prospective study that included four sites and five investigators was undertaken. Prior approval by each institutional ethical committee was obtained, and all patients provided informed consent after an explanation of the nature of the study, including potential risks and benefits. The study was conducted in compliance with the Declaration of Helsinki. A total of 148 eyes of 74 patients binocularly implanted with the Synchrony Vu IOL were followed up for a period of 6 months. The study was a feasibility study to evaluate the safety and visual performance of this new dual-optic accommodating IOL in a consecutive series of patients.
The IOL
Synchrony Vu (model SYNC-200) is a single-piece silicone IOL intended for use following cataract extraction. It comprises a dual-optic system arranged coaxially along the optical axis. The front optic diameter is 5.5 mm and the back optic diameter is 6 mm. The clear optic zone for both optics is 5 mm diameter. They are supported by 9.5 mm long haptic structures extending along opposite directions. Two posterior stabilizers extend laterally from the rear lens and are perpendicular to the direction of the haptic extension, with an overall length of 9.8 mm. In addition, the IOL has a small central aspheric zone (<2.5 mm diameter) in the center of the anterior lens. It is available in powers of 16–28 D.
Inclusion and exclusion criteria
The inclusion criteria were age of at least 40 years at the time of surgery, bilateral age-related cataracts, preoperative corneal astigmatism of 1.5 diopters (D) or less, and requiring Synchrony Vu implantation within the available IOL powers. Preoperative exclusion criteria included history of prior ocular surgery or ocular pathology. Surgical exclusions included traumatic surgery; inability to achieve in-the-bag placement of the dual-optic IOL; irregular, decentered, or large (>5 mm diameter) continuous curvilinear capsulorhexis (CCC); and anterior or posterior capsule tear.
Surgical technique
Surgery was performed by five experienced surgeons in four sites using a standardized protocol. Phacoemulsification was performed in all eyes through a 5 mm (or smaller) CCC to achieve complete overlap of the anterior optic of the lens. The use of a corneal marker (Fujimoto CCC guide) was required to achieve a small anterior CCC sized under 5 mm diameter. IOL implantation was achieved with a preloaded injector designed to deliver the lens into the capsular bag through a 3.8 mm clear corneal incision. Surgeons performed meticulous anterior and posterior capsular bag cleanup to remove epithelial cells in an effort to retard capsular fibrosis. Standard postcataract surgery medications (0.5% moxifloxacin, 1% prednisolone acetate, and 0.5% ketorolac) were used.
Preoperative evaluation
All patients underwent standard preoperative assessments, including subjective refraction, intraocular pressure, and anterior and posterior segment evaluations. Preoperative biometry measurements, including keratometry, axial length, and anterior chamber depth measured with the IOLMaster 500 (Carl Zeiss Meditec AG, Jena, Germany), were used to calculate the IOL power using a proprietary formula. The target refraction was always emmetropia.
Postoperative evaluation
Postoperative examinations were performed at 1-day, 1-week, 1-month, and 6-month time points after surgery. The 1-month and 6-month visits included measurements of uncorrected (U) visual acuity (VA) at 4 m (distance; UDVA), at 80 cm (intermediate; UIVA), and at 40 cm (near; UNVA) as well as manifest refraction, distance-corrected VA at distance (CDVA), intermediate (DCIVA), and near (DCNVA). Monocular VAs were obtained at all visits, and binocular VAs were obtained at 6 months. Patients requiring refractive correction were prescribed glasses 6–8 weeks after the second eye surgery. The Early Treatment Diabetic Retinopathy Study (ETDRS) charts under photopic light levels were used for VA measurements.
Subjective questionnaires evaluated spectacle use (options included never, near only, far only, both far and near), frequency of spectacle wear (never, occasionally, most of the time, always) separately for near, intermediate, and far distances, and symptoms of glare, halo, and double vision on a 5-point scale. Additionally, the ease of performing activities (such as reading a magazine, reading a book, reading medicine labels, playing cards, using computer, using cell phone, and driving car) was evaluated on a 7-point scale, which included an option of not applicable if the task was not commonly performed by the patient. The questionnaires were administered at the 6-month time point.
