Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Clinical and Onychoscopic Features of Benign and Malignant Conditions in Longitudinal Melanonychia in the Thai Population: A Comparative Analysis
Authors Kungvalpivat P, Rojhirunsakool S, Chayavichitsilp P, Suchonwanit P ![]() , Wichayachakorn CT, Rutnin S
, Wichayachakorn CT, Rutnin S ![]()
Received 21 September 2020
Accepted for publication 9 November 2020
Published 19 November 2020 Volume 2020:13 Pages 857—865
DOI https://doi.org/10.2147/CCID.S283112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Pintusorn Kungvalpivat,1 Salinee Rojhirunsakool,1,2 Pamela Chayavichitsilp,1 Poonkiat Suchonwanit,1 Chanitwan T Wichayachakorn,1 Suthinee Rutnin1
1Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Skin Center, Srinakharinwirot University, Bangkok, Thailand
Correspondence: Suthinee Rutnin
Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Ratchathewi, Bangkok, 10400, Thailand
Tel +66-2-2011141
Fax +66-2-201-1211 Ext 4
Email [email protected]
Background: Longitudinal melanonychia can arise from many underlying conditions, both benign and malignant. Practitioners tend to be reluctant to perform a biopsy of this condition due to procedure-related pain and the possibility of permanent nail dystrophy. Onychoscopy has become a useful tool to provide a provisional diagnosis and assist in deciding on a nail biopsy.
Objective: To investigate and differentiate the clinical and onychoscopic features of subungual melanoma (SUM)/subungual melanoma in situ (SMIS) and other benign melanocytic conditions (BM).
Materials and Methods: In this cross-sectional study, a total of 32 cases of longitudinal melanonychia were examined, and baseline characteristics were recorded. Onychoscopic pictures were taken by handheld dermoscopy with 10x and 50x magnification. A biopsy was then performed in each case, and a pathological diagnosis was obtained.
Results: Of the 32 cases, 6 were diagnosed with SMIS and 26 with BM (21 simple lentigines, 5 junctional nevi). The median age was significantly higher among the SMIS group (56 vs 31 years) (p = 0.034). Regarding onychoscopic findings, cases with SMIS were significantly associated with a greater band width percentage (p = 0.014), multicolor presentation (p = 0.005), the presence of granular pigmentation (p = 0.034), and micro-Hutchinson’s sign (p = 0.015). In addition, subungual hyperkeratosis, a newly recognized onychoscopic feature, was more significantly associated with SMIS in comparison to BM (p = 0.002).
Conclusion: Onychoscopy provides useful information to aid in the differential diagnosis of longitudinal melanonychia. From our study, onychoscopy can be utilized to assist in making a decision whether to perform a biopsy in patients with longitudinal melanonychia suspicious of malignant melanocytic conditions.
Keywords: longitudinal melanonychia, subungual melanoma, subungual melanoma in situ, onychoscopy, dermoscopy
Introduction
Cutaneous malignant melanoma is a leading cause of death related to skin cancer. Superficial spreading melanoma is the most common subtype in Caucasians, accounting for approximately 70%,1 while acral lentiginous melanoma (ALM) is most common among Asians and African Americans, accounting for 41.8–65% of all melanoma cases.2–6 ALM is associated with poor prognosis, with 5-year survival rates of 80.6% compared to 93.0% in overall cutaneous melanoma.7 Moreover, a study by Ingkaninanda et al showed that ALM was the most common histologic subtype (76.7%) among Thai patients, most being diagnosed at a locally advanced stage, and subungual site was an independent risk factor relating to worse prognosis.8 Thus, early detection and prompt management are crucial to minimize morbidity and mortality.
Subungual melanoma is considered a subcategory of ALM. Longitudinal melanonychia is a common initial presentation of subungual melanoma in situ (SMIS), an early stage of subungual melanoma, as well as SUM. Other differential diagnoses of longitudinal melanonychia include benign and malignant melanocytic conditions, drug-induced nail hyperpigmentation, systemic illness-induced nail hyperpigmentation, subungual hematoma, onychomycosis and Bowen’s disease.9 Definitive diagnosis of SUM is made based on histopathology. However, practitioners tend to be reluctant to perform a nail biopsy due to the pain associated with the procedure and the possibility of permanent nail dystrophy.
