Back to Journals » Infection and Drug Resistance » Volume 12
Clinical features and outcomes of tetanus: a retrospective study
Authors Fan Z, Zhao Y, Wang S, Zhang F, Zhuang C
Received 9 February 2019
Accepted for publication 29 March 2019
Published 16 May 2019 Volume 2019:12 Pages 1289—1293
DOI https://doi.org/10.2147/IDR.S204650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Zhe Fan,1,2,* Yue Zhao,3,* Shuang Wang,3 Feng Zhang,4 Chengjun Zhuang5
1Department of General Surgery, The Third People’s Hospital of Dalian, Dalian Medical University, Dalian, People’s Republic of China; 2Department of General Surgery, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, People’s Republic of China; 3Graduate School, Dalian Medical University, Dalian, People’s Republic of China; 4Department of General Surgery, The Second Affiliated Hospital of Dalian Medical University, Dalian, People’s Republic of China; 5Department of Critical Care Medicine, The Second Affiliated Hospital of Dalian Medical University, Dalian, People’s Republic of China
*These authors contributed equally to this work
Background: Tetanus is a serious disease resulting in muscle spasm, and even death.
Methods: A retrospective, single-center study was conducted by analyzing demographic and clinical parameters.
Results: The study included 12 males (70.6%) and 5 females (29.4%). The mean age of the patients was 56.71±9.05 years. Patient occupations included farming (47.0%), retired (23.5), homebound (23.5), and workers (6.0%). The causes of patient injuries were as follows: metal injury (52.9%), deep injury (29.4%), electrical injury (5.9%), maxillofacial region and knee injury (5.9%), and skin ulceration (5.9%). The disease duration ranged from 3 to 36 days, and the mean incubation period was 12.65±10.17 days. Four patients had co-morbidities. The infected patients were given tetanus antitoxin (TAT) and antibiotics treatment. One patient was given continuous renal replacement therapy (CRRT) and only one patient died.
Conclusions: In our department, although tetanus is a serious disease, with effective treatment, patients have reasonable cure and low death rates.
Keywords: tetanus, intensive care unit, retrospective study
Introduction
Tetanus is an acute infectious disease caused by the bacterium, Clostridium tetani (C. tetani), as defined by the WHO,1 which generates a neurologic toxin2 Because of the high mortality rate, tetanus is still a significant issue worldwide, especially in developing counties.3,4 In developed countries, tetanus has a low incidence; specifically, there were 43 cases per year between 1998 and 2000.5 In addition to the disease process, a lack of experience in diagnosing tetanus contributes to the high mortality rate6 Tetanus often leads to death, with a reported 213,000–293,000 deaths worldwide.7 The incidence of tetanus is about 1 case per 10,000,000 in the US.8 There are no guidelines with respect to tetanus immunization for adults in China; however, in 2012, China was validated to have eliminated maternal and neonatal tetanus.9 The tetanus bacillus generates tetanospasmin and tetanolysin; the former toxin causes local inflammation by acting on gangliosides within local nerve terminals, resulting in the clinical syndrome.5,10 Muscle spasm is the main characteristic of tetanus; trismus affects 95.7%, neck stiffness affects 89.3%, body spasms/stiffness affect 73%, and dysphagia affects 38.9% of the patients.11 The present study investigated the demographic data, prognosis, and mortality of patients with tetanus.
Tetanus is a preventable infection that results in severe problems worldwide, especially in developing countries.12 It is believed that poor wound care and lack of immunization awareness leads to a high prevalence of tetanus in developing countries.13 The incidence of tetanus is low in high-income countries, which has been attributed to a robust immunization program.14 In China, the government has offered diphtheria–pertussis–tetanus vaccines to children since 1978. Therefore, tetanus-infected people are >33 years of age. In the present study, the youngest tetanus-infected patient was 46 years of age as a result of the aforementioned government program. It has been reported that there are 35–70 people infected with tetanus each year, and most of the patients are >65 years of age in the USA, which is thought to represent waning immunity.15
Patients and methods
We retrospectively analyzed 17 patients infected with tetanus from the intensive care unit (ICU) of the Second Affiliated Hospital of Dalian Medical University. The diagnosis satisfied the World Health Organization (WHO) definition for tetanus. Consent was obtained from all of the patients. The research was approved by the Ethics Committee of the Second Affiliated Hospital of Dalian Medical University.
