Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 17
Clinical Experience and Pitfalls in Using Glycyrrhizic Acid for Treating Anogenital Warts in an HIV-Infected Patient in Indonesia: A Case Report
Authors Arrum RK ![]() , Maharani RH
, Maharani RH ![]() , Sutedja EK
, Sutedja EK ![]() , Tsaqilah L
, Tsaqilah L ![]() , Gunawan H
, Gunawan H ![]() , Achdiat PA
, Achdiat PA ![]()
Received 4 August 2025
Accepted for publication 27 November 2025
Published 3 December 2025 Volume 2025:17 Pages 399—406
DOI https://doi.org/10.2147/HIV.S558240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Ravika Khaila Arrum, Retno Hesty Maharani, Eva Krishna Sutedja, Laila Tsaqilah, Hendra Gunawan, Pati Aji Achdiat
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia
Correspondence: Pati Aji Achdiat, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin General Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +6281322750101, Email [email protected]
Abstract: Anogenital warts (AGW) are a common manifestation of human papillomavirus (HPV) infection, primarily caused by strains 6 and 11. According to results, mucosal HPV is transmitted through sexual contact, with risk factors including immunodeficiency, such as Human Immunodeficiency Virus (HIV). Individuals with HIV experience a higher incidence of AGW due to impaired immune function that hinders HPV clearance. There is currently no specific antiviral therapy available for HPV, although several management options exist. However, some of these treatments may cause pain and discomfort. Glycyrrhizinic acid (GA) has demonstrated potential in managing HPV infection because of its antiviral properties and minimal side effects. Despite these promising results, GA is not yet recognized as a standard therapy for AGW. This case report describes the effectiveness of Glizigen® (topical GA) combined with Viusid® (oral GA) in managing genital warts in a 28-year-old homosexual male living with HIV. The patient, examined by a dermatologist at Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, presented with perianal warts that had developed over 3 months. According to the physical examination carried out, multiple flesh-colored papules were reported, while histopathological analysis showed koilocytes, and polymerase chain reaction (PCR) confirmed HPV types 6 and 11. The treatment process, carried out using topical and oral GA, was administered from August to October 2024. The improvement was reported only in smaller lesions, while larger ones persisted, leading to electrocautery scheduling. The limited response observed in this case might be influenced by the patient’s low CD4+ count, which potentially affects HPV clearance. Factors such as age, number of sexual partners, circumcision status, HPV type, and anatomical location of the lesions may also have played a role.
Keywords: antiviral, anogenital warts, glycyrrhizinic acid, HIV-positive
Introduction
Anogenital warts (AGW) are one of the most common manifestations of human papillomavirus (HPV) infection.1 HPV is non-enveloped virus, approximately 50 nm in size, with a circular double-stranded DNA genome.2 The most prevalent HPV types, 6 and 11, are responsible for more than 90% of genital lesions.3,4 HPV can be transmitted through various forms of sexual contact, including non-penetrative interactions. Several factors increase the risk of HPV infection, such as multiple sexual partners, early age at sexual debut, coexisting sexually transmitted infections (STIs), and immunosuppression, particularly in individuals with Human Immunodeficiency Virus (HIV) infection.4 While most HPV infections resolve spontaneously, underlying conditions such as immunocompromise can lead to persistent infections.5
Individuals who are HIV-positive are significantly more likely to develop AGW than those who are HIV-negative.6 HIV infection affects HPV at both molecular and cellular levels during various phases of the HPV cycle, including entry into target cells, replication, and evasion of the immune response. As HIV progresses, immune suppression increases the risk of infection, leading to higher viral loads, more frequent infections with multiple strains, reduced clearance rates, and a greater likelihood of persistence.7 According to de Pokomandy et al8 only 13% of HIV-positive men who were initially HPV-positive tested negative after 1860 days.
