Back to Journals » Clinical Ophthalmology » Volume 9
Clinical effectiveness of brinzolamide 1%–brimonidine 0.2% fixed combination for primary open-angle glaucoma and ocular hypertension
Authors Sharma S, Trikha S, Perera S ![]() , Aung T
, Aung T
Received 4 September 2015
Accepted for publication 15 October 2015
Published 24 November 2015 Volume 2015:9 Pages 2201—2207
DOI https://doi.org/10.2147/OPTH.S72380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sourabh Sharma,1 Sameer Trikha,1 Shamira A Perera,1 Tin Aung1,2
1Glaucoma Department, Singapore Eye Research Institute, Singapore National Eye Centre, 2Department of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract: The main first-line treatment strategy for glaucoma is to reduce intraocular pressure (IOP) by topical ocular hypotensive medications, but many patients require multiple medications for adequate IOP control. Fixed-combination therapies provide several benefits, including simplified treatment regimens, theoretical improved treatment adherence, elimination of the potential for washout of the first drug by the second, and the reduction in ocular exposure to preservatives. β-Adrenoceptor antagonists (particularly 0.5% timolol) are the most commonly used agents in combination with other classes of drugs as fixed-combination eyedrops, but they are contraindicated in many patients, owing to local allergy or systemic side effects. A fixed-combination preparation without a β-blocker is therefore warranted. This paper reviews the clinical effectiveness of brinzolamide 1% and brimonidine 0.2% fixed combination (BBFC) for use in patients with primary open-angle glaucoma and ocular hypertension. We searched PubMed and the ClinicalTrials.gov registry, and identified three randomized controlled trials comparing BBFC vs its constituents (brimonidine vs brinzolamide), and one comparing BBFC with unfixed brimonidine and brinzolamide. All of the studies demonstrated mean diurnal IOP to be statistically significantly lower in the BBFC group compared with constituent groups and noninferior to that with the concomitant group using two separate bottles. The safety profile of BBFC was consistent with that of its individual components, the most common ocular adverse events being ocular hyperemia, visual disturbances, and ocular allergic reactions. Common systemic adverse effects included altered taste sensation, oral dryness, fatigue, somnolence, and decreased alertness. BBFC seems to be a promising new fixed combination for use in glaucoma patients. However, long-term effects of BBFC on IOP, treatment adherence, and safety need to be determined.
Keywords: Simbrinza, brimonidine, brinzolamide, glaucoma
Background
Pharmacotherapy for glaucoma is commonly commenced with a single topical ocular hypotensive agent.1 Monotherapy, however, may be insufficient in many cases, owing to an inability in achieving target intraocular pressure (IOP) and/or preventing glaucoma progression. In other cases, a single drug may lose its effectiveness over time, due to tachyphylaxis.2 The Ocular Hypertensive Treatment Study reported that at 5 years, about 40% of patients required two medications to achieve a 20% IOP reduction from baseline, while an additional 9% needed more than three medications.3,4 A combination of medications is thus frequently required for adequate control of IOP in the medium to long term. This can be achieved by the concurrent use of two drugs from different classes, either as two separate medications or as a fixed-combination product. The fixed-combination therapies provide multiple potential benefits when compared to concomitant treatment. These include likely increased treatment adherence for patients, decreased exposure to preservatives, and less washout risk on sequential medication instillation. Several studies have established that fixed combinations are equivalent to the unfixed combination dosed concomitantly in terms of IOP control, safety, and support adherence in patients.5–7
β-Adrenoceptor antagonists (particularly 0.5% timolol) are the most commonly used agent in combination with other classes of drugs as fixed-combination eyedrops.8 While they are generally well tolerated, they may be contraindicated or avoided in patients with certain medical conditions, such as asthma, severe chronic obstructive pulmonary disease, sinus bradycardia, impotence, depression, confusion, and memory loss.9
In April 2013, the US Food and Drug Administration (FDA) approved a new fixed-combination ocular antihypertensive that did not include a β-blocker: brinzolamide 1% and brimonidine 0.2% (BBFC).10 In this paper, we review the clinical efficacy of BBFC for use in patients with primary open-angle glaucoma (POAG) and ocular hypertension (OHT).
