Back to Journals » Clinical Interventions in Aging » Volume 18
Clinical Efficacy of Interlaminar and Transforaminal Spinal Endoscopy in the Treatment of Lumbar Spinal Stenosis
Authors Liang M, Wang Y, Jiang Y, Li J, Wang Y
Received 7 February 2023
Accepted for publication 19 May 2023
Published 1 June 2023 Volume 2023:18 Pages 881—890
DOI https://doi.org/10.2147/CIA.S406566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Min Liang, Yangyang Wang, Yunduo Jiang, Jingyu Li, Yansong Wang
Department of Spinal Surgery, the First Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China
Correspondence: Yansong Wang, Department of Spinal Surgery, the First Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China, Email [email protected]
Purpose: To compare the application effect of interlaminar technique (ILT) and transforaminal technique (TFT) spinal endoscopies in lumbar spinal stenosis (LSS) treatment.
Material and Methods: The data of 46 patients aged 65 years or older diagnosed with LSS between January 2019 and March 2021 were retrospectively reviewed in this study. They underwent ILT (21 patients) or TFT (25 patients) spinal endoscopy surgery, and outcomes were analyzed utilizing the visual analog scale (VAS), Oswestry disability index (ODI), and Japanese orthopedic association (JOA) scale. Lumbar stability was also evaluated using the change in dynamic position X-ray of the spine. We also built three-dimensional (3D) finite element of ILT and TFT spine models and compared them with the stability of the intact spine.
Results: The ILT group had a longer operation time than the TFT group, and patients in ILT and TFT groups had comparable VAS scores for back pain. However, the TFT group had higher VAS scores for leg pain than the ILT group 3, 6 and 12 months postoperatively. The JOA and ODI scores of the 2 groups improved after surgery, and there were statistical differences between the 2 groups at 6 and 12 months follow-up, which proved that functional recovery was better in ILT group. The pre- and postoperative change in dynamic position X-ray of the spine proved that ILT and TFT would not destroy the spine’s stability. 3D finite element lumbar spine model analysis also demonstrated this point.
Conclusion: Both ILT and TFT can provide good clinical outcomes; compared with TFT, the ILT approach provided more thorough decompression and was more suitable for treating LSS.
Keywords: lumbar spinal stenosis, interlaminar technique, transforaminal technique, spinal endoscopy
Introduction
Lumbar spinal stenosis (LSS) is a common disease leading to low back and leg pain, especially in elderly patients. The combination of hernia of intervertebral discs, facet hyperplasia, and hypertrophy of ligamentum flavum can cause lumbar spinal canal stenosis and compress the nerves and blood vessels, directly leading to neurogenic claudication and neural symptoms.1,2 When conservative treatment fails, surgical treatment should be considered.
The traditional surgical methods include decompression and fusion. Although sufficient decompression and stability can be achieved, muscle and bone structure damage cannot be ignored. Meanwhile, many older people have chronic diseases and poor tolerance to surgery and general anesthesia;3,4 moreover, osteoporosis in the elderly can cause a risk of internal fixation loosening.5 Therefore, open surgery is not always suitable for the elderly.
Now, spinal endoscopy is in a period of rapid development, its indication range is constantly expanding, currently, many degenerative diseases of the lumbar spine can be done under endoscopy, even including spinal instability and the management of tumors and infection.6 Secondly, the number of approaches continues to grow, cervical, thoracic, lumbar, interlaminar, and transforaminal approaches are now feasible, and there will be more approaches in the future.6
Now, it has been gradually applied to LSS treatment.7,8 While providing effective decompression, the spinal endoscope is less traumatic and costly.9 It can be done under local anesthesia,10,11 effectively decreasing postoperative complications and making it more suitable for the elderly. However, current evidence is still limited, spinal endoscopic techniques still require long-term, extensive follow-up and evaluation with scientific methods to confirm their efficacy, risks and advantages.6
The interlaminar technique (ILT) and transforaminal technique (TFT) are 2 main endoscopic approaches, in order to explore the application effect, we retrospectively analysed the application of ILT and TFT in treating LSS.
Materials and Methods
Patients and Methods
From January 2019 to March 2021, the data of 46 patients with single segment LSS who underwent ILT (21 patients) or TFT (25 patients) spinal endoscopy were collected and retrospectively reviewed.
The inclusion criteria were: 1. neurogenic claudication and/or radicular pain; 2. LSS confirmed by imaging findings [Figures 1A-D and 2A-D]; 3. failure of conservative treatment for at least 3 months; and 4. age of 65 years or older.
