Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Clinical and Functional Determinants of Caregiver Burden in Elderly Patients with Atopic Dermatitis: A Multicentre Cross-Sectional Study
Authors Bighetti S ![]() , Bettolini L
, Bettolini L ![]() , Zerbinati N, Carugno A
, Zerbinati N, Carugno A ![]() , Fratton Z
, Fratton Z ![]() , Errichetti E, Pezzolo E, Venturini M
, Errichetti E, Pezzolo E, Venturini M ![]() , Rossi M
, Rossi M
Received 28 November 2025
Accepted for publication 12 March 2026
Published 13 March 2026 Volume 2026:19 584984
DOI https://doi.org/10.2147/CCID.S584984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Stefano Bighetti,1 Luca Bettolini,1 Nicola Zerbinati,2 Andrea Carugno,3 Zeno Fratton,4 Enzo Errichetti,4 Elena Pezzolo,5 Marina Venturini,1 Mariateresa Rossi1
1Dermatology Department, University of Brescia, ASST Spedali Civili di Brescia, Brescia, Italy; 2Department of Medicine and Innovation Technology (DiMIT), University of Insubria, Varese, Italy; 3Department of Medicine and Surgery, University of Insubria, Varese, Italy; 4Department of Medicine, University of Udine, Udine, Italy; 5Dermatology Unit, Ospedale San Bortolo, Vicenza, Italy
Correspondence: Stefano Bighetti, Dermatology Department, University of Brescia, ASST Spedali Civili di Brescia, Brescia, Italy, Tel +39 030 3995301, Fax +39 030 399505, Email [email protected]
Purpose: This multicentre cross-sectional study aimed to quantify caregiver burden among elderly patients with atopic dermatitis (AD) and to identify its principal clinical, functional, and symptomatic determinants. Specifically, we evaluated the relative contributions of functional impairment, caregiving intensity, and inflammatory severity to overall caregiver burden.
Patients and Methods: A total of 213 patient–caregiver dyads were consecutively recruited from four tertiary dermatology centers in Italy. Eligible patients were aged ≥ 65 years with dermatologist-confirmed AD. Clinical assessments were performed by board-certified dermatologists at each participating centre and included the Eczema Area and Severity Index (EASI), body surface area (BSA), pruritus and sleep disturbance (numeric rating scales), comorbidities, and functional status measured by Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL). Caregivers completed a structured questionnaire on caregiving responsibilities and the Caregiver Burden Inventory (CBI). Associations were examined using Spearman correlation and multivariable linear regression models.
Results: Patients had a mean age of 73.3 ± 7.3 years and moderate disease severity (mean EASI 13.3 ± 11.2). Functional impairment was common (median ADL 4.0), and caregivers reported a median of 2.5 daily hours of assistance. Overall burden was moderate (mean CBI 32.0 ± 14.0). CBI correlated most strongly with ADL impairment (ρ = – 0.50) and daily caregiving hours (ρ = 0.47), with additional associations for sleep disturbance (ρ = 0.35) and EASI (ρ = 0.31). In multivariable analysis, ADL impairment (p < 0.001), caregiving hours (p = 0.031), sleep disturbance (p < 0.001), and EASI (p = 0.005) remained independently associated with burden; pruritus was not significant after adjustment.
Conclusion: Caregiver burden in elderly AD is primarily driven by functional dependence and caregiving intensity, with additional contributions from sleep disturbance and inflammatory severity. Integrating functional assessment and caregiver-focused strategies into routine care may improve outcomes for both patients and caregivers.
