Back to Journals » Clinical Ophthalmology » Volume 20
Clinical Characteristics and Prognostic Factors for Visual Outcome in Intraocular Foreign Body Cases Treated at a Tertiary Eye Hospital in Indonesia
Authors Adriono GA ![]() , Triyoga IF
, Triyoga IF ![]() , Kadharusman MM, Wijaya AN, Paramitha AN, Juffry SK
, Kadharusman MM, Wijaya AN, Paramitha AN, Juffry SK ![]() , Victor AA
, Victor AA ![]() , Djatikusumo A, Yudantha AR, Hutapea MM
, Djatikusumo A, Yudantha AR, Hutapea MM
Received 2 December 2025
Accepted for publication 5 February 2026
Published 17 February 2026 Volume 2026:20 580427
DOI https://doi.org/10.2147/OPTH.S580427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gitalisa Andayani Adriono,1– 3 Ichsan Fauzi Triyoga,2 Marcello Mikhael Kadharusman,2 Amanda Natalie Wijaya,2 Arstiputri Nindya Paramitha,2 Sarah Kamiela Juffry,2 Andi Arus Victor,1,2 Ari Djatikusumo,1,2 Anggun Rama Yudantha,1,2 Mario Marbungaran Hutapea1– 3
1Department of Ophthalmology, Kirana Eye Center, Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia; 2Faculty of Medicine, University of Indonesia, Jakarta, Indonesia; 3Retina Services, JEC Eye Hospitals & Clinics, Jakarta, Indonesia
Correspondence: Gitalisa Andayani Adriono, Department of Ophthalmology, Kirana Eye Center, Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia, Tel +62 811 131 660, Email [email protected]
Objective: Intraocular foreign bodies (IOFB) remain a significant cause of visual impairment worldwide. The complex nature of IOFB cases poses considerable management challenges, contributing to various outcomes. This study aimed to determine clinical characteristics and prognostic factors associated with visual outcomes following IOFB treatments.
Methods and Analysis: We conducted a retrospective review of IOFB patients admitted between January 2019 - January 2024 at a tertiary hospital in Indonesia. Medical records were evaluated based on predefined inclusion and exclusion criteria.
Results: A total of forty-six patients (46 eyes) were analyzed, of which 76.1% had metallic IOFBs (35 eyes), predominantly caused by hammering metal (70%). Cornea was the most frequent entry site (31 eyes). The mean preoperative best-corrected visual acuity (BCVA) was 1.74 ± 1.01 (logMAR), improving to 1.28 ± 1.03 at the final follow-up. Univariate analysis showed larger IOFB size, worse initial BCVA, longer injury-to-surgery intervals, higher complications, endophthalmitis, traumatic cataract, secondary glaucoma, and primary surgery with lensectomy were significantly associated with poor final BCVA. Multiple logistic regression identified poor baseline BCVA and the need of additional lensectomy procedure as independent risk factors for lower final BCVA.
Conclusion: Lower preoperative BCVA and concomitant lensectomy subsequent to IOFB removal were significant predictors of poor visual prognosis.
Plain Language Summary: What is Already Known on this Topic
IOFBs are a major cause of visual loss in open-globe injuries, with visual outcomes influenced by factors such as IOFB size, material, location, associated complications, and timing of surgery. However, data from Indonesia remain limited despite a high burden of ocular trauma in the region.
What this Study Adds
This study shows that poor baseline visual acuity and concomitant lensectomy at the time of IOFB removal are independent predictors of poor final visual outcome. It also highlights the predominance of metal-related IOFBs, mostly caused by welding accidents, among young adult males.
How this Study might Affect Research, Practice or Policy
These findings emphasize the importance of early prognostication and patient counseling based on baseline vision and surgical planning. It also reinforces the need for occupational safety measures, particularly mandatory protective eyewear in high-risk jobs, and for strengthening early detection and referral systems in resource-limited settings.
