Back to Journals » Clinical Ophthalmology » Volume 20
Clinical Analysis of Perforating Globe Injuries with Intraorbital Foreign Bodies: An 18-Year Retrospective Study
Authors Niu L, Ren H, Xu H ![]() , Sun X
, Sun X ![]() , Jiang R
, Jiang R ![]()
Received 15 December 2025
Accepted for publication 2 February 2026
Published 7 February 2026 Volume 2026:20 586656
DOI https://doi.org/10.2147/OPTH.S586656
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Liangliang Niu,1– 4,* Hui Ren,1– 3,* Huan Xu,1– 4 Xinghuai Sun,1– 3,5 Rui Jiang1– 4
1Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China; 2NHC Key Laboratory of Myopia and Related Eye Diseases; Key Laboratory of Myopia and Related Eye Diseases, Chinese Academy of Medical Sciences, Shanghai, 200031, People’s Republic of China; 3Shanghai Key Laboratory of Visual Impairment and Restoration, Shanghai, 200031, People’s Republic of China; 4Ocular Trauma Center, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China; 5State Key Laboratory of Medical Neurobiology and MOE Frontiers Center for Brain Science, Institutes of Brain Science, Fudan University, Shanghai, 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinghuai Sun, Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China, Email [email protected] Rui Jiang, Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China, Email [email protected]
Purpose: This study investigated the clinical characteristics, management strategies, and visual outcomes of perforating ocular injuries associated with intraorbital foreign bodies (IOrFBs).
Methods: We retrospectively reviewed 54 patients with perforating ocular injuries and IOrFBs admitted to the Eye & ENT Hospital of Fudan University from January 1, 2007, to December 31, 2024. This study was reviewed and approved by the Ethics Committee of the Eye & ENT Hospital of Fudan University (Approval No. 2024146). Data collected included demographics, injury circumstances, foreign body composition, size and location (measured on preoperative computed tomography [CT] images), surgical approaches, and visual outcomes. Statistical analyses were performed using R, with significance set at p < 0.05.
Results: Of the 54 patients, 87.0% (47) were male, and 92.6% (50) sustained occupational injuries (both p < 0.001). Ferromagnetic metallic fragments were the predominant cause (77.8%, 42). Anatomically, 40.7% (22) of foreign bodies were confined to the orbit, while 18.5% (10) involved the inferior globe wall and 16.7% (9) extended to the posterior pole. Larger IOrFB diameters were significantly associated with poorer preoperative and postoperative visual acuity (p < 0.05). Surgical interventions were performed as either single-stage or staged procedures, depending on the severity of the injury. The surgical strategies included pars plana vitrectomy (PPV) alone without foreign body removal; PPV combined with IOrFB extraction; PPV followed by subsequent orbital surgery for foreign body removal; orbital surgery for foreign body extraction followed by subsequent PPV; and IOrFB extraction alone without PPV. The most common surgical approach was combined PPV with orbital surgery (35.2%, 19). Notably, surgical approach was not an independent predictor of final visual outcomes.
Conclusion: IOrFBs primarily affect working-age men and are typically caused by occupational metallic trauma. Larger foreign bodies predict worse baseline and final vision, whereas foreign body location and surgical approach do not independently influence visual prognosis. These findings highlight the need for early detection, occupational safety measures, and individualized management to optimize outcomes.
Keywords: open-globe injury, perforating ocular trauma, intraorbital foreign body, surgical strategy, visual acuity
Introduction
Perforating ocular injuries are defined as traumas in which a foreign object enters one part of the eye and exits through another, creating both entry and exit wounds.1–3 When complicated by an intraorbital foreign body (IOrFB), such injuries constitute a severe ophthalmic emergency associated with substantial risks, including retinal detachment, proliferative vitreoretinopathy, optic nerve injury, and orbital cellulitis or infection, posing considerable challenges for ophthalmic surgeons.4–6
An IOrFB refers to a foreign object that has penetrated the ocular wall and lies predominantly or entirely within the orbital cavity, most commonly resulting from high-velocity impacts in industrial or construction environments.7,8 With the progression of industrialization, the incidence of occupational orbital injuries—particularly those caused by metallic projectiles—has been increasing, predominantly affecting working-age males.6,9–11
Previously reported IOrFBs associated with perforating ocular injuries include metal, lead, glass, wood, stone, and plastic. These injuries predominantly affect middle-aged individuals and are closely related to occupational exposure, particularly in industrial and construction settings; other causes include accidental falls and traffic accidents.5,7,9,12,13 Among these, metallic foreign bodies represent the most prevalent type, occasionally leading to periorbital fibrosis, strabismus, fistula formation, or chronic inflammatory reactions.14 In contrast, wooden foreign bodies are more prone to cause optic nerve injury, abscess formation, and pronounced inflammatory responses,15 thereby necessitating urgent medical or surgical intervention.
The diagnosis of perforating ocular injuries complicated by IOrFBs remains challenging due to the wide variability in foreign body composition, morphology, and anatomical distribution. Imaging evaluation plays a pivotal role in diagnosis. Computed tomography (CT) is the preferred modality owing to its high sensitivity for detecting metallic and high-density inorganic materials, as well as its rapid image acquisition. Magnetic resonance imaging (MRI) offers advantages in identifying low-density organic materials such as wood; however, it should be performed cautiously because of the potential hazards in the presence of metallic foreign bodies.6,7,9,15–17
Prompt assessment and the adoption of an optimal management strategy are crucial for preserving visual function and minimizing long-term complications. Surgical decision-making largely depends on the foreign body’s location, its proximity to critical orbital structures, and the patient’s clinical presentation.12,13,18 Nevertheless, controversy persists regarding the optimal timing and surgical approach, and no consensus has been reached on balancing the urgency of intervention against operative risks.