Keywords: atopic dermatitis, caregiver burden, elderly patients, functional impairment
Introduction
Atopic dermatitis (AD) is a chronic, relapsing inflammatory dermatosis characterized by pruritus, eczematous lesions, and impaired epidermal barrier function. Although traditionally regarded as a childhood disease, AD frequently persists into adulthood and may also arise de novo in later life. Recent epidemiological data suggest a second prevalence peak after the age of 50, challenging the traditional perception of AD as predominantly pediatric.1 In older adults, clinical expression is shaped by xerosis, immunosenescence, multimorbidity, and polypharmacy, leading to diagnostic challenges and potentially contributing to complex and variable disease trajectories.1,2
In this population, AD may present with atypical morphology and distribution, often characterized by lichenified plaques, chronic pruritus, and eczematous lesions involving the trunk and extensor surfaces. Differential diagnosis may include asteatotic eczema, prurigo nodularis, contact dermatitis, or drug-related eruptions, further complicating clinical assessment. Moreover, the frequent coexistence of medical comorbidities and age-related functional decline distinguishes elderly patients from younger cohorts and may significantly influence disease management and treatment adherence.1,2
The burden of AD extends far beyond visible skin involvement. Sleep disturbance, social withdrawal, and psychological distress occur across all ages, but older adults tend to experience more persistent symptoms and a more profound impact on daily functioning.1,2 Topical therapy remains the foundation of AD management, yet age-related limitations—such as reduced manual dexterity, impaired vision, physical disability, or cognitive decline—may hinder regular treatment application. These obstacles, together with complex therapeutic regimens, make older patients particularly vulnerable to inconsistent treatment use and suboptimal disease control.3,4
Most evidence on the psychosocial consequences of AD focuses on pediatric populations and their families. Studies consistently describe substantial emotional strain, sleep disruption, work impairment, and deterioration of family functioning.5–9 Parental quality of life closely mirrors disease severity, and caregiver burden spans emotional, physical, and organizational domains.10 In adults, household factors and family dynamics have also been shown to influence disease control and quality of life.11,12 However, this literature is almost entirely derived from children, adolescents, and mixed-age cohorts.13,14
In contrast, caregiver burden in older adults with AD remains largely unexplored. This gap is clinically significant: elderly patients often rely heavily on spouses, adult children, or professional caregivers for essential tasks such as applying topical therapies, managing systemic treatments, attending medical appointments, or recognizing early signs of exacerbation.15 Despite the clear relevance of caregiving in daily disease management, no multicentre studies have systematically evaluated its impact in elderly AD, and no standardized, multidimensional assessment of caregiver burden has been conducted in this population.
To address this gap, we conducted a multicentre cross-sectional study designed to characterize caregiver burden in elderly patients with AD and identify its clinical, functional, and symptomatic determinants. By integrating dermatological severity, functional status, and caregiving dynamics within real-world tertiary care, this study aims to clarify the interplay between aging, chronic inflammatory skin disease, and informal caregiving—an area of increasing relevance in dermatological practice.
Materials and Methods
Study Design and Population
This multicentre, cross-sectional observational study was conducted over a period of 24 months across four tertiary dermatology referral centres in Italy (Brescia, Varese, Udine, and Vicenza), all specializing in chronic inflammatory skin diseases. All evaluations were performed at a single time point during routine clinical visits. Consecutive patients aged 65 years or older with a dermatologist-confirmed diagnosis of AD, made according to standard clinical criteria, were eligible for inclusion. Patients were enrolled regardless of their ongoing treatment regimen, including topical therapy, conventional systemic treatments, biologics or JAK inhibitors. An additional inclusion criterion was the presence of an identifiable primary caregiver actively involved in the patient’s care and available at the time of clinical assessment. Exclusion criteria comprised inability to provide informed consent, severe cognitive impairment precluding questionnaire completion, absence of a caregiver despite a clear need for daily assistance, and presence of concomitant dermatological conditions likely to interfere with symptom attribution.
For each patient, the primary caregiver was identified as the individual most consistently involved in treatment application, symptom monitoring, daily care or accompaniment to medical appointments. Caregivers included spouses or partners, adult children, professional caregivers or other cohabiting individuals providing regular assistance. The study protocol received approval from the Local Ethics Committee of Brescia (NP. 4707), and written informed consent was obtained from all participants in accordance with the Declaration of Helsinki and national regulations.
