Back to Journals » Drug Design, Development and Therapy » Volume 20
Clinical Impact of MeltDose Technology Extended-Release Tacrolimus (LCPT) in Solid Organ Transplantation: A Systematic Review
Authors Almalki BA ![]()
Received 30 March 2026
Accepted for publication 19 June 2026
Published 25 June 2026 Volume 2026:20 613201
DOI https://doi.org/10.2147/DDDT.S613201
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Bassem A Almalki
Department of Pharmacy Practice, College of Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Bassem A Almalki, Email [email protected]
Abstract: Tacrolimus is a narrow-therapeutic-index immunosuppressant whose clinical performance is XR®Envarsus XR®), an extended-release tacrolimus formulation, was developed to enhance dissolution, improve bioavailability, and reduce pharmacokinetic variability. This systematic review evaluated the clinical and translational impact of LCPT compared with immediate-release tacrolimus (IR-Tac) across solid-organ transplantation. A systematic search of PubMed/MEDLINE and Google Scholar was conducted from database inception through October 2025. Owing to heterogeneity in study populations, designs, and outcome reporting, a quantitative meta-analysis was not performed, and findings were synthesized qualitatively. Of 351 identified records, 326 underwent screening, and six studies met inclusion criteria. The primary outcome was biopsy-proven acute rejection (BPAR); secondary outcomes included graft survival, mortality, renal function, metabolic complications, adverse events, and tacrolimus trough concentrations. Across studies, LCPT demonstrated clinical efficacy comparable to IR-Tac. In de novo kidney transplantation, BPAR rates were similar (13.1% vs 13.5%), with comparable graft survival and mortality. In heart transplantation, LCPT maintained noninferior outcomes (BPAR 15% vs 10%). In conversion settings, rejection rates remained comparable. LCPT consistently achieved therapeutic trough concentrations with approximately 20– 30% lower total daily doses, reflecting enhanced bioavailability attributable to MeltDose technology. These findings support LCPT as a formulation-driven optimization of tacrolimus delivery. While pharmacokinetic advantages are evident, their translation into superior long-term clinical outcomes remains to be fully established.
Keywords: LCP-tacrolimus, MeltDose tacrolimus, extended-release tacrolimus, immediate-release tacrolimus, solid organ transplantation, immunosuppression
Introduction
Tacrolimus, a calcineurin inhibitor, remains the foundation of maintenance immunosuppression following solid-organ transplantation.1 Classified as a narrow-therapeutic-index drug, tacrolimus requires precise control of systemic exposure to balance immunosuppressive efficacy against dose-dependent toxicity.1,2 However, the compound exhibits low aqueous solubility and dissolution-limited absorption, properties that contribute to substantial inter- and intra-patient variability in oral bioavailability.2,3 These physicochemical characteristics render tacrolimus highly sensitive to formulation-dependent pharmacokinetics, wherein differences in dissolution behavior and absorption kinetics may produce clinically meaningful variations in drug exposure.3
The immediate-release formulation of tacrolimus (IR-Tac) is characterized by rapid but inconsistent gastrointestinal absorption. This variability is influenced by luminal solubility, intestinal motility, and extensive first-pass metabolism mediated by cytochrome P450 3A (CYP3A) enzymes and P-glycoprotein efflux transporters.2,3 The resultant fluctuations in systemic exposure have well-documented clinical consequences: periods of subtherapeutic concentration increase the risk of acute allograft rejection, whereas supratherapeutic peaks are associated with nephrotoxicity, neurotoxicity, and metabolic sequelae, including new-onset diabetes after transplantation.1,3 These observations suggest that the therapeutic limitations of tacrolimus are attributable, at least in part, to suboptimal drug delivery rather than insufficient pharmacologic activity.
To mitigate these limitations, extended-release tacrolimus formulations have been developed with the objective of modifying the absorption phase and reducing exposure variability. Importantly, extended-release formulations are not pharmacokinetically interchangeable; their performance is determined by the specific drug-delivery technology employed.4 LCP-tacrolimus (LCPT; Envarsus XR®) is an extended-release tacrolimus formulation developed using MeltDose technology, a solid-dispersion platform designed to enhance dissolution of poorly water-soluble compounds.4 This approach reduces drug particle size to a near-molecular dispersion, thereby increasing the effective surface area available for dissolution and facilitating absorption across an extended region of the gastrointestinal tract.4
The pharmacokinetic profile of LCPT differs meaningfully from that of IR-Tac. Published data indicate that LCPT exhibits approximately 30% greater oral bioavailability, a prolonged time to maximum concentration (Tmax ≈ 6 hours), and attenuated peak-to-trough fluctuation compared with IR-Tac.5,6 Consequently, equivalent trough concentrations (C0) can be achieved with approximately 20–30% lower total daily doses, reflecting improved systemic utilization of the administered drug.6,7 From a pharmacokinetic perspective, these characteristics may confer clinical advantages by reducing peak-associated toxicity while maintaining sustained calcineurin inhibition throughout the dosing interval.