Given the importance of delineating epidemiological characteristics to better understand injury mechanisms and inform preventive strategies, this retrospectively study analyzed 54 cases of perforating ocular injuries complicated by IOrFBs treated at the Eye & ENT Hospital of Fudan University between 2007 and 2024, aiming to comprehensively characterize their epidemiological patterns, clinical features, management strategies, and prognostic determinants.
Materials and Methods
Study Design and Inclusion Criteria
This single-center retrospective case series included hospitalized patients diagnosed with perforating ocular injuries complicated by IOrFBs at the Eye & ENT Hospital of Fudan University, Shanghai, between January 1, 2007, and December 31, 2024. As a major tertiary referral center in Eastern China, the hospital specializes in the management of complex and severe ophthalmic conditions.
This study was reviewed and approved by the Ethics Committee of the Eye & ENT Hospital of Fudan University (Approval No. 2024146). Given that this was a retrospective clinical study using previously collected data, did not involve any intervention or additional risk to participants, and all data were anonymized prior to analysis, the Ethics Committee granted a waiver of individual informed consent from study participants. All study procedures complied with the principles outlined in the Declaration of Helsinki.
The inclusion criteria were as follows: (1) patients hospitalized for the treatment of open-globe injury involving posterior segment penetration, which was classified as Zone III open-globe injury and further defined as perforating ocular injury according to the Birmingham Eye Trauma Terminology (BETT) system, characterized by the presence of both entrance and exit wounds;2,3 (2) confirmation of foreign bodies penetrating the globe wall, with most or all of the foreign body located within the orbital cavity, as verified by orbital CT; and (3) availability of at least six months of postoperative follow-up.
Accordingly, only patients with perforating open-globe injuries accompanied by intraorbital foreign bodies were included, whereas cases of isolated intraorbital foreign bodies without globe penetration were excluded.
Given the extended study period (2007–2024), long-term follow-up was not feasible for some patients treated in earlier years, primarily due to the limited use of mobile communication devices at that time. To ensure data consistency and reliability, a minimum follow-up duration of six months was established as the inclusion threshold.
Data Collection and Definitions
Data were retrieved from the hospital’s electronic medical record system and included demographic information (age, sex), injury circumstances, foreign body characteristics, slit-lamp findings of both anterior and posterior segments, imaging results, surgical interventions, and visual outcomes at the final follow-up.
The injury setting was categorized as either occupational or non-occupational. Occupational injuries referred to work-related trauma sustained during machinery operation, welding, construction, or similar activities, whereas non-occupational injuries included accidental trauma occurring in daily life (eg, household incidents, traffic accidents). Classification was based on patient interviews and medical documentation.
Patients with perforating ocular injuries due to IOrFBs present as open-globe injuries, for which orbital CT is the preferred initial imaging modality in the emergency setting, while ocular ultrasonography is performed routinely performed when clinically indicated to further assess intraocular structures. The characteristics of IOrFBs were analyzed according to material composition and anatomical location; materials were classified as metallic, wooden, or other types based on surgical records and pathological findings. Anatomical localization and foreign body size were determined primarily through orbital CT and categorized into six groups: (1) Entirely intraorbital: the foreign body penetrated the globe wall and was located completely within the orbital cavity; (2) Inferior globe wall involvement: the foreign body was partially located in the vitreous cavity and partially traversed the inferior sclera into the orbit; (3) Posterior pole involvement: the foreign body was partially within the vitreous cavity and partially exited through the macular or optic disc region into the orbit; (4) Temporal globe wall involvement: the foreign body was partially located in the vitreous cavity and partially penetrated the temporal sclera into the orbit; (5) Nasal globe wall involvement: the foreign body was partially within the vitreous cavity and partially traversed the nasal sclera into the orbit; (6) Superior globe wall involvement: the foreign body was partially in the vitreous cavity and partially exited through the superior sclera into the orbit.
Surgical Approaches
Operative details and intraoperative observations were reviewed from medical records. Surgical interventions were performed as single-stage or staged procedures, with the approach determined by the characteristics of the IOrFBs, the patient’s ocular condition, and changes in surgical techniques over the study period. Patients were classified into five groups according to the surgical approach: Group 1: Pars plana vitrectomy (PPV) alone without IOrFB removal (single-stage); Group 2: PPV combined with IOrFB extraction (single-stage); Group 3: PPV followed by subsequent orbital surgery for IOrFB removal (staged procedures); Group 4: Orbital surgery for IOrFB removal followed by subsequent PPV (staged procedures); Group 5: Orbital foreign body extraction alone without PPV (single-stage).
Notably, all patients had undergone primary globe repair for ocular trauma in an emergency setting either prior to or concurrently with the above-mentioned procedures.
Visual Acuity Assessment and Statistical Analysis
Best-corrected visual acuity (BCVA) was evaluated preoperatively (Pre-BCVA) and at the final follow-up (Post-BCVA) to assess surgical efficacy. The change in visual acuity (ΔBCVA) was calculated as the difference between Post-BCVA and Pre-BCVA. BCVA values were expressed using the logarithm of the minimum angle of resolution (logMAR) scale.19,20 For qualitative assessments, the following logMAR conversions were applied: counting fingers (CF) = 2.1, hand motion (HM) = 2.4, light perception (LP) = 2.7, and no light perception (NLP) = 3.0.
Statistical analyses were performed using R statistical software (version 3.6.1; R Core Team). As the data were not normally distributed, continuous variables were presented as medians with ranges (minimum–maximum). Intergroup comparisons were conducted using the Mann–Whitney U-test, and paired Pre- and Post-BCVA values were analyzed using the Wilcoxon signed-rank test. Simple linear regression was used to explore associations with foreign body size. No multivariate analyses were performed; therefore, the results reflect associations rather than independent effects. A p-value < 0.05 was considered statistically significant.