Patient Assessment
All questionnaires were self-administered in paper format during the clinical visit under the supervision of trained research personnel to ensure completeness and standardized administration. Patients completed a study-specific, structured questionnaire designed by the investigators to explore treatment use behaviour and caregiver involvement. The questionnaire assessed previous unsupervised interruptions of topical or systemic therapies, reasons for discontinuation (including perceived inefficacy, concerns about adverse events, time constraints, cosmetic attributes of topical formulations, and emotional factors), current motivation towards treatment, expectations regarding therapy, and the degree of caregiver assistance in daily disease management. The instrument also included questions addressing the emotional influence on treatment continuity and the presence of family or professional support in routine care.
Clinical parameters were collected uniformly across centres. Disease severity was assessed using the Eczema Area and Severity Index (EASI), and skin involvement was quantified using body surface area (BSA). Pruritus and sleep disturbance were evaluated using numerical rating scales ranging from 0 to 10. Additional data included disease duration, therapeutic regimen, comorbidities and previous treatments. Functional status was measured using the Activities of Daily Living (ADL) scale, ranging from 0 to 6, and the Instrumental Activities of Daily Living (IADL) scale, ranging from 0 to 8, with lower scores indicating greater dependence.
Caregiver Assessment
Caregiver evaluation was conducted on the same day as patient assessment to ensure temporal alignment of clinical and caregiving data. Caregivers were either informal (family members, such as spouses or adult children) or formal (professional caregivers providing paid assistance). Each caregiver completed a structured, investigator-developed questionnaire designed to collect descriptive information regarding the nature and intensity of caregiving responsibilities. The questionnaire explored assistance with topical and systemic treatments, support in activities of daily living, accompaniment to medical appointments, and daily caregiving time. It also included items addressing the emotional, social, occupational, and sleep-related consequences of caregiving. Caregivers were asked to indicate whether symptoms such as fatigue, stress, or sleep disruption had developed before or after the initiation of caregiving duties. This instrument was developed specifically for the present study and was not previously validated, as its purpose was to provide contextual characterization of caregiving demands rather than to generate standardized psychometric outcome measures.
Caregiver burden was quantified using the Caregiver Burden Inventory (CBI), a validated 24-item multidimensional instrument assessing time-dependent, developmental, physical, social, and emotional burden.16,17 Each item is rated on a 5-point Likert scale ranging from 0 (not at all descriptive) to 4 (very descriptive), yielding a total score between 0 and 96, with higher scores indicating greater perceived caregiver burden. The validated Italian version of the CBI was administered. The total CBI score was predefined as the primary outcome measure of the study. The CBI has demonstrated strong psychometric validity and reliability in populations caring for elderly or chronically ill individuals.
Statistical Analysis
Continuous variables were summarized as mean and standard deviation or as median and interquartile range, depending on distribution, whereas categorical variables were expressed as counts and percentages. Distribution normality was assessed using the Shapiro–Wilk test, inspection of skewness and kurtosis, and visual evaluation of quantile–quantile plots. As most variables exhibited non-normal distribution, associations were examined using Spearman’s rank correlation coefficient.
The primary outcome of interest was the total CBI score. A multivariable linear regression model (ordinary least squares) was specified a priori based on conceptual frameworks of caregiver burden and clinical relevance in elderly AD. The model included ADL, daily hours of caregiving, sleep disturbance, EASI, pruritus, patient age, and years of caregiving. All predictors were entered as continuous variables. The IADL score was excluded due to minimal correlation in preliminary analyses and limited theoretical justification. Multicollinearity was assessed using variance inflation factors, with values greater than 5 indicating potential concern. Model assumptions were evaluated through residual analysis and diagnostic plots. Missing data below 5% were addressed through complete-case analysis without imputation. No adjustment for multiple comparisons was applied, as analyses were hypothesis-driven and based on a predefined model.