In a subset of 40 patients (80 eyes) in three sites, monocular contrast sensitivity was measured with the OPTEC® 6500 with the functional acuity contrast test (FACT) charts (Stereo Optical Co., Inc., Chicago, IL, USA) at 6 months after surgery. Two conditions, with and without a glare source, were tested under mesopic light levels (3 cd/m2).
Statistical analysis
Statistical analyses were performed using Minitab (Minitab version 16; PA, USA). Descriptive statistics as means, standard deviation (SD), and confidence intervals were calculated for continuous variables, and percentages were calculated for categorical variables. Normality of the data was confirmed using the Kolmogorov–Smirnov test.
Results
Demographics
The mean ± SD of patient age was 65.6±9.2 years; 38% were males and 62% females. Monocular data from 148 eyes were available at 1 month and 6 months; binocular data from 74 patients were available at 6 months.
Refraction and visual acuities
On average, manifest spherical equivalent refraction was slightly myopic at -0.60 D at 1 month and improved to within ±0.50 D of the refractive target at the 6-month time point (two-tailed t-tests, P<0.01; Table 1). The percentage of eyes with spherical equivalent refraction within 0.50 D of emmetropia was 64% at the 6-month time point; the refraction within 1.0 D was 89%.
 | Table 1 Refraction and monocular and binocular visual acuities |
Monocular UDVA improved progressively from the early postoperative period (20/40 at the 1-week time point; data not shown) to a later time (20/25 at 6 months), most likely due to a reduction in some degree of myopia through the early postoperative period.
Monocular CDVA of 20/25 or better was achieved in all eyes. DCIVAs and DCNVAs can be considered a measure of the accommodative or depth of focus performance of the lens. Average monocular DCIVA of 20/25 and DCNVA of 20/40 were achieved by the 1-month time point and remained stable thereafter up to 6 months.
Binocular UVA (Figure 1A) at 6 months was on average 20/20 for far and intermediate distances and 20/25 at near. DCNVA (Figure 1B) showed a two-line improvement in binocular viewing compared to monocular at 6 months.
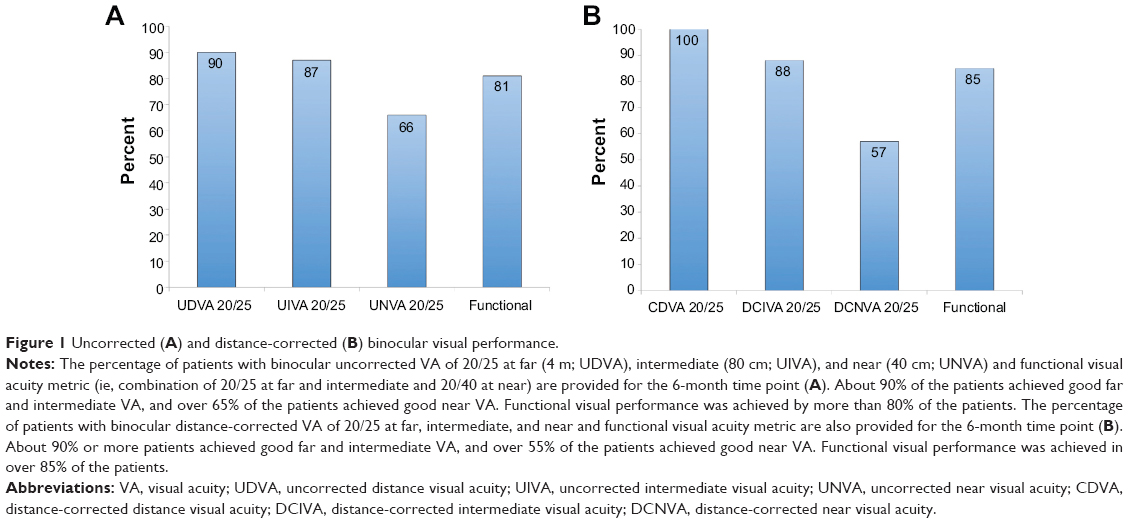 | Figure 1 Uncorrected (A) and distance-corrected (B) binocular visual performance. |
Subjective survey questionnaire
At 6 months, a majority of the patients (78%) reported not wearing spectacles, followed by 13% for near only, 6% for both near and far, and 3% for far only (Figure 2A). On the question of frequency of spectacle wear for different distances, 94% reported never wearing glasses for distance, 95% never for intermediate, and 85% never for near (Figure 2B).