BBFC contains two active ingredients: a carbonic anhydrase inhibitor (brinzolamide) and an α2-agonist (brimonidine). Brinzolamide, approved in April 1998 by the US FDA, noncompetitively and reversibly inhibits the enzyme carbonic anhydrase (CA-II) in the ciliary epithelium, thereby reducing the formation of bicarbonate ions. This leads to a subsequent reduction in sodium and fluid transport across the ciliary epithelium and decreased aqueous humor formation.11 Brimonidine, on the other hand, was approved by the US FDA in September 1996. It is an α2-adrenoceptor agonist, which inhibits the enzyme adenylate cyclase through the activation of a G protein-coupled receptor and suppresses the cAMP-dependent formation of aqueous humor. It also increases aqueous outflow via the uveoscleral pathway by increased prostaglandin release due to α-adrenergic stimulation.12,13 Recent clinical studies have suggested that topical brimonidine treatment may also have neuroprotective effects, particularly in low-tension-glaucoma subjects.14
Rationale for the fixed combination of brinzolamide and brimonidine
BBFC (Simbrinza®; Alcon Laboratories Inc, Fort Worth, TX, USA) is a sterile, preserved ophthalmic suspension formulation of 1% brinzolamide and 0.2% brimonidine. Brinzolamide 1% treatment has been shown to have efficacy in lowering IOP, ranging from 4 to 5 mmHg.15 The safety profile of brinzolamide is also favorable, the most common ocular adverse events being blurred vision, ocular discomfort, and eye pain.16,17 On the other hand, monotherapy with 0.2% brimonidine has been shown to be safe, well tolerated, and effective in the long-term management of glaucoma patients.18 It lowers IOP on average by 5–6 mmHg with twice-daily dosing.19
The combination of 1% brinzolamide and 0.2% brimonidine in a fixed combination is rational for several reasons. The mechanism of action of these two drugs in lowering IOP is complementary. The combination also achieves steady-state plasma pharmacokinetics comparable to administration as single-ingredient products. Both the drugs are rapidly metabolized by hepatic cytochrome P450, thus minimizing potential clinically significant systemic effects on the cardiovascular or pulmonary system.20,21