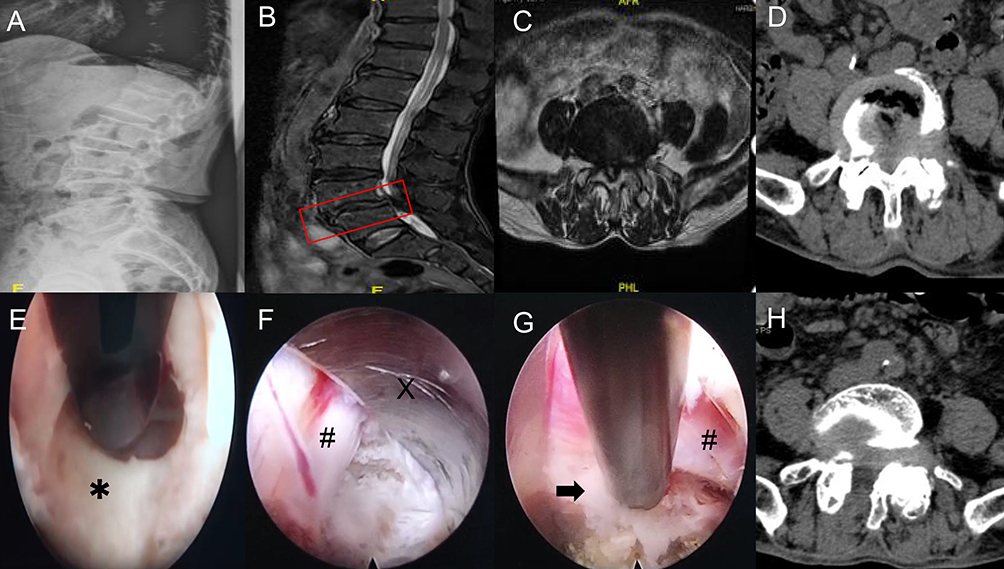 |
Figure 1 Pre-and postoperative imaging data of a patient in the interlaminar technique group. (A–D) The imaging data shows obvious stenosis of the L4-5 spinal canal. The red box in subfigure B indicates the site of lumbar stenosis. (E) Under endoscopic visualization, the ligamentum flavum is cut open. Asterisk shows the ligamentum flavum. (F and G) The working channel (X) is rotated, and the nerve root (#) is pushed gently away from the channel, then the herniated discs (black arrow) could be exposed for removal. (H) Postoperative cross-sectional CT shows a significant enlargement of the spinal canal. |
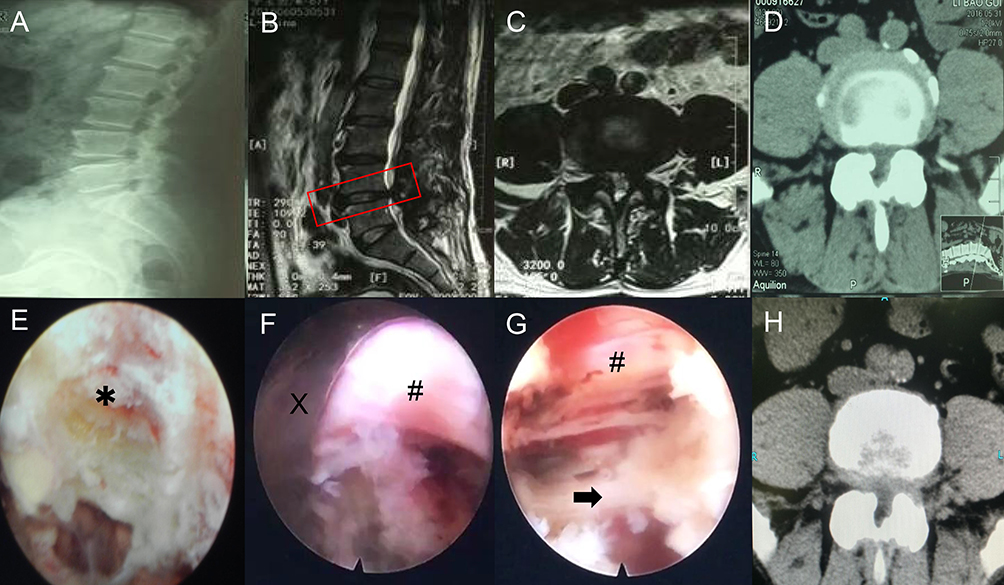 |
Figure 2 Pre-and postoperative imaging data of a patient in the transforaminal technique group. (A–D) The imaging data shows obvious stenosis of the L4-5 spinal canal. The red box in subfigure B indicates the site of lumbar stenosis. (E) Part of the ventral elements on the superior articular process is removed. Asterisk shows the superior articular process. (F and G) The working channel (X) is well established, after the herniated discs are removed, the ventral side of the nerve root (#) is fully decompressed. A black arrow shows the posterior longitudinal ligament. (H) Postoperative cross-sectional CT shows the spinal canal decompression range is limited. |
The exclusion criteria were: 1. previous history of spinal surgery; 2. segmental instability on dynamic radiographs; and 3. low back pain being the main symptom.
The demographic and clinical data of the study patients are shown in Table 1. There was no significant difference in age, sex, and comorbidities between the 2 groups (Table 1).