Results
Patient Demographics and Prognostic Analysis
Between 2007 and 2024, a total of 54 patients with perforating ocular injuries accompanied by IOrFBs were hospitalized at the Eye and ENT Hospital of Fudan University. The baseline characteristics of these patients—including age, sex, IOrFB conditions, primary therapeutic interventions, and BCVA at presentation and at final follow-up (expressed in logMAR)—are summarized in Table 1.
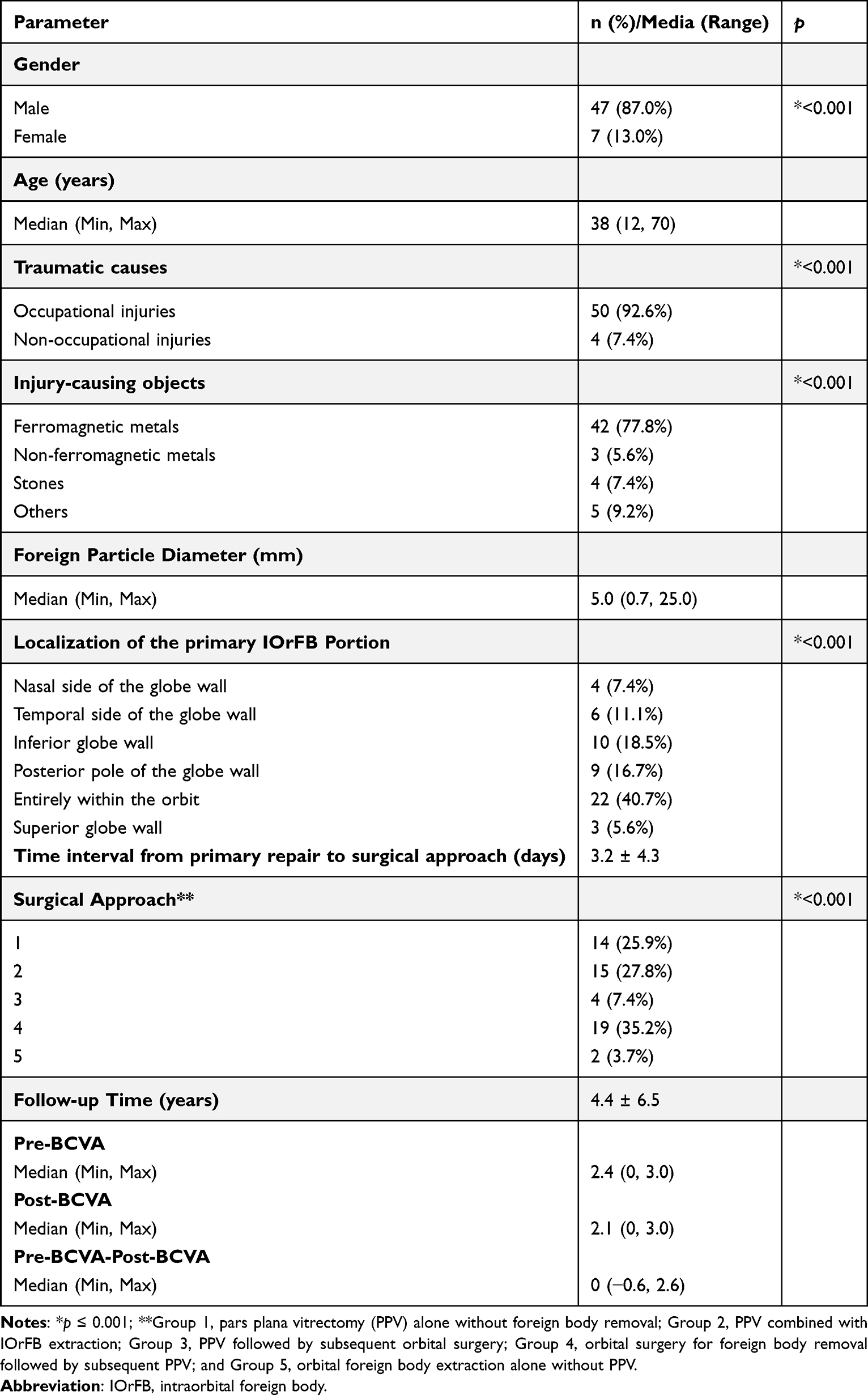 |
Table 1 Baseline Demographics and Visual Outcomes for Patients Entering the Study |
As shown in Table 1, the median age of patients was 38 years (range, 12–70 years). Males were predominantly affected, accounting for 87.0% (47 cases; p < 0.001). Regarding etiology, occupational trauma was the leading cause, representing 92.6% (50 cases; p < 0.001), while non-occupational injuries (eg, domestic or traffic accidents) comprised only 7.4% (4 cases). Further analysis revealed that patients with occupational injuries exhibited relatively better preoperative visual acuity compared with those with non-occupational causes (p1 = 0.04). However, postoperative visual outcomes remained poor in both groups, with no statistically significant difference between them (Table 2).