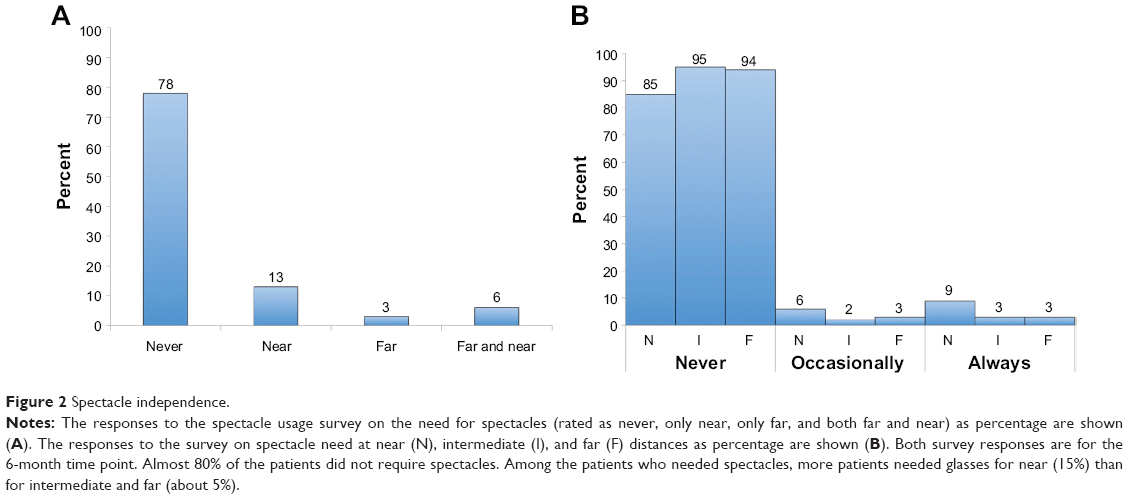 | Figure 2 Spectacle independence. |
The ability to perform various activities was evaluated on a 7-point scale from 0–6 (0= easy and 6= difficult), and is shown as the mean ± SD of the ratings in Figure 3. With closer distance or small target size, the mean ratings tended to increase.
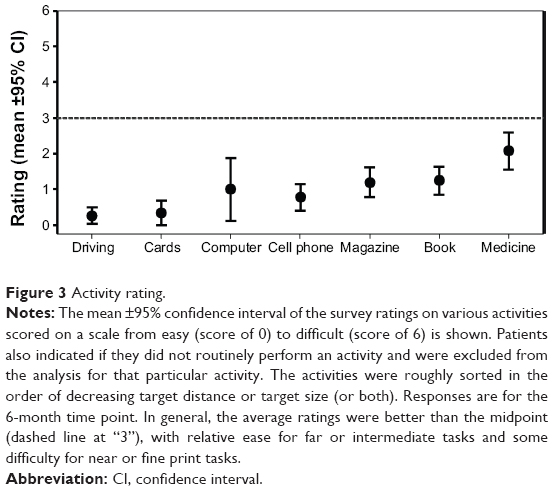 | Figure 3 Activity rating. |
A majority of the patients (69%) reported experiencing none-to-mild symptoms of glare, halo, or double vision. Some patients experienced glare (21% moderate and 10% severe) and halos (18% moderate and 4% severe), while 3% experienced symptoms of double vision (Figure 4).