Clinical evaluation using the ABCDEF rule proposed by Levit et al in 200010 can guide the differential diagnosis; however, fewer than half of the practitioners were familiar with this mnemonic, and a previous study showed low sensitivity of diagnosis associated with this rule.11,12 In addition to clinical assessment, onychoscopy has become an additional tool to provide a provisional diagnosis. However, limited studies on onychoscopic findings among malignant and benign melanocytic conditions have been published.9,11,13–17 The goal of our study is to investigate and differentiate the clinical and onychoscopic features of malignant melanocytic lesions (SUM/SMIS) and other benign melanocytic conditions (BM) in the Thai population.
Materials and Methods
This is a cross-sectional study in which patients with longitudinal melanonychia suspicious for SUM/SMIS were included from the Division of Dermatology in Ramathibodi Hospital between May 1, 2018 and September 30, 2019. Inclusion criteria included patients with histopathological confirmation of benign and malignant melanocytic conditions (Figure 1). Exclusion criteria included individuals who had previous nail injury or any nail procedure within one month, those suspected of drug- or systemic-induced melanonychia or had final histopathological diagnosis as nonmelanocytic conditions. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Committee on Human Rights Related to Research Involving Human Subjects from Faculty of Medicine Ramathibodi Hospital, Mahidol University (ID 03–61-08).
 |
Figure 1 Representative histopathological pictures: (A) Atypical melanocytic proliferation singly and in nests at and above the dermoepidermal junction in subungual melanoma in situ (H&Ex400). (B) An increased number of single melanocytes along the basal cell layer and increased melanin production in simple lentigine (H&E x400). (C) Nest of melanocytes at the dermoepidermal junction in junctional nevus (H&Ex400). |
History and physical examination were obtained and recorded. Prior to nail biopsy, photographs of longitudinal melanonychia were taken using a pocket dermoscope (DermLite® DL3, 3 Gen Inc., CA, USA) and a handheld digital microscope (Dino-Lite®, AnMo Electronics Corp., Taiwan) with 10x and 50x magnification, respectively, focusing on both proximal and lateral nail fold, nail plate and hyponychium. The nail matrix and nail bed were explored intraoperatively, and prominent or most proximal pigmented lesions were chosen for histopathology by tangential biopsy.
The onychoscopic features that were used in assessment included width of pigmented band, width of nail plate, colors of the band (light brown, dark brown, gray, black), multicolor presentation (defined as ≥2 colors), brownish background, presence of granular pigmentation (defined as fine light to dark brown granularity)16 and homogeneity of band including parallelism, thickness and spaces between pigmented bands. The presence of splinter hemorrhage or blood spots was also evaluated. Nail plates and hyponychium were examined for nail plate dystrophy and subungual hyperkeratosis. Nail folds were also thoroughly reviewed for Hutchinson’s (defined as macroscopic periungual pigmentation of the proximal and lateral nail fold or hyponychium), micro-Hutchinson’s (defined as pigmentation of the cuticle seen on onychoscopy but not with naked eye) and pseudo-Hutchinson’s signs (defined as pigmentation of the nail matrix observed through the transparent cuticle at the proximal nail fold). Thereafter, all photographs were evaluated by a blinded dermatologist and histopathological results were confirmed by another blinded dermatopathologist.
Statistical Analysis
Statistical analysis was performed using Stata 14.0 (StataCorp LLC, TX, USA). Continuous variables were expressed as medians with interquartile ranges (IQRs) and were analyzed using Wilcoxon’s rank-sum test. Categorical variables were expressed as proportions and were analyzed using the chi-squared test. A p value <0.05 was considered statistically significant.
Results
Patients’ Demographic Data
From a total of 33 cases, one case was excluded due to histopathological diagnosis of Bowen’s disease. Demographic data are shown in Table 1. Six of 32 cases (18.75%) had SMIS and 26 cases (81.25%) had BM (21 simple lentigines, 5 junctional nevi). None had SUM. Patients with SMIS had a median age of 56 versus 31 years in the BM group (p = 0.034). Patients in the SMIS group had significantly darker skin types with Fitzpatrick skin type 5 (p < 0.001). There were no statistically significant differences in sex or duration of melanonychia (median of 18 vs 24 months, p = 0.747). There was no predilection of affected digits in SMIS cases, but the occurrence of SMIS was higher on fingernails than toenails. No family history of melanoma was present in the SMIS group, while one case was found in the BM group (p = 1.000). A history of nail trauma was elicited in 2 patients in the SMIS group, while 5 of the 26 in the benign group were found to have prior nail trauma (p = 0.590).
