Back to Journals » Open Access Emergency Medicine » Volume 16
Clinical Features of Severe Deep Neck Space Infection: Five Clinical Cases and Our Experience in Their Management
Authors Jin L, Chang Y, Zhao Y, Fan K, Lu J, Wang Y, Yu S ![]()
Received 5 June 2024
Accepted for publication 20 November 2024
Published 26 November 2024 Volume 2024:16 Pages 257—266
DOI https://doi.org/10.2147/OAEM.S476737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Ling Jin,1,* Yongjun Chang,1,* Yihua Zhao,2,* Kai Fan,1,* Jiawei Lu,1 Yang Wang,1 Shaoqing Yu1
1Department of Otolaryngology, Head and Neck Surgery, Tongji Hospital, School of Medicine, Tongji University, Shanghai, 200065, People’s Republic of China; 2Department of Otolaryngology, Jinan Zhangqiu District Hospital of Traditional Chinese Medicine, Jinan, 250200, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shaoqing Yu, Department of Otolaryngology, Head and Neck Surgery, Tongji Hospital, 389 Xincun Road, Putuo District, Shanghai City, 200065, People’s Republic of China, Email [email protected]
Background: Deep neck space infection (DNSI) is an acute and severe condition, with severe cases being relatively rare but considerably more critical. Consequently, in clinical practice, there is a limited understanding and lack of comprehensive reviews on severe DNSI.
Methods: We conducted a retrospective analysis of the diagnosis and treatment of five cases of severe DNSI admitted to our department.
Results: All five patients were diagnosed via neck CT and surgical exploration. Bacterial cultures predominantly revealed mixed infections of Klebsiella and other gram-negative bacilli, along with anaerobic bacteria. Three patients had diabetes, two presented with diabetic ketoacidosis, and three had mediastinal involvement. Three patients underwent tracheotomy, while two required tracheal intubation. All patients were treated with neck incision, drainage, regular dressing changes, and targeted antibiotic therapy. They had an average hospital stay of 35.8 days, and all were discharged fully recovered.
Conclusion: Severe DNSI tends to occur in patients with diabetes and other underlying systemic conditions. Infections involving multiple deep neck spaces, such as the parapharyngeal, pretracheal, and prevertebral spaces, leading to high-risk complications like airway obstruction, cervical necrotizing fasciitis, mediastinitis, and sepsis, are considered severe DNSI. Early diagnosis, timely surgical exploration, drainage to maintain airway patency, and targeted antibiotic therapy are crucial to effective management.
Keywords: deep neck space infection, severe infections, diagnosis, therapeutics, comorbidity
Introduction
Deep neck space infections (DNSIs) refer to the general term for abscesses or cellulitis in the superficial deep tissues of the deep neck fascia,1–3 with an incidence rate of 9–15/100,000 per year.4–6 According to a study conducted in Finland, the incidence rate of DNSIs has been increasing in recent years.7 It is often derived from infections of the teeth, pharynx, tonsils and lymph nodes.8–11 The most common symptoms are neck pain, swelling, dysphagia, and fever, but the disease develops rapidly and aggressively, and severe fatal complications such as airway obstruction, mediastinitis, septicaemia, pericarditis and pneumonia can be caused, etc.12 According to the literature, the reported mortality rate for this disease ranges from 1.6% to 50%,13 making it one of the most acute and life-threatening conditions encountered in Otorhinolaryngology–Head and Neck Surgery, and it cannot be effectively managed with antibiotics alone. The classification of the severity of deep cervical space infections is essential in guiding timely diagnosis and treatment, as well as the timely and effective implementation of multiple therapeutic strategies.
Therefore, in order to raise awareness, five cases of severe DNSI admitted to our department from 2011 to 2020 are summarised and analysed. All patients in this study provided written informed consent regarding their personal or clinical details along with any identifying images to be published in this study.
Materials and Methods
Clinical Data
Case 1
A 43-year-old male was admitted to the hospital in the spring of 2011 with a chief complaint of “pharyngalgia accompanied by fever for two days, along with dysphagia and left-sided neck swelling”. He had a history of diabetes but was not treated. On physical examination upon admission, the patient had a temperature of 38.6°C, mild shortness of breath, and a hemispherical, erythematous, and swollen epiglottis covered with a light yellow pseudomembrane. The skin on the left side of the neck was diffusely erythematous and swollen. The initial diagnosis was acute epiglottitis and deep neck space infection. On the 5th day of admission, the symptoms worsened with high fever (39.7°C), short breath, orthopnea, diffuse swelling of the neck increased, and the left upper chest was involved. CT of the neck showed that the air cavity between the soft tissues of the anterior cervical was multifocal and spread down the anterior trachea to the upper mediastinum and pericardium and there is atelectasis in the left lower lobe (Figure 1a). After general anesthesia, tracheal intubation, and neck incision, there was extensive necrosis of the surface of the deep cervical fascia and a large amount of thick light grayish white pus with between it and the strap muscles, and the pus has a foul smell. The superior boundary of the abscess cavity extended to the level of the hyoid bone, and under endoscopic guidance, the pus was observed spreading inferiorly along the pretracheal fascial plane into the superior mediastinum. The additional diagnoses included cervical necrotizing fasciitis (CNF), mediastinitis, and pericarditis.