Notwithstanding these pharmacokinetic improvements, the extent to which formulation-driven changes in tacrolimus delivery translate into superior clinical outcomes has not been definitively established. Randomized controlled trials and observational studies have generally reported comparable rates of biopsy-proven acute rejection (BPAR) and graft survival between LCPT and IR-Tac.6,7 However, interpretation of the existing literature is complicated by prior systematic reviews that have aggregated LCPT with other once-daily tacrolimus formulations, such as Advagraf® (tacrolimus extended-release capsules) and Astagraf XL®, despite substantial differences in release mechanisms and pharmacokinetic behavior.8,9 This methodological approach limits the capacity to isolate the clinical contribution of specific drug-delivery technologies.
Accordingly, a formulation-specific evaluation is warranted to delineate the translational impact of MeltDose-based tacrolimus delivery. The present systematic review was undertaken to synthesize available evidence comparing LCPT with IR-Tac across solid-organ transplantation, with particular emphasis on the relationship between formulation-driven pharmacokinetic optimization and clinically relevant outcomes.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines and was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration ID: CRD420241178544).
The primary outcome was the incidence of BPAR, a clinically validated endpoint reflecting the adequacy of calcineurin inhibition. Secondary outcomes included graft survival, all-cause mortality, renal function (estimated glomerular filtration rate [eGFR]), metabolic complications (including new-onset diabetes after transplantation [NODAT]), adverse events, and tacrolimus pharmacokinetic parameters. Trough concentration (C0) was evaluated as the principal pharmacokinetic indicator of systemic drug exposure.
This review focused exclusively on LCPT, the only tacrolimus formulation utilizing MeltDose technology. Data from other once-daily extended-release formulations (eg, Advagraf®, Astagraft XL®) were not pooled, given fundamental differences in release mechanisms and pharmacokinetic profiles. A systematic literature search was conducted in PubMed/MEDLINE and Google Scholar from database inception to October 2025, which served as the final search cutoff. The search strategy combined Medical Subject Headings (MeSH) and free-text terms, including “tacrolimus”, “LCPT”, “LCP-tacrolimus”, “Envarsus XR”, “MeltDose”, and “immediate-release tacrolimus”, using Boolean operators (AND, OR). Reference lists of relevant studies and reviews were manually screened to identify additional eligible publications. No language or publication date restrictions were applied.
Eligible studies met the following criteria: (1) adult recipients of solid-organ transplants (kidney, liver, heart, or lung); (2) comparison of LCPT administered once daily with IR-Tac administered twice daily; and (3) reporting of tacrolimus trough concentrations during follow-up. Both randomized controlled trials and comparative observational studies were included. Studies were excluded if they lacked pharmacokinetic data, were single-arm pharmacokinetic analyses, were narrative or systematic reviews, or involved extended-release tacrolimus formulations other than LCPT. Titles, abstracts, and full-text articles were screened independently by two reviewers. Disagreements were resolved through consensus. Data were extracted using a standardized form, which captured study design, transplant type, clinical setting (de novo or conversion), sample size, immunosuppressive regimen, dosing strategy, and tacrolimus trough concentrations (C0) at baseline and predefined follow-up intervals (eg, 1, 3, 6, and 12 months).
Methodological quality was assessed using validated instruments appropriate to study design. Randomized controlled trials were evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool, and observational studies were assessed using the Newcastle–Ottawa Scale (NOS). Assessments were performed independently by two reviewers, with disagreements resolved by consensus. Risk-of-bias judgments were summarized descriptively and considered in the interpretation of findings. Given heterogeneity in transplant populations, study designs, follow-up durations, and outcome definitions, a quantitative meta-analysis was not performed. Instead, findings were synthesized qualitatively, with emphasis on formulation-related differences in tacrolimus pharmacokinetics and their association with clinical outcomes.
Results
A total of 351 records were identified through database searching. Following removal of duplicates, 326 records underwent title and abstract screening, of which 289 were excluded. Thirty-six full-text articles were assessed for eligibility; 30 were excluded for the following reasons: noncomparative design (n = 21), use of non-LCPT formulations (n = 3), cyclosporine comparator (n = 1), and lack of relevant outcomes (n = 5). Ultimately, six studies met inclusion criteria and were included in the qualitative synthesis. The study selection process is summarized in Figure 1. Methodological quality varied across included studies. Randomized controlled trials demonstrated low risk of bias overall, with the exception of one open-label pilot study, which raised some concerns regarding performance and detection bias. Observational studies were of moderate methodological quality, with increased risk of selection bias observed in studies employing historical controls. The single-arm liver transplant study was interpreted descriptively owing to the absence of a concurrent comparator. The characteristics and key clinical outcomes of the included studies are summarized in Tables 1 and 2, and methodological quality assessments are presented in Table 3. Key sources of heterogeneity across the included studies are summarized in Table 4.