According to present reports, there are no effective antiviral treatments for HPV infection.9 According to the 2019 IUSTI-Europe guideline for the management of AGW, the primary goal of treatment is to remove visible lesions and alleviate associated symptoms. The recommended treatment options include patient-applied topical therapies such as imiquimod and podofilox, as well as provider-administered treatments such as cryotherapy, surgical excision, and application of trichloroacetic acid (TCA).10 The treatment modalities, such as electrocautery and imiquimod, were shown to be efficacious in treating AGW in individuals with HIV.11 However, these treatments have been associated with common side effects, including pain, itching, burning, erosion, and inflammation.9,10
Glycyrrhizinic acid (GA) is a novel therapeutic agent with anti-inflammatory, antiulcerative, and antiviral properties.3 This acid interacts with viral proteins, potentially inactivating extracellular virus particles and disrupting the virus structure. GA has shown promise in the treatment of HPV, as supported by evidence from several clinical studies.12 However, it is not currently included in the recommended guidelines for managing AGW.10 When compared to other topical agents, side effects such as burning, pain, and itching are less common,3 making GA a more user-friendly and non-invasive treatment option.13 Majority of published studies have utilized the same topical product or a combination of topical and oral products branded as Glizigen® (Catalysis S.L., Toledo, Spain; distributed by Sintesa Duta Sejahtera, Jakarta, Indonesia), which contains 0.06 mL GA in 30 mL of the vehicle. The oral form of Glizigen®, known in publications as Viusid®, is a nutritional supplement comprising 0.1 g GA in 100 mL of the vehicle. Therefore, the purpose of this case report is to evaluate the efficacy of Glizigen® in combination with Viusid® for treating AGW in an HIV-infected patient.
Case Illustration
A 28-year-old homosexual man came in with multiple painless, non-itchy, skin-colored papules in the perianal area. The lesions first appeared 3 months prior to the initial visit and had significantly increased in both number and size, and reported a history of promiscuity, with more than 10 sexual partners. The patient has been HIV-positive for 6 years and has been receiving HAART (zidovudine, lamivudine, and nevirapine) for the past 5 months, with a CD4 cell count of 192 cells/µL (normal range: 404–1612 cells/µL). Upon examination, vegetative lesions resembling cauliflower were reported, the largest measuring 1.5 × 1 × 0.1 cm (Figure 1a), and no other lesions or lymphadenopathy were found. Dermoscopy examination showed a finger-like pattern (Figure 2).