BBFC was administered thrice daily in most clinical trials, which is consistent with the approved dosing regimens of brinzolamide and brimonidine. Lastly, it provides an alternative to patients who wish to avoid prostaglandin analogs, which is a common constituent of the currently available fixed-drug combinations. Prostaglandin analogs have been reported to cause conjunctival hyperemia, eyelash growth, and hyperpigmentation of the iris and periocular skin, looking unsightly, particularly if used uniocularly.11,22
Efficacy of 1% brinzolamide and 0.2% brimonidine fixed combination
The efficacy of BBFC in achieving IOP reduction in eyes with POAG and OHT has been established in several well-designed and adequately powered Phase III clinical trials. Table 1 summarizes the findings of the clinical trials published on the use of BBFC.
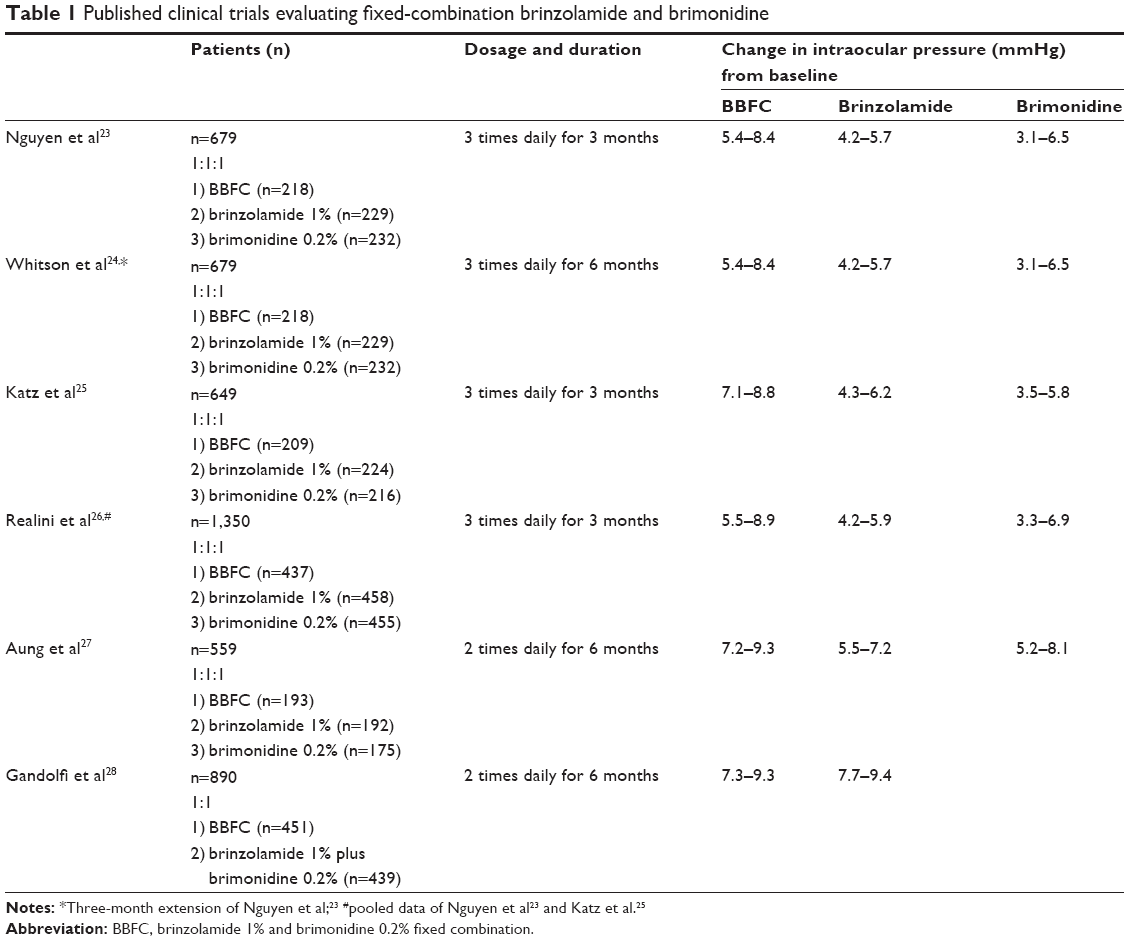 | Table 1 Published clinical trials evaluating fixed-combination brinzolamide and brimonidine |
BBFC vs brimonidine vs brinzolamide
Nguyen et al conducted a multicenter, double-masked, parallel-group study in which 679 patients were randomized 1:1:1 to treatment with BBFC, brinzolamide, or brimonidine thrice daily at 8 am, 3 pm, and 10 pm.23,24 Patients with a clinical diagnosis of POAG or OHT were screened and instructed to discontinue use of all IOP-lowering medications. The washout period ranged from 5 to 28 days, depending on the drug used. Eligible subjects had untreated IOP between 24 and 36 mmHg at the 8 am time point and between 21 and 36 mmHg at the 10 am time point on two qualifying visits 3–8 days apart. IOP was assessed at 2 weeks, 6 weeks, 3 months, and 6 months after the second eligibility visit. At the 3-month end point, mean IOP of the BBFC group was statistically significantly lower than that of either the brinzolamide group or the brimonidine group (P<0.005) across all time points. The IOP superiority observed in the BBFC group ranged from a 3.7% improvement to a 13.4% improvement in IOP reduction from baseline.
