Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Clinical Characteristics, Dermoscopic Features and Prognosis of Acquired Facial Pigmented Macules in Young Children: A Retrospective Analysis of 160 Cases
Received 2 April 2026
Accepted for publication 30 May 2026
Published 20 June 2026 Volume 2026:19 613888
DOI https://doi.org/10.2147/CCID.S613888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Chen Sun, Hongye Zhang
Department of Dermatology, Children’s Hospital of Nanjing Medical University, Nanjing, Jiangsu, 210008, People’s Republic of China
Correspondence: Hongye Zhang, Department of Dermatology, Children’s Hospital of Nanjing Medical University, No. 72 Guangzhou Road, Gulou District, Nanjing, Jiangsu, 210008, People’s Republic of China, Tel +86 139 5191 6649, Email [email protected]
Objective: To investigate the clinical manifestations, dermoscopic features, and long-term prognosis of acquired facial pigmented macules in young children, and to provide evidence for clinical diagnosis and management.
Patients and Methods: A retrospective study was conducted on 160 children diagnosed with acquired facial pigmented macules at the Dermatology Outpatient Clinic of the Children’s Hospital of Nanjing Medical University between January 2017 and September 2025. Clinical data, including sex, age of onset, lesion distribution, color, morphology, and dermoscopic features, were analyzed. Follow-up was performed during outpatient visits or during WeChat to assess lesion regression and prognosis.
Results: The male-to-female ratio was 1.46:1, with a mean onset age of (0.66 ± 0.35) years, mostly within 6– 8 months after birth. Lesions were irregular brown or brownish-red macules (4mm– 3cm, mainly 4mm– 1cm), predominantly located on the forehead and temporal regions. Two dermoscopic patterns were identified: a non-infiltrating pattern (pseudogrid-like brown pigmentation with linear or punctate telangiectasia), and an infiltrating pattern (pseudogrid-like brown pigmentation without vascular changes). Among 110 followed-up children, 93.64% achieved complete lesion regression at a mean age of (2.82 ± 0.69) years, mostly within 4 years old.
Conclusion: Acquired facial pigmented macules in young children are benign, self-limiting disorders with characteristic clinical and dermoscopic findings. Spontaneous regression occurs in most cases and no specific treatment is required.
Keywords: acquired pigmented macules, facial pigmentation, young children, dermoscopy, self-limited
Introduction
Non-segmental brown or brownish-red macules on the forehead and temporal regions are relatively common in infants and young children. Onset usually occurs within the first year of life without obvious symptoms. Lesions often darken when the child cries, causing parental anxiety and frequent medical visits. This condition was first described as acquired facial pigmented macules by Hernandez-Martin et al in 2014.1 Since then, only small case series have been published.2,3 The pathogenesis remains unclear, and large-sample studies are lacking.
The differential diagnoses of acquired facial pigmented macules in young children include pityriasis versicolor, café-au-lait macules, urticaria pigmentosa, erythema dyschromicum perstans, benign cephalic histiocytosis, post-inflammatory hyperpigmentation, phototoxic reaction, and pigmented contact dermatitis. Dermoscopy is particularly valuable in young children because it is non-invasive, painless, rapid, and well-tolerated in this vulnerable population who cannot cooperate with invasive procedures such as skin biopsy. It enables clear visualization of pigment distribution and vascular structures, reveals specific patterns that are not visible to the naked eye, and helps establish an accurate and reliable diagnosis without any harm to the child. Thus, dermoscopy has become the preferred auxiliary examination for evaluating childhood facial pigmented lesions.
To date, the largest case series on acquired facial pigmented macules included only 25 patients,1 and long-term follow-up data from large samples are lacking. In addition, dermoscopic features have not been classified in previous studies. This study retrospectively analyzed 160 cases to clarify their clinical features, dermoscopic findings, and natural prognosis, with the aim of improving clinical recognition and avoiding unnecessary interventions.