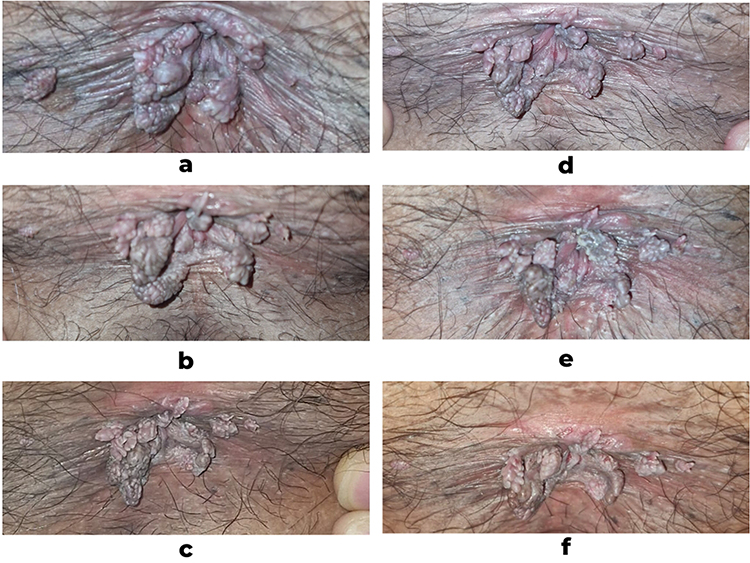 |
Figure 1 Clinical manifestation before treatment (a); second follow-up (b); third follow-up (c); fourth follow-up (d); fifth follow-up (e); and sixth follow-up (f). |
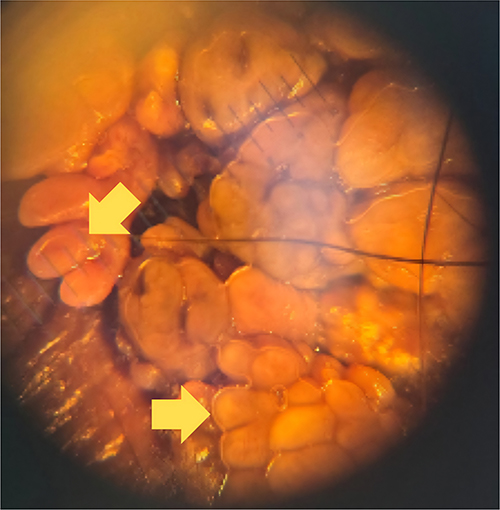 |
Figure 2 The dermoscopy examination revealed finger-like projections (yellow arrow). |
A shave biopsy was conducted, showing keratinized stratified squamous epithelium with features of hyperplasia, acanthosis, hyperkeratosis, and papillomatosis. Koilocytosis was observed in some nuclei, but there were no indications of a malignancy pattern (Figure 3). Polymerase chain reaction (PCR) testing identified HPV types 6 and 11. Based on the anamnesis, the physical examination, venereological assessment, dermoscopy, histological examination, and PCR testing, the patient was diagnosed with condylomata acuminata (CA).
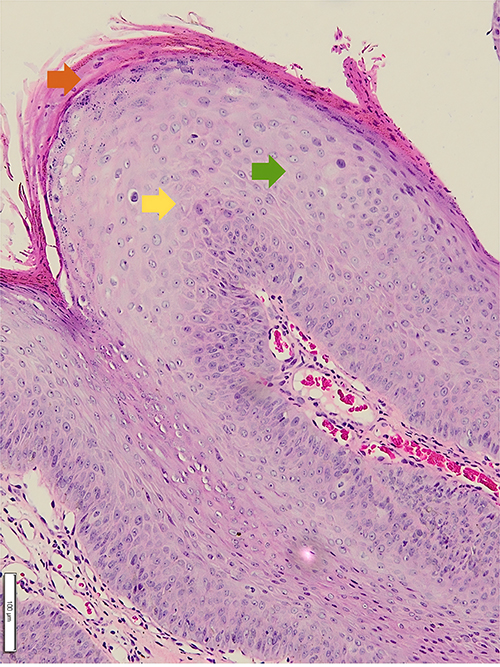 |
Figure 3 The histopathological characteristics of the lesions revealed keratinized stratified squamous epithelium with hyperplasia (Orange arrow), acanthosis (green arrow), and koilocytosis (yellow arrow). |
The patient requested a painless, home-based treatment. A recommendation of a combination of topical and oral GA, with the topical GA to be applied three times daily and a 10 mL oral dose taken every 8 hours. The treatment effectiveness was assessed by monitoring the size and number of warts at each follow-up visit. The patient showed good adherence to both topical and oral GA therapy in the 6-week treatment period. The patient applied Glizigen® spray twice daily to the affected perianal area and took Viusid® orally as prescribed, reporting no missed doses during follow-up visits. No significant adverse events were observed during treatment. The patient denied experiencing pain, burning, or irritation at the application site, and no systemic side effects were reported. However, after six weeks of therapy, there was an improvement in the smaller lesions, but no significant changes occurred in the larger lesions (Figure 1b–f). The patient was therefore scheduled for electrocautery to eliminate the visible skin lesions that were causing discomfort.