Keywords: ophthalmic trauma, intraocular foreign body, clinical characteristics, prognostic factors
Introduction
Intraocular foreign body (IOFB) injuries represent a severe subset of open-globe trauma, defined by a penetrating or lacerating injury to the eyewall with retention of a foreign object within the intraocular compartments. Mechanical eye injuries are broadly classified into open-globe and closed-globe injuries, with further subclassification proposed by the Ocular Trauma Classification Group (OTCG). The OTCG system is more comprehensive than earlier frameworks, incorporating injury type, grade (based on visual acuity), pupillary response, and wound location (zone), thus enabling a more systematic approach to prognosis and management. Open-globe injuries involve a full-thickness wound of the eyewall, including ruptures and lacerations, whereas closed-globe injuries maintain eyewall integrity and include contusions, lamellar lacerations, and foreign bodies.1 These injuries can lead to significant ocular morbidity, with potential complications such as endophthalmitis, retinal detachment, and permanent vision loss. Despite preventive efforts, IOFBs account for approximately 18–41% of all open-globe injuries, primarily affecting the posterior segment of the eye.2–5 The primary causes of IOFB injuries include occupational accidents, particularly in industrial and construction settings, as well as high-risk activities involving metal fragments, such as hammering and drilling.6
Management of IOFB involves prompt surgical intervention, with the approach tailored to the location, composition, and associated ocular damage to reduce complications and improve visual outcomes.3 Surgical removal can be immediate or delayed after globe closure, depending on patient health, visibility of the IOFB, and care environment. Pars plana vitrectomy (PPV) and removal of metallic IOFB with intraocular magnet is the standard approach for posterior segment IOFBs. Diamond-coated forceps, or emerging tools like the nitinol stone extractors, offer improved removal of hard-to-grasp IOFBs.7 Due to the complex nature of each case, the visual prognosis of patients with IOFB remains highly variable, with a subset experiencing significant visual impairment.8
While numerous studies have explored the clinical characteristics and prognostic factors associated with IOFB injuries in high-income settings, data on IOFB cases in low- and middle-income countries, including Indonesia, remain scarce. Differences in occupational risk profiles, resource availability, and referral pathways may impact both presentation of injury and outcomes, highlighting the need for region-specific studies. Ocular trauma in Indonesia is a significant public health concern, with an estimated 46,000 cases annually and 8,000 cases in East Java alone. Most cases occur in males (80.3%) aged 21–30, often caused by sharp or blunt objects.9 Given the high burden of ocular trauma in the region, this study aims to identify the clinical characteristics, prognostic factors, and visual outcomes of patients with IOFB treated at a large, public, tertiary care referral hospital in Jakarta, Indonesia. By identifying key determinants of visual outcomes, physicians can improve risk stratification, guide surgical decision-making, and provide more accurate visual prognostication to patients and their families. This study aims to provide insights regarding the clinical characteristics of IOFB injuries treated at a tertiary referral center in Indonesia and to identify prognostic factors associated with final visual outcomes.
Methods
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Ethics Committee of the Faculty of Medicine, University of Indonesia – Cipto Mangunkusumo Hospital (protocol number: 24–12-1903). Due to the retrospective nature of the study, the Ethics Committee waived the requirement for informed consent. Patient confidentiality was strictly maintained by anonymizing all data prior to analysis, with no personally identifiable information accessed or reported.
Study Design and Sample Collection
A retrospective cohort study reviewed medical records of patients diagnosed with IOFB at the eye unit of a tertiary referral hospital over a five-year period, from December 2019 to December 2024. Patient selection was done using a consecutive sampling method to ensure comprehensive case inclusion.
Inclusion and Exclusion Criteria
Eligible patients were those with a confirmed diagnosis of IOFB through imaging techniques, including X-ray, ultrasonography, and/or orbital CT scans. Both IOFB in the anterior segment and the posterior segment were included. Additionally, patients must have received IOFB treatment at the study institution and attended at least one postoperative follow-up visit, with a minimum duration of one month. Patients with incomplete medical records or those who underwent secondary procedures such as evisceration, enucleation, or exenteration were excluded from the study, as meaningful assessment of final visual acuity and prognostic modeling was not possible in these eyes. Patients with pre-existing severe ocular conditions that significantly affect vision (eg, advanced diabetic retinopathy, chronic glaucoma, or retinal dystrophies) were also excluded, to minimize confounding.
Data Collection
Collected data included demographic details (age, gender), clinical parameters (affected eye, injury-to-presentation time, presentation-to-surgery time, IOFB size, location, and material composition), injury characteristics classified according to the OTCG system (injury grade, type, and zone), OTS, mechanism of injury, secondary clinical features at initial presentation, and best-corrected visual acuity (BCVA) at presentation and first follow-up. Visual acuity was assessed using the Snellen chart and converted to logMAR values for statistical analysis. Following the WHO criteria for blindness, poor final vision was determined as logMAR worse than 1.30 (equivalent to Snellen 20/400).10 Patients were categorized into two groups based on their BCVA: a good VA group (logMAR < 1.30, equivalent to Snellen 20/400) and a poor VA group (logMAR ≥ 1.30). Additional data recorded included the interval between hospital discharge and the first follow-up, the period between the first and last follow-up, and the duration between primary and secondary procedures when applicable.
Statistical Analysis
Normality of continuous variables was assessed using the Shapiro–Wilk test. Variables with normal distribution were presented as mean ± standard deviation (SD) and compared using the independent Student’s t-test, while non-normally distributed variables were presented as median (interquartile range, IQR) and analyzed using the Mann–Whitney U-test. Categorical variables were analyzed using Fisher’s exact test due to small expected cell counts. For categorical variables with more than two categories, the Fisher–Freeman–Halton exact test with Monte Carlo simulation was applied.