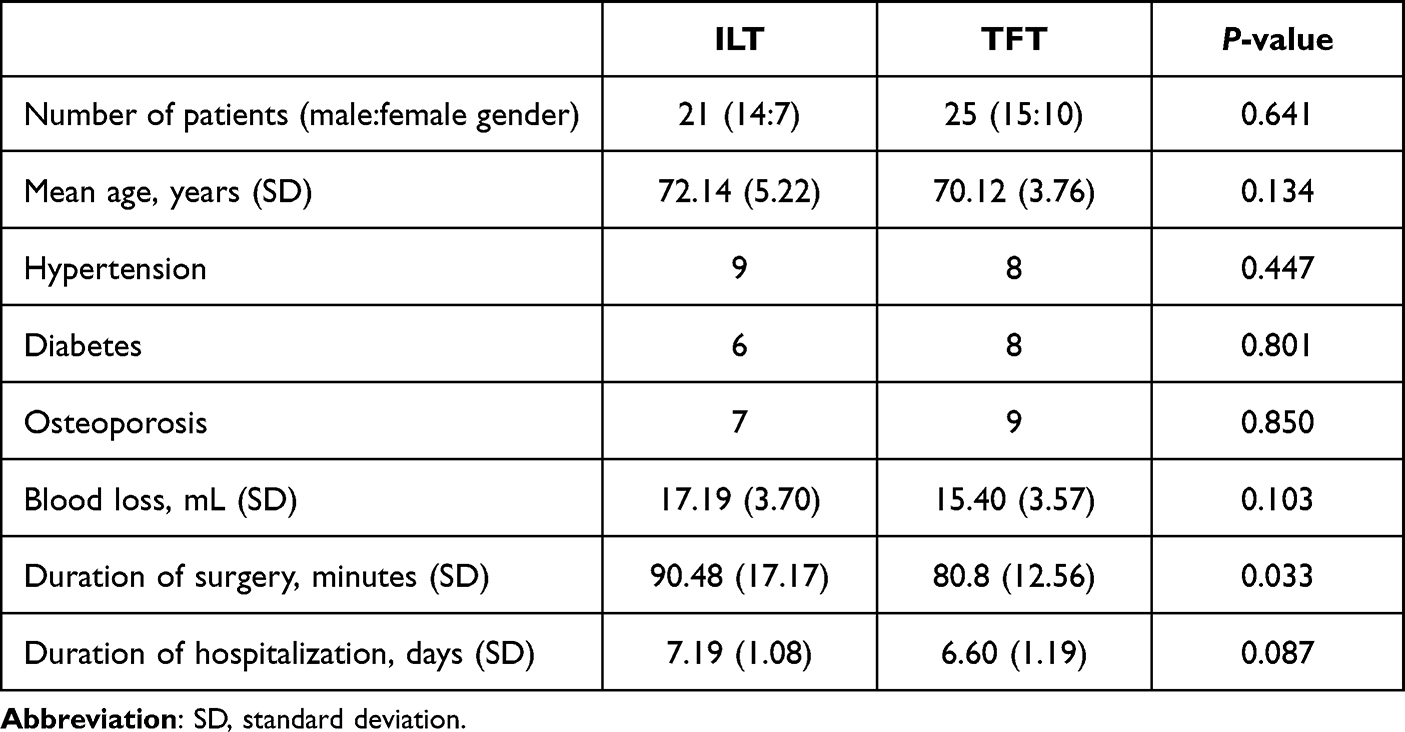 |
Table 1 Demographics and Comorbidities of Study Patients |
Surgical Procedure
ILT endoscopic approach: the patient took a prone position, and the entry point was above the corresponding lamina space and 2–3 cm from the midline horizontally [Figure 3A]. Then, 15–20 mL of 0.25% lidocaine was injected layer-by-layer into the lumbar facet joint and ligamentum flavum. A transverse incision, approximately 15 mm long, was made, the working channel was placed, and the 10-mm large channel endoscope (Spinendos GmbH, München, Germany) was placed. The translaminar space was enlarged by removing part of the facet joint, and the thickened ligamentum flavum [Figure 1E] and hyperplastic facet joint were resected carefully. The resection range did not exceed the outer edge of the nerve root and the attachment point of ligamentum flavum [Figure 3B]; after the epidural space was exposed, 3–5 mL of 1% lidocaine was injected into the epidural space. Soon after the anesthesia took effect, the working channel was rotated, and the nerve root was pushed gently away from the channel to avoid nerve damage [Figure 1F]. Then, the herniated discs could be exposed for removal [Figure 1G].
 |
Figure 3 The entry point and osteotomy range of interlaminar and transforaminal techniques. (A) The entry point of interlaminar technique was above the corresponding lamina space and 2–3 cm from the midline. (B) The range of translaminar space in interlaminar technique did not exceed the outer edge of the nerve root and the attachment point of ligamentum flavum. The yellow box indicates the extent of facet joint and ligamentum flavum resection in ILT. (C) The entry point of transforaminal technique was 8–12 cm from the midline. (D) The grinding ratio of the superior articular process was limited to less than 25%. The yellow box indicates the range of removal of upper articular process in TFT. |
TFT endoscopic approach: The posture and anesthesia method were the same as ILT, but the entry point was 8–12 cm from the midline [Figure 3C]. Generally, part of the ventral elements on the superior articular process needed to be removed to place the working channel [Figure 2E]. Still, the grinding ratio of the superior articular process was limited to less than 25% [Figure 3D]. When the working channel was well established, the endoscope (Spinendos GmbH, München, Germany) can be inserted [Figure 2F], and the protruding lumbar intervertebral disc that compressed the nerve was removed step by step, the ventral side of the nerve root was fully decompressed [Figure 2G].
The 2 methods were compared using the visual analog scale (VAS), Oswestry Disability Index (ODI), and Japanese Orthopedic Association scores (JOA) to evaluate the clinical outcomes. The therapeutic effects were recorded preoperatively and 1 week, 1 month, 3 months, 6 months, and 12 months postoperatively.