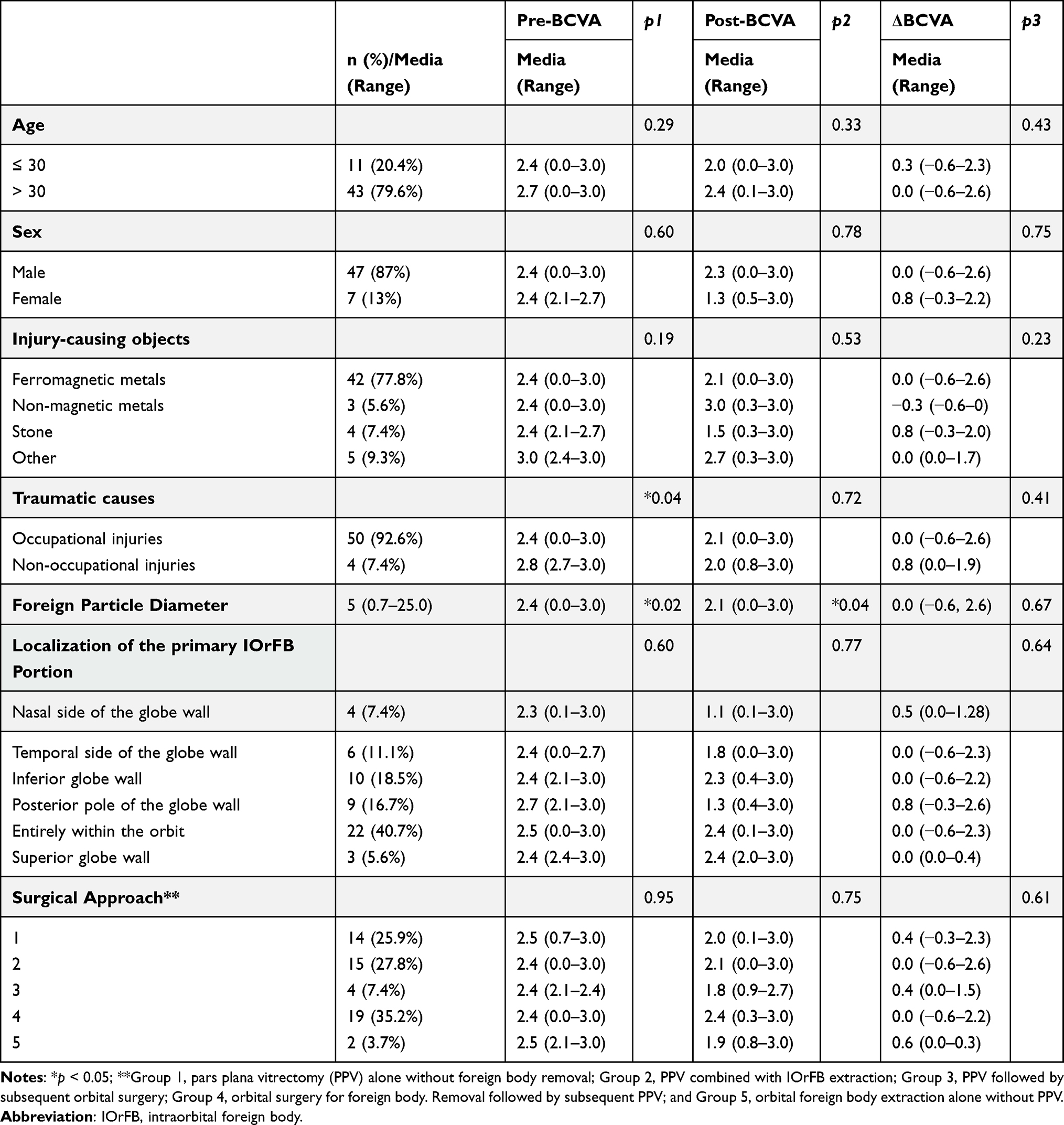 |
Table 2 Relevant Factors for Visual Outcome Among Patients Entering the Study |
With the aid of a clinical case database, we listed the total number of patients who underwent foreign bodies removal surgery in our hospital and calculated the incidence of IOrFBs from the year 2007 to 2024. We found that approximately 2571 patients underwent foreign bodies remove surgery in our hospital, and the proportion of IOcbFBs was approximately 2.1%.
Injury-Causing Objects Material, Location and Prognostic Analysis
As shown in Table 1, ferromagnetic metals were the predominant causative material, accounting for 77.8% of cases (42/54; p < 0.001), which was significantly higher than non-ferromagnetic metals (3 cases), stone (4 cases), and other materials (5 cases: wood, glass, detonator fragments, bone fragments, and concrete; one case each).
Regarding the anatomical distribution of the foreign bodies, 40.7% (22/54; p < 0.001) were entirely confined to the orbit. Other locations included the inferior globe wall (18.5%, 10 cases), posterior pole (16.7%, 9 cases), temporal globe wall (11.1%, 6 cases), nasal globe wall (7.4%, 4 cases), and superior globe wall (5.6%, 3 cases). These findings indicate that most IOrFBs were caused by high-energy projectiles or sharp objects that penetrated the globe and became lodged within the orbital cavity. Representative orbital CT images from selected patients are shown in Figure 1.