Discussion
HPV is part of the Papillomaviridae family, which is able to replicate in the stratified epithelia.14 There are already more than 200 distinct double-stranded DNA viruses known to exist.4,9 Out of these, 45 types specifically target the genital tract, while the remaining types are associated with cutaneous manifestations.4 HPV is classed as high-risk or low-risk based on its oncogenicity.9 The International Agency for Research on Cancer has identified 13 α-HPV as group 1 carcinogens, including types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 66, also known as “high-risk HPV” (HR-HPV). In contrast, types 6, 11, 40, 42, 43, 44, and 54 are classed as “low-risk HPV” (LR-HPV) since they are associated with benign diseases such as condylomas acuminata.2 Although HPV is most commonly transmitted through sexual contact, the virus has also been detected in infants’ oral cavities, breast milk, amniotic fluid, the placenta, and umbilical blood.15
The virus infects basal epithelial cells in the skin and mucous membranes.2,15 HPV genome consists of eight open reading frames (ORFs), including seven early (E) genes and two late (L) genes. The late genes encode the viral capsid proteins. Oncogenic proteins E5, E6, and E7, produced by HR-HPV types, can drive cell transformation and stimulate growth in the basal and parabasal layers.15 Upon entering basal epithelial cells, HPV disrupts cell cycle regulation through the actions of E6 and E7 proteins. E6 protein binds to p53, a crucial regulator of cell growth, leading to uncontrolled cell division and the accumulation of chromosomal mutations without proper DNA repair. Meanwhile, E7 protein targets p130, another cell-cycle regulator, which promotes increased cell growth and contributes to uncontrolled proliferation.5 HPV is currently one of the most prevalent sexually transmitted infections, often leading to the development of AGW. Infection rates are notably higher among men who have sex with men and individuals who are HIV-positive.15 In this case report, the patient was a man who was HIV-positive and identified as homosexual.
Most AGW are diagnosed clinically based on their distinct appearance and location.6 The four types of AGW are: condyloma acuminata, which have a cauliflower-like appearance; papular warts, which are flesh-colored and dome-shaped, typically 1–4 mm in diameter; keratotic warts, which feature a thick, crusty surface and may resemble common skin warts or seborrheic keratosis; and flat-topped papules, which are either macular or slightly raised.1 HPV prevalence in mucosal lesions is distributed as follows: 36.21% in the penile region, 25.68% in the anal region, 24.11% in the uterine cervical region, and 11.89% in the oral region.16 For atypical lesions suspected to be precancerous or cancerous, or when the diagnosis is uncertain, a pathological examination and HPV genotyping are recommended. Additionally, dermoscopy can assist in the diagnostic process.9 AGW dermoscopic patterns are finger-like, knob-like, or a mosaic pattern, with vascular structure. Histopathologically, HPV-infected cells are identified by the presence of atypical keratinocytes called “koilocytes,” which are enlarged cells with eccentric, pyknotic nuclei often surrounded by a perinuclear halo.17 In this case report, the patient presented with multiple perianal vegetative lesions resembling cauliflower. Histopathological results showed koilocytic changes, and PCR examination was positive for HPV types 6 and 11. Dermoscopy of the lesions showed finger-like projections.
Immunosuppression is a significant risk factor for HPV-related lesions.4 When compared to HIV-negative individuals, HIV positive individuals have a higher prevalence of genital HPV infection4,18 and are more likely to have multiple HPV types.18 A 2024 study by Fracella et al14 found that 83.5% of HIV-positive men were infected with HPV. The prevalence of anal HPV infection in HIV-infected men is reported to be high, estimated at 86%, and these individuals are also more likely to have anal infections with multiple HPV types.8 Additionally, AGW tends to be more extensive and challenging to treat in HIV-positive patients. These poor clinical outcomes are largely due to immunosuppression, which impairs the body’s ability to clear HPV infections.18 HIV reduces CD4+ lymphocyte levels and disrupts the activation of dendritic cells and the activity of CD8+ lymphocytes. Remarkably, CD8+ lymphocytes may play an important role in removing HPV-infected epithelial cells. HIV impact on both CD4+ and CD8+ lymphocytes may decrease the clearance of HPV-infected epithelial cells and facilitate cell-cycle dysregulation.5 In a 2019 study by Chikandiwa et al18 it was found that 90% of HIV-positive participants had genital HPV DNA, with persistent infection associated with low CD4+ counts. Only 20% of participants achieved complete clearance in 6 months. Additionally, HIV-positive men with a CD4+ count of at least 350 cells/µL were nearly 3.7 times more likely to clear AGW compared to those with a CD4+ count of less than 350 cells/µL. The patient’s CD4 count was only 192 cells/µL, which suggests a low likelihood of achieving clearance.