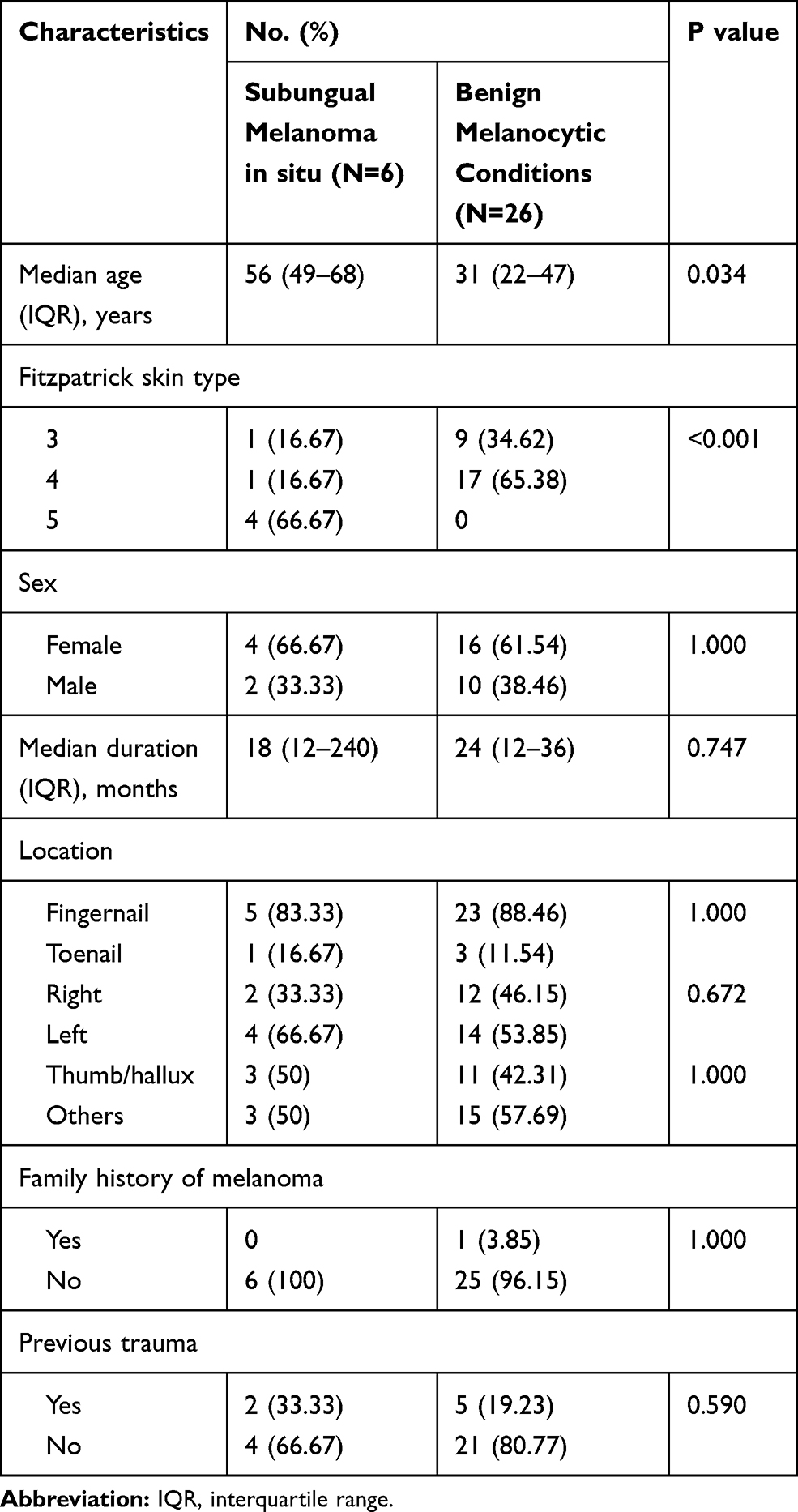 |
Table 1 Demographic Characteristics of 32 Patients Diagnosed with Subungual Melanoma in situ or Benign Melanocytic Conditions |
Onychoscopic Assessment
Patients with SMIS had a significantly wider pigmented band with a median of 6.69 mm versus 3.02 mm in patients with BM (p = 0.023) (Table 2). Similar to the median band width, the percentage of pigmented bands on the nail plate in the SMIS group was significantly higher than that in the BM group (65.11 vs 26.96%, p = 0.014) (Figure 2). All cases with SMIS had multiple colors in longitudinal melanonychia with a median of 2.5 colors versus single color in cases with BM (p = 0.005) (Figure 3). The most prominent color in the SMIS group was black (6/6, 100%), followed by dark brown (4/6, 66.67%), while dark brown (15/26, 57.7%) was the most common color in BM, followed by light brown (12/26, 46.2%). Most cases in both groups showed brownish backgrounds (p = 1.000). Three of 6 patients with SMIS (50%) had granular pigmentation versus 2 of 26 (7.69%) in the BM (p = 0.034) (Figure 2). In terms of homogeneity of pigmented bands, including parallelism, thickness and spaces between bands, there was no significant difference between the two groups. There was no significant difference in nail plate dystrophy (33.33 vs 23.08%, p = 0.625). However, subungual hyperkeratosis was significantly associated with SMIS (66.67% vs 3.85%, p = 0.002) (Figure 4). Only one patient with SMIS had Hutchinson’s sign versus none in the BM group. Interestingly, micro-Hutchinson’s signs were detected in 3 more cases and showed a significant association with SMIS (p = 0.015) (Figure 5). Eight of 26 cases with BM had pseudo-Hutchinson’s sign versus none in the SMIS group (p = 0.296). The presence of blood, both splinter hemorrhage and blood spots, was not associated with either SMIS or BM by statistical analysis.