A similar “sister” trial was conducted in 660 subjects by Katz et al, who showed that at the end of 3 months, BBFC lowered IOP by 24.1%–34.9% from untreated baseline, while the brinzolamide- and brimonidine-group IOP reductions ranged from 16.9% to 22.6% and 14.3% to 25.8%, respectively.25
Realini et al reported a pooled analysis of the two preceding studies that included 1,350 subjects. Pair-wise comparison of pooled mean IOP (BBFC vs brinzolamide and BBFC vs brimonidine) showed reductions in IOP from baseline across visits and time points of 5.5–8.9 mmHg in the BBFC group, 4.2–5.9 mmHg in the brinzolamide group, and 3.3–6.9 mmHg in the brimonidine group.26
More recently, Aung et al performed a randomized, multicenter, double-masked trial evaluating the efficacy and safety of BBFC dosed twice daily versus each individual active component (ie, brinzolamide 1% and brimonidine 0.2%) for IOP reduction in patients with POAG or OHT.27 In this study, 560 subjects with baseline IOP between 24 and 36 mmHg (assessed at 9 am over two eligibility visits), underwent washout followed by a treatment phase with four on-therapy visits at week 2, week 6, month 3, and month 6. Baseline diurnal IOP was similar among the three groups (BBFC 25.9±0.19 mmHg; brinzolamide 25.9±0.20 mmHg; brimonidine 26.0±0.19 mmHg). At 3 months, the mean change in diurnal IOP was statistically significantly greater with BBFC versus brinzolamide (mean difference for BBFC minus brinzolamide −1.4 mmHg, P<0.0001) and brimonidine (mean difference for BBFC minus brimonidine −1.5 mmHg, P<0.0001). In addition, the percentages of patients with IOP <18 mmHg were numerically greater in the BBFC group versus brinzolamide or brimonidine alone at most study visits and time points. The results of this study (which included many Asian patients) concurred with those in Caucasians.
BBFC vs concomitant brimonidine and brinzolamide
Gandolfi et al conducted a double-masked noninferiority trial of BBFC versus concomitant therapy of brinzolamide 1% plus brimonidine 0.2% (in two separate bottles), both dosed twice daily.28 Overall, 890 subjects with POAG or OHT were randomly allocated (1:1) to treatment with BBFC or concomitant therapy. Subjects were eligible if after the required washout period, their mean IOP measurements were 24–36 mmHg at 9 am and 21–36 mmHg at 11 am. IOP was assessed at 2 weeks, 6 weeks, 3 months, and 6 months. They observed that after 3 months, the mean diurnal IOP change from baseline with BBFC (−8.5±0.16 mmHg) was noninferior to that with the concomitant treatment (−8.3±0.16 mmHg). The margin of equivalence (the upper limit of the 95% confidence interval of the between-group difference being <1.5 mmHg) between the fixed and unfixed combinations was met at all time points. The percentage of patients with IOP <18 mmHg across study visits was 68.9%–71.6% for those receiving BBFC and 65.8%–71.6% for those receiving the combined regimen.28
Based on the results of the aforementioned studies, it has been established that the fixed combination lowers IOP to a greater extent than either constituent dosed as monotherapy, and is equivalent to the combination when dosed concomitantly. Moreover, this effect occurred early in the treatment course and was maintained throughout the course of treatment.
Safety and tolerability of BBFC
From Phase III trials, the safety profile of BBFC was consistent with the known safety profile of its individual components, and did not pose any additional risk to patients compared to the individual components. Table 2 summarizes the safety characteristics of the individual drugs.
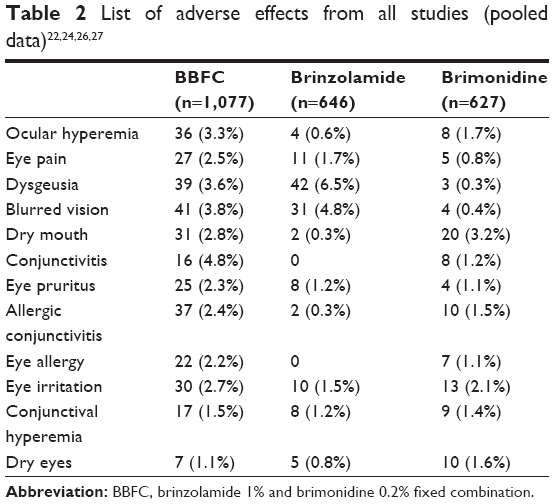 | Table 2 List of adverse effects from all studies (pooled data)22,24,26,27 |
Common ocular adverse events associated with the use of BBFC have been reported to be ocular hyperemia, visual disturbances, conjunctivitis, ocular allergic-type reactions, and ocular discomfort. Common systemic adverse effects reported in the trials included altered taste sensation, oral dryness, fatigue, somnolence, and decreased alertness.23–28 All of these adverse effects occurred in less than 8% of subjects, and had a known association with either brinzolamide or brimonidine. The trials that were randomized 1:1:1 to treatment with BBFC, brinzolamide, or brimonidine had more adverse events in the BBFC group (22%–26%) compared to others (18%–19% in brinzolamide, 17%–18% in brimonidine). On the other hand, adverse drug reactions were reported in a similar percentage of patients receiving BBFC (23.5%) and concomitant therapy of brinzolamide 1% plus brimonidine 0.2% (26.8%). In addition, the monotherapy trials had greater numbers of patients discontinuing participation due to nonserious treatment-related adverse events in the BBFC group (8%–11%) than in others (2%–3% brinzolamide, 5%–9% brimonidine).23–27 The discontinuations were however similar in the 1:1 trial (10% in BBFC and 11.7% in the concomitant group).28 Nevertheless, nonocular serious adverse events associated with either component were uncommon, and there were no clinically meaningful alterations found during systemic assessments.