The patient records were collected from January 2011 to December 2017. When admitted to the hospital, because of different levels of local injury, all patients received antibiotic treatment; because of muscle spasm, all patients were administered TAT. The following data were collected: age, sex, occupation, etiology, incubation period, comorbidities, onset of symptoms, degree of dyspnea, Sequential Organ Failure Assessment (SOFA), whether or not mechanical ventilation was used, dosage of tetanus immunoglobulin, continuous renal replacement therapy (CRRT), antibiotic; length of hospital stay, pneumonia (defined by the findings on chest computed tomography), and death. Patient consent was obtained by written informed consent, and this study was conducted in accordance with the Declaration of Helsinki.
Results
The study included 12 males (70.6%) and 5 females (29.4%), for a male-to-female ratio of 2.4:1. The mean age of the patients was 56.71±9.05 years (range, 46–70 years) and 76.5% of the patients were >50 years of age. The patients’ occupations included farming (47.0%), retired (23.5), homebound (23.5), and worker (6.0%). The causes of patient injuries were as follows: metal injury (52.9%), deep injury (29.4%), electric injury (5.9%), maxillofacial region and knee injury (5.9%), and skin ulcer (5.9%). None of the patients received DTP, Td, Tdp, or Tdap vaccinations (Table 1).
 | Table 1 Demographic characteristics of the patients |
The duration of disease ranged from 3 to 36 days, and the mean incubation period was 12.65±10.17 days. Four patients had comorbidities. When the patients presented to the hospital, onset of symptoms differed: trismus was the most common presentation accounting for 70.6%, followed by dysarthria (35.3%), and muscle spasm (17.6%). There were varying degrees of dyspnea based on the oxygenation index (PaO2/FiO2), reflecting the severity of the disease, as follows: severe degrees of dyspnea (PaO2/FiO2 ≤100 mmHg; 11.8%), moderate degrees of dyspnea (100 mmHg < PaO2/FiO2 ≤200 mmHg; 17.6%), mild degrees of dyspnea (200 mmHg < PaO2/FiO2 ≤300 mmHg; 58.8%), and no dyspnea (11.8%). Patients with severe and moderate dyspnea were treated in the ICU; the other patients were observed in the general ward with supervision by the ICU staff as needed.