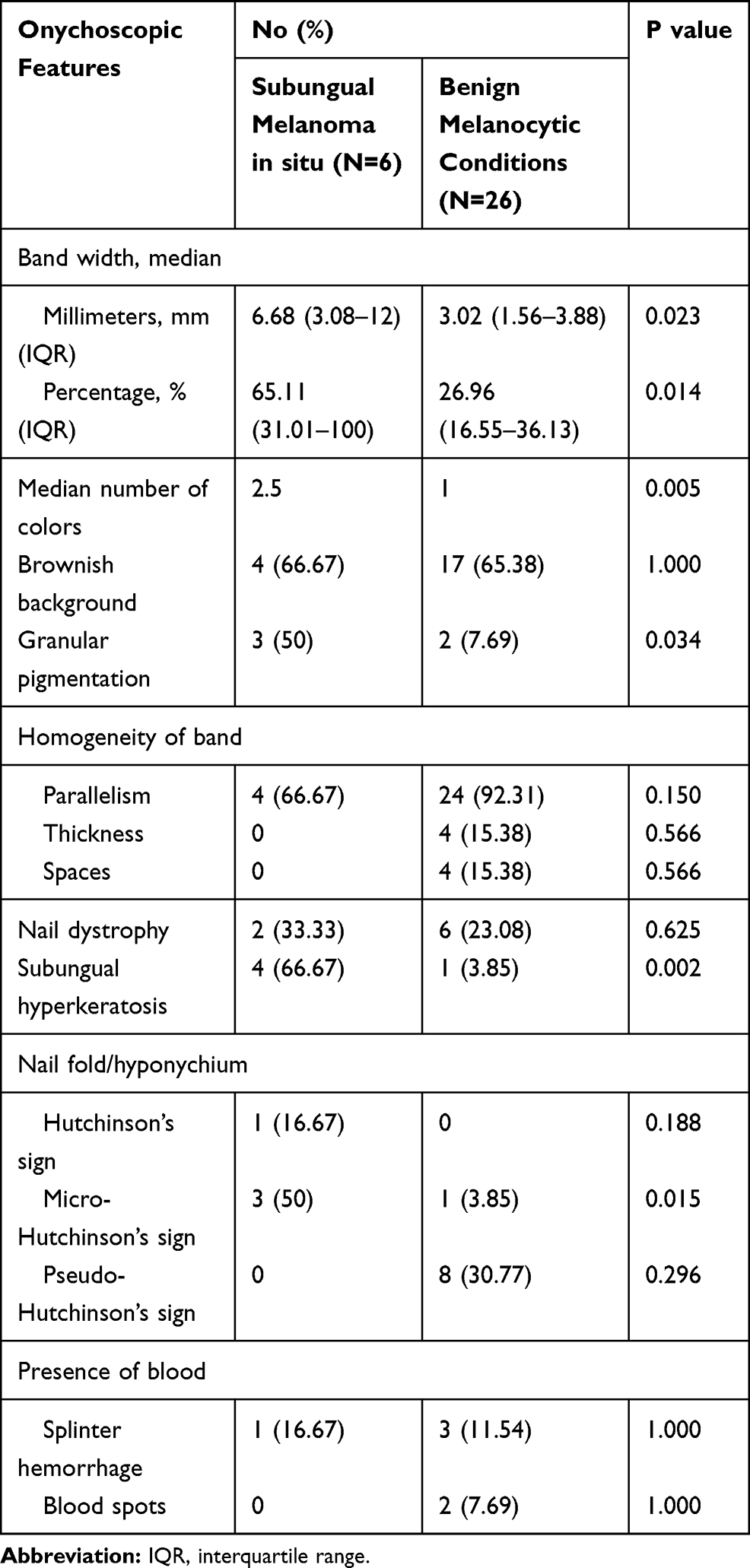 |
Table 2 Comparison of Onychoscopic Features of Longitudinal Melanonychia Between Subungual Melanoma in situ and Benign Melanocytic Conditions |
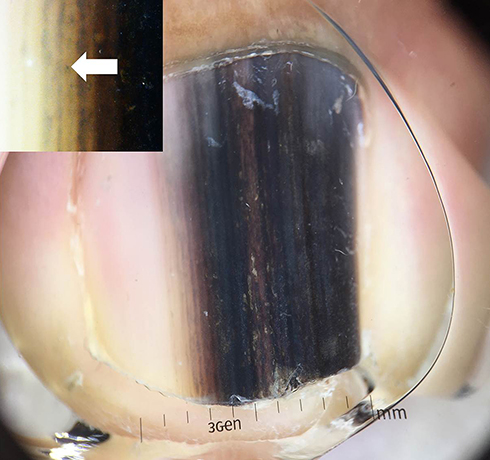 |
Figure 2 Subungual melanoma in situ of the right thumb in a 58-year-old male showing an 8.7-mm band width, involving 67% of nail plate and a mixture of dark brown and black color. Inset, granular pigmentation examined by handheld microscopy with 50x magnification (white arrow). |
 |
Figure 3 Subungual melanoma in situ of the left second toenail in a 68-year-old female showing brown, gray and black colors. |
 |
Figure 4 Distal edge onychoscopy in subungual melanoma in situ of the right thumb in a 58-year-old male showing subungual hyperkeratosis. |
 |
Figure 5 Onychoscopic picture showing micro-Hutchinson’s sign in subungual melanoma in situ of the right thumbnail in a 36-year-old male. |
Discussion
In patients presenting with longitudinal melanonychia, early detection and prompt treatment of SMIS is essential to minimize the morbidity and mortality associated with subungual melanoma. SMIS is definitively diagnosed via nail matrix biopsy with histopathological confirmation. However, the procedure is invasive and carries a high risk for permanent nail dystrophy. In addition to clinical assessment, onychoscopy has become a useful tool to help distinguish malignant from benign etiologies of longitudinal melanonychia and to determine the necessity of nail matrix biopsy. Several studies have described onychoscopic findings associated with SUM and SMIS.9,13,14,18–20 However, no universally accepted guidelines have been established.
In this study, the age of onset in the SMIS group was significantly older than that in the BM group, with a median age of 56 versus 31 (p = 0.034), consistent with previous studies that reported a high incidence during the fifth to seventh decades of life.2,10,21,22 In contrast, Ko et al11 reported a younger age group of SMIS with a mean age of 36.1 years, and they advocated that younger adults should also be screened for SMIS. Similar to prior studies,11,17 this study did not find any association with gender and diagnosis, but female patients were slightly higher in number than male patients in both SMIS and BM conditions.
In our study, Fitzpatrick’s skin type 5 was significantly associated with SMIS, supporting previous studies that mentioned that ALM was commonly found among deeply pigmented skin.21,23,24 Thumb, followed by hallux, were previously reported as the most commonly affected digits;10,22,24–26 however, our study as well as more recent studies did not find any of the digits affected.11,17 Therefore, digit affected may not aid in the differentiation between malignant and benign causes of melanonychia.
Regarding the onset of melanonychia, patients with SMIS had a shorter median duration of 18 months versus 24 months in patients with BM (p = 0.746), following a similar trend as a previous study.17 Trauma and family history of melanoma have been reported as risk factors for SMIS;9,10,27 however, our study did not find any aforementioned association. The small number of SMIS cases may explain this.