Some of the warnings to be kept in mind while using BBFC include sulfonamide hypersensitivity, the risk of corneal edema, and caution about the use of the product in patients with severe renal impairment, because of the possible risk of metabolic acidosis. Furthermore, when evaluating its cardiovascular safety profile, researchers noted that there was a small decrease in resting pulse rate and mean systolic and diastolic blood pressure, very similar to what has been seen in those using brimonidine 0.2%.23,24 Therefore, caution is advised when using BBFC concomitantly with antihypertensives and in patients with hypotension and severe or unstable/uncontrolled cardiovascular disease. It is also contraindicated in neonates and children less than 2 years of age, due to the potential for central nervous system depression by brimonidine.29 There are other studies comparing BBFC with fixed combinations that are ongoing.30
Discussion
The current literature supports the efficacy and safety of BBFC, but there are certain limitations of the trials performed so far. For instance, most studies have been short-term. The long-term effect of BBFC on IOP and safety is thus unknown. Moreover, IOP was not measured over a 24-hour period, and thus IOP readings during nocturnal periods were not inferred. Each IOP-lowering medication exhibits significant peaks and troughs at various time points throughout the day, and may not offer a sustained steady-state delivery system. To date, most of the studies have compared the efficacy of BBFC with its two constituent monotherapy treatments, while only one compared it with a concomitant regime. Also, the dosing schedules of BBFC have been different in the various studies. Though the efficacy and safety of twice-daily dosing in one study were similar to thrice-daily dosing in another,23–28 a direct comparison trial is lacking. Both brinzolamide and brimonidine are approved for twice-daily dosing in the EU and many countries outside it. In view of this and comparable results with thrice-daily dosing, a trend toward use of twice-daily dosing is advocated. However, further studies are needed to validate the optimal dosing of BBFC. Moreover, studies do not provide insight as to how BBFC might compare with other fixed-combination therapies. Future studies evaluating alternative combinations, such as dorzolamide/brimonidine FC or even triple-therapy agents are eagerly anticipated. There is also a need for trials to establish the IOP-lowering efficacy of BBFC in other forms of glaucoma, such as primary angle-closure glaucoma, a major form of glaucoma worldwide.
BBFC has superior IOP-lowering activity compared with monotherapy agents in patients with POAG or OHT. Despite this, it has more ocular adverse effects than each of the component agents used alone. Administration of the separate components brimonidine 0.2% and brinzolamide 1% is an alternative; however, the advantages of a fixed-dose regimen favor BBFC. Moreover, it is the only fixed-combination medication for the treatment of glaucoma that does not contain a β-blocker. Additional studies with long-term follow-up will determine if efficacy is maintained over longer periods.
BBFC contains benzalkonium chloride (BAK; 0.03 mg/mL), which may have detrimental effects on the ocular surface, including decreased tear-film stability, increased corneal and conjunctival staining, and increased tear-film osmolarity.31,32 In view of these adverse effects of BAK, efforts are being made to develop preservative-free preparations (eg, tafluprost, travoprost, timolol/bimatoprost fixed combination, travoprost/timolol fixed combination) or to replace BAK with preservatives that are less harmful, like Purite (as in Alphagan® P 0.15%; Allergan Inc, Irvine, CA, USA), a stabilized oxychloro complex and oxidative preservative that is converted to natural tear components when exposed to light.33 A preservative-free formulation of BBFC would thus be a viable option in decreasing BAK-mediated ocular surface toxicity and tolerability issues. Though BAK is considered to increase absorption of coadministered medications, studies have shown that the IOP-lowering efficacy of preservative-free or in particular BAK-free regimens is comparable to their comparators containing BAK.34–36 It would be interesting to know whether the advantages of preservative-free or BAK-free preparations are maintained if used as a part of a fixed combination.