Materials and Methods
Study Population
This retrospective study included children diagnosed with acquired pigmented macules on the face at the Dermatology Department of the Children’s Hospital of Nanjing Medical University from January 1, 2017, to September 30, 2025.
Inclusion Criteria
1. Typical clinical manifestations include brown or brownish-red macules on the forehead and/or temporal region, smooth surface, and no scaling, atrophy, or symptoms.
2. Consistent dermoscopic features.
3. Complete medical records and follow-up data.
Exclusion Criteria
Other facial pigmentary or vascular diseases, including café au lait macules, urticaria pigmentosa, port-wine stain, post-inflammatory hyperpigmentation, phototoxic reaction, pigmented contact dermatitis, pityriasis versicolor, erythema dyschromicum perstans, and benign cephalic histiocytosis.
Data Collection
Clinical data included sex, age at onset, lesion location, color, size, number, and dermoscopic features. Follow-up was conducted via outpatient visits or WeChat with guardians to record regression age and duration.
Dermoscopic Evaluation
Dermoscopic images were obtained using a polarized dermoscope (×20 magnification). All dermoscopic images were independently evaluated by two experienced pediatric dermatologists who were blinded to clinical information.
A consensus diagnosis was reached by discussion in case of disagreement. Inter-observer agreement was assessed using simple consistency comparison and was considered satisfactory for pattern classification.
Follow-Up Protocol
Follow-up was conducted via outpatient revisit or standardized WeChat follow-up. The WeChat follow-up was performed in a uniform manner:
1. Guardians were asked to provide clear facial photographs at consistent lighting and angle.
2. A fixed questionnaire was used to record whether lesions had completely regressed, partially regressed, or persisted.