In terms of onychoscopic assessment, the width of the pigmented band is an important risk factor associated with SMIS. Based on the ABCDEF rule by Levit et al, a minimum width of 3 mm has been used in detecting SMIS.10 In our study, patients with BM had a median band width of 3.02 mm; however, the SMIS group had a significantly wider pigmented band with a median of 6.69 mm (p = 0.023). These findings were consistent with a recent study by Ohn et al,17 which demonstrated that a 6 mm minimum width was more strongly associated with SMIS than a minimum of 3 mm. Similar to median band width, the percentage of width of pigment to the total nail width was greater in the SMIS group (65.11% compared to 26.95% in the BM group) (p = 0.014). Benati et al proposed width of pigmentation involving more than 2/3 of the nail plate as an important predictor of SUM.16 Later, a band width percentage cutoff of more than 40% was proposed by Ko et al to suggest SMIS over benign longitudinal melanonychia.11 In terms of pigmented band width measurement, we favor using band width percentage over band width in millimeters due to varying sizes of affected digits.
The multicolor pigmented band (defined as ≥2 colors) was significantly associated with SMIS (p = 0.024) with a median number of colors of 2.5 (p = 0.004), similar to a prior study that found multicolor features as a significant feature in distinguishing between SMIS and BM.17 In terms of specific colors, there was no consensus among previous studies. One reported gray to be most specifically associated with SMIS, while another reported gray and black to be associated.16,17 Moreover, the ABCDEF criteria used brown-black pigmentation in the clinical mnemonic of SUM.10 In our study, all lesions diagnosed with SMIS had black color as one of the features, followed by dark brown color. Therefore, we suggest a multicolor band as a predictive feature of SMIS rather than the actual color of the band.
A brownish background was considered to be associated with melanocytic hyperplasia in both subungual nevi and melanoma in a previous study.13 However, our study showed no difference in background color between the two conditions. Moreover, loss of homogeneity of the pigmented band, including parallelism, thickness and spaces, was proposed as an important feature of SMIS.13,16,20,28 However, our study did not demonstrate the difference between benign and malignant conditions in terms of nonhomogeneity of the pigmented band. Recently, Ohn et al17 suggested evaluating malignant lesions from asymmetry by drawing a longitudinal midline and then comparing the pattern and pigmentation of the bisected halves. They claimed that this method might be more straightforward than evaluating the pattern of homogeneity.
Granular pigmentation, defined as the presence of fine light to dark brown colors, has been found more commonly among subungual melanoma and rarely in benign lesions.16 Half of the lesions in our study with SMIS also significantly demonstrated granular pigmentation (p = 0.034). This may be explained by irregularity of melanocytic activity resulting in variable melanin clumping. However, larger studies are still needed to prove the sensitivity and specificity of this feature.
Previous studies have mentioned the significance of nail plate dystrophy in differentiating between subungual melanoma and benign conditions.9,10,22 Benati et al mentioned that changes in the nail plate, including thinning, splitting, and partial and total absence of nail plate, could increase the risk of detecting subungual melanoma up to three times.16 However, our study did not find an association between nail dystrophy and SMIS, which could be due to the small number of cases in our study. In terms of hemorrhage, neither splinter hemorrhage nor blood spots could differentiate SMIS from BM in our study, similar to a previous study.13 The presence of blood was more suggestive of subungual hemorrhage. However, Phan et al found blood spots and linear microhemorrhages in 23% and 14% of patients with SUM, respectively.14 Thus, clinicians should keep a high suspicion for SUM/SMIS hidden under subungual hemorrhage.
To our knowledge, this study was the first to signify the importance of onychoscopic subungual hyperkeratosis in the recognition of SMIS. Our study showed that subungual hyperkeratosis is a statistically significant feature of SMIS. All patients with subungual hyperkeratosis underwent potassium hydroxide examination, nail clipping with periodic acid-Schiff staining and fungal culture and had negative results, excluding onychomycosis. This finding could be explained by the proposed pathogenesis in which melanoma cells influence the differentiation pattern of human epidermal keratinocytes in a way that causes an increase in highly aberrant suprabasal expression of keratin 14, which is normally present only in the basal cell layer, as well as the simultaneous absence of keratin 10, a marker of suprabasal terminally differentiated cells in the epithelium.29 In addition, McCarty et al also demonstrated that melanoma cells induced keratinocyte proliferation, therefore, leading to epidermal hyperplasia.30 Together, these findings are possible explanations of subungual hyperkeratosis as an associated feature of malignancy, namely SMIS, found in our study.
Hutchinson and micro-Hutchinson’s signs are characteristics of subungual melanoma. We found Hutchinson’s sign in only one case with SMIS. Interestingly, micro-Hutchinson’s sign could be detected in three more cases with SMIS by onychoscopy (p = 0.015). This could be explained by the fact that in the early stage of SMIS, Hutchinson’s sign may be subtle and difficult to appreciate by naked eye examination. This finding confirmed the importance of onychoscopy in aiding the differentiation between SMIS and benign longitudinal melanonychia.