In addition to an individual’s immunological status, several factors have been identified as influencing the clearance of HPV infection. A correlation exists between age and viral clearance, with individuals aged 26–30 years showing a lower likelihood of clearing the infection compared with those aged 18–20 years.19 The patient in this case report is 28 years old, which may make clearing HPV infection more challenging. The number of sexual partners also influences the clearance, although the impact is contradictory.19 According to the report, having more lifetime sexual partners is inversely associated with persistent HPV infection.20 However, Lu et al19 found that men who reported more than 16 lifetime sexual partners were 4.9 times more likely to clear oncogenic HPV infection compared to those who reported 0–4 partners. The patient in this case report had over 10 sexual partners. Clinically confirmed circumcision was significantly linked to a higher likelihood of clearing any HPV infection.19 Furthermore, prior clinical trials suggest that penile circumcision lowers the risk of both HIV and HPV infections, although the underlying mechanisms for this effect remain unclear.5 In this case, the patient had already undergone circumcision. Various types of HPV exhibit different clearance rates. HPV-16 had the lowest rate, while HPV-6 and HPV-11 were slightly higher, with clearance rates of 13.5 and 14.1 cleared episodes per 1000 person-months, respectively, and an average infection duration of 33.5 months. In contrast, HPV-26, HPV-34, HPV-40, and HPV-66 demonstrated the highest clearance rates.8 PCR examination performed in this case showed positivity for HPV types 6 and 11. Different anatomical sites exhibit varying clearance rates for HPV. In the cervix, HPV infections typically resolve in 1 to 2 years,21 while the clearance rates of HPV DNA in the anus are lower than those in the penis.22 Tian et al22 found that anal HPV-6 had the lowest clearance rate, at 21.6 per 1000 person-months, among MSM patients. In this case report, our patient had manifestations of perianal lesions.
AGW treatment focuses on eliminating visible warts that cause symptoms. However, no therapy has been proven to completely eradicate HPV infection.12 Self-application treatments include topical podophyllotoxin, imiquimod, and sinecatechins, while clinic-based options are cryotherapy, TCA solutions at 80–90%, electrosurgery, electrocautery, excision, and other surgical methods.11,12 Although recurrences can occur with any treatment, surgical methods are the most effective, with a primary clearance rate approaching 100%.11 Individuals with HIV are treated using the same approaches as those without.12 The treatments are typically painful,23 leading the patient in this case report to seek alternate therapies. GA is a natural triterpene saponin found in the root and rhizomes of plants in the genus Glycyrrhiza (eg, Glycyrrhiza glabra and G. uralensis), commonly known as liquorice.12,24 This compound has demonstrated antiviral properties24 and has shown effectiveness in treating HPV infection.25 Specifically, GA has been noted for its ability to inhibit the expression of viral oncoproteins E6 and E7, which are involved in cell proliferation and transformation.26 Nine clinical trials have been published on the use of GA for treating HPV infection, encompassing a total of 531 participants. These individuals included those with HPV and low-grade squamous intraepithelial lesion (LSIL) in the cervix, vagina, or vulva, as well as men and women with anogenital condylomas and patients with focal multi-epithelial hyperplasia in the oral cavity.12
A 2015 study compared the effectiveness of GA to liquid nitrogen (LN) in treating focal multiepithelial hyperplasia. The GA group achieved a 63% effectiveness rate, while the LN group reached 81%. This proves that GA is effective, although its efficacy is lower than that of LN.27 A 2005 study assessed the use of topical GA over 10 days in 100 female patients diagnosed with LSIL, finding an effectiveness rate exceeding 90% by the end of treatment, with only minimal side effects reported.28 A similar study involving patients with LSIL was conducted in 2011. In this study, combination therapy with topical and oral GA was administered to 62 female patients, resulting in improvement for 74% of patients by 12 weeks and for all patients by 13 weeks.25 GA may also reduce HPV transmission. This was demonstrated in a 2020 observational study involving 26 women with vaginal papillomatosis who received topical GA in the form of a spray 3 times a day, one week before the expected birth. Samples were collected from both the oral and genital regions on the first day after delivery and analyzed for HPV infection using the PCR method. All neonates tested negative for HPV. Follow-up observations over a period of 18 months also revealed no evidence of viral presence. As a result, all infants were HPV negative, and vaginal papillomatosis was eliminated after delivery.29