3. The age at regression and total duration of lesions were documented uniformly.
Handling of Missing Data and Potential Bias
Missing data were handled by complete case analysis, only patients with complete follow-up data were included in the prognostic analysis. Potential selection bias and attrition bias due to loss to follow-up were acknowledged as study limitations and are discussed in the Discussion section.
Statistical Analysis
SPSS 19.0 was used for statistical analysis. Continuous variables are expressed as the mean ± standard deviation. Categorical variables were presented as counts and percentages (95% confidence interval, 95% CI).
Results
Clinical Characteristics
The clinical features of the 160 pediatric patients, including sex, age, age at onset, lesion size, lesion color, lesion site, and lesion count, are summarized in Table 1. The male to female ratio was 1.46:1. The mean age of onset was 0.66 ± 0.35 years. The peak onset was 6–8 months (48.13%).
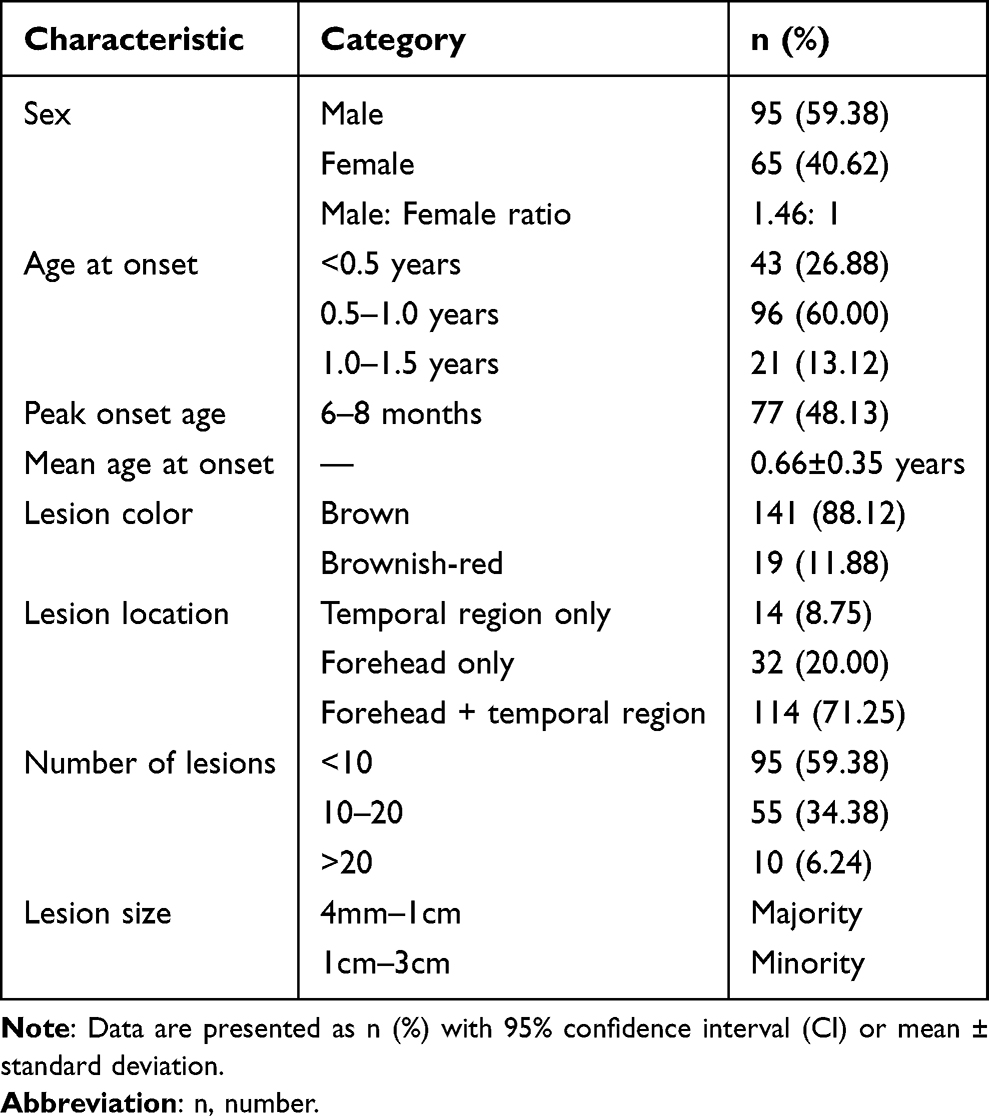 |
Table 1 Clinical Characteristics of 160 Children |
The lesions were irregular and measured 4mm–3 cm (predominantly 4mm–1 cm). Most were brown (88.12%), with 11.88% brownish-red. Lesions mainly involved the forehead and temporal region (71.25%) and were numbered <10 in 59.38% of the cases. Representative clinical images are shown in Figure 1.
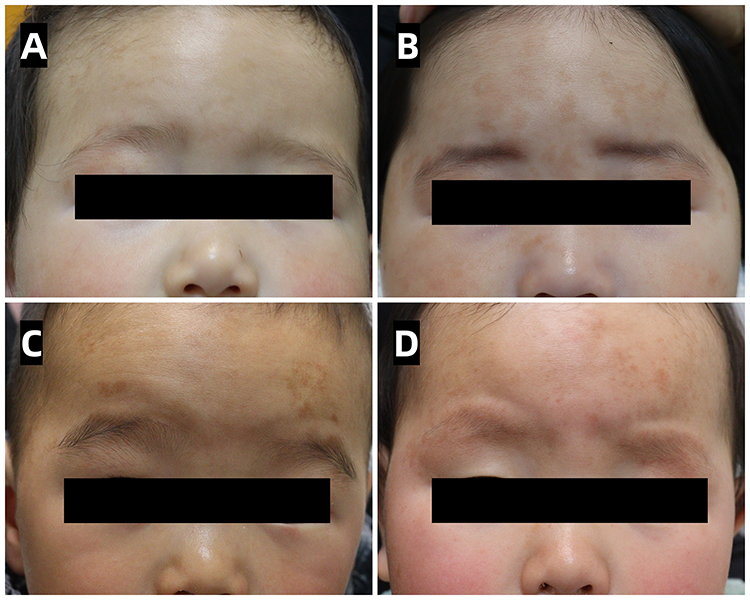 |
Figure 1 Clinical photographs of acquired pigmented macules on the face in young children. (A) Brown pigmented macules of various sizes on the forehead. (B–D) Brownish-red pigmented macules of various sizes on the forehead and temporal region. |
Follow-Up Outcomes
Among the 110 children with a complete follow-up, 103 (93.64%) showed complete regression. The mean age at regression was 2.82 ± 0.69 years. Mean duration of lesions was 2.19 ± 0.68 year, as summarized in Table 2.