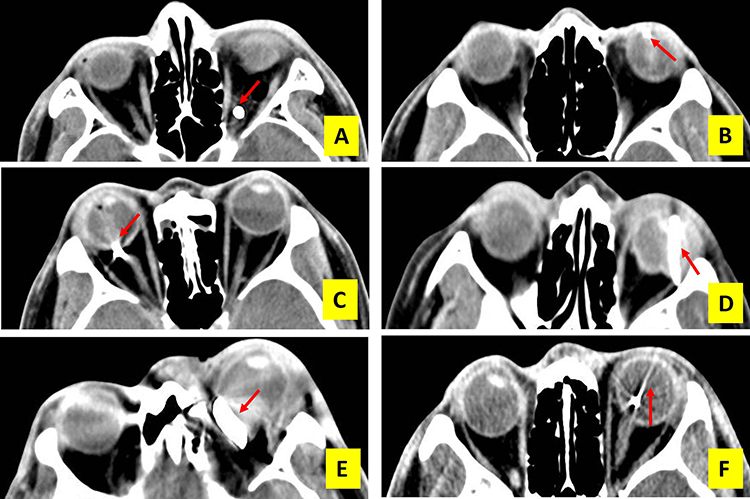 |
Figure 1 Representative orbital CT images illustrating the anatomical localization of intraorbital foreign bodies (IOrFBs). (A) Entirely intraorbital: CT shows a foreign body completely confined within the orbit; (B) Inferior globe wall involvement: CT demonstrates a foreign body at the inferior globe wall (approximately the 6:30 o’clock position) with trans-scleral extension into the orbit; (C) Posterior pole involvement: CT reveals a foreign body at the posterior pole involving the optic nerve, with trans-scleral extension into the orbit; (D) Temporal globe wall involvement: CT shows a foreign body at the temporal globe wall with trans-scleral extension into the orbit; (E) Nasal globe wall involvement: CT demonstrates a foreign body at the nasal globe wall (approximately the 7:30–8 o’clock position) with trans-scleral extension into the orbit; (F) Superior globe wall involvement: CT depicts an elongated foreign body within the vitreous cavity exiting through the superior sclera, with trans-scleral extension into the orbit. (Red arrows indicate IOrFBs). |
However, no statistically significant differences in either preoperative or postoperative visual acuity were observed among groups stratified by foreign body material or location (Table 2; p > 0.05). This indicates that, while clinically important for surgical planning, neither the anatomical distribution nor the material composition of IOrFBs independently predicted visual prognosis in this cohort.
Foreign Particle Diameter and Prognostic Analysis
In this study, the diameters of IOrFBs were measured in 54 patients with perforating ocular injuries. The mean diameter was 5.0 mm (range, 0.7–25.0 mm), reflecting the diversity of foreign body types and substantial variation in size (Table 1).
To assess the clinical significance of size, we analyzed its correlation with visual acuity. As shown in Table 2 and Figure 2, linear regression analysis demonstrated that larger IOrFB diameters were significantly associated with poorer visual acuity both preoperatively (p1 = 0.02) and postoperatively (p2 = 0.04), suggesting that larger foreign bodies may predict worse baseline and postoperative vision in this cohort.
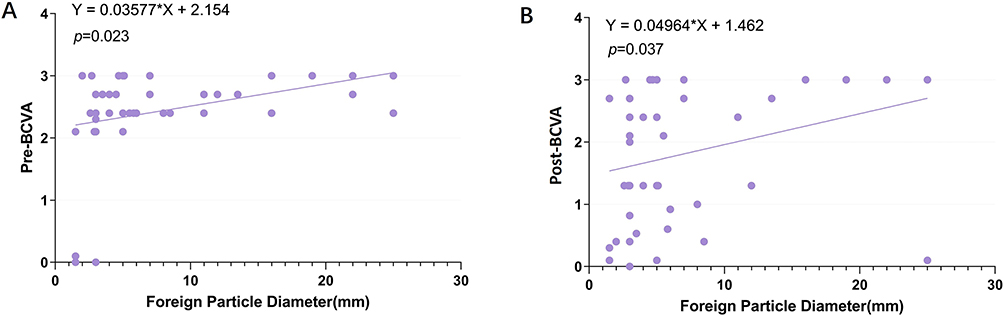 |
Figure 2 Linear regression analysis of the effect of foreign body diameter on VA in patients with perforating ocular injuries. (A) Preoperative BCVA and (B) postoperative BCVA both showed significant negative correlations with IOrFBs diameter (*p<0.05). Abbreviations: IOrFBs, intraorbital foreign bodies; BCVA, best-corrected visual acuity; Pre-BCVA, preoperative BCVA; Post-BCVA, BCVA at final follow-up. |
However, comparison of the degree of visual improvement (postoperative versus preoperative acuity) across different size groups revealed no statistically significant differences (p3 > 0.05), indicating that the extent of visual recovery following surgery is not substantially influenced by foreign body size.
Overview of Surgical Approaches and Prognostic Analysis
After primary globe repair, patients underwent PPV or orbital surgery according to their clinical condition. As shown in Table 1, five surgical approaches were employed: PPV alone (25.9%, 14 cases), PPV with concurrent foreign body removal (27.8%, 15 cases), PPV followed by subsequent orbital surgery (7.4%, 4 cases), orbital surgery followed by PPV (35.2%, 19 cases), and orbital surgery alone (3.7%, 2 cases). Orbital surgery followed by PPV was the most frequently performed approach (p < 0.001), reflecting the variety of surgical strategies required to manage these complex injuries.
As shown in Table 2, there were no statistically significant differences among the five surgical groups in preoperative BCVA, postoperative BCVA, or visual improvement (all p > 0.05). These findings suggest that, although the choice of surgical approach is clinically important for operative planning, it did not independently predict visual prognosis in this cohort.
Surgical Approaches by Injury-Causing Objects Material
All 42 patients with ferromagnetic metal IOrFBs underwent surgical intervention, with procedures tailored to individual clinical conditions. Twelve patients underwent PPV alone without foreign body removal, 13 underwent PPV combined with IOrFB extraction, 13 underwent orbital surgery for foreign body removal followed by subsequent PPV, and 4 underwent PPV followed by subsequent orbital surgery for foreign body removal. Notably, in 22.2% of all 54 patients (28.6% of those with ferromagnetic IOrFBs; 12/42), the foreign bodies remained in situ and stable at the final follow-up.
Three patients with non-ferromagnetic metal (copper) IOrFBs all underwent foreign body removal. Two patients, with foreign bodies entirely intraorbital or partly located at the temporal globe wall, underwent orbital extraction followed by PPV, while one patient, with a foreign body partially at the inferior globe wall, underwent PPV combined with IOrFB extraction.