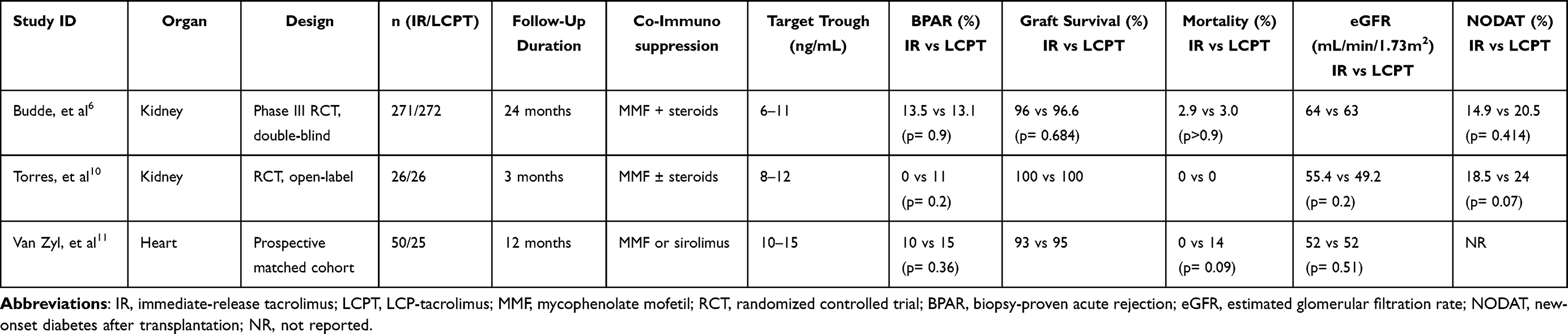 |
Table 1 De Novo Use of LCPT vs Immediate-Release Tacrolimus |
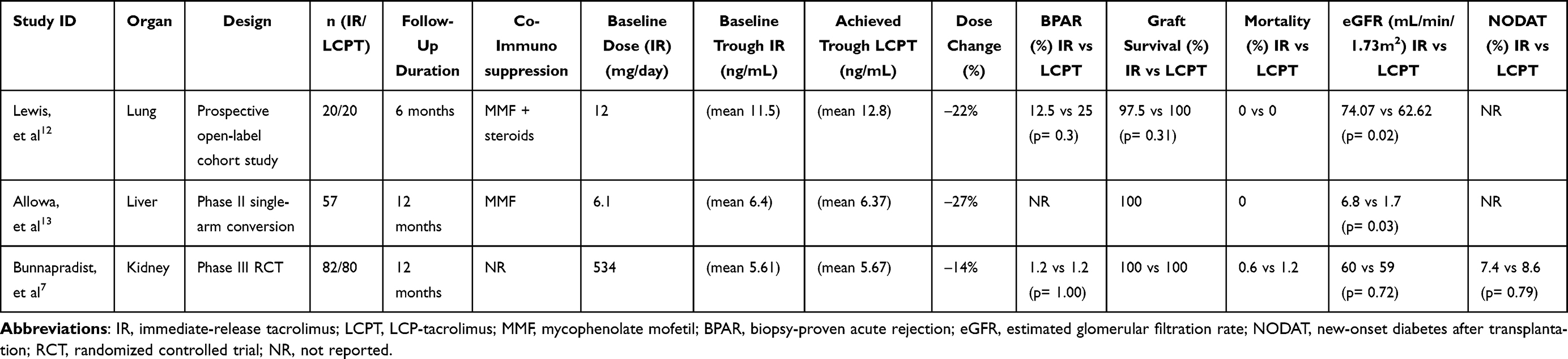 |
Table 2 Clinical Outcomes After Conversion from IR-Tac to LCPT |
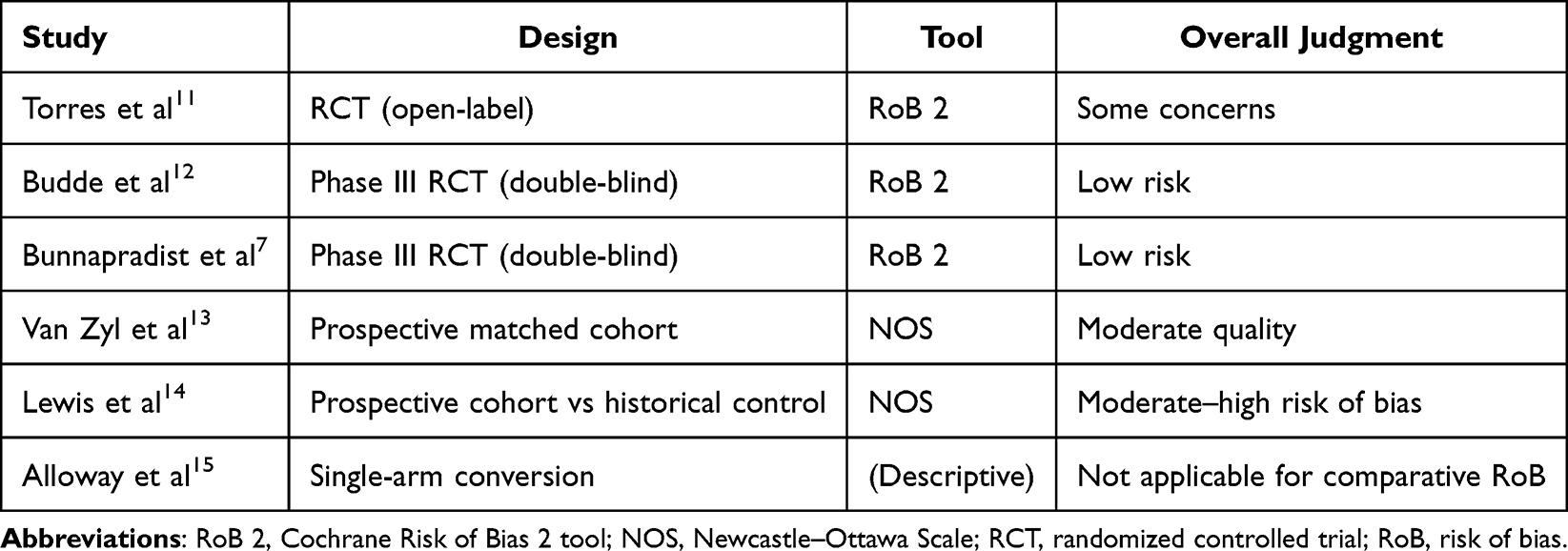 |
Table 3 Risk-of-Bias/Quality Assessment Summary |
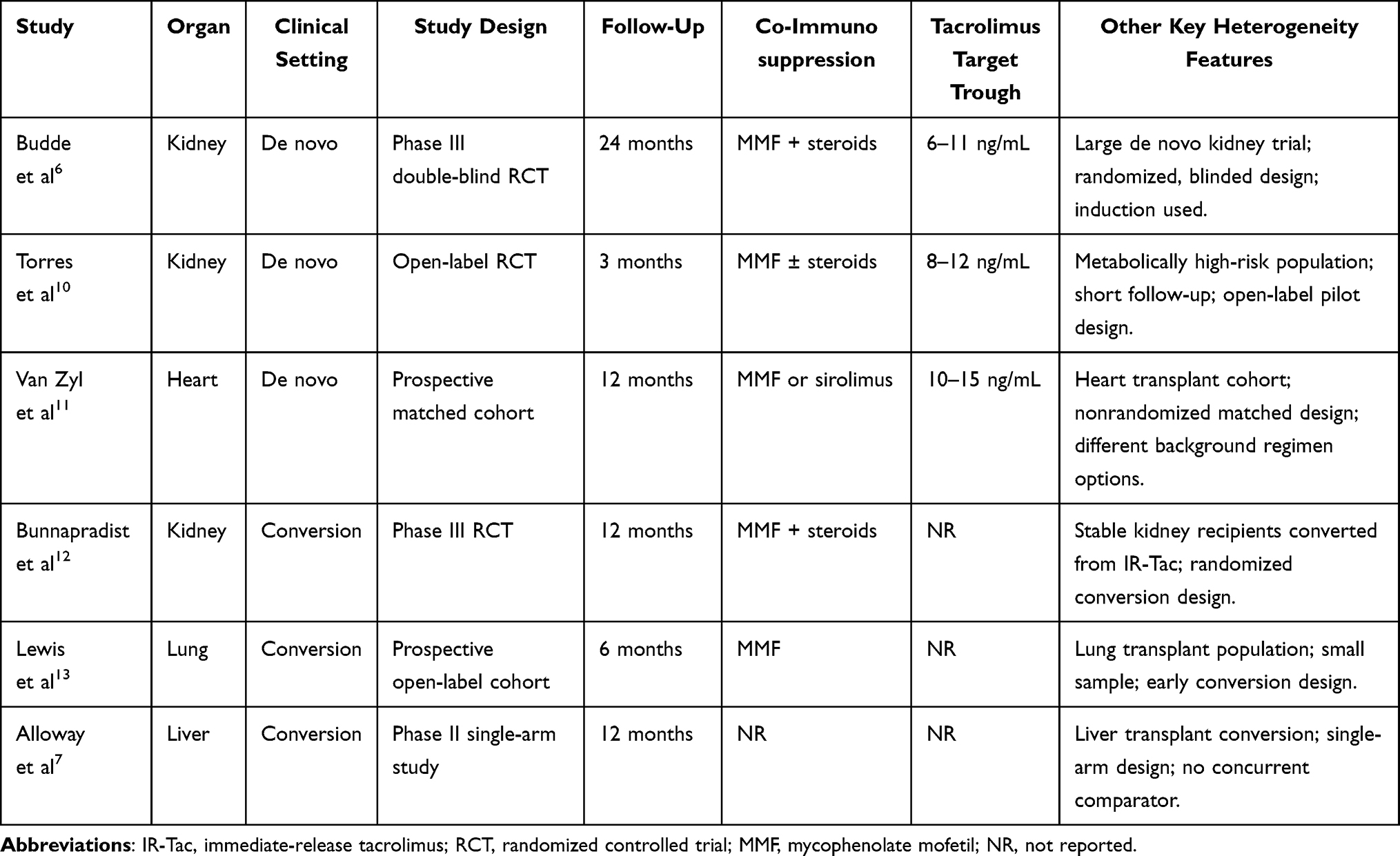 |
Table 4 Key Sources of Heterogeneity Across Included Studies |
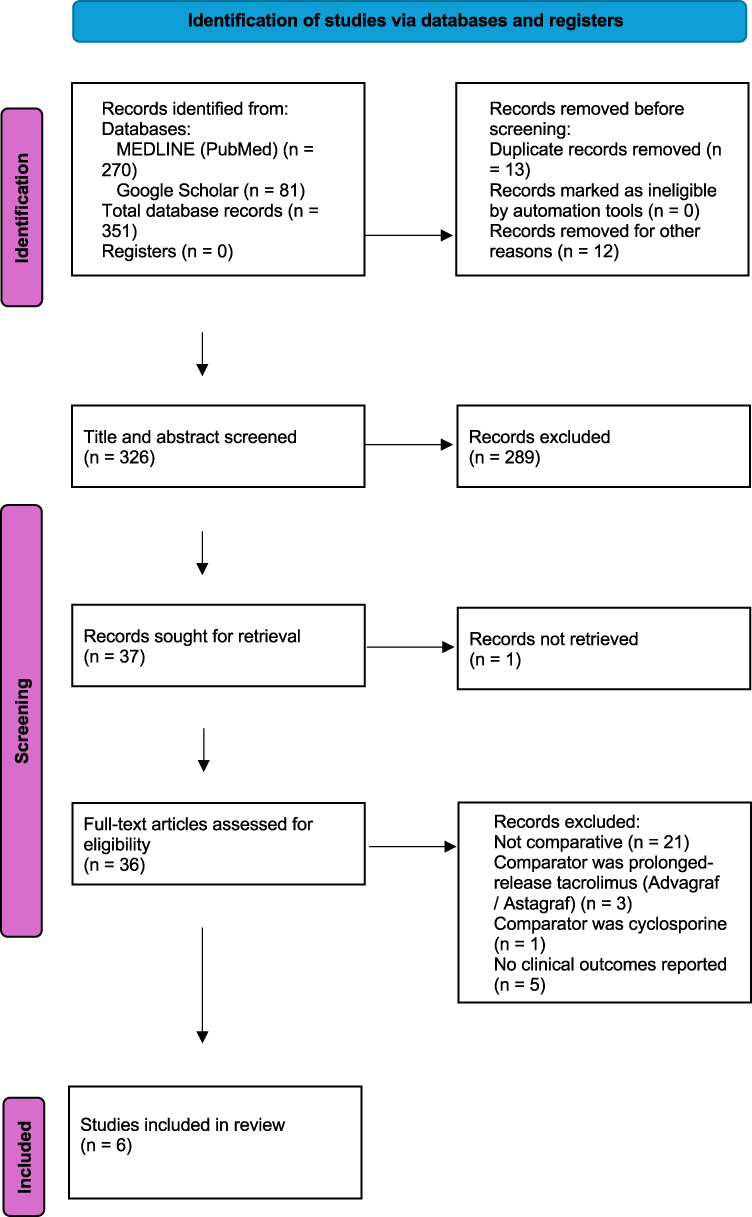 |
Figure 1 PRISMA 2020 flow diagram showing the identification, screening, eligibility assessment, and final inclusion of studies in this systematic review. |
In de novo kidney transplantation, two studies evaluated LCPT initiation. A pilot randomized trial with a small sample size involving metabolically