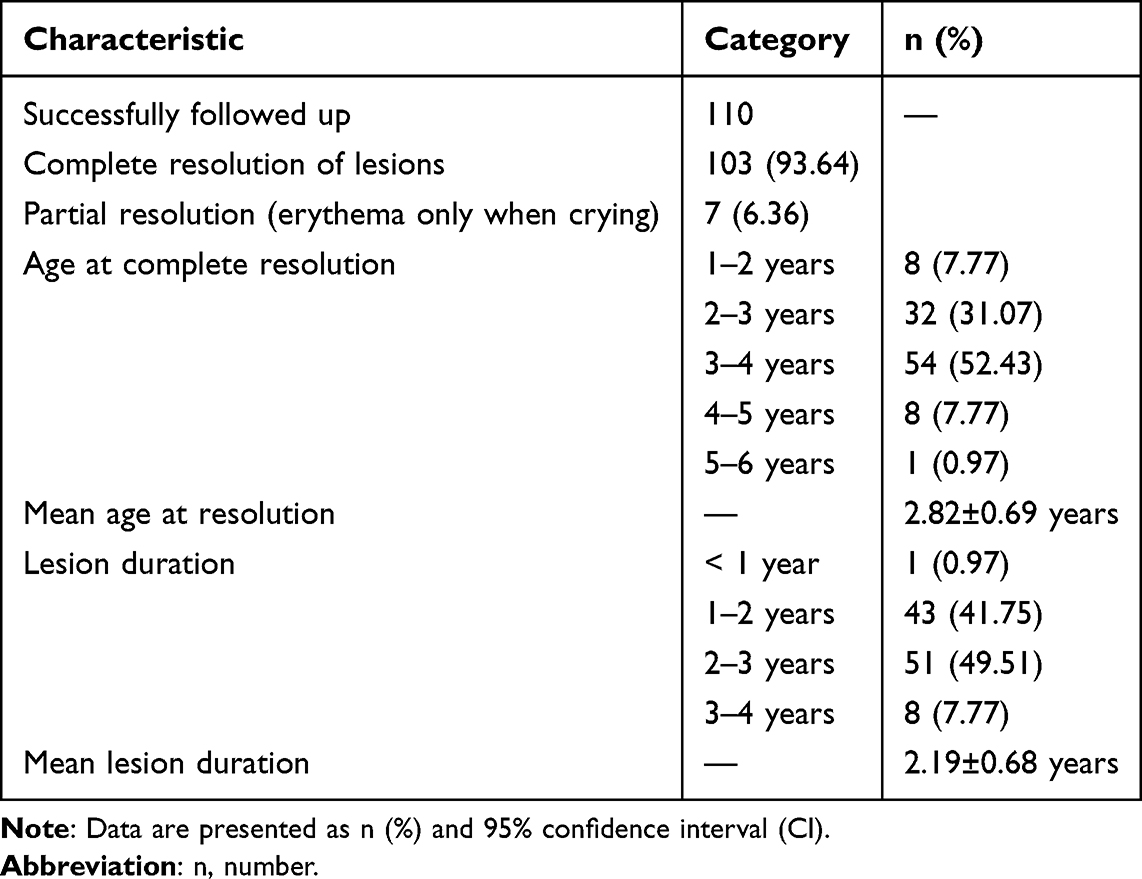 |
Table 2 Follow-Up and Prognostic Outcomes |
Dermoscopic Findings
Two patterns were observed, as shown in Figure 2:
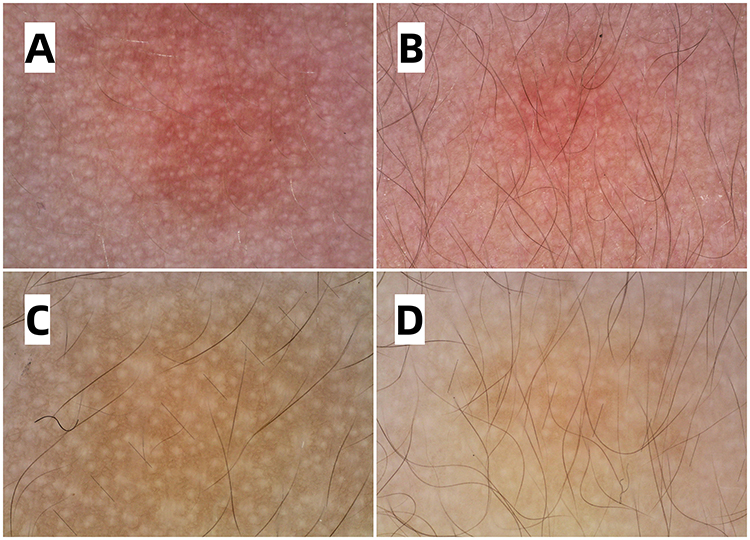 |
Figure 2 Dermoscopic images of acquired pigmented macules. (A and B) Non-infiltrative pattern (20× magnification): pseudogrid-like light brown pigmentation with linear or punctate telangiectasia. (C and D) Infiltrative pattern (20× magnification): Pseudogrid-like brown pigmentation without obvious vascular changes. |
Non-infiltrative pattern: pseudogrid-like brown pigment with linear or punctate telangiectasia.
Infiltrative pattern: only pseudogrid-like brown pigment without vascular changes.
Discussion
Acquired facial pigmented macules in young children are common, benign, and self-limiting dematoses that mainly affects infants and young children. Since first described by Hernandez-Martin et al, 1 this condition has been increasingly recognized in clinical practice, although large-sample studies remain limited. The pathogenesis is unclear, and clinical misdiagnosis is common due to overlapping features with other pigmentary and vascular lesions. Our study is the largest sample size reported to date for this entity, which is is the first large-sample study based on Chinese young children. In this retrospective study, We confirmed a long-term complete resolution rate and defined a clear self-limiting window, which can provide evidence-based data for parental counseling by reporting. And we proposed and classified two distinct dermoscopic patterns for the first time. Our results confirm that this disease has distinctive clinical and dermoscopic features and follows an excellent natural course without active treatment.