Four patients with stone IOrFBs were treated using different management strategies. One patient, whose foreign body was entirely located within the orbit, underwent PPV alone without foreign body removal. Another patient, with a foreign body partially involving the nasal-inferior globe wall, underwent PPV combined with IOrFB extraction. A third patient, whose foreign body was partially embedded in the inferior globe wall, received orbital extraction followed by PPV. The fourth patient, whose foreign body was partially positioned at the nasal globe wall and had traversed the nasal sclera into the orbit, underwent orbital extraction alone without PPV. One patient with a glass IOrFB extending from the orbit to the posterior pole underwent orbital extraction followed by PPV.
One patient with a glass IOrFB extending from the orbit to the posterior pole underwent orbital extraction followed by PPV.
One patient with a wooden IOrFB entirely within the orbit underwent orbital extraction followed by PPV but ultimately required enucleation with hydroxyapatite implantation due to phthisis bulbi.
The remaining three patients presented with IOrFBs from uncommon sources: a detonator fragment (possibly containing copper, aluminum, and iron), bone fragments, and concrete. Of these, one (bone fragment) underwent PPV alone without removal; one (detonator fragment) underwent orbital extraction alone; and one (concrete) underwent orbital extraction followed by subsequent PPV.
Surgical Approaches by Foreign Body Location Distribution
Four patients with IOrFBs at the nasal globe wall all underwent foreign body removal: one underwent PPV after extraction, two underwent simultaneous PPV with extraction, and one underwent orbital extraction alone without PPV.
Six patients with IOrFBs at the temporal globe wall underwent foreign body removal: four underwent orbital extraction followed by PPV, and two underwent simultaneous PPV with extraction.
Ten patients with IOrFBs at the inferior globe wall underwent foreign body removal: three underwent orbital extraction followed by PPV, and seven underwent simultaneous PPV with extraction.
Three patients had IOrFBs at the superior globe wall (all presumed ferromagnetic). Their management varied: one underwent orbital extraction followed by PPV, another underwent simultaneous PPV with extraction, and one, whose ferromagnetic foreign body was minimally embedded in the superior globe wall with most of the body in the orbit, underwent PPV alone without removal.
Nine patients had IOrFBs at the posterior pole: three underwent PPV with simultaneous extraction, four underwent orbital extraction followed by PPV, one underwent PPV first followed by extraction, and one, with a minimally embedded ferromagnetic IOrFB at the optic disc and majority orbital, underwent PPV combined with intraoperative amniotic membrane transplantation without foreign body removal.
Among 22 patients with IOrFBs located entirely within the orbit, 12 (10 ferromagnetic metals, 1 stone, 1 bone fragment) underwent PPV without removal, three underwent PPV followed by orbital extraction, six underwent orbital extraction prior to PPV, and one patient with a detonator fragment underwent orbital extraction alone without PPV.
Discussion
In this retrospective cohort of Zone III perforating open-globe injuries accompanied by IOrFBs, we analyzed demographic characteristics, causative materials, foreign body size and location, and surgical strategies in relation to visual outcomes. All included cases involved posterior segment penetration, representing a clinically severe and relatively homogeneous subgroup of open-globe trauma. The injuries predominantly affected working-age males and were largely occupational in nature, consistent with prior reports highlighting the vulnerability of industrial workers to high-velocity ocular trauma.13,21–23 Many injuries occurred in factory environments involving metal grinding, cutting, drilling, or explosive mechanical forces, which generate high-speed projectiles capable of penetrating the globe. Factors such as prolonged exposure to hazardous tools, inconsistent use of protective eyewear, and limited safety supervision may further contribute to injury risk. These findings reinforce the importance of strengthened eye protection protocols, targeted safety training, and stricter enforcement of occupational health regulations in high-risk workplaces.
Ferromagnetic metals were the most common causative material, and most foreign bodies were retained predominantly within the orbital cavity. Within this Zone III perforating injury cohort, larger foreign body size was associated with poorer baseline visual acuity, whereas foreign body location (intraorbital versus intraocular extension) and surgical approach were not significantly associated with final visual outcomes. These findings should be interpreted in the context of a uniform injury zone and do not diminish the established prognostic importance of injury zone severity in open-globe trauma (Figure 2).
The optimal management of retained IOrFBs remains controversial. Decisions regarding removal are influenced by multiple factors, including size, composition, location, and potential complications associated with the foreign body. In our cohort, ferromagnetic metals were the leading cause of injury, accounting for 77.8% of cases (42/54), consistent with previous reports identifying metallic IOrFBs as the most frequent etiology in industrial settings.8,9,13 Prior studies have shown that ferromagnetic metal IOrFBs can remain in situ for periods ranging from 6 months to 68 years, with some patients ultimately requiring surgical removal due to pain, visual impairment, or other complications.12–14 These findings suggest that certain metallic foreign bodies may be well-tolerated over extended periods but can later give rise to delayed complications, emphasizing the need for long-term monitoring and timely intervention even in initially asymptomatic cases. Consistent with previous reports, 22.2% of all patients in our cohort (28.6% of those with ferromagnetic IOrFBs; 12/42) retained ferromagnetic foreign bodies that remained stable at the final follow-up.
Intraorbital wooden foreign bodies represent another clinically significant type of IOrFB associated with globe perforation. Due to their low density on CT, wooden foreign bodies can be misidentified as air or fat, resulting in missed or incorrect diagnoses.7,24,25 MRI can provide valuable complementary information, though it should be used cautiously when the composition of the foreign body is uncertain.9,25 Wooden IOrFBs are highly reactive because of their organic composition, often causing tissue necrosis, infection, or abscess formation, which may lead to severe visual loss and thus necessitate urgent removal.26–31 Moreover, organic materials can induce more extensive initial ocular damage, underscoring the importance of early detection and prompt intervention. In our cohort, one patient with a wooden IOrFB located entirely within the orbit underwent orbital extraction followed by PPV; however, the eye ultimately progressed to phthisis bulbi, requiring enucleation with hydroxyapatite implantation.