The mean SOFA grade was 5.29±4.37 (range, 2–19; Table 2).
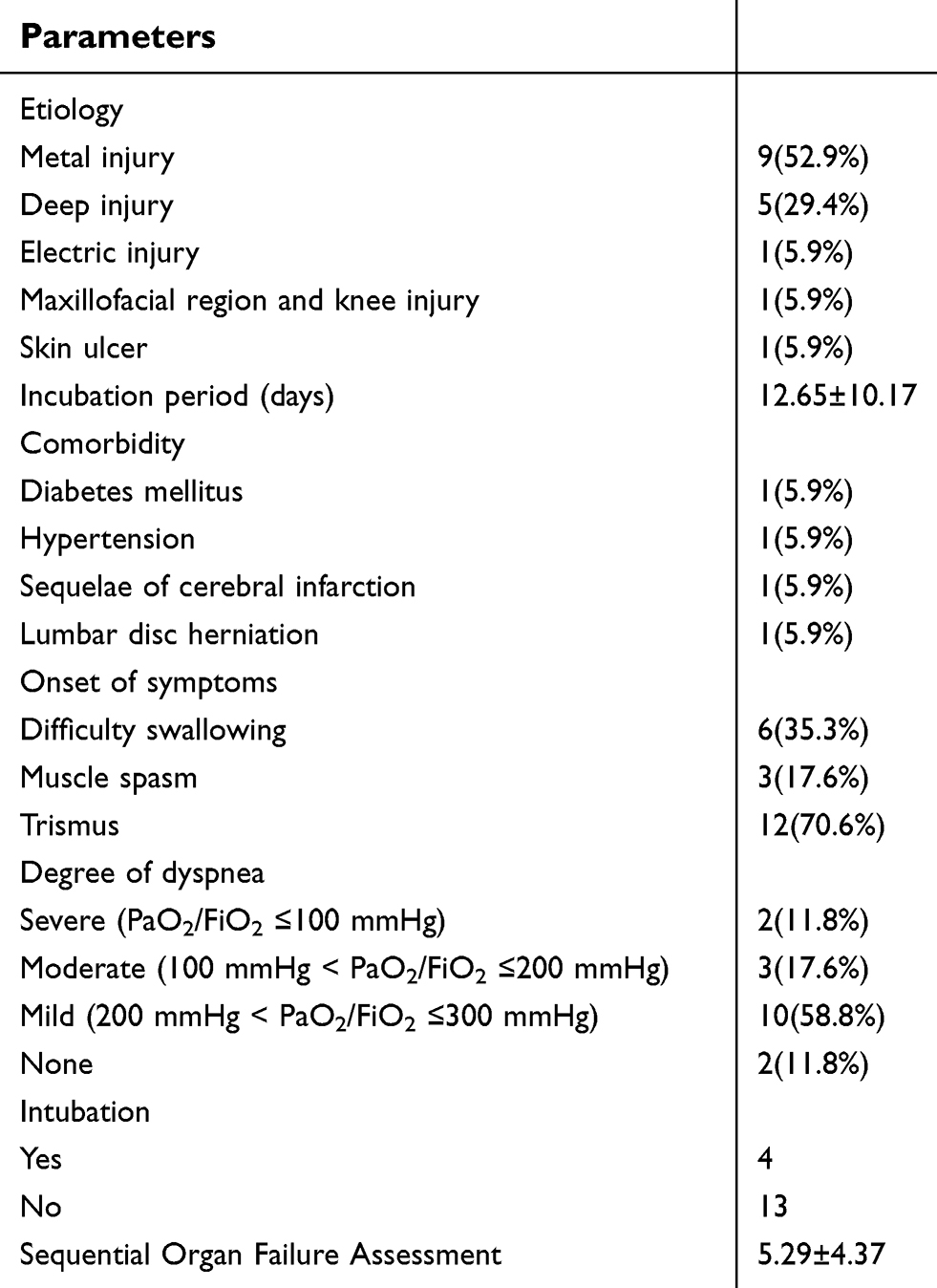 | Table 2 Disease characteristics of the patients |
Upon admission to the hospital, positive treatment was initiated, including open wound, tetanus antitoxin (TAT), antibiotics, improving breathing, and continuous renal replacement therapy (CRRT), if necessary. The patients were given different O2 treatments based on the different degrees of dyspnea, as follows: intubation for severe dyspnea (2 patients); nasal cannula for moderate dyspnea (3 patients [2 of the 3 patients were intubated using transient nasal intermittent positive pressure ventilation {NIPPV}]); and nasal cannula for mild dyspnea (10 patients). All infected patients were given TAT treatment, and the mean dosages were 11,294.12±8970.54 IU/day (range, 1,500–30,000 IU). The patients were administered penicillin or piperacillin-tazobactam empirically based on the presentation of the injury as inpatients because it was more likely for the injury to be associated with coccal infections. Secretion of the wound was collected for guiding and administrating the administration of antibiotics. When local infection was controlled, the antibiotics were terminated. Sputum cultures were collected routinely from all of the patients, and the results were as follows: normal throat bacteria (4), none (11), and C. baumanii (1). The patient with a C. baumanii infection was administered tigecycline for treatment. Antibiotics were administrated for remedying the infection; piperacillin-tazobactam and penicillin were both effective. Because of respiratory muscle fatigue, there were four patients who were placed on mechanical ventilation. Because of multiple organ dysfunction syndromes, one patient was given CRRT. Pneumonia was the main complication of tetanus-infected patients and was diagnosed based on clinical symptoms and chest computed tomography (CT). In the present study, there were four patients with pneumonia; one patient had a C. baumanii infection and was treated with tigecycline, while the antibiotics were not changed in the other three patients (treated with piperacillin-tazobactam according to the sputum cultures). After aggressive treatment, only one patient died (Table 3).