Lumbar segmental instability was an abnormal motion to physiologic loads, which was greater than the normal range of motion.12,13 Despite limitations, dynamic analysis in flexion-extension remains the most common standard reference for the diagnosis of structural lumbar segment instability,14,15 and we selected a commonly used definition in this study: change in angulation greater than 10° or translation greater than 4 mm on the dynamic position X-ray of the spine was considered segmental instability [Figure 4A-D].16,17 We also used the three-dimensional finite element method to establish the ILT, TFT, and intact lumbar spine models and compared the von Mises stress, shear stress, and total deformation of different groups.
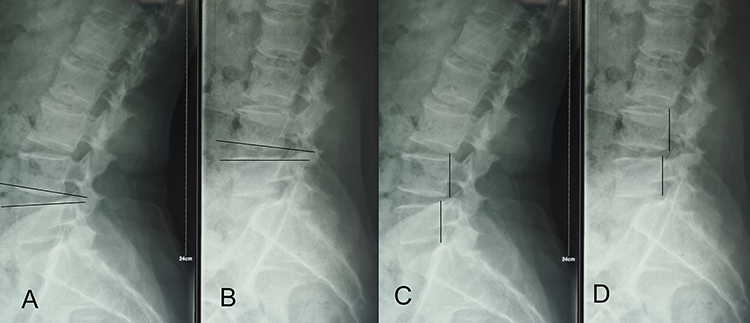 |
Figure 4 The changes in angulation (A and B) and translation distance (C and D) on the lateral flexion and extension were used to reflect the spine’s stability. |
Statistical Analysis
Another researcher, who was blinded to group allocation, made an independent collection and assessment of data.
The categorical variables were compared using the chi-square test and the independent continuous variables were compared using the t-test; p<0.05 was considered significant. The statistical analyses were performed using IBM SPSS (version 23.0, IBM Corp.).
Results
Preoperative Demographic Characteristics and Outcome
The preoperative demographic characteristics and outcomes are shown in Table 1. Twenty-nine men and 17 women were included in this study, the average age was 72.14 and 70.12 years in the ILT and TFT groups, respectively. Analysis showed that there were no significant differences in terms of gender, age and co-morbidities of hypertension, diabetes, and osteoporosis, and these diseases were not conducive to open surgery. The ILT group had a