In our cohort, the male-to-female ratio was 1.46:1, indicating slight male predominance, with a mean onset age of 0.66 ± 0.35 years, peaking at 6–8 months. These findings are consistent with those of a previous report by Martin et al,1 who observed a mean onset age of 12 months in 25 affected children, suggesting an early infantile onset pattern across studies. The lesions in our study were mostly brown (88.12%), with a small proportion being brownish-red, and were distributed mainly in the forehead and temporal regions (71.25%). Most lesions were irregular, 4mm–3 cm in diameter and predominantly 4mm–1 cm in size. The number of lesions was less than 10 in 59.38% of patients. These typical morphological features help clinicians establish a reliable preliminary diagnosis and reduce misdiagnosis.
Dermoscopy revealed two distinct patterns: a non-infiltrative pattern characterized by pseudogrid-like brown pigmentation with linear or punctate telangiectasia, and an infiltrative pattern showing only pseudogrid-like pigmentation without obvious vascular changes. The presence of telangiectasia in the non-infiltrative pattern correlates well with the clinical observation that lesions become more prominent and reddish when the child cries. These dermoscopic findings are highly consistent with those reported in Lai et al study.4 Thus, dermoscopy serves as a convenient, non-invasive tool to support diagnosis and avoid unnecessary skin biopsy. Similarly, Zhang et al (2021) reported irregular brown macules under dermoscopy and sparse inflammatory cells and melanophages in the superficial dermis on reflectance confocal microscopy, without prominent basal pigmentation.3 These findings further support the idea that pigmentary changes originate mainly from dermal melanophages rather than epidermal hyperpigmentation.