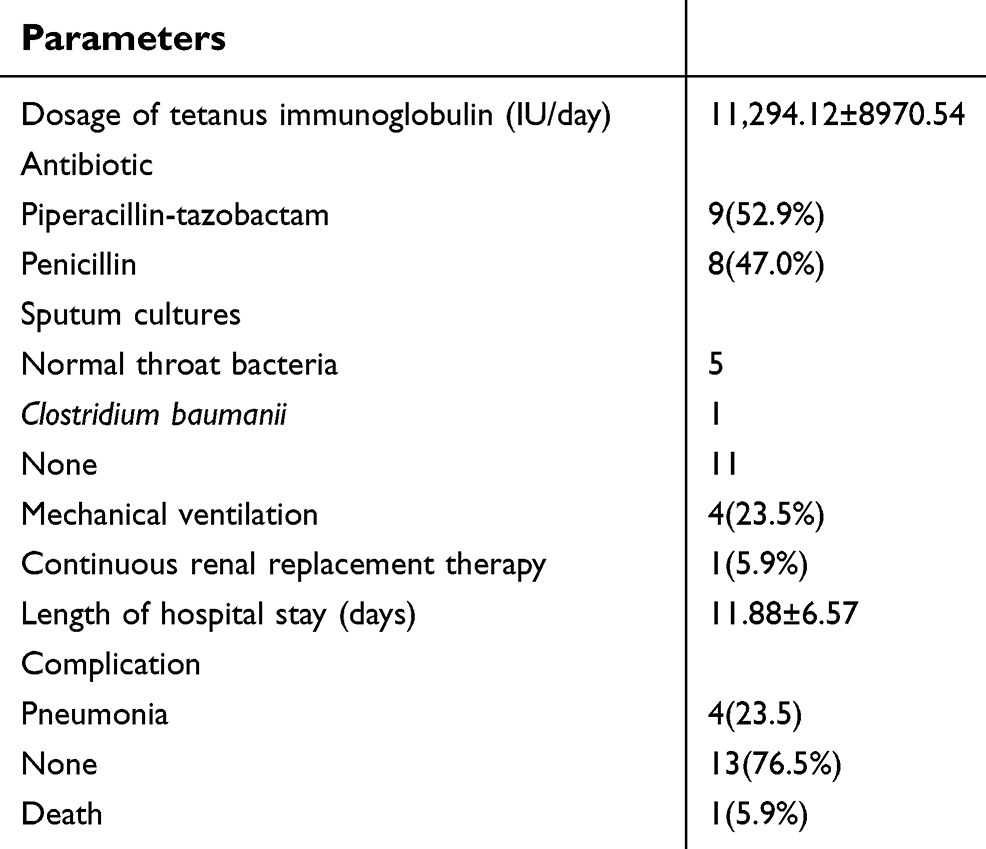 | Table 3 Treatment characteristics of the patients |
Discussion
In the present research, the percentage of males (70.6%) was greater than the percentage of females (29.4%), which differs from other research: Fawibe20 reported 85.7% males and 14.3% females and Chukwubike and God’spower16 reported 58.1% males and 41.9% females in their studies. Males often do outdoor jobs, such as farming or skilled jobs, that have an increased probability of injuries. In our study, the patients had metal and deep injuries when they did heavy work, while females often did light work with fewer injuries. Females may have a low incidence of tetanus because of immunization during pregnancy.17 Patient occupation is an important risk factor for tetanus. Farmers have a tetanus incidence of 47.0% in the present tetanus cases, while the retired and homebound have an incidence of 23.5% in the present tetanus cases. Chukwubike et al16 reported that 46.5% of the patients with tetanus were students and civil servants, while artisans and commercial motorcyclists accounted for 25.6% of the infections and farmers represented 4.7%.16 Other studies have shown the dominance of farming among tetanus-infected patients,18 which is in agreement with our study. The cause may be that the elderly have less medical knowledge and less health consciousness. In the USA, the Centers for Disease Control and Prevention advise people to receive a dose of tetanus vaccine every 10 years to remain immunized.19
The pathogenesis of tetanus consists of several cases in which there is contamination of the wound by tetanus. It is well known that tetanus originates from puncture wounds, abrasions, burns, injections, surgery, compound fractures, animal bites or scratches, gastrointestinal infections, abortion, and childbirth.5 In the present research, metal and deep injuries separately account for 52.9% and 29.4% of the cases, respectively. Tetanus is a gram-positive bacillus and obligates anaerobe. Rusted metal is full of anaerobions, therefore metal injuries have a high infection rate. The disease has characteristic regions similar to snake bites or scorpion stings in Nigeria.20
The incubation period ranged from 3 to 36 days with a mean period of 12.65 days, which is similar to the results by Zielinski and Rudowska21 Because of a lack of health consciousness, the entire patient cohort in our study had not been previously vaccinated. The incubation period was not so short that patients did not have time to accept immunotherapy. There were four patients with comorbidities. Rogers and Frykberg22 reported that diabetic foot could result in tetanus because immunopathy, vasculopathy, and ulceration increase the risk. Therefore, diabetes mellitus may be a relevant factor with tetanus. Hypertension, sequelae of cerebral infarction, and lumbar disc herniation are not associated with tetanus.