high-risk recipients reported that BPAR occurred more frequently with LCPT than with IR-Tac (11% vs 0%) over a 3-month follow-up period.10 Graft survival was 100% in both groups, with no mortality observed. Renal function was comparable between groups (eGFR 49.2 vs 55.4 mL/min/1.73 m2; p = 0.2), and rates of new-onset diabetes after transplantation did not differ significantly (24% vs 18.5%; p = 0.07).10 More robust evidence derives from a phase III double-blind randomized controlled trial (n = 543) with 24-month follow-up.6 In this study, BPAR rates were similar between LCPT and IR-Tac (13.1% vs 13.5%; p = 0.9), with comparable graft survival (96.6% vs 96%; p = 0.684) and mortality (3.0% vs 2.9%; p > 0.999). Renal function remained stable in both groups (eGFR 63 vs 64 mL/min/1.73 m2), and the incidence of new-onset diabetes after transplantation did not differ significantly between formulations (20.5% vs 14.9%; p = 0.414).6
In heart transplantation, a prospective matched-cohort study evaluated LCPT initiation and demonstrated noninferiority for the composite endpoint of death, rejection, or graft dysfunction at 12 months.11 BPAR rates were numerically higher with LCPT compared with IR-Tac (15% vs 10%; p = 0.36), although this difference did not achieve statistical significance. Graft survival remained high in both groups (95% vs 93%), and renal function trajectories were comparable throughout the follow-up period.11 Detailed outcome data for de novo studies are presented in Table 1.