Medication compliance and adherence is low in glaucoma, partly due to the asymptomatic nature of the condition in the early stages.37 Nonadherence is one of the major factors of treatment failure in glaucoma, as almost 80% of patients do not take their medications as prescribed.38,39 This can thus contribute to progression of the disease, necessitating more frequent specialist visits and increased health care costs. A number of factors, such as inadequate patient education, complexity of treatment regimens, side effects of medications, and challenges with regular and correct instillation of eye drops, have been identified as possible barriers to optimal adherence.40–43 Studies have suggested that persistence with glaucoma medications is also low when multiple medications are required.44–46 Fixed-combination therapies, including BBFC, can potentially alleviate a number of these issues. However, one problem lies in the objective estimation of adherence in the long term. Adherence with various topical medication regimens in clinical trials may not reflect the actual clinical practice scenario, and may be an overestimate. The development of delivery- and medication-monitoring devices like the Travatan dosing aid (Alcon), an electronic device designed to assist patients in taking travoprost, may help improve patients’ adherence.47 In turn, this will provide better overall IOP control and improve patient outcomes.
In summary, BBFC seems to be a promising new combination therapy for lowering IOP in patients with POAG and OHT. It has superior IOP-lowering effects compared with monotherapy agents, and comparable adverse events compared to the concomitant regimen. The introduction of this medication has provided us with a new option in the clinician’s glaucoma-management armamentarium.
Disclosure
TA is a consultant to Alcon, and has received research funding, travel support, and honoraria from Alcon. The other authors report no conflicts of interest in this work.
References
Webers CA, Beckers HJ, Nuijts RM, Schouten JS. Pharmacological management of primary open-angle glaucoma: second-line options and beyond. Drugs Aging. 2008;25:729–759. | ||
Boger WP 3rd. Shortterm “escape” and longterm “drift”. The dissipation effects of the beta adrenergic blocking agents. Surv Ophthalmol. 1983;28 Suppl:235–242. | ||
Quigley HA, Enger C, Katz J, Sommer A, Scott R, Gilbert D. Risk factors for the development of glaucomatous visual field loss in ocular hypertension. Arch Ophthalmol. 1994;112:644–649. | ||
Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701–713. | ||
Barnebey H, Orengo-Nania S, Flowers BE, et al. The safety and efficacy of travoprost 0.004%/timolol 0.5% fixed combination ophthalmic solution. Am J Ophthalmol. 2005;140:1–7. | ||
Lee AJ, McCluskey P. Fixed combination of topical brimonidine 0.2% and timolol 0.5% for glaucoma and uncontrolled intraocular pressure. Clin Ophthalmol. 2008;2:545–555. | ||
Inoue K, Shiokawa M, Sugahara M, Wakakura M, Soeda S, Tomita G. Three-month evaluation of dorzolamide hydrochloride/timolol maleate fixed-combination eye drops versus the separate use of both drugs. Jpn J Ophthalmol. 2012;56:559–563. | ||
Higginbotham EJ, Hansen J, Davis EJ, Walt JG, Guckian A. Glaucoma medication persistence with a fixed combination versus multiple bottles. Curr Med Res Opin. 2009;25:2543–2547. | ||
Taniguchi T, Kitazawa Y. The potential systemic effect of topically applied β-blockers in glaucoma therapy. Curr Opin Ophthalmol. 1997;8:55–58. | ||
US Food and Drug Administration. FDA approves Simbrinza for glaucoma, ocular hypertension. 2013. Available from: http://www.medscape.com/viewarticle/803064. Accessed April 18, 2015. | ||