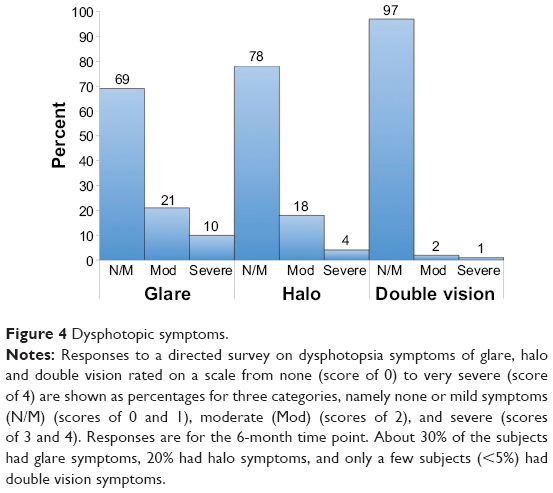 | Figure 4 Dysphotopic symptoms. |
Contrast sensitivity
Mesopic contrast sensitivity of Synchrony Vu patients tested both without or with glare (Figure 5), was within the normal limits of the 40–49 years age cohort measured by Hohberger et al10 using the same instrument.
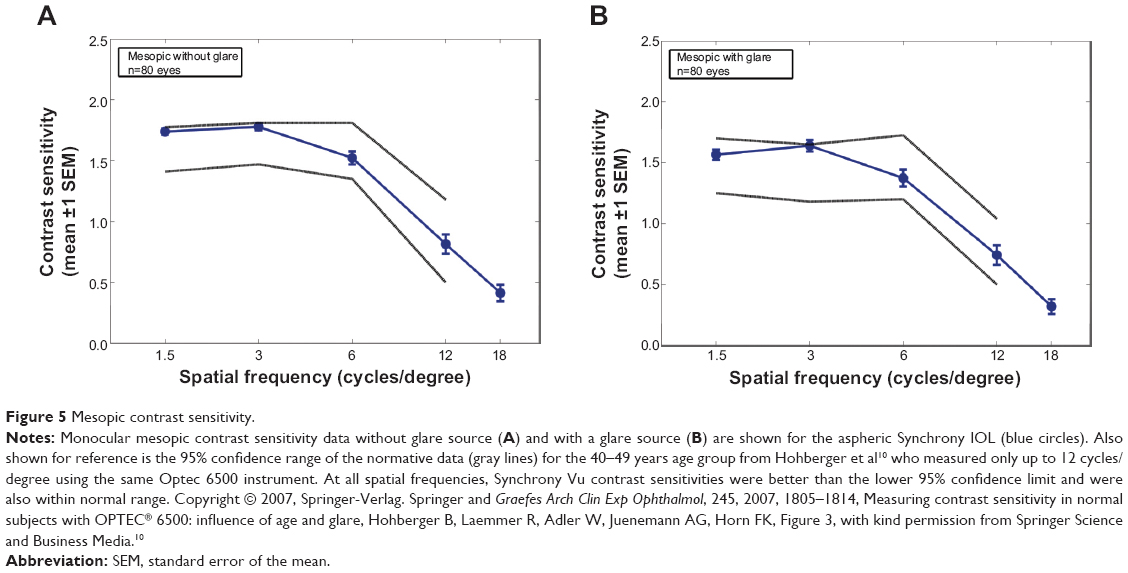 | Figure 5 Mesopic contrast sensitivity. |
Safety
None of the study eyes underwent Nd-YAG capsulotomy in the first 6 months after cataract surgery.
IOL optic decentration was noted in three eyes from one site. The UDVA for all the three eyes was 20/20; however, the patients did complain of glare symptoms. All three eyes were monitored throughout the duration of the study without any surgical intervention.
In one eye, the IOL was repositioned within 1 month of surgery due to a partial anterior prolapse of the anterior optic from the capsular bag. The IOL was stable in the bag following repositioning, and at the 6-month visit the patient had a UDVA of 20/32 and CDVA of 20/20.