 |
Figure 1 Image of the patients. (a) Case 1 Coronal reconstruction CT: larynx, anterior tracheal space of neck and patchy pneumatosis of anterior superior mediastinum (white arrow), anterior middle superior mediastinum fat structure is blurred. (b) Case 2 CT in transverse position: bilateral neck swelling with pneumatosis (white arrow), obvious on the left side. (c) Case 3 sagittal CT: epiglottis to thyroid cartilage layer soft tissue swelling with pneumatosis (white arrow). (d) Case 4 Coronal CT: Abscess formation in the lower neck and paratracheal space with pneumatosis (white arrow). (e) Case 5 coronal CT: left side oropharyngeal side wall, left parotid gland area, submandibular, inferior neck and upper mediastinum pneumatosis (white arrow). |
Case 2
A 75-year-old male was admitted to the hospital in the summer of 2016 with a 4-day history of facial and neck swelling accompanied by pain, which had worsened with the onset of dyspnea over the past day. He had a history of hypertension, cerebral infarction, and no history of diabetes. Physical examination on admission: T: 37.4°C, shortness of breath, orthopnea, diffuse redness on face, bilateral neck (submandibular to clavicle below about 3 transverse fingers), diffuse erythema and swelling, obvious on the left side; high skin temperature, tenderness, local subcutaneous crepitus, neck activity is restricted; left-sided tonsillar congestion and swelling II degree, left soft palate and palatoglossal arch hyperemia and swelling. Preliminary diagnosis: left peritonsillar abscess, deep neck space infection. Incising the left swollen palatoglossal arch, no obvious pus overflow was observed, but the cavity was grayish brown with odor. On the day of admission, “tracheotomy” was performed under general anesthesia to keep the airway open. On the fourth day after admission, enhanced CT of the neck showed diffuse swelling in the neck, anterior mediastinum, left pharyngeal recess, parotid gland, masseter muscle area with local low-density area and pneumatosis sign, and abscess formation in the left neck was considered (Figure 1b). Neck incision was performed to drain pus, and there was a large amount of stench and gray-brown pus overflowed from the deep side of the platysma. The deep normal tissue structure of neck was destroyed, fascia diffuse necrosis and part of soft tissue necrosis were observed. The pus cavity reaches the level of the clavicle from the lower edge of the mandible and reaches the prevertebral space backwards, scattered small blood vessel occlusion and muscle swelling but no obvious necrosis. Further diagnosis: left CNF, anterior superior mediastinitis.
Case 3
An 81-year-old male was admitted to the hospital in the spring of 2019 with a three-day history of pharyngalgia and dysphagia. He has hypertension and diabetes. Physical examination: T: 37.5°C, breathing is stable, the lingual surface of epiglottis congestion and swelling. Initial diagnosis of “acute epiglottis”. On the fourth day of admission to the hospital, there was hyperemia and swelling in the suprathyroid cartilage in the middle of the neck, accompanied by laborious breathing. Neck CT showed soft tissue swelling with pneumatosis from left epiglottis to thyroid cartilage (Figure 1c). Perform tracheotomy and neck incision exploration, and saw the formation of abscesses in the anterior epiglottic space between thyroid cartilage and hyoid bone, which were thick yellow pus with smelly. Further diagnosis: Abscess of deep neck space abscess.
Case 4
A 62-year-old male was admitted to the hospital in the summer of 2019 with a 5-day history of pharyngalgia, fever, and dysphagia, along with neck swelling and pain for 2 days, with no history of diabetes or other underlying conditions. Physical examination: T: 38.2°C, left laryngopharyngeal side wall swelling obvious, epiglottis without hyperemia, swelling; bilateral upper neck swelling obvious with tenderness. On the second day of admission, the neck swelling became worse, spreading to the upper sternum fossa, and there was a feeling of crepitus. Neck CT: The swelling of the left parapharyngeal space and the soft tissue of the lower neck was accompanied by a large liquid low-density shadow, considering abscess formation (Figure 1d). Under general anesthesia, an oral endotracheal intubation was performed, followed by a neck incision and drainage. A large amount of thick, yellow, foul-smelling pus was observed, with the abscess cavity involving the submandibular space, supraclavicular fossa, and pretracheal space. Diagnosis: left parapharyngeal space infection with involvement of multiple deep neck spaces.