Poor final visual outcome was defined as best-corrected visual acuity (BCVA) ≥ 1.30 logMAR (equivalent to Snellen 20/400). A multivariable logistic regression model was constructed to identify independent predictors of poor visual outcome, with variables selected while respecting the recommended minimum of 5–9 events per predictor variable.11 Due to the retrospective nature of the study and the rarity of intraocular foreign body cases, all eligible patients during the study period were included using consecutive sampling, and no a priori sample size calculation was performed. Data analysis was conducted using IBM SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05.
Patient and Public Involvement
Patients and the public were not involved in the design, conduct, reporting, or dissemination plans of this retrospective cohort study.
Results
Of the 55 patients with IOFB, 46 participants (46 eyes) were included in the study. Excluded cases were those with a follow-up duration of less than 3 months (n = 2), missing medical records (n = 2), incomplete baseline examination data (n = 3), and eyes that underwent evisceration following IOFB removal (n = 2) (Figure 1). Two eyes were eviscerated due to post-traumatic endophthalmitis with scleral abscess and panophthalmitis. The patient age ranged from 9 to 59 years old, with a mean age of 32.78 ± 12.68. Subjects were dominated by males (93.5%) rather than females (6.5%). Foreign bodies were equally distributed between the right and left eyes, with 23 cases each (Table 1).
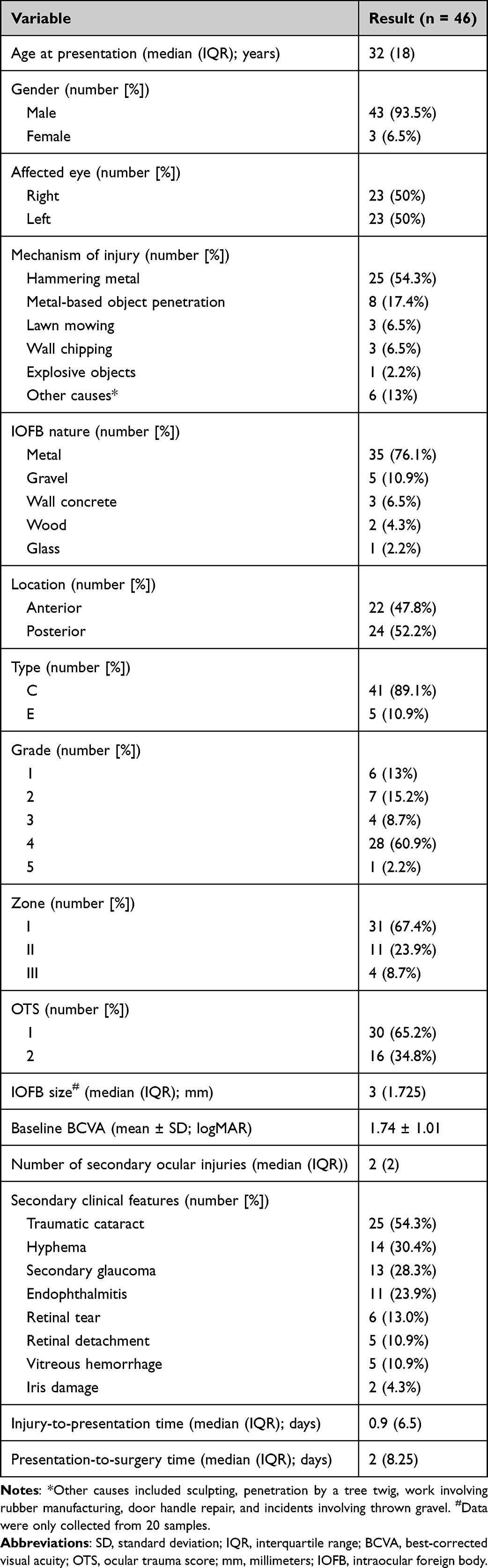 |
Table 1 Baseline Demographics and Clinical Characteristics |
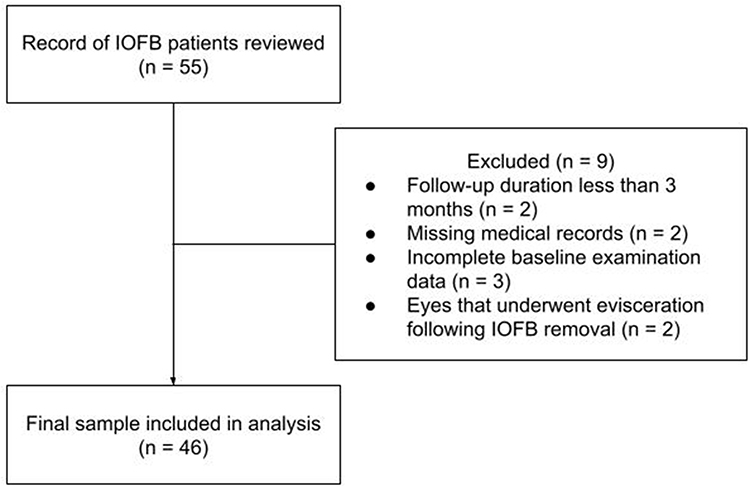 |
Figure 1 Flow diagram showing the patient selection process. |
The leading cause of IOFBs was metal-related injuries from welding (54.3%), followed by metal foreign body penetration (17.4%), lawn mowing (6.5%), wall chipping (6.5%), and explosive objects (2.2%), with other causes accounting for 13%. In terms of the material of the foreign bodies, metal was responsible for 76.1% of cases, followed by gravel (10.9%), wall concrete (6.5%), wood (4.3%), and glass (2.2%).