All statistical tests were two-sided with significance defined as p < 0.05. Analyses were performed using R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 213 elderly patients with AD and their primary caregivers were included across four tertiary dermatology centres. Of the 213 patients included, 56.3% were female and 43.7% male, while caregivers were predominantly female (62.4%). The primary caregiving roles consisted of adult children (51.2%), spouses or partners (32.9%), and professional or non-familial caregivers (15.9%). The mean age of patients was 73.3 ± 7.3 years, with a median disease duration of 49.5 years (IQR 35.7–67.7). Baseline AD severity was moderate (mean EASI 13.3 ± 11.2; median BSA 14.4%), while pruritus and sleep disturbance were generally mild to moderate (median NRS 2.8 and 2.0, respectively) (Table 1).
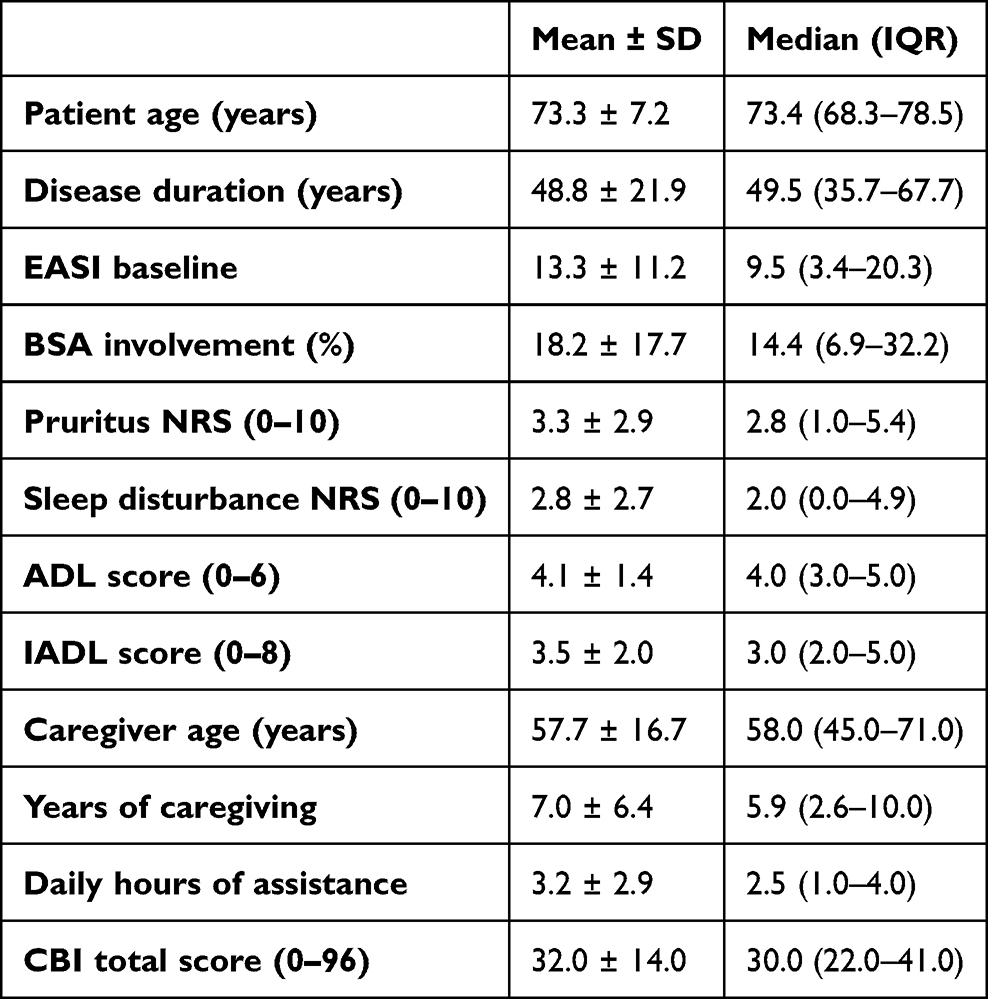 |
Table 1 Baseline Characteristics of Elderly Patients with Atopic Dermatitis and Their Primary Caregivers |
Regarding treatment, 6.1% of patients were receiving topical therapy alone, 23.0% were treated with conventional systemic agents, and the majority (59.6%) were on biologic therapy, predominantly dupilumab. JAK inhibitors were used in 4.7% of patients, and 6.6% were receiving tralokinumab at the time of assessment.