Case 5
A 48-year-old male was admitted to the hospital in the spring of 2020 with a 3-day history of left-sided sore throat, restricted mouth opening, neck swelling, and fever. He had a history of diabetes, poor normal control, and a history of drug abuse and 10 years of detoxification. Physical examination on admission: T: 38.5 C, heart rate 108 beats/min, short breath, limited mouth opening (one finger), most of the lower left teeth are missing or only have residual roots; Left tonsil II degree swelling, left soft palate and Palatoglossal arch swelling obviously, epiglottis and Laryngopharynx cannot be examined; the skin on the left parotid gland, submandibular area, and left upper neck was hyperemic, with mild swelling and tenderness. Initial diagnosis peritonsillar abscess with infection of the deep neck space. The next day, the symptoms worsened, the patient was mentally depressed, drowsiness, heart rate continued to be 110 beats per minute and dyspnea. The left parotid gland area, submandibular and upper neck swelling aggravated, the skin temperature was high, and there was a feeling of crepitus. Ketoacidosis and sepsis also appeared. Head and neck CT: left oropharynx lateral wall, left facial parotid region, bilateral submandibular, left neck and upper mediastinum pneumatosis (Figure 1e).
Tracheotomy and a total of 3 neck incisions for drainage, the pus cavity spread to the left anterior parotid space, left parapharyngeal space, left sublingual, bilateral submandibular, submental space, left suprasternal space and the anterior superior mediastinum with a lot of gray-brown pus, odor. Fascial necrosis was like a pseudomembrane. Further diagnosis: CNF, upper mediastinitis.
Diagnostic Assessment
Bacterial cultures were performed on all 5 patients. One culture was negative, while 4 showed mixed infections of gram-negative bacilli, streptococci, and anaerobic bacteria. Among these, 2 cases involved drug-resistant Acinetobacter baumannii, 1 case involved anaerobic bacteria (Peptostreptococcus), and 1 case involved facultative anaerobic bacteria (Klebsiella oxytoca). See Table 1.
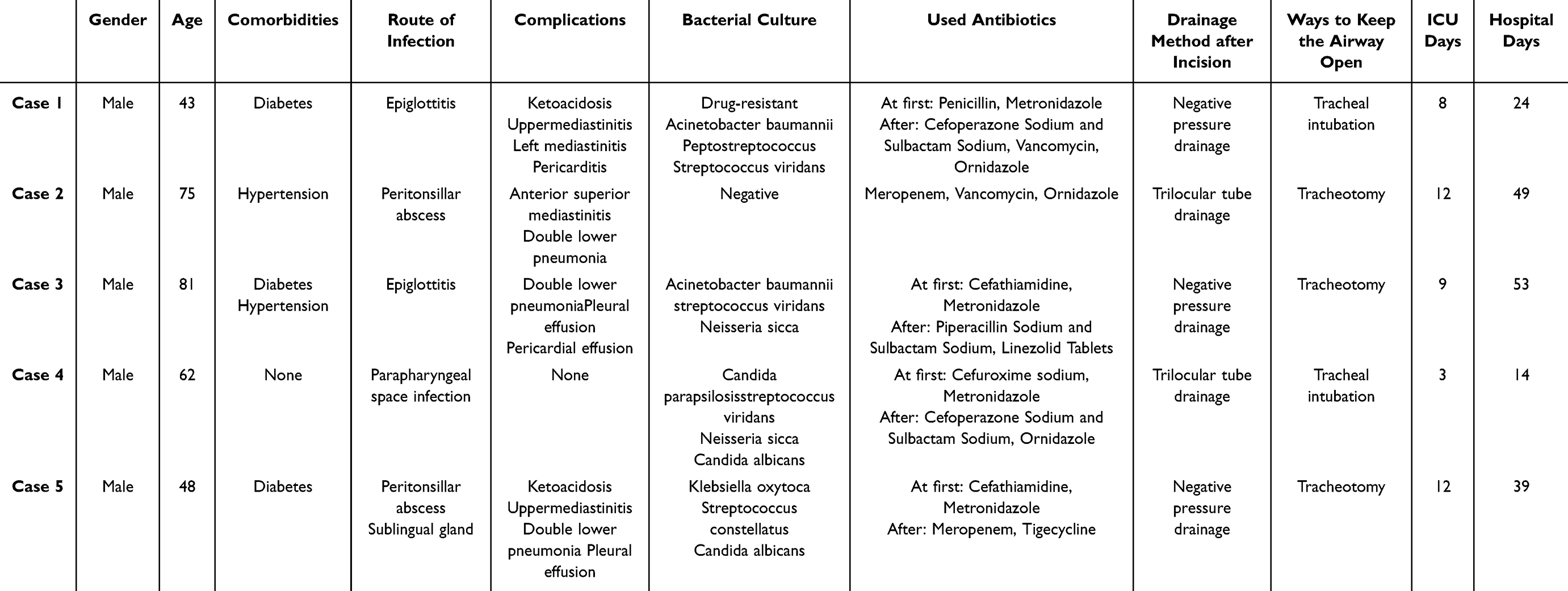 |
Table 1 Summary of the Features and Clinical Course of the Patients |
Treatment
Antibiotic treatment
All five patients were treated with cephalosporin antibiotics and metronidazole intravenous drip in the early stage of the disease, while vancomycin, linezolid, meropenem, ornidazole and other antibiotics were empirically upgraded in the progression of infection, and then antibiotics were adjusted according to bacterial culture and drug sensitivity.