Long-term follow-up of 110 children showed that 93.64% achieved complete spontaneous regression at a mean age of 2.82 ± 0.69 years, mostly by 4 years of age. The resolution rate was higher than that in earlier study by Martin et al (2014), 1 only five of 19 patients achieved complete resolution during a follow-up period of 3 months to 4 years, likely due to our larger sample size and longer follow-up duration. Our results strongly confirmed the self-limiting nature of this condition. No residual scarring or long-term skin changes were observed, supporting the conservative approach with reassurance and observation.
The differential diagnosis of acquired facial pigmented macules includes café-au-lait macules, urticaria pigmentosa, postinflammatory hyperpigmentation, pigmented contact dermatitis, phototoxic reactions, pityriasis versicolor, erythema dyschromicum perstans, benign cephalic histiocytosis, and port-wine stain.5–9 Key distinguishing features include the typical frontotemporal distribution, exacerbation upon crying, negative Darier’s sign, absence of scale or induration, no response to sun exposure, and characteristic dermoscopic findings. In particular, port-wine stains in the midline forehead and eyelid regions are limited to a few bands, such as large red lesions, which can be easily distinguished. A negative potassium hydroxide fluorescent fungal examination and no yellowish-brown fluorescence on Wood’s lamp examination ruled out pityriasis versicolor, which typically presents as regular uniform lesions. Urticaria pigmentosa shows widespread lesions and a positive Darier’s sign,5 in contrast to the localized, smooth, and non-inflammatory lesions in our patients, urticaria pigmentosa showed widespread lesions and a positive Darier’s sign. Café-au-lait macules are not restricted to the frontotemporal region, do not darken with crying, and multiple café-au-lait maculesmay indicate neurofibromatosis.6 Postinflammatory hyperpigmentation shows preceding skin lesions, whereas pigmented contact dermatosis shows confluent involvement corresponding to contact areas and resolves after allergen avoidance.7 Phototoxic reactions demonstrate seasonal variation and sunlight-related exacerbation.8 Benign cephalic histiocytosis presents with papular lesions and histiocytic infiltration on pathology,9 which are distinct from our findings.
The etiology and pathogenesis of acquired pigmented facial macules in young children remain unclear. No definite triggering factors such as trauma, infection, chemical exposure, or cosmetic use were identified in this study. Several points warrant interpretation. First, Giacaman et al (2016) reported two affected sisters,2 suggesting a possible genetic predisposition, however, the sample size is extremely small, and this entity cannot be defined as a hereditary disease. Second, Wang et al (2025) described histopathological findings in 10 affected children, revealing a normal or mildly hyperkeratotic epidermis, mild capillary dilation and proliferation in the dermis, sparse perivascular lymphocytic infiltration, and scattered melanophages.10 These features are are suggestive of post-inflammatory pigmentation at a subclinical level and consistent with a self-limited, reactive pigmentary process. Nevertheless, this explanation cannot fully account for the strict localization to the frontotemporal region or the absence of preceding clinically obvious dermatitis. Third, we propose a hypothesis that vasoreactive dilation amplifies the pigmentary effect, which may explain why lesions become reddish and more prominent during crying. Overall, the precise etiology remains unclear, all hypotheses are still at the speculative stage without definitive confirmation, and future prospective studies are required for further verification.
Based on the existing literature and our large-sample analysis, acquired facial pigmented macules appears to represent an independent disease entity different from other known form of early-onset infantile hyperpigmentation, supporting its status as an independent disease entity. Our long-term follow-up confirmed that this was a benign, self-limiting disorder that resolved spontaneously. Therefore, no specific treatment is required and clinicians should provide appropriate parental reassurance to avoid unnecessary testing or interventions.