Conversion from IR-Tac to LCPT was evaluated across kidney, liver, and lung transplantation, with generally comparable clinical outcomes observed despite heterogeneity in study design and follow-up duration. In stable kidney transplant recipients, the phase III MELT trial provided the most robust conversion data.7 BPAR rates were identical between LCPT and IR-Tac (1.2% vs 1.2%), with graft survival of 100% in both groups. Mortality rates were low (1.2% vs 0.6%), and renal function remained stable throughout the 12-month follow-up period (eGFR 59 vs 60 mL/min/1.73 m2). The incidence of new-onset diabetes after transplantation was similar between groups (8.6% vs 7.4%).7 In lung transplantation, a prospective cohort study compared LCPT with IR-Tac over 6 months of follow-up.12 BPAR rates were numerically higher with LCPT (25% vs 12.5%; p = 0.30), although this difference did not reach statistical significance. Graft survival was high in both groups (100% vs 97.5%), and no mortality was observed. Renal function favored IR-Tac (eGFR 74.07 vs 62.62 mL/min/1.73 m2; p = 0.02), although interpretation is limited by the small sample size.12 In liver transplantation, a phase II single-arm study evaluated conversion from IR-Tac to LCPT in stable recipients over 12 months.13 Graft survival was 100%, and no mortality was observed. The incidence of renal impairment was numerically lower following conversion compared with baseline IR-Tac exposure (1.7% vs 6.8%; p = 0.03), and upper respiratory infections were less frequent after conversion (1.7% vs 5.1%).13 However, the absence of a concurrent comparator limits causal inference. Detailed outcome data for conversion studies are presented in Table 2.
Across all included studies, LCPT consistently achieved therapeutic tacrolimus C0 with lower total daily doses compared with IR-Tac, reflecting the enhanced bioavailability conferred by MeltDose technology.6,7 The magnitude of dose reduction ranged from approximately 14% to 27% across studies, while trough concentrations remained within established therapeutic targets.6,7,12,13
Discussion
This systematic review offers a formulation-specific assessment of LCPT relative to immediate-release tacrolimus, focusing on how drug-delivery design, pharmacokinetic performance, and clinical outcomes intersect in solid-organ transplantation. Across the included studies, LCPT showed comparable efficacy in terms of BPAR, graft survival, and mortality while achieving therapeutic exposure at lower total daily doses. Nevertheless, from a clinical transplant perspective, long-term outcomes remain more important than pharmacokinetic efficiency alone, and current evidence does not demonstrate clear clinical superiority of LCPT in these domains.
From a drug-delivery perspective, tacrolimus is a narrow therapeutic index drug whose clinical performance is highly dependent on formulation-driven pharmacokinetics.1,14 Immediate-release tacrolimus is characterized by variable gastrointestinal absorption and substantial inter- and intra-patient variability due to solubility limitations, CYP3A metabolism, and P-glycoprotein transport.2,14 LCPT was specifically developed to address these limitations through MeltDose solid-dispersion technology, resulting in improved dissolution and a more controlled absorption profile.4,5 This produces a distinct pharmacokinetic profile characterized by increased bioavailability, delayed peak concentration, and reduced peak-to-trough fluctuation.4,5
Recent pharmacokinetic data provide quantitative confirmation of these formulation differences. LCPT demonstrates a markedly prolonged effective half-life compared with IR-Tac (48.4 vs 12.5 hours) and a higher accumulation ratio (3.18 vs 2.06), indicating greater persistence of systemic exposure across the dosing interval.16 Importantly, this prolonged effective half-life reflects extended absorption rather than delayed elimination, highlighting that LCPT fundamentally modifies the input kinetics of tacrolimus delivery. From a translational standpoint, this results in a smoother exposure profile with reduced fluctuation, which may improve exposure consistency. These pharmacokinetic advantages are reflected in clinical outcomes, particularly in kidney transplantation. In the phase III randomized trial, LCPT maintained comparable BPAR (13.1% vs 13.5%), graft survival (96.6% vs 96.0%), and mortality (3.0% vs 2.9%) despite a 20–30% lower total daily dose, supporting improved absorption efficiency without loss of efficacy.6 However, this effect was not uniform across all settings. In a pilot randomized trial of metabolically high-risk recipients, LCPT was associated with a numerically higher BPAR (11% vs 0%) over short follow-up, despite similar renal function and nonsignificant differences in metabolic outcomes.10 These findings suggest that early post-transplant physiology and patient-specific risk factors may influence the clinical impact of formulation-driven pharmacokinetic improvements.