Surgical treatment
All 5 patients underwent neck incision, debridement and drainage in time. Daily rinsing and dressing changes after surgery: Trilocular tube irrigation in 2 cases (cases 2 and 4); 2 cases of negative pressure drainage (case 1, 3); 1 case (case 5) negative pressure drainage combined with partial wound opening and dressing change. And 3 cases (cases 2, 4, 5) tracheotomy, three cases (cases 2, 4, and 5) had tracheotomy, and two cases (cases 1, 3) were intubated through the mouth to keep the airway open.
Supportive Treatment and Treatment of Comorbidities and Complications
Nasal Feeding, Intravenous Fluid Supplement and Timely Correction of Hypoproteinemia
Three cases (cases 1, 3, and 5) with diabetes were treated with hypoglycemic therapy by insulin, of which cases 1 and 5 were also expanded with blood volume to correct ketoacidosis. Except for case 2, the remaining 4 cases were complicated by pneumonia and pleural effusion, and were actively treated for anti-inflammatory, atomizing inhalation, and sputum excretion.
Follow-up and Outcomes
The five patients were all in the SICU intensive care unit after surgical drainage and were transferred back to the general ward after stable disease. After the above systemic treatment, all patients were cured and discharged, hospitalized for 14–53 days, with an average hospitalization of 35.8 days. Three cases (Case 1, Case 2, case 5) were finally diagnosed as “neck Necrotizing Fasciitis”, which underwent more than 2 times of debridement and drainage, and had a long time of washing and dressing change. Two cases had ketoacidosis, three had mediastinum infection, and four had pneumonia. We summarize the relevant information on the diagnosis and treatment of these 5 patients as follows, in Table 1.
Discussion
The fascia of the neck divides the neck into many potential cell ulitis spaces, with the hyoid bone as the boundary, which can be divided into the submandibular space, the submental space, and the parapharyngeal space above the hyoid bone and the pretracheal space, the suprasternal space and the superficial cervical space, the retropharyngeal space, the visceral vascular space, and the prevertebral space below the hyoid bone that communicates with each other. Due to the interconnection between the deep gaps of the neck,14 after the gap infection, the infection where the pus accumulates can spread along the anatomical pathway or between adjacent gaps. These spaces communicate downward with the pericardium, parietal pleura and mediastinum, thus becoming the entrance and passage for neck and throat infections to enter the thoracic cavity. DNSIs are mostly caused by infection sources around them, such as pharynx, tonsils, teeth and other infections, not limited to a single space but can spread to adjacent spaces and tissues to cause airway obstruction, pneumonia, neck necrotizing fasciitis, descending mediastinum inflammation, septicemia, sepsis and other high-risk complications,15–17 so it can be considered that the development of the above complications is a serious DNI. All cases have airway obstruction; 4 cases complicated with pneumonia; 3 cases caused upper mediastinitis and pericarditis; 3 cases developed cervical necrotizing fasciitis (CNS). We believe that CNF is a serious DNSI, and its diagnosis is not established at one time but is gradually confirmed according to the development and changes of the disease. Some authors believe that gas formation indicates a more serious infectious process.18 In this group of all cases, there is gas formation on CT images. It can be considered that one of the characteristics of severe DNSI is the formation of “gas”.