Functional impairment was common. The median ADL score was 4.0 (IQR 3.0–5.0), indicating varying degrees of dependence in basic daily activities, while the median IADL score was 3.0 (IQR 2.0–5.0), reflecting substantial limitations in more complex tasks. Caregivers had a mean age of 57.7 ± 16.7 years and reported assisting patients for a median of 5.9 years and 2.5 hours per day. The overall caregiver burden was moderate, with a mean CBI score of 32.0 ± 14.0 (Table 1).
Correlation Analyses
Spearman correlation analysis demonstrated that caregiver burden was most strongly associated with the patient’s functional status and caregiving demands. The total CBI score showed its highest correlation with ADL impairment (ρ = –0.50) and with the number of daily hours of caregiving (ρ = 0.47). Sleep disturbance also showed a moderate association with burden (ρ = 0.35). Dermatological severity correlated more modestly with burden, with EASI showing a correlation of ρ = 0.31. Pruritus exhibited a weaker correlation (ρ = 0.29), and associations with age (ρ = 0.06) or disease duration (ρ = 0.04) were negligible (Table 2).
 |
Table 2 Determinants of Caregiver Burden (CBI Total Score): Spearman Correlations and Multivariable Linear Regression |
Multivariable Analysis
In the multivariable linear regression model, ADL impairment emerged as the strongest independent determinant of caregiver burden (β = –4.16, p < 0.001). Daily hours of caregiving remained a significant contributor (β = 1.34, p = 0.031), as did sleep disturbance (β = 1.63, p < 0.001) and baseline EASI severity (β = 0.27, p = 0.005). Years of caregiving (β = 0.46, p = 0.029) and patient age (β = 0.24, p = 0.018) also showed more minor yet statistically significant effects. Pruritus did not maintain statistical significance in the adjusted model. This finding indicates that itch, although clinically relevant, contributes less to caregiver burden once functional dependence and sleep disturbance are considered. IADL scores, despite greater variability, were not associated with caregiver burden (ρ = 0.04), suggesting that limitations in basic daily tasks weigh more heavily on caregivers than impairments in instrumental activities (Table 2).
Discussion
The present multicentre study provides one of the most comprehensive evaluations to date of caregiver burden in elderly patients with AD, integrating dermatological severity, functional status, and caregiving dynamics within a real-world tertiary-care context. Previous research on caregiver burden in AD has focused almost exclusively on paediatric patients and their families, with numerous studies documenting substantial emotional, social, and practical strain among parents of affected children.6–12 In contrast, evidence addressing caregiver burden in adults, and particularly in older adults, remains extremely limited.18–20 Our findings, therefore, help fill a critical knowledge gap by characterizing the determinants of caregiver burden in an elderly population, which presents unique functional and therapeutic challenges.1,2
A key result of this study is the central role of functional impairment. Dependence in basic activities of daily living (ADL) was the strongest independent determinant of caregiver burden, surpassing dermatological severity or symptomatic measures. This observation aligns with the broader geriatric and chronic-care literature, where loss of autonomy consistently emerges as a major driver of caregiver strain.15 In elderly individuals with AD, reduced autonomy translates into greater reliance on caregivers for topical therapy, systemic medication administration, and symptom monitoring—care demands that are known to generate psychological fatigue and reduced social participation in caregiving populations.3,12 It should also be acknowledged that, in elderly populations, functional dependence may be influenced not only by dermatological disease but also by coexisting medical comorbidities typical of advanced age. Although multimorbidity was recorded descriptively, the present study did not include a structured quantitative assessment of comorbidity burden, and its potential contribution to caregiver strain warrants further investigation.