significant longer operation time (p<0.05) than the TFT group, and the mean value of blood loss and duration of hospitalization in ILT group were also higher, but they had no statistical differences (p>0.05). During the follow-up periods, there were no reoperations and no surgery-related complications, such as dural tears, nerve root injuries, or wound infections in the 2 groups.
Clinical Results
We used the VAS scores to describe the degree of back and leg pain quantitatively. As shown in Figure 5A and B and Table 2, there was no difference in back and leg pain levels in ILT and TFT groups preoperatively; the postoperative scores of back pain in the 2 groups decreased, and there was no significant difference in the VAS back pain scores over time (p>0.05) [Figure 5A]. In terms of relief of leg pain symptoms, at the initial stage, there was no significant difference (p>0.05), but the score of the TFT group was higher than that of the ILT group at 3, 6 and 12 months (p<0.05), which proved ILT can more effectively relieve limb symptoms [Figure 5B].
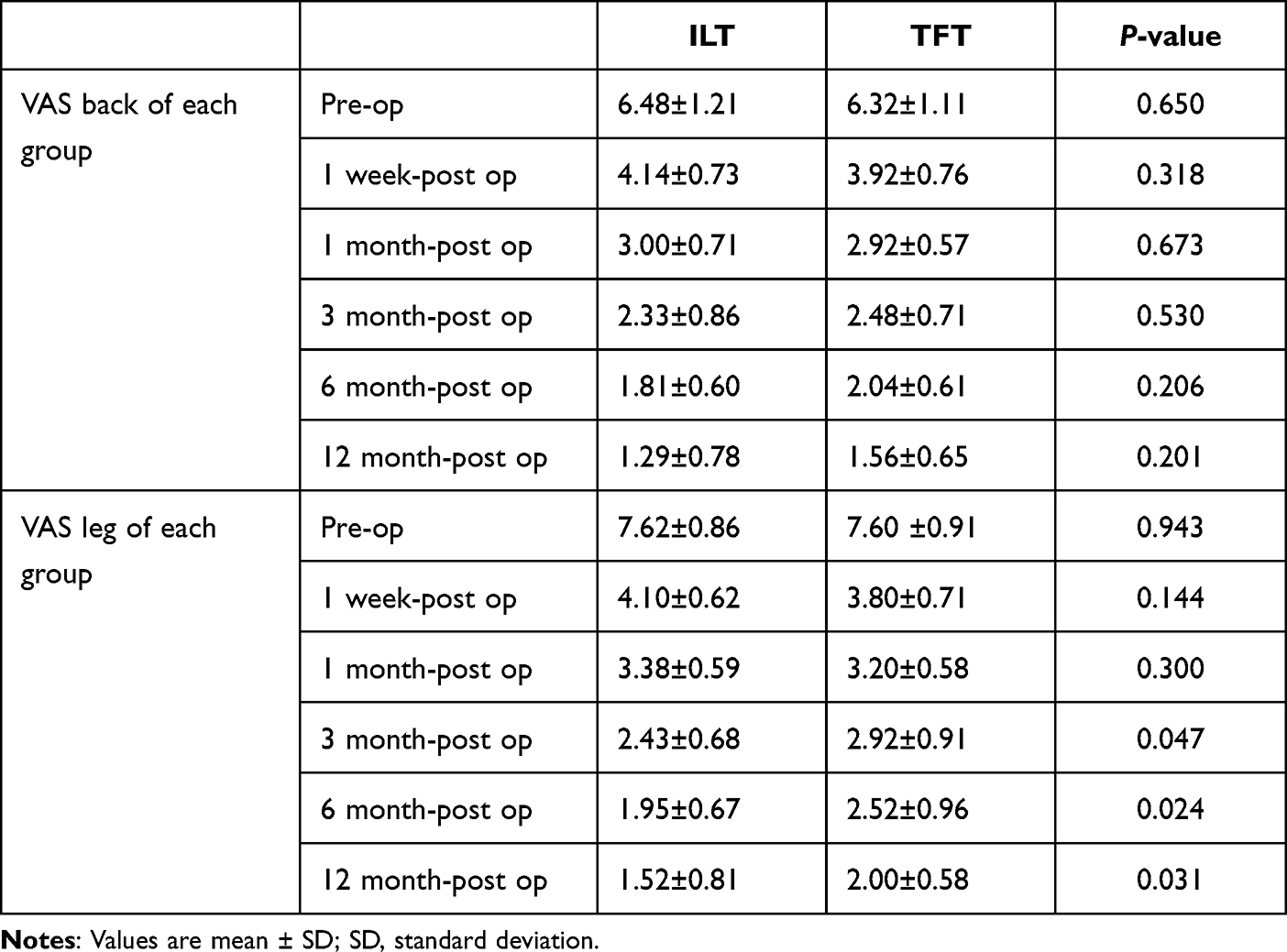 |
Table 2 VAS of the 2 Groups |
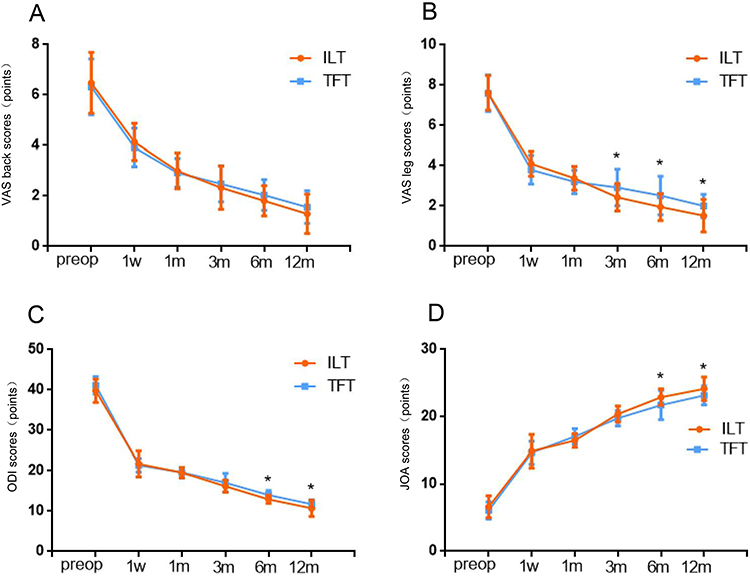 |
Figure 5 Effects of clinical outcomes over time. (A and B) The VAS scores of back and leg pain in different groups. (C and D) The ODI and JOA scores in different groups. *p < 0.05. |
We also used the ODI and JOA scores to evaluate the recovery of lower limb function and patients’ quality of life [Figure 5C and D; Table 3]. The ODI and JOA scores of the 2 groups improved after surgery, and from 3 months onwards, functional recovery was better in the ILT group than in the TFT group. There were statistical differences between them at 6 and 12 months (p<0.05) [Figure 5C and D]. This result was consistent with the result of postoperative leg pain scores.