In this study, 3 of 5 patients had a history of diabetes, and all the 3 patients who with descending mediastinitis had a history of diabetes. Umeda et al reported 48 cases of CNF patients with descending mediastinitis.19 Among them, the mortality rate of patients with diabetes was 39.5%, which was significantly higher than the mortality rate of patients without underlying diseases (16.7%). Diabetes has been identified as the most common systemic disease of deep neck infections.1,2,4,20–22 In particular, patients with more than 10 years of diabetes are more prone to multi-space infections in the deep neck.23 DNSIs combined with diabetes are more severe and difficult to control, prone to ketoacidosis, and in severe cases, may have complications such as septicemia and sepsis, and have a higher mortality rate.15
The possible mechanisms for analysis are as follows: ① Disorders of substance metabolism, dysfunction of carbohydrates, increased lipolysis, and negative balance of protein metabolism in diabetic patients make the body’s immune function decline, and it is in a susceptible state; ② At the same time, the fat metabolites of diabetic patients increase and accumulate in the body, which increases the growth and reproduction of Gram-negative in the body;③Hyperglycemia is also conducive to the growth of pathogenic microorganisms such as bacteria, and concurrent infections can form a vicious circle, that is, infections cause uncontrollable hyperglycemia to further aggravate the infection; ④Monocyte IL-1β expression is abnormally low in diabetes, which can increase the body’s susceptibility to certain virulent bacteria;24 ⑤ The risk of periodontal infection, caries, and apical abscess in diabetic patients is significantly higher than that in non-diabetic patients, and it is more prone to odontogenic DNSI. Therefore, diabetes is an important cause of severe DNSI.
Analysis of DNSI in 173 cases by Srivanitchapoom et al showed that DNSI infection route was odontogenic > pharyngeal > with unknown cause > glandular origin (48.6%, 19.7%, 16.8%, 6.9%).25 Although the routes of infection have been reported to be different, the routes of infection for most DNSI are still predominantly of pharyngeal and odontogenic origin,26 but there are still some unknown causes. In this study, 2 of the 5 patients were acute epiglottitis, and 3 were DNSI secondary to peritonsillar abscess, all of which were pharyngeal. These 5 cases were all non-odontogenic in origin. This may be due to the long time span of 10 years and the small number of cases, which may not reflect the recent trend where odontogenic infections are more common.26
Another study believes that advanced age is one of the high-risk factors for DNSI.27 Cases in this group are 43–81 years old, with an average age of 61.8. It can be considered that elderly DNSI tend to develop into severe cases. All of the severe DNSI in our group were male, whether males are more likely to develop into severe DNSI remains to be further investigated in the future, but it has been reported in the literature in the past that there is a trend for DNSI to be more common in men than in women.3,28
Streptococcus species and anaerobic bacteria are the primary pathogens in deep neck space infections, including Staphylococcus coagulase negative (CNS),29 with mixed infections predominating.3,30,31 In this group of cases, the bacterial culture results were also mixed infection of negative bacilli and anaerobic bacteria (Table 1), which was consistent with the above characteristics.
CT has the advantages of fast and intuitive and has obvious advantages in the diagnosis of DNSI, especially contrast-enhanced CT. Therefore, imaging examination is particularly important. The characteristic manifestations of CT diagnosis of DNSI are as follows: When cellulitis occurs, the infected muscle is swollen, the edge is blurred, the fat in the fascial space disappears, and the flocculent density increases. After the formation of the abscess, the pus cavity showed a low density, the pus wall strengthened annularly, and some pus cavity had gas.3 CT can promptly diagnose potential serious complications such as upper airway obstruction, jugular vein thrombosis,32 and descending mediastinitis.33 The CT of this group of patients showed a large amount of gas accumulation in multiple spaces of the fascia, and some of the soft tissues were torn in the center and the edges were uneven, which was consistent with the imaging characteristics of severe DNSI.
Aggressive antimicrobial, incision and drainage and supportive therapy are the basic treatment of DNSI. Some scholars believe that if CT examination reveals that abscesses are widespread, early surgical incision and drainage is the key method of treatment.15 It has been reported in the literature that patients with dyspnea and a maximum abscess diameter >2.0 cm should be surgically interventioned as soon as possible.34,35 Incision and drainage can reduce local pressure, prevent infection from spreading further to the deep neck and mediastinum, inhibit anaerobic bacteria, and reduce upper airway obstruction.