In non-kidney transplant populations, the evidence is more limited and heterogeneous. In heart transplantation, LCPT was associated with numerically higher BPAR (15% vs 10%) with comparable graft survival (95% vs 93%), although differences were not statistically significant.11 In lung transplantation, a larger numerical difference was observed (25% vs 12.5%), again without statistical significance but clinically notable given the magnitude of the absolute difference.12 These findings suggest that formulation-driven pharmacokinetic optimization does not uniformly translate into improved clinical outcomes, particularly in populations characterized by high physiologic variability and complex early post-transplant dynamics.
Conversion studies further support the pharmacokinetic efficiency of LCPT. In the MELT trial, rejection rates were identical between LCPT and IR-Tac (1.2% vs 1.2%), with preserved graft survival and stable renal function (eGFR 59 vs 60 mL/min/1.73 m2) despite dose reduction.7 Similarly, in liver transplantation, conversion to LCPT was associated with numerically lower renal impairment (1.7% vs 6.8%) and fewer infectious complications compared with baseline IR-Tac exposure, although the absence of a concurrent comparator limits causal inference.13 Collectively, these findings support improved dose efficiency and maintenance of immunologic stability following conversion.
A central mechanistic advantage of LCPT relates to exposure variability. High intrapatient variability in tacrolimus exposure has been strongly associated with adverse outcomes, including rejection, donor-specific antibody formation, and graft loss.17,18 LCPT is theoretically positioned to mitigate this risk through prolonged absorption and reduced peak-to-trough fluctuation. However, pharmacokinetic variability measures such as intra- and interpatient coefficient of variation and time in therapeutic range were not reported in the included primary studies and therefore could not be systematically evaluated in this review. As a result, the hypothesized benefit of LCPT in reducing clinically meaningful variability remains inferred rather than directly demonstrated.
From a pharmacodynamic perspective, these observations are consistent with current understanding of tacrolimus activity. Tacrolimus efficacy is mediated by sustained intracellular calcineurin inhibition rather than transient peak concentrations.14,19 Therefore, a formulation that reduces fluctuation and prolongs exposure may enhance immunologic stability. At the same time, reduced peak exposure may mitigate concentration-dependent toxicity, particularly nephrotoxicity, which is linked to calcineurin inhibitor–induced vasoconstriction and chronic injury.20 The numerically lower renal impairment observed in liver transplant conversion studies is consistent with this mechanism, although not definitive.13
Safety outcomes overall remain inconsistent. While some studies suggest potential renal or neurologic benefit, others show no meaningful differences or numerically higher rates of metabolic complications, such as new-onset diabetes after transplantation (20.5% vs 14.9% in the phase III trial).6 These findings indicate that pharmacokinetic optimization does not uniformly translate into improved safety, reflecting the multifactorial nature of tacrolimus-associated toxicity.
This review has several strengths, including its formulation-specific focus and integration of pharmacokinetic and clinical outcome data. By isolating LCPT, this analysis avoids the methodological limitations of prior reviews that grouped pharmacokinetically distinct extended-release tacrolimus formulations together.8,9 However, important limitations remain. The number of included studies is limited, particularly outside kidney transplantation; many studies are underpowered to detect moderate differences in clinical outcomes; heterogeneity in study design and follow-up limits comparability; and pharmacokinetic variability was not systematically assessed. Additionally, observational data are inherently subject to selection bias, as conversion to LCPT is often performed in clinically stable recipients.
In aggregate, the available evidence supports the conclusion that LCPT achieves pharmacokinetic optimization without consistent clinical superiority. While it improves bioavailability, prolongs effective exposure, and reduces dose requirements, it does not uniformly improve rejection rates, graft survival, or safety outcomes across all populations. Notably, several studies demonstrate numerically higher rejection rates with LCPT in specific contexts, suggesting that equivalence may not be uniform. The clinical role of LCPT may therefore lie in targeted application, particularly in patients with high pharmacokinetic variability, dose inefficiency, adherence challenges, or intolerance to peak-related toxicity. Future studies should directly evaluate intrapatient variability, exposure–response relationships, and long-term outcomes using standardized pharmacokinetic endpoints. Until such data are available, LCPT should be considered a pharmacokinetically optimized formulation with selective clinical advantages, rather than a universally superior alternative to immediate-release tacrolimus. Its clinical role may be greatest in selected patients, including those with high pharmacokinetic variability, adherence challenges, intolerance to peak-related toxicity, or dose inefficiency related to drug interactions; however, its role in higher-risk early post-transplant settings requires further study.
Acknowledgments
The author acknowledge the contributions of the independent reviewers who assisted with study design, literature screening, and data extraction, which supported the methodological rigor of this systematic review.