Study Limitations
This study has several limitations. First, this is a retrospective, single-center observational study, which may lead to potential selection bias and limited generalizability. Second, only descriptive statistical analysis was performed, and no inferential statistics or hypothesis testing were conducted, as the study aimed to characterize clinical features rather than compare groups or test causality. Third, 50 of 160 patients were lost to follow-up, lost-to-follow-up patients may have achieved spontaneous resolution without further follow-up, which may introduce attrition bias. These limitations should be considered when interpreting the results. These points warrant further supplementation and clarification in future prospective studies.
Conclusion
Acquired facial pigmented macules in young children are common, benign, and self-limiting dermatoses with characteristic clinical and dermoscopic features. Onset occurs in early infancy and most lesions resolve spontaneously without treatment. Clinicians should be aware of this condition to avoid unnecessary testing and therapy. Whether this condition represents an independent disease entity requires more comprehensive and sufficient evidence for validation.
Ethical Approval
This study was approved by the Ethics Committee of the Children’s Hospital of Nanjing Medical University (Approval No.: 202602025-1). Due to the retrospective nature of this study and that it did not involve any intervention to the patients or affect their routine diagnosis and treatment, the requirement for individual informed consent was waived by the Ethics Committee. All patient data were anonymized and kept strictly confidential during the research process, and the study was conducted in compliance with the Declaration of Helsinki.
Acknowledgments
The authors thank all patients and their guardians for their participation in this study. We also thank the staff of the Department of Dermatology for their assistance with the data collection and follow-up.
Funding
This work was not supported by any funding source.
Disclosure
The authors declare no conflict of interest.
References
1. Hernandez-Martin A, Gilliam AE, Baselga E, et al. Hyperpigmented macules on the face of young children: a series of 25 cases. J Am Acad Dermatol. 2014;70(2):288–7. doi:10.1016/j.jaad.2013.10.045
2. Giacaman A, Knöpfel N, Campos M, et al. Acquired facial hyperpigmented macules in children: 3 new cases. Actas Dermosifiliogr. 2016;107(1):81–83. doi:10.1016/j.ad.2015.05.012
3. Zhang LW, Li CH, Lu YH. Acquired hyperpigmented macules on the forehead and temples in a child. Eur J Dermatol. 2021;31(4):590–591. doi:10.1684/ejd.2021.4116
4. Lai S, Lu Y, Huang X, et al. Characteristic dermatoscopic features of hyperpigmented macules on the faces of young children. Clin Pediatr. 2024;63(2):244–248. doi:10.1177/00099228231167842
5. Di Raimondo C, Del Duca E, Silvaggio D, Pavone L. Cutaneous mastocytosis: a dermatological perspective. Australas J Dermatol. 2021;62(1):e1–e7. doi:10.1111/ajd.13443
6. Chen T, Wu J, Yang X, et al. Clinical characteristics of multiple café-au-lait macules and their potential significance in the early screening of genetic diseases. Clin Cosmet Invest Dermatol. 2025;18:1339–1347. doi:10.2147/CCID.S521076
7. Hinton AN, Goldminz AM. Feeling the burn: phototoxicity and photoallergy. Dermatologic Clin. 2020;38(1):165–175. doi:10.1016/j.det.2019.08.010
8. Mindrup R, Idoate R. Neurofibromatosis and a Portrait of 1 in 3000. AMA J Ethics. 2020;22(6):e513–e524. doi:10.1001/amajethics.2020.513
9. Fraitag S, Emile JF. Cutaneous histiocytoses in children. Histopathology. 2022;80(1):196–215. doi:10.1111/his.14569
10. Wang J, Zhang N, Zhang B. Clinicopathologic characteristics of acquired facial telangiectatic hyperpigmented macular dermatosis: a series of 15 cases. J Am Acad Dermatol. 2026;94(4):1309–1310. doi:10.1016/j.jaad.2025.12.062
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.