Therefore, incision and drainage is the key to the treatment of severe DNSI. We believe that individualized drainage schemes should be selected according to the infection gap, location and scope: 1) Direct incision and drainage: the debridement can be repeated multiple times, the disadvantages are the need for multiple dressing changes, excessive trauma, and large scars left on the skin after recovery. 2) Negative pressure drainage: sucking out the pus after debridement, which can continuously discharge the pus out of the body, and it is also convenient for continuous washing and uninterrupted negative pressure suction can close the gap caused by the formation of abscess, Cases 1 and 3 adopted this method. 3) Trilocular tube drainage: It has negative pressure suction and is also conducive to washing when dressing change. Cases 2 and 4 use this method. Case 5 due to multiple gap infections and abscess formation on both sides of the deep neck, a combination of direct incision and negative pressure drainage was used. Therefore, according to the condition of the patient and choosing the appropriate incision and drainage method for the patient, it is conducive to treatment. Some studies have found that using a drainage tube does not prolong the patient’s hospital stay.22
In DNSI, tracheotomy has been stated as the gold standard in the management of compromised airway.36 Maintaining airway unobstructed is also a top priority for treatment. Severe DNSIs are often associated with airway obstruction. When surgical incision and drainage are performed, intraoperative traction and damage to the tissue of the posterior pharyngeal space and upper mediastinal tracheoesophageal sulcus can cause tissue edema. Postoperative airway obstruction may be aggravated. Therefore, the airway should be closely observed, and emergency tracheal intubation or tracheotomy should be prepared at any time to maintain the airway patency. For example, patients with moderate-to-severe laryngeal obstruction and difficulty in opening mouth should consider tracheotomy. However, tracheotomy is an operation after all, and it will aggravate neck trauma, so it still needs to be cautious. In this group of cases, there are 2 cases of tracheal intubation, extubation within one week, close observation to avoid tracheotomy, and from these 5 patients, tracheotomy patients treated in ICU longer than tracheal intubation. But some studies think that, in DNSI, tracheotomy may decrease the need for ICU care and decrease complications related to longer intubation periods.37 Some studies suggest that the precise location of the infection may significantly influence the selection of airway management strategies.38 Therefore, for severe DNSI, the choice of tracheal intubation or tracheotomy needs to be individually evaluated according to the disease and systemic condition.
Although there is no uniform standard for the use of antibiotics, antibiotics are used empirically in the early stages of treatment, and then sensitive antibiotics are selected based on bacterial culture.39 Monitoring of vital signs and attention should be paid to the treatment of patients with underlying diseases. Patients with severe DNSI often have diabetes, should control blood sugar, and correct ketoacidosis. To strengthen systemic nutrition support, those who have difficulty opening their mouth or cannot eat due to intubation, need to nasally feed a high-protein, high-vitamin and low-fat diet, regularly review electrolytes, liver and kidney function, etc., pay attention to liver and kidney function damage and other complications caused by drugs and diseases themselves, pay attention to water and electrolyte balance and correct it in time.
In recent years, procalcitonin and neutrophil index have been used as markers of suppurative inflammation,40,41 which have important reference value for diagnosis, treatment and follow-up. Although these 5 patients were eventually recovered and discharged from hospital, unfortunately, the 5 patients were not followed up on these two indicators because they were cases from 2011 to 2020.
Conclusion
Severe DNSIs often occur in patients with low immunity such as diabetes. Infection involved multiple spaces in the neck and caused mediastinal infection and other complications are classified as severeI DNSI. The “pneumatosis” of CT is the imaging feature of severe DNSI. Based on the scope of the patient’s neck abscess, incisions (one or more incisions) in different locations were selected promptly for incision and drainage, correct evaluation of the disease, choose tracheal intubation or tracheotomy to maintain airway opening, combine with the results of bacteriological culture to select sensitive antibiotics, and pay attention to the treatment of comorbidities.
Ethics and Consent Statements
All patients provided written informed consent for the case details and images to be published. Since this study was retrospective and non-interventionist, no Ethics committee approval was sought. No institutional approval was required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Clinical Research Program of National Key R&D Program of China (2022YFC2504100), Shanghai Municipal Health Commission (No.202140293),Clinical Research Project of Tongji Hospital of Tongji University (No. ITJ(ZD)2207), Clinical Research Plan of SHDC (No. SHDC2020CR4090), National Science Foundation of Shanghai (No. 23ZR1458000), Shanghai General Hospital Integrated Traditional Chinese and Western Medicine (No. ZHYY-ZXYJHZX-202118).
Disclosure
The authors report no conflicts of interest in this work. This paper is available on Research Square as a preprint https://www.researchsquare.com/article/rs-597200/v1.