Beyond ferromagnetic metals, other reported orbital foreign bodies include glass, stone, and plastic, with varied management approaches.5,9 In our study, postoperative visual outcomes did not significantly differ between materials, suggesting that while surgical intervention may stabilize or modestly improve vision, the initial severity of the injury is likely the primary determinant of visual prognosis.
Larger IOrFB size was associated with poorer preoperative and postoperative visual acuity in the present study (Figure 2). While few previous studies have directly examined the relationship between orbital foreign body size and visual outcomes, numerous investigations of open-globe injuries have reported that larger foreign bodies cause greater ocular disruption and are associated with worse visual prognosis. For example, a retrospective cohort study of 669 patients with intraocular foreign bodies (IOFBs) classified foreign body size as small (≤ 4 mm2), medium (4–16 mm2), or large (> 16 mm2). Patients with larger IOFBs had significantly poorer final visual acuity, with 45.3% achieving <20/200, whereas 50.3% of patients in the small-size group achieved ≥20/40 vision.32 Similarly, a medium-sized cohort study identified maximum IOFB volume (measured by diameter or length) as an independent predictor of postoperative visual outcomes, indicating that larger foreign body volume correlates with poorer visual prognosis.33
The management of foreign bodies located entirely or predominantly within the orbit remains debated. In our series, among 22 patients with IOrFBs entirely within the orbit, 12 (10 ferromagnetic metals, 1 stone, 1 bone fragment) underwent PPV without foreign body removal. Additionally, two patients with ferromagnetic foreign bodies minimally embedded in the superior or posterior globe wall, with the majority located in the orbit, also underwent PPV alone. This conservative approach was considered appropriate given the absence of active infection, compressive optic neuropathy, or other indications for urgent removal, as well as the elevated risk of iatrogenic ocular or orbital injury during extraction. Inert materials that do not pose immediate threats may therefore be managed conservatively.
Selected cases may benefit from conservative management, minimizing surgical morbidity while achieving satisfactory anatomical and visual outcomes. Prior studies support this approach, reporting that inert metallic or inorganic IOrFBs, particularly when posterior and asymptomatic, can be safely retained.34 Nonetheless, careful long-term follow-up is essential to monitor for delayed complications, including migration, chronic inflammation, or secondary infection.12–14 These findings highlight the need for individualized treatment planning and further research to clarify the indications for surgical removal versus retention of intraorbital foreign bodies.
Given that all included cases represented Zone III open-globe injuries, comparisons of visual outcomes across different injury zones could not be performed. Consequently, the absence of a significant association between foreign body location and baseline visual acuity in this study reflects findings within a homogeneous Zone III injury cohort and should not be extrapolated to open-globe injuries of other zones, in which injury location remains an important prognostic factor.
This study is limited by its retrospective, single-center design, which may restrict the generalizability of the findings. Potential selection bias and incomplete medical records could have affected the accuracy of the collected variables. In addition, the limited sample size and the absence of multivariate analyses mean that observed associations should not be interpreted as independent prognostic factors. Other relevant prognostic variables, such as surgical timing or concomitant ocular injuries, were not fully evaluated, and long-term visual function and quality-of-life outcomes were not assessed. These limitations should be considered when interpreting the study results.
In summary, ferromagnetic metals were the most common cause of perforating ocular injuries with IOrFBs in our cohort, predominantly affecting work-related individuals and often located entirely within the orbit. Larger foreign body size was associated with worse baseline visual acuity, emphasizing the importance of early detection and timely intervention. However, neither foreign body location nor surgical approach independently influenced final visual outcomes, suggesting that prompt and appropriate surgical management can effectively address the anatomical complexity of these injuries.
Conclusions
This study demonstrates that perforating ocular injuries with IOrFBs predominantly affect male laborers, with occupational ferromagnetic foreign bodies as the major cause. Larger IOrFBs were strongly associated with poorer visual outcomes, whereas foreign body location and surgical approach had limited impact. These findings underscore the importance of early diagnosis, timely intervention, and reinforced workplace eye-safety measures to reduce injury incidence. Continued research is needed to optimize surgical management and improve visual rehabilitation.