The cornea was the most common site of entry for IOFBs, accounting for 67.4% of cases, followed by the sclera at 19.6% and the corneoscleral junction at 13%. The size of the foreign bodies, as measured through CT scans, varied between 1 and 9 mm, with an average of 3.79 ± 2.38 mm. On initial presentation, the mean BCVA was 1.74 ± 1.01 logMAR. Traumatic cataract was the most frequently observed complication (54.3%), with other common complications including hyphema (30.4%), secondary glaucoma (28.3%), endophthalmitis (23.9%), retinal tears (13.0%), retinal detachment (10.9%), vitreous hemorrhage (10.9%), and iris damage (4.3%).
The median duration from the occurrence of the injury to the patient’s initial presentation at our eye center was 0.9 days (IQR: 6.5 days). Following the presentation, the median time to IOFB removal was 2 days (IQR: 8.25 days).
Univariate analysis revealed poor final BCVA to be significantly associated with several factors (Table 2), including larger IOFB size (p < 0.05), lower baseline BCVA (p < 0.001), higher secondary ocular injuries (p < 0.01), and the presence of complications such as traumatic cataract (p < 0.02), secondary glaucoma (p < 0.04), and endophthalmitis (p < 0.02). Furthermore, lensectomy (p < 0.01) was significantly associated with poorer visual outcomes. OTCG Grade classification was significantly associated with final visual outcome, with better outcomes in Grades 1–3 and worse outcomes in Grades 4–5 (Fisher–Freeman–Halton exact test via Monte Carlo simulation, p = 0.013, 99% CI [0.012, 0.014]). Significant association between OTS score and final visual acuity was demonstrated, with higher OTS scores (Score 2) correlating with better visual outcomes (p < 0.001).
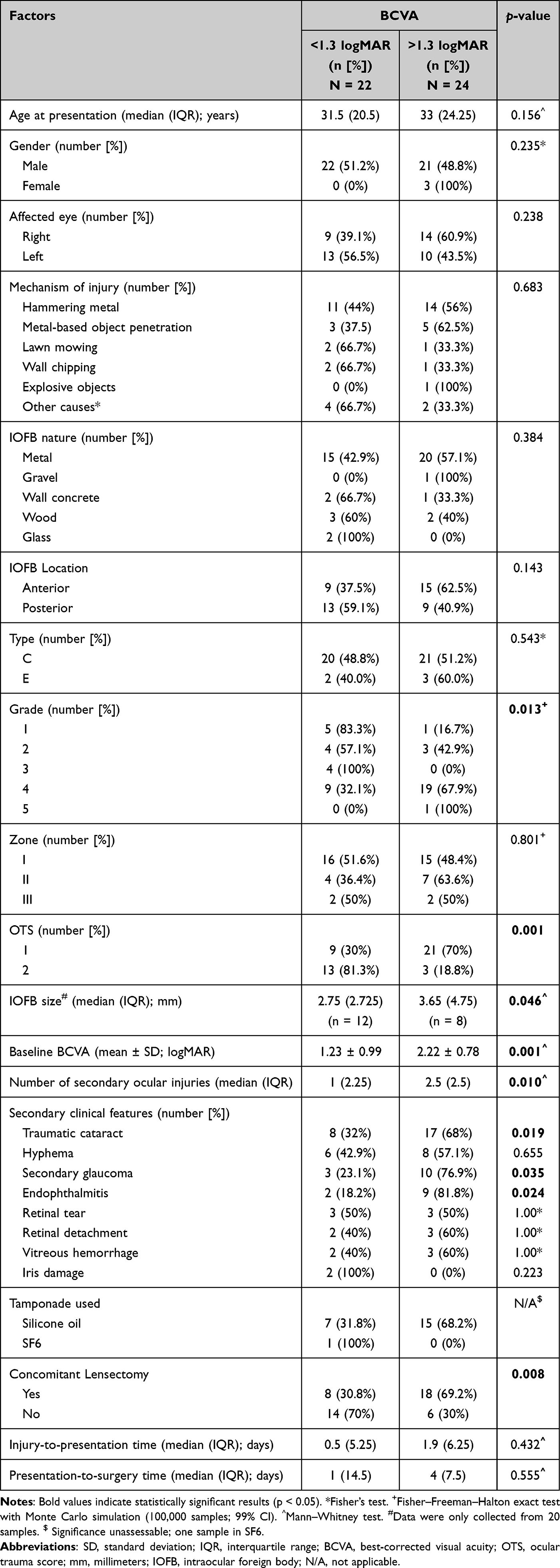 |
Table 2 Univariate Analysis of Factors Affecting Visual Outcomes in IOFB Patients |
A multiple logistic regression analysis was conducted to identify independent risk factors for poor visual outcomes (Table 3). Significant predictors of poor final BCVA (BCVA > 1.3 logMAR) were a worse initial BCVA (p < 0.005) and concomitant lensectomy surgery (p < 0.03).