References
1. Priyamvada S, Motwani G. A study on deep neck space infections. Indian J Otolaryngol Head Neck Surg. 2019;71(Suppl 1):912–917. doi:10.1007/s12070-019-01583-4
2. Nwashindi A. Analysis of facial and deep neck space infections in patients with comorbidities. Int J Health Allied Sci. 2019;8:48–52. doi:10.4103/ijhas.IJHAS_40_17
3. Bakir S, Tanriverdi MH, Gün R, et al. Deep neck space infections: a retrospective review of 173 cases. Am J Otolaryngol. 2012;33(1):56–63. doi:10.1016/j.amjoto.2011.01.003
4. Boscolo-Rizzo P, Stellin M, Muzzi E, et al. Deep neck infections: a study of 365 cases highlighting recommendations for management and treatment. Eur Arch Otorhinolaryngol. 2012;269(4):1241–1249. doi:10.1007/s00405-011-1761-1
5. Staffieri C, Fasanaro E, Favaretto N, et al. Multivariate approach to investigating prognostic factors in deep neck infections. Eur Arch Otorhinolaryngol. 2014;271(7):2061–2067. doi:10.1007/s00405-014-2926-5
6. Adoviča A, Veidere L, Ronis M, Sumeraga G. Deep neck infections: review of 263 cases. Otolaryngol Pol. 2017;71(5):37–42. doi:10.5604/01.3001.0010.5315
7. Seppänen L, Rautemaa R, Lindqvist C, Lauhio A. Changing clinical features of odontogenic maxillofacial infections. Clin Oral Investig. 2010;14(4):459–465. doi:10.1007/s00784-009-0281-5
8. Yankov YG, Stoev LL. Demographic distribution, etiological bacterial spectrum and antibacterial treatment of patients with odontogenic abscesses and phlegmons of the head and neck. J IMAB. 2023;29(4):5276–5281. doi:10.5272/jimab.2023294.5276
9. Yankov YG, Stoev LL. Demographic distribution and etiological bacterial spectrum of patients with non- odontogenic abscesses and phlegmons of the head and neck. Actamicrobio. 2023;39(4):475–478. doi:10.59393/amb23390416
10. Yankov YG. The etiological bacterial spectrum of neck abscesses of lymph node origin - gram-positive and gram-negative bacteria. Cureus. 2023;15(10):e46940. doi:10.7759/cureus.46940
11. Yankov YG, Mechkarova ID. Etiological spectrum of odontogenic and non-odontogenic abscesses in oral and maxillofacial surgery. Scripta Scientifica Medicinae Dentalis. 2023;9:68–74. doi:10.14748/ssmd.v9i1.9130
12. Kauffmann P, Cordesmeyer R, Tröltzsch M, Sömmer C, Laskawi R. Deep neck infections: a single-center analysis of 63 cases. Med Oral Patol Oral Cir Bucal. 2017;22(5):e536–e541. doi:10.4317/medoral.21799
13. Huang TT, Liu TC, Chen PR, Tseng FY, Yeh TH, Chen YS. Deep neck infection: analysis of 185 cases. Head Neck. 2004;26(10):854–860. doi:10.1002/hed.20014
14. Hyun SY, Oh HK, Ryu JY, Kim JJ, Cho JY, Kim HM. Closed suction drainage for deep neck infections. J Craniomaxillofac Surg. 2014;42(6):751–756. doi:10.1016/j.jcms.2013.11.006
15. Dalla Torre D, Burtscher D, Höfer D, Kloss FR. Odontogenic deep neck space infection as life-threatening condition in pregnancy. Aust Dent J. 2014;59(3):375–378. doi:10.1111/adj.12189
16. Raffaldi I, Le Serre D, Garazzino S, et al. Diagnosis and management of deep neck infections in children: the experience of an Italian paediatric centre. J Infect Chemother. 2015;21(2):110–113. doi:10.1016/j.jiac.2014.10.011
17. Yankov YG, Mechkarova ID. Microbiological spectrum, clinic and treatment of patients with phlegmons of the floor of the mouth. Int J Med Sci Clin Invent. 2023;10(5):6704–6710. doi:10.18535/ijmsci/v10i5.02
18. Velhonoja J, Lääveri M, Soukka T, Irjala H, Kinnunen I. Deep neck space infections: an upward trend and changing characteristics. Eur Arch Otorhinolaryngol. 2020;277(3):863–872. doi:10.1007/s00405-019-05742-9
19. Umeda M, Minamikawa T, Komatsubara H, Shibuya Y, Yokoo S, Komori T. Necrotizing fasciitis caused by dental infection: a retrospective analysis of 9 cases and a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95(3):283–290. doi:10.1067/moe.2003.85
20. Hidaka H, Yamaguchi T, Hasegawa J, et al. Clinical and bacteriological influence of diabetes mellitus on deep neck infection: systematic review and meta-analysis. Head Neck. 2015;37(10):1536–1546. doi:10.1002/hed.23776
21. Sharma K, Das D, Joshi M, Barman D, Sarma AJ. Deep neck space infections-a study in diabetic population in a tertiary care centre. Indian J Otolaryngol Head Neck Surg. 2018;70(1):22–27. doi:10.1007/s12070-017-1196-0
22. O’Brien KJ, Snapp KR, Dugan AJ, Westgate PM, Gupta N. Risk factors affecting length of stay in patients with deep neck space infection. Laryngoscope. 2020;130(9):2133–2137. doi:10.1002/lary.28367
23. Juncar M, Popa AR, Baciuţ MF, et al. Evolution assessment of head and neck infections in diabetic patients--a case control study. J Craniomaxillofac Surg. 2014;42(5):498–502. doi:10.1016/j.jcms.2013.06.009
24. Pongcharoen S, Chansantor W, Supalap K, Jienmongkol P, Niumsup PR. Impaired interleukin-1beta expression by monocytes stimulated with Staphylococcus aureus in diabetes. Southeast Asian J Trop Med Public Health. 2011;42(5):1197–1203.