Cvetkovic RS, Perry CM. Brinzolamide: a review of its use in the management of primary open-angle glaucoma and ocular hypertension. Drugs Aging. 2003;20:919–947. | ||
European Glaucoma Society. Terminology and Guidelines for Glaucoma. 3rd ed. Savona, Italy: Editrice Dogma SRL; 2008. | ||
Adkins JC, Balfour JA. Brimonidine. A review of its pharmacological properties and clinical potential in the management of open-angle glaucoma and ocular hypertension. Drugs Aging. 1998;12:225–241. | ||
Krupin T, Liebmann JM, Greenfield DS, Ritch R, Gardiner S. A randomized trial of brimonidine versus timolol in preserving visual function: results from the Low-Pressure Glaucoma Treatment study. Am J Ophthalmol. 2011;151:671–681. | ||
Wang TH, Huang JY, Hung PT, Shieh JW, Chen YF. Ocular hypotensive effect and safety of brinzolamide ophthalmic solution in open angle glaucoma patients. J Formos Med Assoc. 2004;103:369–373. | ||
Iester M. Brinzolamide ophthalmic suspension: a review of its pharmacology and use in the treatment of open angle glaucoma and ocular hypertension. Clin Ophthalmol. 2008;2:517–523. | ||
van der Valk R, Webers CA, Schouten JS, Zeegers MP, Hendrikse F, Prins MH. Intraocular pressure-lowering effects of all commonly used glaucoma drugs. A meta-analysis of randomized clinical trials. Ophthalmology. 2005;112:1177–1185. | ||
Melamed S, David R. Ongoing clinical assessment of the safety profile and efficacy of brimonidine compared with timolol: year-three results. Brimonidine Study Group II. Clin Ther. 2000;22:103–111. | ||
Toris C, Camras C, Yablonski M. Acute versus chronic effects of brimonidine on aqueous humor dynamics in ocular hypertensive patients. Am J Ophthalmol. 1999;128:8–14. | ||
Centre for Drug Evaluation and Research. Clinical pharmacology and biopharmaceutics review(s). 2013. Available from: www.accessdata.fda.gov/drugsatfda_docs/nda/2013/204251Orig1s000ClinPharmR.pdf. Accessed October 18, 2015. | ||
Simbrinza (brinzolamide/brimonidine tartrate ophthalmic suspension) 1%/0.2% [package insert]. Fort Worth, TX: Alcon Laboratories Inc; 2013. | ||
Fellman RL, Sullivan EK, Ratliff M, et al. Comparison of travoprost 0.0015% and 0.004% with timolol 0.5% in patients with elevated intraocular pressure: a 6-month, masked, multicenter trial. Ophthalmology. 2002;109:998–1008. | ||
Nguyen QH, McMenemy MG, Realini T, Whitson JT, Goode SM. Phase 3 randomized 3-month trial with an ongoing 3-month safety extension of fixed-combination brinzolamide 1%/brimonidine 0.2%. J Ocul Pharmacol Ther. 2013;29:290–297. | ||
Whitson JT, Realini T, Nguyen QH, McMenemy MG, Goode SM. Six-month results from a phase III randomized trial of fixed-combination brinzolamide 1% + brimonidine 0.2% versus brinzolamide or brimonidine monotherapy in glaucoma or ocular hypertension. Clin Ophthalmol. 2013;7:1053–1060. | ||
Katz G, Dubiner H, Samples J, Vold S, Sall K. Three month randomized trial of fixed combination brinzolamide, 1%, and brimonidine, 0.2%. JAMA Ophthalmol. 2013;131:724–730. | ||
Realini T, Nguyen QH, Katz G, Dubiner H. Fixed-combination brinzolamide 1%/brimonidine 0.2% vs monotherapy with brinzolamide or brimonidine in patients with open-angle glaucoma or ocular hypertension: results of a pooled analysis of two phase 3 studies. Eye (Lond). 2013;27:841–847. | ||
Aung T, Laganovska G, Hernandez Paredes TJ, Branch JD, Tsorbatzoglou A, Goldberg I. Twice-daily brinzolamide/brimonidine fixed combination versus brinzolamide or brimonidine in open-angle glaucoma or ocular hypertension. Ophthalmology. 2014;121: 2348–2355. | ||
Gandolfi SA, Lim J, Sanseau AC, Parra Restrepo JC, Hamacher T. Randomized trial of brinzolamide/brimonidine versus brinzolamide plus brimonidine for open-angle glaucoma or ocular hypertension. Adv Ther. 2014;31:1213–1227. | ||