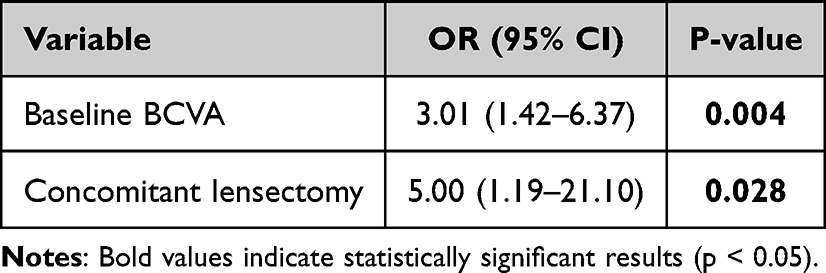 |
Table 3 Multivariate Analysis of Categorical Risk Factors Associated with Worse Final BCVA in IOFB Patients |
Discussion
Intraocular foreign bodies (IOFBs) remain a major contributor to vision loss in cases of open globe injury (OGI). Vision impairment results from direct mechanical trauma to ocular structures, infection, toxic effects of iron and copper, and secondary ocular pathologies such as retinal detachment, traumatic optic neuropathy, and glaucoma, which can ultimately cause permanent visual damage.3,12
A major contributing factor is the inadequate use of protective eyewear during high-risk activities, particularly in manual labor occupations.13,14 This is evident in the predominance of male patients in our study, which is consistent with previous studies that report similar gender trends.8,15–17 Such a trend is likely attributed to the higher involvement of males in occupations, which increases the risk for such injuries. Furthermore, the mean age in our study (32.78 ± 12.68 years) falls within the working-age range, further supporting this association. Although our study found no significant association between age and final BCVA, multiple reports have shown that visual improvement tends to be less favorable in patients aged ≥ 50 years.17,18 Moreover, older people are at higher risk of post-traumatic endophthalmitis, which could worsen visual prognosis if not given proper care.2,19
Further analysis of injury causes showed that welding accidents were the most common (54.3%), followed by accidental penetrations involving metal objects. This finding also explains why most detected IOFBs in our center were metallic (76.1%). Most published articles also found metals to be the most common IOFB material (75.7–89%).8,15,16 The most common metallic IOFB materials are iron, lead, nickel, copper, aluminum, and zinc. Some of these substances can cause more complications, such as chalcosis (copper) and siderosis bulbi (iron). Furthermore, earlier research suggested that metallic IOFBs were more likely to cause poor visual outcomes (> 1.00 logMAR) if located posteriorly. The predominance of metal-related IOFBs in young adult males underscores the need for targeted occupational safety interventions, such as mandatory use of protective eyewear in high-risk jobs like welding and construction. On the other hand, non-metallic IOFBs tend to minimize visual improvement due to their high risk of post-trauma endophthalmitis, which is significantly associated with poor BCVA in this and prior research.2,20
Earlier studies have suggested larger IOFB size or larger entrance wound as a significant predictor of poor BCVA, and our findings were consistent, with a mean IOFB size of 3.79 ± 2.38 mm.15,17,21 However, our multivariate analysis did not identify IOFB size as an independent risk factor for worse final VA. Liu et al proposed that larger size increases the risk of complications, such as traumatic cataract, uveal prolapse, and hemorrhage, which may explain why size alone does not serve as an independent risk factor.17
The association between final BCVA and the presentation-to-surgery time has been inconsistent across studies. Previously, delayed surgery was considered crucial for preserving vision, with delayed intervention recommended only for younger patients due to the challenges of posterior hyaloid removal and the high risk of intraoperative hemorrhage in inflamed eyes.17,22 In contrast, our study found no significant association between delayed presentation and final BCVA, consistent with findings by Wickham et al and Rozon et al16,23 Although our center prioritizes IOFB removal within 24 hours of initial examination, especially when resources allow, several cases were managed beyond this timeframe. Thus, the impact on visual outcomes may be more closely related to injury-to-presentation time. However, similar to Liu et al, this study found no significant association in this regard.17 Regarding the risk of developing endophthalmitis from delayed surgery, Colyer et al observed that satisfactory visual outcomes can be achieved with delayed surgery when combined with systemic and topical antibiotic coverage, without a marked increase in the risk of endophthalmitis or other serious complications.24 However, later studies identified that delayed surgery and initial management are significant factors in the development of endophthalmitis, suggesting that delaying intervention should be reconsidered, particularly in situations where timely treatment is possible, to reduce the risk of endophthalmitis and improve visual outcomes.25,26