Limitations of our study include the small number of cases due to its relatively rare nature and all cases being from a single institution. A further large-scale, prospective, multicenter study should be conducted to provide more accurate information. Despite the limitations, our study provided a comprehensive method, using both clinical and onychoscopic assessment, to enable early detection of SMIS in patients presenting with longitudinal melanonychia.
Conclusion
In conclusion, individuals with longitudinal melanonychia in at least the sixth decade of life with Fitzpatrick’s skin type 5 are faced with higher risks of SMIS. This study confirmed that onychoscopy can provide useful information to aid in the diagnosis of longitudinal melanonychia. Longitudinal melanonychia with a bandwidth percentage higher than 65%, multicolor features, granular pigmentation, subungual hyperkeratosis and/or micro-Hutchinson’s sign strongly suggest the diagnosis of SMIS. From these findings, onychoscopy can be utilized to aid in the decision of whether to perform a nail biopsy in individuals presenting with longitudinal melanonychia.
Consent Statement
The patients provided written informed consent to perform all necessary investigations, to take clinical photographs, and to use them for research purposes and publication.
Acknowledgments
We would like to thank Dr. Kunlawat Thadanipon from Department of Clinical Epidemiology and Biostatistics for statistical analysis, Dr. Suthep Jirasutus for his kind support and intellectual input in this research, and also thank the Department of Pathology, Faculty of Medicine, Ramathibodi Hospital, for preparation of biopsy specimens.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Markovic SN, Erickson LA, Rao RD, et al. Malignant melanoma in the 21st century, part 1: epidemiology, risk factors, screening, prevention, and diagnosis. Mayo Clin Proc. 2007;82(3):364–380. doi:10.4065/82.3.364
2. Chi Z, Li S, Sheng X, et al. Clinical presentation, histology, and prognoses of malignant melanoma in ethnic Chinese: a study of 522 consecutive cases. BMC Cancer. 2011;11:85. doi:10.1186/1471-2407-11-85
3. Roh MR, Kim J, Chung KY. Treatment and outcomes of melanoma in acral location in Korean patients. Yonsei Med J. 2010;51(4):562–568. doi:10.3349/ymj.2010.51.4.562
4. Ishihara K, Saida T, Otsuka F, Yamazaki N. Statistical profiles of malignant melanoma and other skin cancers in Japan: 2007 update. Int J Clin Oncol. 2008;13(1):33–41. doi:10.1007/s10147-007-0751-1
5. Lee HY, Chay WY, Tang MB, Chio MT, Tan SH. Melanoma: differences between Asian and Caucasian patients. Ann Acad Med Singap. 2012;41(1):17–20. doi:10.1201/b12510-3
6. Chang JW, Yeh KY, Wang CH, et al. Malignant melanoma in Taiwan: a prognostic study of 181 cases. Melanoma Res. 2004;14(6):537–541. doi:10.1097/00008390-200412000-00016
7. Huang K, Fan J, Misra S. Acral lentiginous melanoma: incidence and survival in the United States, 2006–2015, an analysis of the SEER registry. J Surg Res. 2020;251:329–339. doi:10.1016/j.jss.2020.02.010
8. Ingkaninanda P, Visessiri Y, Rutnin S. Clinicopathological features and prognostic factors of malignant melanoma: a retrospective analysis of Thai patients in Ramathibodi hospital. J Med Assoc Thai. 2015;98(8):820–827.