Funding
This research received no external funding.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Scalea JR, Levi ST, Ally W, Brayman KL. Tacrolimus for the prevention and treatment of rejection of solid organ transplants. Expert Rev Clin Immunol. 2016;12(3):333–10. doi:10.1586/1744666X.2016.1123093
2. Coste G, Lemaitre F. The role of intra-patient variability of tacrolimus drug concentrations in solid organ transplantation: a critical appraisal of the literature. Pharmaceutics. 2022;14(2):379. doi:10.3390/pharmaceutics14020379
3. Rostaing L, Jouve T, Terrec F, Malvezzi P, Noble J. Adverse drug events after kidney transplantation. J Pers Med. 2023;13(12):1706. doi:10.3390/jpm13121706
4. Tremblay S, Nigro V, Weinberg J, Woodle ES, Alloway RR. A steady-state head-to-head pharmacokinetic comparison of all FK-506 (tacrolimus) formulations (ASTCOFF): an open-label, prospective, randomized, two-period, crossover study. Am J Transplant. 2017;17(2):432–442. doi:10.1111/ajt.13935
5. Kamar N, Cassuto E, Piotti G, et al. Pharmacokinetics of prolonged-release once-daily formulations of tacrolimus in de novo kidney transplant recipients: a randomized, parallel-group, open-label, multicenter study. Adv Ther. 2019;36(2):462–477. doi:10.1007/s12325-018-0855-1
6. Budde K, Bunnapradist S, Grinyo JM, et al. Novel once-daily extended-release tacrolimus (LCPT) versus twice-daily tacrolimus in de novo kidney transplants: one-year results of Phase III, double-blind, randomized trial. Am J Transplant. 2014;14(12):2796–2806. doi:10.1111/ajt.12955
7. Bunnapradist S, Ciechanowski K, West-Thielke P, et al. Conversion from twice-daily tacrolimus to once-daily extended release tacrolimus (LCPT): the phase III randomized MELT trial. Am J Transplant. 2013;13(3):760–769. doi:10.1111/ajt.12035
8. Saengram W, Vadcharavivad S, Poolsup N, Chancharoenthana W. Extended-release versus immediate-release tacrolimus in kidney transplant recipients: a systematic review and meta-analysis. Eur J Clin Pharmacol. 2018;74(10):1249–1260. doi:10.1007/s00228-018-2512-7
9. Vadcharavivad S, Saengram W, Phupradit A, Poolsup N, Chancharoenthana W. Once-daily versus twice-daily tacrolimus in kidney transplantation: a systematic review and meta-analysis of observational studies. Drugs. 2019;79(18):1947–1962. doi:10.1007/s40265-019-01217-7
10. Torres A, Rodríguez-Adanero C, Fernández-Rivera C, et al. LCP-tacrolimus versus immediate-release tacrolimus in metabolically high-risk de novo kidney transplant recipients: a pilot randomized controlled trial. J Clin Med. 2024;13(24):7802. doi:10.3390/jcm13247802
11. van Zyl JS, Sam T, Clark DM, et al. LCP-tacrolimus versus immediate-release tacrolimus in heart transplantation: a single-center matched cohort study. Clin Transplant. 2021;35(12):e14487. doi:10.1111/ctr.14487
12. Lewis TC, Hotchkis P, Wong A, et al. Extended-release tacrolimus (LCPT) in lung transplant recipients: a prospective cohort study. Clin Transplant. 2025;39(5):e70159. doi:10.1111/ctr.70159
13. Alloway RR, Eckhoff DE, Washburn WK, Teperman LW. Conversion from twice-daily tacrolimus to once-daily extended-release tacrolimus (LCPT) in stable liver transplant recipients: results of a phase II open-label study. Liver Transpl. 2014;20(5):564–575. doi:10.1002/lt.23844
14. Staatz CE, Tett SE. Clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantation. Clin Pharmacokinet. 2004;43(10):623–653. doi:10.2165/00003088-200443100-00001
15. Ekberg H, Tedesco-Silva H, Demirbas A, et al. Reduced exposure to calcineurin inhibitors in renal transplantation. N Engl J Med. 2007;357(25):2562–2575. doi:10.1056/NEJMoa067411
16. Momper JD, Venkataramanan R, Jantz AS, et al. Evaluation of effective half-life and its impact on time to steady state for oral MeltDose tacrolimus (LCPT) in de novo kidney transplant recipients. Ther Drug Monit. 2025;47(1):169–173. doi:10.1097/FTD.0000000000001270.
17. Kuypers DRJ. Intrapatient variability of tacrolimus exposure in solid organ transplantation: a novel marker for clinical outcome. Clin Pharmacol Ther. 2020;107(2):347–358. doi:10.1002/cpt.1618
18. Shuker N, Shuker L, Van Rosmalen J, et al. A high intrapatient variability in tacrolimus exposure is associated with poor long-term outcome of kidney transplantation. Transpl Int. 2016;29(11):1158–1167. doi:10.1111/tri.12798
19. Fontova P, Van Merendonk LN, Vidal-Alabró A, et al. Intracellular tacrolimus concentration correlates with T-cell calcineurin phosphatase inhibition. Pharmaceutics. 2023;15(5):1481. doi:10.3390/pharmaceutics15051481
20. Naesens M, Kuypers DRJ, Sarwal M. Calcineurin inhibitor nephrotoxicity. Clin J Am Soc Nephrol. 2009;4(2):481–508. doi:10.2215/CJN.04800908
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.