Discussion
To evaluate the safety and effectiveness of the new Synchrony Vu aspheric IOL, a multicenter clinical trial was undertaken. The clinical trial was primarily a feasibility study to evaluate the performance of this new IOL. The lack of a control group can be considered a drawback of the study design, and future studies may be performed with adequate control groups, although the study is strengthened with the use of standardized testing procedures across multiple sites. It was found that following an initial period of myopia, average refractive error close to emmetropia was achieved by the 6-month time point. UDVA largely stabilized by 1 month. It should be noted that all patients were targeted for emmetropia and no intentional monovision was attempted. The initial myopia may be explained by the dual-optics of the Synchrony Vu IOL, designed to allow forward movements of the front optic. The IOL relies on capsular bag forces to maintain the two optics in a compressed state, with a 0.5 mm separation between the optics for emmetropia. Any forward movement of the front optic will lead to accommodation or, in other words, myopic refractive error. It is likely that in the initial postoperative period, the two optics were separated by greater than 0.5 mm and gradually compressed as the capsular bag underwent postoperative changes and adapted to the IOL. In general, patients achieved good UDVAs both monocularly (20/25) and binocularly (20/20) by 6 months.
IVAs were similar to distance vision (ie, 20/25 monocularly and 20/20 binocularly) with or without distance refractive correction. Similarly, near vision was, on average, 20/40 monocularly and 20/25 binocularly with or without distance refractive correction. It is important to note that distance refractive correction did not reduce intermediate and near visual performance, as might be expected with any monovision strategy.
As a measure of functional performance, it was observed that 80%–90% of the patients achieved a combination of 20/25 VA at distance and intermediate and 20/40 VA at near (Figure 1). If one considers typical newspaper print to be about 20/50,11 then these patients can be considered spectacle-free for most day-to-day visual tasks. This is supported by survey data showing 78% of patients not requiring spectacles (Figure 2). When evaluating ease of performing various tasks, in general the tasks were rated to be easy to moderate, including reading a medicine bottle label (Figure 3).
The safety profile of a dual-optic IOL may be expected to be different from a single-optic IOL. It is possible that a dual-optic IOL could experience greater tilt or decentration than a single-optic IOL. The haptic design of an accommodating IOL should be capable of allowing dynamic movements of the IOL as opposed to a single-optic IOL designed for good stability within the capsular bag. Three eyes in the current study were noted to have IOL decentration, with subjective glare symptoms, even though 20/20 VA was achieved in each case. Directed survey on glare, halo, and double vision indicated generally few symptoms. About 30% of the patients experienced some degree of glare, and 20% experienced some degree of halo (Figure 4), which is currently better than that reported for multifocal IOLs (up to 70%).12,13
As further evidence of good imaging quality, mesopic contrast sensitivity with or without glare (Figure 5) was within normal limits.10,14
The current clinical study did not include objective accommodation testing because it was designed as a feasibility study with clinically viable test methods. Future studies with Synchrony Vu IOL should consider further optical characterization, objective accommodation testing, and an appropriate control group.
Current options to correct presbyopia during cataract surgery include monovision, multifocal IOLs, and accommodating IOLs. Compared to monovision, multifocal and accommodating IOLs have the potential to maintain binocular function at all distances. The main limitations of multifocal IOLs are the high incidence of dysphotopic phenomena such as glare and halos,15,16 and the loss of contrast inherent to a design that causes loss of incident light to higher orders of aberration.17 Single-optic accommodating IOLs have in common somewhat limited amplitude of accommodation,18 and often provide inadequate or inconsistent near vision. Quality of vision has also been a challenge with single-optic accommodating lenses.19 These difficulties led to the development of the dual-optic accommodating IOL in an attempt to provide adequate levels of spectacle independence while maintaining good image quality. The current study showed that overall good visual outcomes can be expected with the Synchrony Vu IOL at intermediate and near distances with or without distance refractive correction.
In conclusion, an aspheric version of the dual-optic accommodating IOL (Synchrony Vu) was evaluated in a multicenter clinical trial to show good functional visual performance at a range of distances with minimal visual side effects. The safety profile of an accommodating IOL, especially a dual-optic IOL, is expected to be different from a nonaccommodating single-optic IOL and should be considered together with the benefit.
Acknowledgments
The authors thank Ricardo Alarcon, MD, and Victor Bohorquez, MD (Department of Ophthalmology, ServiOftalmos, Bogota, Colombia); Ivan Ossma, MD (Fundación Valle de Lili, Cali, Colombia); Cristina Peris-Martinez, MD, PhD (Fundación Oftalmológica del Mediterráneo, Valencia, Spain) for help in data collection. Sanjeev Kasthurirangan, PhD (Abbott Medical Optics Inc., Santa Ana, CA, USA) for help with data analysis and for writing assistance.