Sleep disturbance also emerged as an essential contributor to caregiver burden. This is consistent with evidence showing that nocturnal symptoms have a considerable impact on well-being in patients with AD and that interventions targeting sleep quality can improve overall household functioning.21,22 In our cohort, sleep disturbance remained significant after adjustment for other clinical variables, underscoring its disproportionate impact on caregiving demands, daily fatigue, and stress.
Dermatological severity, measured by EASI, contributed independently to caregiver burden, though to a lesser extent than functional dependence or sleep disturbance. This finding is consistent with previous work showing that AD severity correlates with poorer quality of life and higher psychological distress in both patients and their families.6–12 However, in elderly patients, the impact of skin inflammation appears partly overshadowed by the practical challenges associated with functional decline.
Pruritus, despite being a hallmark symptom of AD, did not remain significant in the multivariable model. This finding should not be interpreted as a lack of clinical relevance. Instead, it suggests that in elderly populations, the consequences of itch, particularly nocturnal restlessness and prolonged caregiving vigilance, are captured more effectively by measures of sleep disturbance. Prior literature supports the concept that night-time manifestations of AD often exert a greater influence on both patient and caregiver burden than daytime itch intensity.21
Daily caregiving intensity was another independent determinant of burden. Even modest increases in daily assistance were associated with higher CBI scores, consistent with recognised caregiving models. 20 Years of caregiving and patient age showed more minor, yet significant, effects, indicating that caregiver burden is more closely tied to present functional and symptomatic demands than to chronological age or disease duration.
Therapeutic considerations may also play an indirect role. The evolving landscape of systemic treatments for AD, including targeted biologic therapies (such as IL-4/IL-13 pathway inhibitors) and oral Janus kinase inhibitors, has expanded therapeutic opportunities for older adults.23,24 In our cohort, the majority of patients were receiving biologic therapies, which generally require less daily caregiver involvement compared with complex topical regimens. By improving inflammatory control and simplifying daily management demands, these treatments may contribute to a reduction in caregiving intensity. However, the present study was not designed to compare treatment modalities, and further research is needed to evaluate how different systemic strategies influence caregiver burden in elderly populations.
The study benefits from several strengths, including its multicentre design, large sample size, and simultaneous assessment of dermatological, functional, and caregiving variables. The use of the validated CBI further supports the robustness of our findings.16,17 However, some limitations must be acknowledged. The cross-sectional design precludes causal inference, and caregiver-reported measures may introduce perception or recall bias.25,26 Socioeconomic factors were not assessed, limiting the interpretation of contextual influences on burden.25 In addition, although multimorbidity and polypharmacy are highly prevalent in elderly populations and may increase caregiving complexity through medication management demands and monitoring requirements, the present study did not include a quantitative assessment of total medication load beyond AD-specific treatments. This may have limited our ability to fully capture the contribution of global therapeutic burden to caregiver strain. Furthermore, the majority of patients in our cohort were receiving systemic therapies, particularly biologics, which may involve less daily management complexity compared with intensive topical regimens. This treatment distribution may have influenced the magnitude and structure of caregiver burden observed and potentially limits generalizability to elderly populations managed primarily with complex topical therapy. In addition, participants with severe cognitive impairment or without available caregivers were excluded, which may have led to underrepresentation of the most vulnerable patient–caregiver dyads. Although caregiver categories were described, the present study was not designed to compare burden across different caregiver types. Moreover, although the multidimensional structure of the CBI allows for domain-specific exploration, the present study focused on the total burden score as the predefined primary outcome. Domain-level analyses may provide additional descriptive insight and should be explored in future research to further characterize specific dimensions of caregiver strain in elderly AD. Future studies should explore whether spouses, adult children, and professional caregivers experience distinct patterns of burden, as these roles may involve different emotional, social, and practical dynamics.