Trismus was the more frequent initial symptom, accounting for 70.6% of the patients because the muscles of the jaw with shorter axonal pathways facilitate the toxin effect on inhibitory neurons.5,10 The initial presentation of tetanus lockjaw includes stiff neck, dysarthria, and abdominal muscle stiffness, which are usually affected by noise and light. Other symptoms follow, such as fever, sweating, and high blood pressure. Muscle stiffness also extends from the jaw to the limb muscles.21 There were different degrees of dyspnea, but mild symptoms occurred in the majority of patients. The SOFA score reflected the severity of ICU patients. Vora et al23 concluded that a mean SOFA score <2.15 was safer than for patients who expired (SOFA score of 2.89).23 In the present study, the mean SOFA was 5.29, which was higher than reported by Vora et al.23 Patient death was associated with a high SOFA score of 19. Treatment for tetanus includes the following: stop further toxin release, neutralize toxins, and reduce toxicity.24 In our study, the infected patients underwent debridement to clean the wound and were administered antibiotics to reduce inflammation; TAT was used to neutralize toxins; mechanical ventilation supported respiratory failure. Formal research suggests that penicillin and metronidazole are two effective antibiotics.10,24 Our experience showed that piperacillin-tazobactam and penicillin were effective as well.
Neutralizing toxins can be achieved with equine/human tetanus immunoglobulin by passive immunization. The suggested dose of adults is 3,000–6,000 IU17 In our study, the minimal dose of tetanus immunoglobulin was 1,500 IU, and the maximal dose was 30,000 IU. Most patients enrolled in the study recovered.
When the respiratory muscles are affected by tetanus toxin, mechanical ventilation must be performed. Among the infected patients on mechanical ventilation, there were three affected by pneumonia and one developed renal failure, who underwent CRRT treatment. Loan et al25 reported >90% of the patients with severe tetanus had pneumonia. Nobrega et al26 concluded that 84.8% of the patients had pneumonia. The incidence of pneumonia in our study was low. Spasm was the main symptom, often lasting 1–2 weeks, while stiffness persisted a long time.10 One report advised that patients required 11–30 days of treatment in the hospital.27 Our study indicated a mean of 11.88 days of treatment, which was less than the previous reports. A report found that 45% of the deaths occurred in south Asia.28 Only one patient (5.9%) died of multiple organ dysfunction syndrome (MODS) in our study; however, because of the small sample size, a large sample, multi-center study should be conducted.
Although the number of tetanus infections from the single center was small, there was an absence of vaccines. There are two recommendations for settling the present issue. First, it is vitally important for the general population and health staff to realize the necessity of tetanus vaccines. Second, there should be more effort supported by the government regarding an adult vaccine policy.
Conclusion
Tetanus is a critical disease and often has a high mortality rate. When injury occurs, it is important to acquire immunity. In a retrospective single-center study, most patients were cured by stopping further toxin release, neutralizing toxins, and reducing toxicity. The mortality of patients infected by tetanus was low. A vaccination policy and program should be implemented by our government.
Acknowledgments
We thank International Science Editing (
Disclosure
The authors have no conflicts of interest in this work.
References
1.
2. Mahieu R, Reydel T, Maamar A, et al. Admission of tetanus patients to the ICU: a retrospective multicentre study. Ann Intensive Care. 2017;7(1):112.
3. Oladiran I, Meier DE, Ojelade AA, OlaOlorun DA, Adeniran A, Tarpley JL. Tetanus: continuing problem in the developing world. World J Surg. 2002;26(10):1282–1285. doi:10.1007/s00268-002-6497-z
4. Chalya PL, Mabula JB, Dass RM, Mbelenge N, Mshana SE, Gilyoma JM. Ten-year experiences with Tetanus at a Tertiary hospital in Northwestern Tanzania: a retrospective review of 102 cases. World J Emerg Surg. 2011;6:20. doi:10.1186/1749-7922-6-20
5. Poudel P, Budhathoki S, Manandhar S. Tetanus. Kathmandu Univ Med J. 2009;7(27):315–322.
6. Sun C, Zhao H, Lu Y, et al. Prognostic factors for generalized tetanus in adults: a retrospective study in a Chinese hospital. Am J Emerg Med. 2018;37(2) 254–259.
7. Narang M, Khurana A, Gomber S, Choudhary N. Epidemiological trends of tetanus from East Delhi, India: a hospital-based study. J Infect Public Health. 2014;7(2):121–124. doi:10.1016/j.jiph.2013.07.006
8. Liang JL, Tejpratap T, Pedro M, et al. Prevention of pertussis, tetanus, and diphtheria with vaccines in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2018;67(2):1–44.