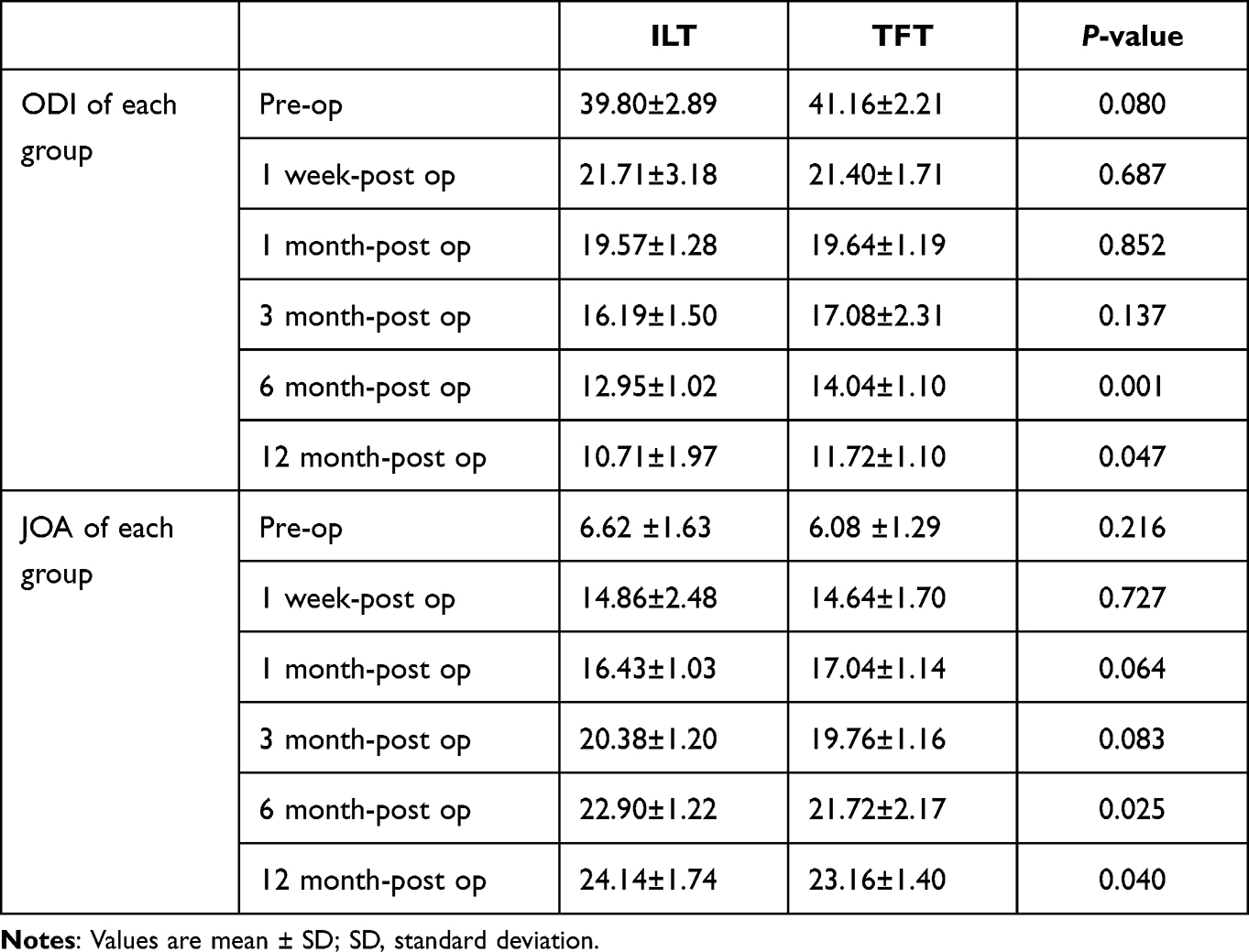 |
Table 3 ODI and JOA of the 2 Groups |
Stability of the Lumbar Spine
In this study, the change in angulation and translation distance on the dynamic position X-ray of the spine were recorded to estimate the spine’s stability [Figure 6A and B]. After the surgery, the change in angulation was still less than 10°, and the translation distance was still within 4 mm in both groups, so the surgical segment remained stable after the operation.
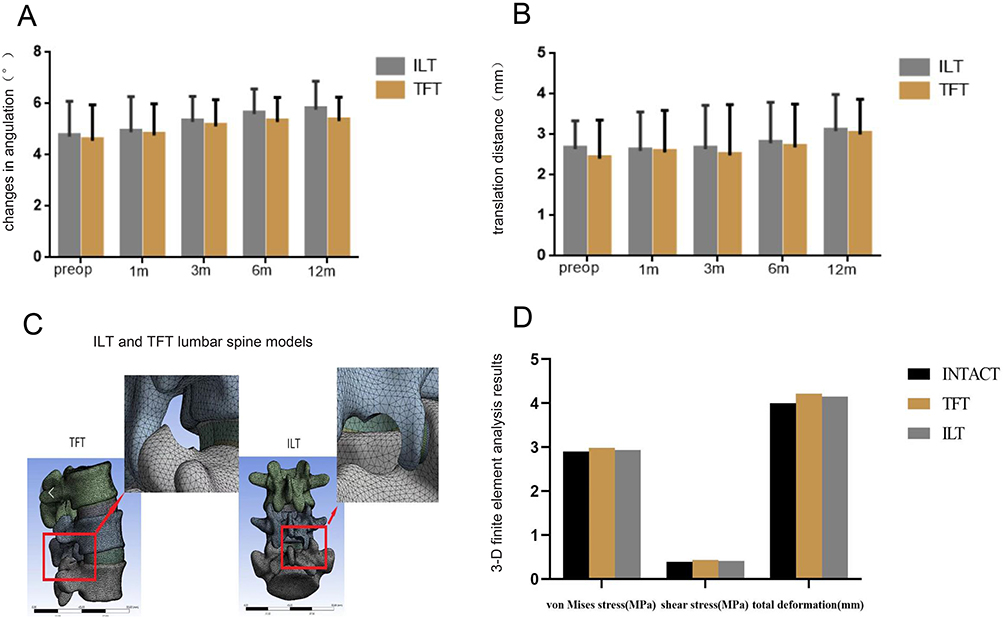 |
Figure 6 Effects of lumbar stability over time and 3-D finite element analysis. (A) The change in angulation of the spine in different groups. (B) The translation distance of the spine in different groups. (C) Establishment of ILT and TFT lumbar spine models. (D) 3-D finite element analysis results of spine models. |
At each time point of this study, there were no statistical differences between the 2 groups (p>0.05), which demonstrated no difference in the effect of the 2 endoscopic modalities on spine’s stability. Low back pain is the main symptom of lumbar instability,18 and this symptom in the 2 groups was continuously relieved after surgery. This also suggested that there was no lumbar instability.