Romo et al13 conducted a Phase IV clinical trial in pediatric patients in 2013, with 76 participants. In this study, 68.4% of the patients (26 individuals) had complete clearance of their lesions, while 28.9% (11 patients) had a reduction in lesions of more than 75%. In a 2012 study by Dominguez Gomez et al,3 100 individuals with anogenital lesions were divided into two groups of 50. One group was given Glizigen® and Viusid®, while the other received 25% podophyllin in alcohol. The Glizigen®-Viusid® combination had an 87.5% effectiveness rate, which was higher than the podophyllin treatment. Furthermore, the adverse effects were minimal.
There have been no reported clinical trials of GA in HIV-infected individuals. Achdiat et al17 reported a case series on the response to GA 0.1% application, where clinical observations in two cases showed limited improvement, with only minor reductions in the number and size of lesions. However, dermoscopic findings showed a transition from a finger-like to a knob-like pattern, demonstrating a favorable response to the GA 0.1% spray treatment.17 The combination of topical and oral GA therapy has no effect in this case report. This is most likely because HIV has already infected and destroyed CD4+ T cells, which are essential for the immunological response to viruses. The poor response could be attributed to a low CD4 level in our patient (CD4 cell count of 192 cells/µL).
Although preliminary results are encouraging, the existing evidence remains limited. Well-designed randomized controlled trials are required to substantiate the efficacy of GA, particularly in immunocompromised populations. More studies are also needed to explore the relationship between CD4 levels and treatment outcomes in AGW patients receiving GA therapy. As a single-case observation, the results in this case cannot be generalized to all patients with anogenital warts, particularly those with HIV infection. Future studies should include larger case series or controlled clinical studies to better assess the effectiveness and safety of GA in managing AGW among HIV-infected patients.
Conclusion
In conclusion, numerous studies have shown that the treatment of AGW with Glizigen® in combination with Viusid® can yield excellent outcomes. However, this combination therapy appears to be less effective in individuals living with HIV. Factors such as low CD4+ count, age, number of sexual partners, HPV type, and anatomical site of infection may significantly influence HPV clearance in these patients. This case emphasizes the necessity of developing less destructive but equally effective therapeutic alternatives for the management of AGW in HIV-infected individuals. Further large-scale, controlled studies are warranted to comprehensively assess the efficacy and safety of GA as a potential treatment option in this population.
Abbreviations
AGW, anogenital warts; GA, glycyrrhizinic acid; HIV, human immunodeficiency virus; HPV, human papillomavirus; HR-HPV, high-risk HPV; LN, liquid nitrogen; LR-HPV, low-risk HPV; LSIL, low-grade squamous intraepithelial lesion; ORF, open reading frames; PCR, polymerase chain reaction; STI, sexually transmitted infections; TCA, trichloroacetic acid.
Ethical Approval and Consent to Participate
Ethical review and approval were required to publish the case details in accordance with the local legislation and institutional requirements. This study’s ethics approval was obtained from the Research Ethics Committee of Dr. Hasan Sadikin General Hospital, Bandung, with the registry number DP.04.03/D.XIV.6.5/164/2025.
Consent for Publication
The patient has signed the consent forms for the use of case details, images for publication, and scientific purposes. Approval has been obtained from Dr. Hasan Sadikin General Hospital to publish the case details.