9. Thwaites CL, Beeching NJ, Newton CR. Maternal and neonatal tetanus. Lancet. 2015;385(9965):362–370. doi:10.1016/S0140-6736(14)60236-1
10. Cook TM, Protheroe RT, Handel JM. Tetanus: a review of the literature. Br J Anaesth. 2001;87(3):477–487.
11. Melkert D, Kahema L, Melkert P. Reduction of mortality due to tetanus by immunisation and proper wound management of the patients in Sengerema Designated District Hospital, Tanzania. Trop Doct. 2014;44(3):163–165. doi:10.1177/0049475514521804
12. Naseem F, Hussain A, Arif F. Frequency of acute kidney injury in tetanus patients of paedriatic intensive care unit: a public hospital experience. Pak J Med Sci. 2018;34(2):363–367. doi:10.12669/pjms.342.14254
13. Arogundade FA, Bello IS, Kuteyi EA, Akinsola A. Patterns of presentation and mortality in tetanus: a 10-year retrospective review. Niger Postgrad Med J. 2004;11(1):58–63.
14. Aziz R, Colombe S, Mwakisambwe G, et al. Pre-post effects of a tetanus care protocol implementation in a sub-Saharan African intensive care unit. PLoS Negl Trop Dis. 2018;12(8):e0006667. doi:10.1371/journal.pntd.0006667
15. Sahan S, Demirbilek Y, Sonmez C, Temel F, Sencan I. The research of the tetanus seropositivity levels in registered family physicians in Ankara province, Turkey, 2017. Jpn J Infect Dis. 2019; 72(1):14–18.
16. Chukwubike OA, God’spower AE. A 10-year review of outcome of management of tetanus in adults at a Nigerian tertiary hospital. Ann Afr Med. 2009;8(3):168–172. doi:10.4103/1596-3519.57239
17. Andersen A, Bjerregaard-Andersen M, Rodrigues A, Umbasse P, Fisker AB. Sex-differential effects of diphtheria-tetanus-pertussis vaccine for the outcome of paediatric admissions? A hospital based observational study from Guinea-Bissau. Vaccine. 2017;35(50):7018–7025. doi:10.1016/j.vaccine.2017.10.047
18. Ojini FI, Danesi MA. Mortality of tetanus at the Lagos University Teaching Hospital, Nigeria. Trop Doct. 2005;35(3):178–181. doi:10.1258/0049475054620806
19. Available from:
20. Fawibe AE. The pattern and outcome of adult tetanus at a sub-urban tertiary hospital in Nigeria. J Coll Physicians Surg Pak. 2010;20(1):68–70.
21. Zielinski A, Rudowska J. Tetanus in Poland in 2015. Przegl Epidemiol. 2017;71(3):373–378.
22. Rogers LC, Frykberg RG. Tetanus prophylaxis for diabetic foot ulcers. Clin Podiatr Med Surg. 2006;23(4):
23. Vora CS, Karnik ND, Gupta V, Nadkar MY, Shetye JV. Clinical profile of patients requiring prolonged mechanical ventilation and their outcome in a tertiary care medical ICU. J Assoc Physicians India. 2015;63(10):14–19.
24. Bhatia R, Prabhakar S, Grover VK. Tetanus. Neurology India. 2002;50(4):398–407.
25. Loan HT, Parry J, Nga NT, et al. Semi-recumbent body position fails to prevent healthcare-associated pneumonia in Vietnamese patients with severe tetanus. Trans R Soc Trop Med Hyg. 2012;106(2):90–97. doi:10.1016/j.trstmh.2011.10.010
26. Nobrega MV, Reis RC, Aguiar IC, et al. Patients with severe accidental tetanus admitted to an intensive care unit in Northeastern Brazil: clinical-epidemiological profile and risk factors for mortality. Braz J Infect Dis. 2016;20(5):457–461. doi:10.1016/j.bjid.2016.06.007
27. Lau LG, Kong KO, Chew PH. A ten-year retrospective study of tetanus at a general hospital in Malaysia. Singapore Med J. 2001;42(8):346–350.
28. Kyu HH, Mumford JE, Stanaway JD, et al. Mortality from tetanus between 1990 and 2015: findings from the global burden of disease study 2015. BMC Public Health. 2017;17(1):179.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.