The presence of complications in IOFB was associated with poorer visual outcomes in our study, with a higher number of complications significantly correlating with reduced final VA. Traumatic cataracts, endophthalmitis, and secondary glaucoma were among the complications most strongly linked to worse outcomes. Endophthalmitis, known to be a severe issue in open globe injuries, has been reported in up to 34% of IOFB cases.27 Although glaucoma is less common, it poses a risk of irreversible vision loss if left untreated. After adjusting for other variables, no individual complication emerged as an independent prognostic factor for the final BCVA. The severity and specific types of complications likely had a greater influence on visual outcomes, which may explain the lack of significance in the multivariate analysis. In the case of secondary glaucoma, the nonsignificant result may be attributed to the fact that almost half of our patients were treated with silicone oil tamponade, which is known to contribute to secondary glaucoma, potentially influencing the findings.
Traumatic cataract was the most common complication in our study. Surgery is typically performed early, alongside laceration repair in open globe injuries, or later in a stabilized eye. Early lensectomy is generally recommended to prevent complications like glaucoma, lens particle-induced uveitis, and inflammation.28 Despite most patients in our study undergoing early lensectomy, our multivariate analysis identified that performing lensectomy as part of the primary procedure was associated with poorer final visual outcomes, an association that has been infrequently reported in prior studies. It is imperative to distinguish the observed association between concomitant lensectomy and poorer visual outcomes from a causal relationship, as lensectomy may reflect greater injury severity or surgical complexity. Plausible mechanisms include increased surgical trauma, elevated intraocular inflammation, and additional intraoperative stress. Memon et al preferred lensectomy as a secondary procedure to minimize risk of postoperative inflammation.29 Furthermore, the eye may not be optimally stable during the primary repair, leading to greater challenges in fully clearing lens material, managing intraocular pressure, and preserving the integrity of surrounding structures. These factors could contribute directly to poorer visual outcomes, even after adjusting for the severity of the initial trauma.
Timing of surgery depends on several factors, including the patient’s overall condition, the mechanism of injury, the IOFB’s composition and location, and available resources. Prompt surgery can lower the risk of endophthalmitis and proliferative vitreoretinopathy, particularly in contaminated injuries. However, primary globe closure and systemic antibiotics should be prioritized in hemodynamically unstable patients, with IOFB extraction postponed. Delayed removal may help manage inflammation, provide better visualization for intraocular evaluation, and benefit from spontaneous posterior vitreous detachment, which can facilitate surgery. Still, if the IOFB is contaminated, delaying surgery increases the risk of infection.3,30
Other factors to consider in IOFB management include the difficulty in localizing entry sites, particularly when no external wound is visible, which can delay diagnosis and management. A case has been reported where the entry site was undetectable, yet delayed intervention still resulted in favorable visual recovery.31 Detection is further complicated by non-metallic IOFBs, such as vegetable matter, plastic, or glass, which are less apparent on conventional imaging and require multimodal imaging and thorough clinical assessment.
The object’s size, material, location, and any coexisting ocular damage determine the surgical approach. Small metallic IOFBs (less than 1 mm) can often be extracted using an intraocular magnet, while non-metallic ones may need a vitreous cutter. Forceps are typically used for medium-sized IOFBs (1–3 mm), whereas larger or glass fragments may require diamond-coated forceps. IOFBs located in the anterior chamber are usually removed through a secondary limbal incision instead of the original entry site, and pars plana vitrectomy is often unnecessary in such cases. The primary objective is to limit further trauma and maintain ocular structure.3,30
Our study is limited by its retrospective nature, which may introduce selection bias and limit the ability to control for confounding variables. Although the sample size was adequate for statistical analysis, the single-center nature of this study and the limited number of cases may reduce the generalizability of the findings. Additionally, the lack of long-term follow-up data prevents us from assessing the full impact of certain complications, particularly those that manifest over extended periods. These limitations should be considered when interpreting the observed associations, particularly regarding surgical factors such as lensectomy, as residual confounding by injury severity or surgical complexity cannot be fully excluded.