9. Braun RP, Baran R, Le Gal FA, et al. Diagnosis and management of nail pigmentations. J Am Acad Dermatol. 2007;56(5):835–847. doi:10.1016/j.jaad.2006.12.021
10. Levit EK, Kagen MH, Scher RK, Grossman M, Altman E. The ABC rule for clinical detection of subungual melanoma. J Am Acad Dermatol. 2000;42(2):269–274. doi:10.1016/S0190-9622(00)90137-3
11. Ko D, Oromendia C, Scher R, Lipner SR. Retrospective single-center study evaluating clinical and dermoscopic features of longitudinal melanonychia, ABCDEF criteria, and risk of malignancy. J Am Acad Dermatol. 2019;80(5):1272–1283. doi:10.1016/j.jaad.2018.08.033
12. Halteh P, Scher R, Artis A, Lipner SR. A survey-based study of management of longitudinal melanonychia amongst attending and resident dermatologists. J Am Acad Dermatol. 2017;76(5):994–996. doi:10.1016/j.jaad.2016.11.053
13. Ronger S, Touzet S, Ligeron C, et al. Dermoscopic examination of nail pigmentation. Arch Dermatol. 2002;138(10):1327–1333. doi:10.1001/archderm.138.10.1327
14. Phan A, Dalle S, Touzet S, Ronger-Savle S, Balme B, Thomas L. Dermoscopic features of acral lentiginous melanoma in a large series of 110 cases in a white population. Br J Dermatol. 2010;162(4):765–771. doi:10.1111/j.1365-2133.2009.09594.x
15. Di Chiacchio ND, Farias DC, Piraccini BM, et al. Consensus on melanonychia nail plate dermoscopy. An Bras Dermatol. 2013;88(2):309–313. doi:10.1590/S0365-05962013000200029
16. Benati E, Ribero S, Longo C, et al. Clinical and dermoscopic clues to differentiate pigmented nail bands: an International Dermoscopy Society study. J Eur Acad Dermatol Venereol. 2017;31(4):732–736. doi:10.1111/jdv.13991
17. Ohn J, Jo G, Cho Y, Sheu SL, Cho KH, Mun JH. Assessment of a predictive scoring model for dermoscopy of subungual melanoma in situ. JAMA Dermatol. 2018;154(8):890–896. doi:10.1001/jamadermatol.2018.1372
18. Di Chiacchio N, Hirata SH, Enokihara MY, Michalany NS, Fabbrocini G, Tosti A. Dermatologists’ accuracy in early diagnosis of melanoma of the nail matrix. Arch Dermatol. 2010;146(4):382–387. doi:10.1001/archdermatol.2010.27
19. Adigun CG, Scher RK. Longitudinal melanonychia: when to biopsy and is dermoscopy helpful? Dermatol Ther. 2012;25(6):491–497. doi:10.1111/j.1529-8019.2012.01554.x
20. Koga H, Saida T, Uhara H. Key point in dermoscopic differentiation between early nail apparatus melanoma and benign longitudinal melanonychia. J Dermatol. 2011;38(1):45–52. doi:10.1111/j.1346-8138.2010.01175.x
21. Bellew S, Del Rosso JQ, Kim GK. Skin cancer in Asians: part 2: melanoma. J Clin Aesthet Dermatol. 2009;2(10):34–36.
22. Jin H, Kim JM, Kim GW, et al. Diagnostic criteria for and clinical review of melanonychia in Korean patients. J Am Acad Dermatol. 2016;74(6):1121–1127. doi:10.1016/j.jaad.2015.12.039
23. Cormier JN, Xing Y, Ding M, et al. Ethnic differences among patients with cutaneous melanoma. Arch Intern Med. 2006;166(17):1907–1914. doi:10.1001/archinte.166.17.1907
24. Chang JW, Guo J, Hung CY, et al. Sunrise in melanoma management: time to focus on melanoma burden in Asia. Asia Pac J Clin Oncol. 2017;13(6):423–427. doi:10.1111/ajco.12670
25. Thai KE, Young R, Sinclair RD. Nail apparatus melanoma. Australas J Dermatol. 2001;42(2):71–73. doi:10.1046/j.1440-0960.2001.00486.x
26. Jung HJ, Kweon SS, Lee JB, Lee SC, Yun SJ. A clinicopathologic analysis of 177 acral melanomas in Koreans: relevance of spreading pattern and physical stress. JAMA Dermatol. 2013;149(11):1281–1288. doi:10.1001/jamadermatol.2013.5853
27. Mohrle M, Hafner HM. Is subungual melanoma related to trauma? Dermatology. 2002;204(4):259–261. doi:10.1159/000063354
28. Duarte AF, Correia O, Barros AM, Ventura F, Haneke E. Nail melanoma in situ: clinical, dermoscopic, pathologic clues, and steps for minimally invasive treatment. Dermatol Surg. 2015;41(1):59–68. doi:10.1097/DSS.0000000000000243
29. Kodet O, Lacina L, Krejci E, et al. Melanoma cells influence the differentiation pattern of human epidermal keratinocytes. Mol Cancer. 2015;14:1. doi:10.1186/1476-4598-14-1
30. McCarty MF, Bielenberg DR, Nilsson MB, et al. Epidermal hyperplasia overlying human melanoma correlates with tumour depth and angiogenesis. Melanoma Res. 2003;13(4):379–387. doi:10.1097/00008390-200308000-00007
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.