Disclosure
Eduardo F Marques was consultant and clinical investigator for Abbott Medical Optics during the study. The study was sponsored by Abbott Medical Optics Inc., Santa Ana, CA, USA. The authors report no other conflicts of interest in this work.
References
Charman W. Restoring accommodation: a dream or an approaching reality? Ophthalmic Physiol Opt. 2005;25:1–6. | ||
Menapace R, Findl O, Kriechbaum K, Leydolt-Koeppl Ch. Accommodating intraocular lenses: a critical review of present and future concepts. Graefes Arch Clin Exp Ophthalmol. 2007;245:473–489. | ||
McLeod SD. Optical principles, biomechanics, and initial clinical performance of a dual-optic accommodating intraocular lens (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2006;104:437–452. | ||
McLeod S, Vargas L, Portney V, Ting A. Synchrony dual-optic accommodating intraocular lens, Part 1: optical and biomechanical principles and design considerations. J Cataract Refract Surg. 2007;33:37–46. | ||
Ossma I, Galvis A, Vargas L, Trager MJ, Vagefi MR, McLeod SD. Synchrony dual-optic accommodating intraocular lens, Part 2: pilot clinical evaluation. J Cataract Refract Surg. 2007;33:47–52. | ||
McLeod S, Portney V, Ting A. A dual optic accommodating foldable intraocular lens. Br J Ophthalmol. 2003;87:1083–1085. | ||
Bohórquez V, Alarcon R. Long-term reading performance in patients with bilateral dual-optic accommodating IOL. J Cataract Refract Surg. 2010;36:1880–1886. | ||
Vilupuru A, Roorda A, Glasser A. Spatially variant changes in lens power during ocular accommodation in a rhesus monkey eye. J Vis. 2004;4:299–309. | ||
Cheng H, Barnett JK, Vilupuru AS, et al. A population study on changes in wave aberrations with accommodation. J Vis. 2004;4:272–280. | ||
Hohberger B, Laemmer R, Adler W, Juenemann AG, Horn FK. Measuring contrast sensitivity in normal subjects with OPTEC® 6500: influence of age and glare. Graefes Arch Clin Exp Ophthalmol. 2007;245:1805–1814. | ||
Oduntan AO. An analysis of print sizes of South African newspapers in relation to prescription of reading devices for low vision patients. S Afr Optom. 2005;64(2):64–70. | ||
Summary of Safety and Effectiveness Data Report AcrySof® ReSTOR® Apodized Diffractive Optic, 2005. Available at http://www.fda.gov/ohrms/dockets/dockets/05m0117/05m-0117-aav0001-03-SSED-vol1.pdf. Accessed 18 September 2014. | ||
Summary of Safety and Effectiveness Data Report No. Tecnis® Multifocal Posterior Chamber Intraocular Lens, 2009. Available at http://www.accessdata.fda.gov/cdrh_docs/pdf8/P080010b.pdf. Accessed18 September 2014. | ||
Pomerance G, Evans D. Test-retest reliability of the CSV-1000 contrast test and its relationship to glaucoma therapy. Invest Ophthalmol Vis Sci. 1994;35:3357–3361. | ||
Summary of Safety and Effectiveness Data Report No. AcrySof® ReSTOR® Apodized Diffractive Optic, 2005. | ||
Summary of Safety and Effectiveness Data Report No. Tecnis® Multifocal Posterior Chamber Intraocular Lens, 2009. | ||
Pieh S, Marvan P, Lackner B, et al. Quantitative performance of bifocal and multifocal intraocular lenses in a model eye: point spread function in multifocal intraocular lenses. Arch Ophthalmol. 2002;120:23–38. | ||
Kuchle M, Nguyen NX, Langenbucher A, et al. Implantation of a new accommodating posterior chamber intraocular lens. J Refract Surg. 2002;18:208–216. | ||
Alió JL, Plaza-Puche AB, Montalban R. Near visual outcomes with single-optic and dual-optic accommodating intraocular lenses. J Cataract Refract Surg. 2012;38:1568–1575. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.