Despite its limitations, this study identifies poor baseline BCVA and the need for concomitant lensectomy as independently associated with poor visual outcomes in IOFB cases, supporting their use in early prognostication and patient counseling. These findings provide clinically relevant insights into IOFB management in similar tertiary referral or resource-limited settings, where early risk stratification may help prioritize high-risk patients for timely referral, individualized timing of additional procedures, and closer postoperative monitoring. The high rate of complications such as traumatic cataract, secondary glaucoma, and endophthalmitis also highlights the need for early detection and integrated management in post-traumatic care. The short median injury-to-presentation and presentation-to-surgery time underscores the importance of equipping primary care and peripheral centers to promptly recognize and refer IOFB cases. Our findings also reinforce the need for improved protective measures and public awareness, particularly among high-risk occupational groups. Further prospective, multicenter studies are needed to validate these findings and explore strategies to improve visual prognosis in such injuries. These conclusions were derived from a single-center retrospective cohort, and should be interpreted accordingly.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of University of Indonesia (protocol code 24-12-1903 – February 07, 2025).
Acknowledgments
Presentation: Asia-Pacific Ophthalmic Trauma Society (APOTS) Meeting – November 8-10, 2024.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Pieramici DJ, Sternberg P, Aaberg TM, et al. A system for classifying mechanical injuries of the eye (globe). The Ocular Trauma Classification Group. Am J Ophthalmol. 1997;123(6):820–11. doi:10.1016/S0002-9394(14)71132-8
2. Duan F, Yuan Z, Liao J, Zheng Y, Yang Y, Lin X. Incidence and risk factors of intraocular foreign body-related endophthalmitis in Southern China. J Ophthalmol. 2018;2018:1–5. doi:10.1155/2018/8959108
3. Loporchio D, Mukkamala L, Gorukanti K, Zarbin M, Langer P, Bhagat N. Intraocular foreign bodies: a review. Surv Ophthalmol. 2016;61(5):582–596. doi:10.1016/j.survophthal.2016.03.005
4. Zhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in China: clinical characteristics, prognostic factors, and visual outcomes in 1421 eyes. Am J Ophthalmol. 2011;152(1):66–73.e1. doi:10.1016/j.ajo.2011.01.014
5. Ehlers JP, Kunimoto DY, Ittoop S, Maguire JI, Ho AC, Regillo CD. Metallic intraocular foreign bodies: characteristics, interventions, and prognostic factors for visual outcome and globe survival. Am J Ophthalmol. 2008;146(3):427–433.e2. doi:10.1016/j.ajo.2008.05.021
6. Yeh S, Colyer MH, Weichel ED. Current trends in the management of intraocular foreign bodies. Curr Opin Ophthalmol. 2008;19(3):225–233. doi:10.1097/ICU.0b013e3282fa75f1
7. Ohlhausen M, Menke BA, Begley J, et al. Advances in the management of intraocular foreign bodies. Front Ophthalmol. 2024;4(1):1422466. doi:10.3389/fopht.2024.1422466
8. Liang Y, Liang S, Liu X, Liu D, Duan J. Intraocular foreign bodies: clinical characteristics and factors affecting visual outcome. J Ophthalmol. 2021;2021:1–9. doi:10.1155/2021/9933403
9. Widjaja SA, Hiratsuka Y, Ono K, Yustiarini I, Nurwasis N, Murakami A. Ocular trauma trends in Indonesia: poor initial uncorrected visual acuity associated with mechanism of injury. Open Access Maced J Med Sci. 2020;9(B):903–908. doi:10.3889/oamjms.2021.6862
10. Lee SY, Gurnani B, Mesfin FB. Blindness. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. http://www.ncbi.nlm.nih.gov/books/NBK448182/.
11. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and cox regression. Am J Epidemiol. 2007;165(6):710–718. doi:10.1093/aje/kwk052
12. Usgaonkar UPS, Shirodkar RM. Intra ocular foreign bodies (IOFBs): a review. Kerala J Ophthalmol. 2023;35(3):243. doi:10.4103/kjo.kjo_67_23
13. Bourke L, Bourke E, Cullinane A, O’Connell E, Idrees Z. Clinical outcomes and epidemiology of intraocular foreign body injuries in Cork University Hospital, Ireland: an 11-year review. Ir J Med Sci. 2021;190(3):1225–1230. doi:10.1007/s11845-020-02443-9
14. Kousiouris P, Gouliopoulos N, Kourtesa A, et al. The demographic and social characteristics of patients with ocular foreign bodies in a Greek tertiary hospital. Clin Ophthalmol. 2022;16:2323–2328. doi:10.2147/OPTH.S370188
15. Watanachai N, Choovuthayakorn J, Nanegrungsunk O, et al. Intraocular foreign body: characteristics, visual outcomes, and predictive values of ocular trauma score. Heliyon. 2023;9(10):e20640. doi:10.1016/j.heliyon.2023.e20640
16. Rozon JP, Lavertu G, Hébert M, et al. Clinical characteristics and prognostic factors of posterior segment intraocular foreign body: canadian experience from a tertiary university hospital in Quebec. J Ophthalmol. 2021;2021:1–7. doi:10.1155/2021/9990290
17. Liu Y, Wang S, Li Y, Gong Q, Su G, Zhao J. Intraocular foreign bodies: clinical characteristics and prognostic factors influencing visual outcome and globe survival in 373 eyes. J Ophthalmol. 2019;2019:1–7. doi:10.1155/2019/5208092
18. Sternberg P, de Juan E, Michels RG, Auer C. Multivariate analysis of prognostic factors in penetrating ocular injuries. Am J Ophthalmol. 1984;98(4):467–472. doi:10.1016/0002-9394(84)90133-8
19. Thompson JT, Parver LM, Enger CL, Mieler WF, Liggett PE. Infectious endophthalmitis after penetrating injuries with retained intraocular foreign bodies. National Eye Trauma System. Ophthalmology. 1993;100(10):1468–1474. doi:10.1016/s0161-6420(93)31454-5
20. Liu X, Bai Q, Song X. Clinical and imaging characteristics, outcomes and prognostic factors of intraocular foreign bodies extracted by vitrectomy. Sci Rep. 2023;13(1):14136. doi:10.1038/s41598-023-41105-5
21. Liu CCH, Tong JMK, Li PSH, Li KKW. Epidemiology and clinical outcome of intraocular foreign bodies in Hong Kong: a 13-year review. Int Ophthalmol. 2017;37(1):55–61. doi:10.1007/s10792-016-0225-4
22. Wani VB, Al-Ajmi M, Thalib L, et al. Vitrectomy for posterior segment intraocular foreign bodies: visual results and prognostic factors. Retina. 2003;23(5):654–660. doi:10.1097/00006982-200310000-00008
23. Wickham L, Xing W, Bunce C, Sullivan P. Outcomes of surgery for posterior segment intraocular foreign bodies--a retrospective review of 17 years of clinical experience. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2006;244(12):1620–1626. doi:10.1007/s00417-006-0359-6
24. Colyer MH, Weber ED, Weichel ED, et al. Delayed intraocular foreign body removal without endophthalmitis during operations Iraqi Freedom and Enduring Freedom. Ophthalmology. 2007;114(8):1439–1447. doi:10.1016/j.ophtha.2006.10.052
25. Chaudhry IA, Shamsi FA, Al-Harthi E, Al-Theeb A, Elzaridi E, Riley FC. Incidence and visual outcome of endophthalmitis associated with intraocular foreign bodies. Graefes Arch Clin Exp Ophthalmol. 2008;246(2):181–186. doi:10.1007/s00417-007-0586-5
26. Parke DW, Pathengay A, Flynn HW, Albini T, Schwartz SG. Risk factors for endophthalmitis and retinal detachment with retained intraocular foreign bodies. J Ophthalmol. 2012;2012(1):758526. doi:10.1155/2012/758526
27. Nicoară SD, Irimescu I, Călinici T, Cristian C. Outcome and prognostic factors for traumatic endophthalmitis over a 5-year period. J Ophthalmol. 2014;2014(1):747015. doi:10.1155/2014/747015
28. Tabatabaei SA, Rajabi MB, Tabatabaei SM, Soleimani M, Rahimi F, Yaseri M. Early versus late traumatic cataract surgery and intraocular lens implantation. Eye. 2017;31(8):1199–1204. doi:10.1038/eye.2017.57
29. Memon MN, Narsani AK, Nizamani NB. Visual outcome of unilateral traumatic cataract. J Coll Physicians Surg--Pak. 2012;22(8):497–500.
30. Jung HC, Lee SY, Yoon CK, Park UC, Heo JW, Lee EK. Intraocular foreign body: diagnostic protocols and treatment strategies in ocular trauma patients. J Clin Med. 2021;10(9):1861. doi:10.3390/jcm10091861
31. Rai BB, Dorji S, Zangmo P, Tshering T. Retained intraocular metallic foreign body causing retinal detachment. Bhutan Health J. 2016;2(1):34–37. doi:10.47811/bhj.23
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.