Acknowledgments
The authors are grateful to the staff of the Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Funding
The authors declare that this study has received no financial support.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Winer R, Koutsky L. Genital human papillomavirus infection. In: Holmes K, Sparling P, Stamm W, Piot P, Wasserheit J, Corey L, editors. Sexually Transmitted Diseases. New York: McGraw-Hill; 2008:489–501.
2. Sichero L, Giuliano AR, Villa LL. Human papillomavirus and genital disease in men: what we have learned from the HIM Study. Acta Cytol. 2019;63(2):109–117. doi:10.1159/000493737
3. Domínguez Gómez J, Simón RD, Abreu Daniel A, Zelenkova H. Effectiveness of glycyrrhizinic Acid (glizigen) and an immunostimulant (viusid) to treat anogenital warts. ISRN Dermatol. 2012;2012:1–6. doi:10.5402/2012/863692
4. Magalhães GM, Vieira ÉC, Garcia LC, De Carvalho-Leite MLR, Guedes ACM, Araújo MG. Update on human papilloma virus - part I: epidemiology, pathogenesis, and clinical spectrum. An Bras Dermatol. 2021;96(1):1–16. doi:10.1016/j.abd.2020.11.003
5. Pérez-González A, Cachay E, Ocampo A, Poveda E. Update on the epidemiological features and clinical implications of Human Papillomavirus Infection (HPV) and Human Immunodeficiency Virus (HIV) coinfection. Microorganisms. 2022;10(5):1–22. doi:10.3390/microorganisms10051047
6. Sindhuja T, Bhari N, Gupta S. Asian guidelines for condyloma acuminatum. J Infect Chemother. 2022;28(7):845–852. doi:10.1016/j.jiac.2022.03.004
7. Konopnicki D, De Wit S, Clumeck N. HPV and HIV coinfection: a complex interaction resulting in epidemiological, clinical and therapeutic implications. Future Virol. 2013;8(9):903–915. doi:10.2217/fvl.13.69
8. de Pokomandy A, Rouleau D, Ghattas G, et al. Prevalence, clearance, and incidence of anal human papillomavirus infection in HIV-infected men: the HIPVIRG Cohort Study. J Infect Dis. 2009;199(1):965–973. doi:10.1086/597207
9. Zhu P, Qi R, Yang Y, Huo W, Zhang Y, He L. Clinical guideline for the diagnosis and treatment of cutaneous warts. J Evid Based Med. 2022;15(3):284–301. doi:10.1111/jebm.12494
10. Gilson R, Nugent D, Werner RN, Ballesteros J, Ross J. 2019 IUSTI‐Europe guideline for the management of anogenital warts. J Eur Acad Dermatol Venereol. 2020;34(8):1644–1653. doi:10.1111/jdv.16522
11. Shah M, Timoney MT, Atrio JM, et al. Prevention and Management of Human Papillomavirus Infection in Adults with HIV. Baltimore (MD): Johns Hopkins University; 2022.
12. Bravo V, Serrano M, Duque A, Ferragud J, Coronado PJ. Glycyrrhizinic acid as an antiviral and anticancer agent in the treatment of human papillomavirus. J Pers Med. 2023;13(12):1–13. doi:10.3390/jpm13121639
13. Romo EM, Fundora FP, Ramirez CR, Rodriguez AY, Hana Z. Effectiveness of glycyrrhizinic acid and an immunostimulant to treat genital warts in the pediatric patient population. Int J Med Health Sci. 2013;3(1):88–93.