The 3D finite element modeling analysis showed that in 3 different test items, the outcomes of the 3 groups were similar, with no statistical difference (p>0.05) [Figure 6C and D]. Thus, the overall impact on the stability of the lumbar spine was very small for both endoscopic modalities.
Discussion
Through the imaging data, we found that LSS is very common in older people, but many people have no symptoms; only when the imaging examination is consistent with the clinical manifestations can it have diagnostic significance. The choice of surgical treatment for LSS should be based on the cause, scope, and degree of LSS, and the treatment effect depends on precise and adequate decompression rather than the choice of minimally invasive or open surgery.
Compared with open surgery, endoscopic surgery has some obvious advantages, such as local anesthesia,10 minimal invasion,19,20 less blood loss, and lower cost.21 Before endoscopic spinal surgery, careful analysis of imaging data must be undertaken to determine the range and degree of decompression. In this study, in order to avoid the influence of multi segment lumbar spinal stenosis, We selected single segment lumbar spinal stenosis as the research object.
According to different surgical approaches, lumbar spinal endoscopy can be divided into ILT and TFT. It has been previously reported that ILT can effectively decompress LSS caused by disc fragments, ligamentum flavum hypertrophy, facet hyperplasia and osteophytes,22,23 The area of the dural tube can be increased up to 408.0% by ILT (range: 211–774%),21 while TFT mainly relieves the compression caused by disc herniation.21 Many studies have examined the clinical effectiveness of ILT and TFT for lumbar disc herniation, with mixed findings,24 but few studies focused on the clinical efficacy of ILT and TFT for LSS. In this study, most cases were accompanied by facet joint hyperplasia and ligamentum flavum hypertrophy, and there were few cases of lumbar stenosis caused by simple disc herniation. The postoperative CT imaging showed that ILT could effectively remove the hypertrophic ligamentum flavum, osteophyte, and protruding lumbar intervertebral disc, and the canal was fully decompressed [Figure 1H]. However, TFT had a limited decompression range [Figure 2H], which may be why ILT was superior to TFT in relieving symptoms and functional recovery of legs after operation in this study.
But, the operation process of ILT was more complicated, the thickened ligamentum flavum and hyperplastic facet joint need to be carefully removed, and before the nerve root was pushed by working channel, another epidural injection of lidocaine was required. In TFT surgery, once the working channel was established, the endoscope was inserted, and the protruding lumbar intervertebral disc can be removed directly. So the operation time of ILT was longer.
Many are worried that the destruction of the spinal posterior column during endoscopic spinal surgery may cause spinal instability, especially ILT, which requires the removal of the ligamentum flavum, and part of the facet joint. TFT requires the removal of part of the ventral side of the superior articular process, which has relatively less impact on the spine’s stability. In this study, the range of translaminar space in ILT did not exceed the outer edge of the nerve root and the attachment point of ligamentum flavum. In TFT, the grinding ratio of the superior articular process was less than 25%, and there was no lumbar instability in both groups after the operation. We also built ILT and TFT lumbar spine models and found that lumbar spinal endoscopic procedures would not cause lumbar instability as long as they are properly performed.
Limitations
The present study has some limitations, with a relatively small number of observed cases and a short follow-up period, and the surgical effect is also affected by the operation of the surgeon, so, the study is not generalizable and need further improvement.
Conclusion
For patients with spinal stenosis, spinal endoscopy makes the surgical procedure minimally invasive and endoscopic, which has the advantages of less trauma, less bleeding, and faster recovery, without affecting spinal stability, for the elderly, spinal endoscopy surgery is a more suitable option. Compared with the TFT approach, the ILT approach provided more thorough spinal canal decompression, which is suitable for patients with disc herniation accompanied by hypertrophy of ligamentum flavum and facet joint hyperplasia. For patients with spinal canal stenosis mainly caused by disc herniation, TFT surgery can be selected.
Abbreviations
LSS, Lumbar spinal stenosis; ILT, interlaminar technique; TFT, transforaminal technique; VAS, visual analog scale; ODI, Oswestry disability index; JOA, Japanese orthopedic association; 3D, three-dimensional; CT, computed tomography.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
This study was approved by the institutional review board of the First Affiliated Hospital of Harbin Medical University, and written informed consent was obtained from participants prior to data collection. This study was conducted in accordance with the Declaration of Helsinki.