Enyedi LB, Freedman SF. Safety and efficacy of brimonidine in children with glaucoma. J AAPOS. 2001;5:281–284. | ||
Tepedino M. Comparison of combigan BID versus simbrinza TID. Available from: https://clinicaltrials.gov/ct2/show/NCT02167035. NLM identifier NCT02167035. Accessed April 18, 2015. | ||
Skalicky SE, Goldberg I, McCluskey P. Ocular surface disease and quality of life in patients with glaucoma. Am J Ophthalmol. 2012;153:1–9.e2. | ||
Rossi GC, Pasinetti GM, Scudeller L, Raimondi M, Lanteri S, Bianchi PE. Risk factors to develop ocular surface disease in treated glaucoma or ocular hypertension patients. Eur J Ophthalmol. 2013;23:296–302. | ||
Cantor LB. Brimonidine in the treatment of glaucoma and ocular hypertension. Ther Clin Risk Manag. 2006;2:337–346. | ||
Goldberg I, Gil Pina R, Lanzagorta-Aresti A, Schiffman RM, Liu C, Bejanian M. Bimatoprost 0.03%/timolol 0.5% preservative-free ophthalmic solution versus bimatoprost 0.03%/timolol 0.5% ophthalmic solution (Ganfort) for glaucoma or ocular hypertension: a 12-week randomized controlled trial. Br J Ophthalmol. 2014;98:926–931. | ||
Holló G, Hommer A, Antón López A, Ropo A. Efficacy, safety, and tolerability of preservative-free fixed combination of tafluprost 0.0015%/timolol 0.5% versus concomitant use of the ingredients. J Ocul Pharmacol Ther. 2014;30:468–475. | ||
Gandolfi S, Paredes T, Goldberg I, et al. Comparison of a travoprost BAK-free formulation preserved with polyquaternium-1 with BAK-preserved travoprost in ocular hypertension or open-angle glaucoma. Eur J Ophthalmol. 2012;22:34–44. | ||
Reardon G, Kotak S, Schwartz GF. Objective assessment of compliance and persistence among patients treated for glaucoma and ocular hypertension: a systematic review. Patient Prefer Adherence. 2011;5:441–463. | ||
Olthoff CM, Schouten JS, van de Borne BW, Webers CA. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension: an evidence-based review. Ophthalmology. 2005;112:953–961. | ||
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. | ||
Rossi GC, Pasinetti GM, Scudeller L, Tinelli C, Milano G, Bianchi PE. Monitoring adherence rates in glaucoma patients using the Travatan dosing aid. A 6-month study comparing patients on travoprost 0.004% and patients on travoprost 0.004%/timolol 0.5% fixed combination. Expert Opin Pharmacother. 2010;11:499–504. | ||
Sleath B, Robin AL, Covert D, Byrd JE, Tudor G, Svarstad B. Patient-reported behavior and problems in using glaucoma medications. Ophthalmology. 2006;113:431–436. | ||
Djafari F, Lesk MR, Harasymowycz PJ, Desjardins D, Lachaine J. Determinants of adherence to glaucoma medical therapy in a long-term patient population. J Glaucoma. 2009;18:238–243. | ||
Taylor SA, Galbraith SM, Mills RP. Causes of non-compliance with drug regimens in glaucoma patients: a qualitative study. J Ocul Pharmacol Ther. 2002;18:401–409. | ||
Robin AL, Novack GD, Covert DW, Crockett RS, Marcic TS. Adherence in glaucoma: objective measurements of once-daily and adjunctive medication use. Am J Ophthalmol. 2007;144:533–540. | ||
Gurwitz JH, Glynn RJ, Monane M, et al. Treatment for glaucoma: adherence by the elderly. Am J Public Health. 1993;83:711–716. | ||
Rotchford AP, Murphy KM. Compliance with timolol treatment in glaucoma. Eye (Lond). 1998;12:234–236. | ||
Flowers B, Wand M, Piltz-Seymour J, et al. Patients’ and physicians’ perceptions of the travoprost dosing aid: an open-label, multicenter study of adherence with prostaglandin analogue therapy for open-angle glaucoma or ocular hypertension. Clin Ther. 2006;28:1803–1811. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.