Despite these limitations, our findings have meaningful implications for clinical practice. Routine assessment of functional status should be incorporated into the care of elderly patients with AD, particularly when management relies heavily on complex topical regimens. Simplifying treatment plans, particularly in patients requiring complex topical regimens, may theoretically reduce caregiving demands and associated burden, although this relationship warrants further dedicated investigation. Integrating caregivers into shared decision-making is essential, as they play a pivotal role in ensuring treatment adherence, continuity of care, and long-term disease stability, in line with emerging caregiver-focused perspectives in dermatologic care.27,28
Conclusion
Caregiver burden in elderly patients with atopic dermatitis is a multidimensional phenomenon that reflects the combined impact of functional dependence, daily caregiving demands, sleep disturbance, and, to a lesser extent, inflammatory disease severity. In this multicentre cohort, loss of autonomy and the intensity of caregiving emerged as the strongest independent determinants of burden, highlighting the need for routine functional assessment and simplification of therapeutic regimens in older adults. Understanding these determinants is essential for developing individualized, caregiver-centred management strategies that address both the dermatological and practical challenges of daily care, ultimately improving outcomes for patients and those who support them.
Data Sharing Statement
Data is available from corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any sponsor or funder.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maurelli M, Chiricozzi A, Peris K, Gisondi P, Girolomoni G. Atopic dermatitis in the elderly population. Acta Derm Venereol. 2023;103:adv13363. doi:10.2340/actadv.v103.13363
2. Tanei R. Atopic dermatitis in older adults: a review of treatment options. Drugs Aging. 2020;37(3):149–8. doi:10.1007/s40266-020-00750-5
3. Tier HL, Balogh EA, Bashyam AM, et al. Tolerability of and adherence to topical treatments in atopic dermatitis: a narrative review. Dermatol Ther. 2021;11(2):415–431. doi:10.1007/s13555-021-00500-4
4. Sagransky MJ, Yentzer BA, Williams LL, et al. A randomized controlled pilot study of the effects of an extra office visit on adherence and outcomes in atopic dermatitis. Arch Dermatol. 2010;146(12):1428–1431. doi:10.1001/archdermatol.2010.368
5. Bass AM, Anderson KL, Feldman SR. Interventions to increase treatment adherence in pediatric atopic dermatitis: a systematic review. J Clin Med. 2015;4(2):231–242. doi:10.3390/jcm4020231
6. Barbarot S, Auziere S, Gadkari A, et al. Impact of atopic dermatitis on quality of life of children and their families. J Pediatr. 2022;246:220–226.e5. doi:10.1016/j.jpeds.2022.04.027
7. Marciniak J, Reich A, Szepietowski JC. Quality of life of parents of children with atopic dermatitis. Acta Derm Venereol. 2017;97(6):711–714. doi:10.2340/00015555-2633
8. Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact questionnaire. Br J Dermatol. 1998;138(1):107–113. doi:10.1046/j.1365-2133.1998.02034.x
9. Kisielienė I, Drėlingytė V, Blažytė E, et al. Burden of pediatric atopic dermatitis on patients and their families. J Clin Med. 2024;13(6):1700. doi:10.3390/jcm13061700
10. Xu X, Zhang J, Wang Y, et al. Factors influencing quality of life in children with atopic dermatitis and their caregivers. Sci Rep. 2019;9:15990. doi:10.1038/s41598-019-51129-5