25. Srivanitchapoom C, Sittitrai P, Pattarasakulchai T, Tananuvat R. Deep neck infection in Northern Thailand. Eur Arch Otorhinolaryngol. 2012;269(1):241–246. doi:10.1007/s00405-011-1576-0
26. Maharaj S, Ahmed S, Pillay P. Deep neck space infections: a case series and review of the literature. Clin Med Insights Ear Nose Throat. 2019;12:1179550619871274. doi:10.1177/1179550619871274
27. Wang LF, Kuo WR, Tsai SM, Huang KJ. Characterizations of life-threatening deep cervical space infections: a review of one hundred ninety-six cases. Am J Otolaryngol. 2003;24(2):111–117. doi:10.1053/ajot.2003.31
28. Favaretto N, Fasanaro E, Staffieri A, et al. Deep neck infections originating from the major salivary glands. Am J Otolaryngol. 2015;36(4):559–564. doi:10.1016/j.amjoto.2015.01.003
29. Yankov YG. Etiological bacterial spectrum of patients with odontogenic and non-odontogenic abscesses and phlegmons in the maxillofacial area. J IMAB. 2023;29(2):4958–4962. doi:10.5272/jimab.2023292.4958
30. Al-Qamachi LH, Aga H, McMahon J, Leanord A, Hammersley N. Microbiology of odontogenic infections in deep neck spaces: a retrospective study. Br J Oral Maxillofac Surg. 2010;48(1):37–39. doi:10.1016/j.bjoms.2008.12.007
31. Farmahan S, Tuopar D, Ameerally PJ, Kotecha R, Sisodia B. Microbiological examination and antibiotic sensitivity of infections in the head and neck. Has anything changed? Br J Oral Maxillofac Surg. 2014;52(7):632–635. doi:10.1016/j.bjoms.2014.02.028
32. Valerio L, Riva N. Head, neck, and abdominopelvic septic thrombophlebitis: current evidence and challenges in diagnosis and treatment. Hamostaseologie. 2020;40(3):301–310. doi:10.1055/a-1177-5127
33. Gonzalez-Beicos A, Nunez D. Imaging of acute head and neck infections. Radiol Clin North Am. 2012;50(1):73–83. doi:10.1016/j.rcl.2011.08.004
34. Adil E, Tarshish Y, Roberson D, Jang J, Licameli G, Kenna M. The public health impact of pediatric deep neck space infections. Otolaryngol Head Neck Surg. 2015;153(6):1036–1041. doi:10.1177/0194599815606412
35. Hoffmann C, Pierrot S, Contencin P, Morisseau-Durand MP, Manach Y, Couloigner V. Retropharyngeal infections in children. Treatment strategies and outcomes. Int J Pediatr Otorhinolaryngol. 2011;75(9):1099–1103. doi:10.1016/j.ijporl.2011.05.024
36. Karkos PD, Leong SC, Beer H, Apostolidou MT, Panarese A. Challenging airways in deep neck space infections. Am J Otolaryngol. 2007;28(6):415–418. doi:10.1016/j.amjoto.2006.10.012
37. Tapiovaara L, Bäck L, Aro K. Comparison of intubation and tracheotomy in patients with deep neck infection. Eur Arch Otorhinolaryngol. 2017;274(10):3767–3772. doi:10.1007/s00405-017-4694-5
38. Cho SY, Woo JH, Kim YJ, et al. Airway management in patients with deep neck infections: a retrospective analysis [published correction appears in Medicine (Baltimore). 2016 Oct 21;95(42):e36c2. doi: 10.1097/01.md.0000504793.45336.c2]. Medicine (Baltimore). 2016;95(27):e4125. doi:10.1097/MD.0000000000004125
39. Yankov YG, Dimanov S, Nikolaev NI, Stoev L, Yotsova RV, Stoeva M. Etiology and demographic distribution of odontogenic abscesses in the maxillofacial area in patients over 18 years of age: a five-year retrospective study. Cureus. 2024;16(4):e59334. doi:10.7759/cureus.59334
40. Yankov YG, Bocheva Y. Comparative characterization of procalcitonin (sensitivity, specificity, predictability, and cut-off reference values) as a marker of inflammation in odontogenic abscesses of the head and neck in the female population. Cureus. 2023;15(11):e48207. doi:10.7759/cureus.48207
41. Yankov YG. Delta neutrophil index as a new marker of purulent inflammation in men with non-odontogenic abscesses of the neck. Cureus. 2023;15(10):e47165. doi:10.7759/cureus.47165
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.