14. Fracella M, Oliveto G, Roberto P, et al. The epidemiology of anal Human Papillomavirus (HPV) in HIV-positive and HIV-negative women and men: a ten-year retrospective observational study in Rome (Italy). Pathogens. 2024;13(2):1–11. doi:10.3390/pathogens13020163
15. Milano G, Guarducci G, Nante N, Montomoli E, Manini I. Human papillomavirus epidemiology and prevention: is there still a gender gap? Vaccines. 2023;11(6):1–16. doi:10.3390/vaccines11061060
16. Colpani V, Falcetta FS, Bidinotto AB, et al. Prevalence of human papillomavirus (HPV) in Brazil: a systematic review and meta-analysis. PLoS One. 2020;15:e0229154. doi:10.1371/journal.pone.0229154
17. Achdiat PA, Rowawi R, Gunawan H, Suwarsa O, Sutantoyo CJ. Clinical dermatoscopical response of glycyrrhizinic acid 0.1% spray in treating external anogenital warts in HIV patients: a case series. HIV AIDS Rev. 2021;20(1):65–69. doi:10.5114/hivar.2021.105050
18. Chikandiwa A, Pisa PT, Muller EE, et al. Incidence, persistence, clearance, and correlates of genital human Papillomavirus infection and anogenital warts in a cohort of men living with human immunodeficiency virus in South Africa. Sex Transm Dis. 2019;46(5):347–353. doi:10.1097/OLQ.0000000000000979
19. Lu B, Wu Y, Nielson CM, et al. Factors associated with acquisition and clearance of human papillomavirus infection in a cohort of US men: a prospective study. J Infect Dis. 2009;199(3):362–367. doi:10.1086/596050
20. Bettampadi D, Sirak BA, Abrahamsen ME, et al. Factors associated with persistence and clearance of high-risk oral Human Papillomavirus (HPV) among participants in the HPV Infection in Men (HIM) Study. Clin Infect Dis. 2021;73(9):e3227–34. doi:10.1093/cid/ciaa1701
21. Wierzbicka M, San Giorgi MRM, Dikkers FG. Transmission and clearance of human papillomavirus infection in the oral cavity and its role in oropharyngeal carcinoma - A review. Rev Med Virol. 2023;33(1):1–9. doi:10.1002/rmv.2337
22. Tian T, Fu L, Wang B, et al. Clearance of anal and penile HPV 6, 11, 16, and 18 DNA and antibodies among adolescent men who have sex with men (HYPER): an observational cohort study. Vaccine X. 2024;20(1):1–6. doi:10.1016/j.jvacx.2024.100551
23. Özkaya DB, Erfan G, Çıtamak B. The effectiveness of genital wart treatments. J Urol Surg. 2023;10(3):179–188. doi:10.4274/jus.galenos.2023.2023-6-8
24. Huan C, Xu Y, Zhang W, Guo T, Pan H, Gao S. Research progress on the antiviral activity of glycyrrhizin and its derivatives in liquorice. Front Pharmacol. 2021;12(1):1–10. doi:10.3389/fphar.2021.680674
25. Hernández-Valencia M, Carrillo-Pacheco A, Hernández-Quijano T, Vargas Girón A, Vargas López C. Clinical response to glycyrrhizinic acid in genital infection due to human papillomavirus and low-grade squamous intraepithelial lesion. Clin Pract. 2011;1(e93):200–202.
26. Ahmad A, Tiwari RK, Mishra P, et al. Antiproliferative and apoptotic potential of Glycyrrhizin against HPV16+ Caski cervical cancer cells: a plausible association with downreguation of HPV E6 and E7 oncogenes and Notch signaling pathway. Saudi J Biol Sci. 2022;29(5):3264–3275. doi:10.1016/j.sjbs.2022.01.054
27. Cáceres SO, Fragoso RR, Mena CC, et al. Focal multiepithelial hyperplasia: comparative treatment, glycyrrhizinic acid versus liquid nitrogen. Rev Odont Mex. 2015;19(1):101–105.
28. Espinoza de Los Monteros JA, Álvarez A, Castillo M, Barragán LA. Clinical and endoscopic efficacy of activated glycyrrhizinic acid (Epigen) in the treatment of the infection due to human papillomavirus in the cervix. Rev Clim. 2005;8(1):187–192.
29. Sakaniia LR, Gurguliia AA, Korsunskaia IM. Preparing for childbirth in HPV-compromised women. Gynecology. 2020;22(1):108–110.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.