11. Ali F, Vyas J, Finlay AY. Counting the burden: atopic dermatitis and health-related quality of life. Acta Derm Venereol. 2020;100(12):adv00161. doi:10.2340/00015555-3511
12. Saeki H, Ito M, Minoura H, et al. Impact of family and household environment on quality of life in atopic dermatitis. J Clin Med. 2023;12(8):2988. doi:10.3390/jcm12082988
13. Yang EJ, Beck KM, Sekhon S, Bhutani T, Koo J. The impact of pediatric atopic dermatitis on families: a review. Pediatr Dermatol. 2019;36(1):66–71. doi:10.1111/pde.13727
14. Serup J, Kettis Lindblad Å, Maroti M, et al. To follow or not to follow dermatological treatment: a review. Acta Derm Venereol. 2006;86(3):193–197. doi:10.2340/00015555-0073
15. Schulz R, Beach SR. Caregiving as a risk factor for mortality. JAMA. 1999;282(23):2215–2219. doi:10.1001/jama.282.23.2215
16. Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontologist. 1989;29(6):798–803. doi:10.1093/geront/29.6.798
17. Luchetti L, Uhunmwangho E, Dordoni G, et al. The subjective feeling of burden in caregivers of elderly with dementia: how to intervene? Arch Gerontol Geriatr. 2009;49(Suppl 1):153–161. doi:10.1016/j.archger.2009.09.025
18. Yap JCH, Yew YW. Impact of atopic dermatitis on quality of life of caregivers: a systematic review and meta-analysis. Dermatitis. 2024;35(6):554–595. doi:10.1089/derm.2023.0362
19. Kilic N, Kilic M. Investigation of quality of life of patients with atopic dermatitis and quality of life, psychiatric symptomatology, and caregiver burden of their mothers. Children. 2023;10(9):1487. doi:10.3390/children10091487
20. Kelbore AG, Enbiale W, van Wyk JM, Mosam A. The impact of atopic dermatitis on caregivers’ quality of life in Ethiopia. Front Med. 2025;12:1537089. doi:10.3389/fmed.2025.1537089
21. Bawany F, Northcott CA, Beck LA, Pigeon WR. Sleep disturbances and atopic dermatitis: relationships, methods for assessment, and therapies. J Allergy Clin Immunol Pract. 2021;9(4):1488–1500. doi:10.1016/j.jaip.2020.12.007
22. Yasuda KI, Ishiuji Y, Ebata T, et al. Monitoring sleep and scratch improves quality of life in patients with atopic dermatitis. Acta Derm Venereol. 2023;103:adv11922. doi:10.2340/actadv.v103.11922
23. Bettolini L, Bighetti S, Ferrucci SM, et al. Safety and effectiveness of dupilumab in atopic dermatitis patients with hematologic comorbidities: a multicenter retrospective study. Antibodies. 2025;14(3):75. doi:10.3390/antib14030075
24. Rossi M, Bighetti S, Narcisi A, et al. JAK inhibitors in atopic dermatitis: does weight matter? A real-world nationwide retrospective study: IL-AD (Italian Landscape Atopic Dermatitis). Dermatol Ther. 2025;15(10):2833–2851. doi:10.1007/s13555-025-01477-0
25. Li Z, Gu J, Tang T, et al. The global burden of atopic dermatitis in elderly populations: trends, disparities, and future projections. Healthcare. 2025;13(7):788. doi:10.3390/healthcare13070788
26. Wójcik E, Krajewski PK, Szepietowski JC. Chronic dermatoses affect not only sick individuals: a review of family and caregiver burden assessment tools. Postepy Dermatol Alergol. 2024;41(5):433–445. doi:10.5114/ada.2024.141685
27. Feldman SR, Chan AWM, Ammoury A, et al. Patients’ and caregivers’ perspectives of the atopic dermatitis journey. J Dermatol Treat. 2024;35(1):2315145. doi:10.1080/09546634.2024.2315145
28. Willard K, Novak S, Lio PA, et al. Patient and caregiver perceptions on education and treatment needs in atopic dermatitis from an international survey. Dermatol Ther. 2025.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.