Funding
There is no financial support for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Storm PB, Chou D, Tamargo RJ. Lumbar spinal stenosis, cauda equina syndrome, and multiple lum bosacral radiculopathies. Phys Med Rehabil Clin N Am. 2002;13(3):713–733. doi:10.1016/S1047-9651(02)00013-X
2. Botwin KP, Gruber RD. Lumbar spinal stenosis: anatomy and pathogenesis - ScienceDirect. Phys Med Rehabil Clin N Am. 2003;14(1):1–15. doi:10.1016/S1047-9651(02)00063-3
3. Pan W, Ruan B. Surgical decompression via the unilateral intervertebral foraminal approach with local anesthesia for treating elderly patients with lumbar central canal stenosis. Neurosurg Focus. 2021;51(6):E5. doi:10.3171/2021.9.FOCUS21420
4. Katz JN. Point of view: surgical outcome of 438 patients treated surgically for lumbar spinal stenosis. Spine. 1997;22(19):2282. doi:10.1097/00007632-199710010-00017
5. Wang T, Zhao Y, Cai Z, Wang Y. Effect of osteoporosis on internal fixation after spinal osteotomy: a finite element analysis. CLIN BIOMECH. 2019;69:178–183. doi:10.1016/j.clinbiomech.2019.07.032
6. Chung AS, Mcknight B, Wang JC. Scientific view on endoscopic spine surgery: can spinal endoscopy become a mainstream surgical tool? World Neurosurg. 2020;145:708–711. doi:10.1016/j.wneu.2020.05.238
7. Dong HH, Quillo-Olvera J, Park CK. Can the biportal endoscopic surgery achieve enough canal decompression for degenerative lumbar stenosis? Prospective case-control study. World Neurosurg. 2018;117:120. doi:10.1016/j.wneu.2018.06.028
8. Lu HG, Pan XK, Hu MJ, et al. Percutaneous transforaminal endoscopic decompression for lumbar lateral recess stenosis. Front Surg. 2021;8:631419. doi:10.3389/fsurg.2021.631419
9. Mattei TA, Fassett DR. Endoscope-assisted spinal decompression surgery for lumbar spinal stenosis: technical note. J Neurosurg Spine. 2013;19(6):644–671. doi:10.3171/2013.5.SPINE13474
10. Guan Y, Huang T, An G. Percutaneous endoscopic interlaminar lumbar discectomy with local anesthesia for L5-S1 disc herniation: a feasibility study. Pain Phys. 2019;22(6):E649–E654.
11. Hou KD, Dong-Yin MA, Zhou ZG, et al. Surgical strategy of percutaneous endoscopic interlaminar lumbar discectomy for L5-S1 disc herniation under local anesthesia. Chine J Med. 2018;1:45.
12. Friberg O. Instability in spondylolisthesis. Orthopedics. 1991;14(4):463–465. doi:10.3928/0147-7447-19910401-11
13. Frymoyer JW, Selby DK. Segmental instability. Rationale for Treatment Spine. 1985;10(3):280–286. doi:10.1097/00007632-198504000-00017
14. Iguchi T, Kanemura A, Kasahara K, et al. Lumbar instability and clinical symptoms: which is the more critical factor for symptoms: sagittal translation or segment angulation? J Spinal Disord Tech. 2004;17(4):284–290. doi:10.1097/01.bsd.0000102473.95064.9d
15. Pitkanen MT, Manninen HI, Lindgren KAJ, et al. Segmental lumbar spine instability at flexion–extension radiography can be predicted by conventional radiography. Clin Radiol. 2002;57(7):632–639. doi:10.1053/crad.2001.0899
16. Hanley EN. The indications for lumbar spinal fusion with and without instrumentation. Spine. 1995;20:143S–53S. doi:10.1097/00007632-199512151-00012
17. Shaffer W, Spratt KF, Weinstein J, Lehmann TR, Goel V. 1990 Volvo Award in clinical sciences. The consistency and accuracy of roentgenograms for measuring sagittal translation in the lumbar vertebral motion segment. An experimental model. Spine. 1990;15(8):741.
18. Silvano F, Manni T, Bonetti F, Villafañe JH, Vanti C. A literature review of clinical tests for lumbar instability in low back pain: validity and applicability in clinical practice. Chiropr Man Therap. 2015;23:14. doi:10.1186/s12998-015-0058-7
19. Shin DA, Kim KN, Shin HC, et al. The efficacy of microendoscopic discectomy in reducing iatrogenic muscle injury. J Neurosurg Spine. 2008;8(1):39–43. doi:10.3171/SPI-08/01/039
20. Huang TJ, Hsu RW, Li YY, et al. Less systemic cytokine response in patients following microendoscopic versus open lumbar discectomy. J Orthop Res. 2005;23:406–411. doi:10.1016/j.orthres.2004.08.010
21. Yadav YR, Parihar V, Kher Y, et al. Endoscopic inter laminar management of lumbar disease. Asian J Neurosurg. 2016;11(1):1. doi:10.4103/1793-5482.145377
22. Sairyo K, Sakai T, Higashino K, et al. Complications of endoscopic lumbar decompression surgery. Minim Invasive Neurosurg. 2010;53(04):175–178. doi:10.1055/s-0030-1262814
23. Ikuta K, Tono O, Tanaka T, et al. Surgical complications of microendoscopic procedures for lumbar spinal stenosis. Minim Invas Neurosur. 2007;50(3):145–149. doi:10.1055/s-2007-985152
24. Liu HQ, Hu BS, Chen CM, et al. Comparison of full endoscopic lumbar discectomy using the transforaminal approach versus interlaminar approach for L5-S1 lumbar disc herniation treatment: a meta-analysis. J Neurol Surg Part A;1:54.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.