Ethics Approval
This study was reviewed and approved by the Ethics Committee of the Eye and ENT Hospital of Fudan University (Reference No. 2024146; August 2024). Given that this was a retrospective clinical study using previously collected data and did not involve any intervention or additional risk to patients, and that all data were anonymized, the requirement for individual informed consent was waived by the Committee. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We thank Dr. Jing Wang, also as a data analyst, for her sincere efforts and valuable assistance in statistical work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by National Natural Science Foundation of China (grant nos. 82101087 to LN, grant nos. 82201226 to HX).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Pieramici DJ, Sternberg P, Aaberg TM, et al; The Ocular Trauma Classification Group. A system for classifying mechanical injuries of the eye (globe). Am J Ophthalmol. 1997;123(6):820–12. doi:10.1016/s0002-9394(14)71132-8
2. Kuhn F, Morris R, Witherspoon CD. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am. 2002;15(2):139–143. doi:10.1016/s0896-1549(02)00004-4
3. Kuhn F, Morris R, Witherspoon CD, Mester V. The Birmingham Eye Trauma Terminology system (BETT). J Fr Ophtalmol. 2004;27(2):206–210. doi:10.1016/s0181-5512(04)96122-0
4. Martin DF, Meredith TA, Topping TM, Sternberg P, Kaplan HJ. Perforating (through-and-through) injuries of the globe. Surgical results with vitrectomy. Arch Ophthalmol. 1991;109(7):951–956. doi:10.1001/archopht.1991.01080070063036
5. Chai GR, Chen M, Song ZX, Liu L. Clinical features, radiological imaging, and treatment strategies of nonmetallic intraorbital foreign bodies: a retrospective analysis. Int J Ophthalmol. 2023;16(7):1130–1137. doi:10.18240/ijo.2023.07.19
6. Kanu LN, Jiang Y, Gonzalez AF, Mieler WF. Visual and anatomic outcomes in perforating ocular injuries. J Vitreoretin Dis. 2019;3(6):428–437. doi:10.1177/2474126419865992
7. Lakshmanan A, Bala S, Belfer KF. Intraorbital organic foreign body--a diagnostic challenge. Orbit. 2008;27(2):131–133. doi:10.1080/01676830701512650
8. Szabo B, Pascalau R, Bartoè D, Bartos A, Szabo I. Intraorbital penetrating and retained foreign bodies - a neurosurgical case series. Turk Neurosurg. 2019;29(4):538–548. doi:10.5137/1019-5149.JTN.24265-18.2
9. You Y, Wang X, Cheng S, et al. Clinical analysis of 96 patients with intraorbital foreign bodies: a 10-year retrospective study. Front Med. 2022;9:1018905. doi:10.3389/fmed.2022.1018905
10. Sheng I, Bauza A, Langer P, Zarbin M, Bhagat N. A 10-year review of open-globe trauma in elderly patients at an urban hospital. Retina. 2015;35(1):105–110. doi:10.1097/IAE.0000000000000261
11. Rahman I, Maino A, Devadason D, Leatherbarrow B. Open globe injuries: factors predictive of poor outcome. Eye. 2006;20(12):1336–1341. doi:10.1038/sj.eye.6702099
12. Ho VH, Wilson MW, Fleming JC, Haik BG. Retained intraorbital metallic foreign bodies. Ophthalmic Plast Reconstr Surg. 2004;20(3):232–236. doi:10.1097/01.iop.0000129014.94384.e6
13. Hung KH, Yang CS, Kao SC, Lee FL, Lee SM. Management of double-penetrating ocular injury with retained intraorbital metallic foreign body. J Chin Med Assoc. 2011;74(11):523–526. doi:10.1016/j.jcma.2011.09.010
14. Germano C, Fossataro F, Abbate V, et al. Delayed presentation of an intraorbital metallic foreign body: a case report and surgical intervention. Cureus. 2025;17(2):e79701. doi:10.7759/cureus.79701
15. Mittal P, Verma V, Singh P, Ahuja N. Successful management of a rare intraorbital wooden foreign body extending to the orbital apex in a paediatric patient. BMJ Case Rep. 2025;18(3):e264403. doi:10.1136/bcr-2024-264403
16. Brunnquell CL, Vasconcelos AG, Hoff MN, et al. A comparison of radiography, X-Ray tomosynthesis, and CT for intraorbital metallic foreign body screening. J Am Coll Radiol. 2025;22(3):386–394. doi:10.1016/j.jacr.2024.12.002
17. Ayalon A, Fanadka F, Levov D, Saabni R, Moisseiev E. Detection of intraorbital foreign bodies using magnetic resonance imaging and computed tomography. Curr Eye Res. 2021;46(12):1917–1922. doi:10.1080/02713683.2021.1945108
18. Han SL, Wang TT, Wen Y, Liu LB, Zhao R. Management of multiple non-magnetic intraocular and intraorbital foreign bodies following a motor vehicle accident: a case report. Front Med. 2025;12:1519711. doi:10.3389/fmed.2025.1519711
19. Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including ‘counting fingers’, ‘hand movement’, ‘light perception’ and ‘no light perception’ and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2021;99(6):e963–e965. doi:10.1111/aos.14659
20. Lange C, Feltgen N, Junker B, Schulze-Bonsel K, Bach M. Resolving the clinical acuity categories “hand motion” and “counting fingers” using the Freiburg Visual Acuity Test (FrACT). Graefes Arch Clin Exp Ophthalmol. 2009;247(1):137–142. doi:10.1007/s00417-008-0926-0
21. Zhou Y, DiSclafani M, Jeang L, Shah AA. Open globe injuries: review of evaluation, management, and surgical pearls. Clin Ophthalmol. 2022;16:2545–2559. doi:10.2147/OPTH.S372011
22. Cui Y, Li Z, Wang Y, Shi L. Removal of an intraorbital metallic foreign body following double-penetrating ocular injury: a case report. Medicine. 2018;97(51):e13790. doi:10.1097/MD.0000000000013790
23. Chen J, Shen T, Wu Y, Yan J. Clinical characteristics and surgical treatment of intraorbital foreign bodies in a tertiary eye center. J Craniofac Surg. 2015;26(6):e486–9. doi:10.1097/SCS.0000000000001973
24. Adesanya OO, Dawkins DM. Intraorbital wooden foreign body (IOFB): mimicking air on CT. Emerg Radiol. 2007;14(1):45–49. doi:10.1007/s10140-007-0576-2
25. Nadarajasundaram A. Organic foreign body in the eye, a diagnostic challenge: a case of a wooden, intra-orbital foreign body presenting at the emergency department. Cureus. 2024;16(12):e75011. doi:10.7759/cureus.75011
26. Singh P, Desai A, Das D, Bajaj MS. Large wooden orbital foreign body: case report and literature review. Trop Doct. 2021;51(2):235–237. doi:10.1177/0049475520946167
27. Li J, Zhou LP, Jin J, Yuan HF. Clinical diagnosis and treatment of intraorbital wooden foreign bodies. Chin J Traumatol. 2016;19(6):322–325. doi:10.1016/j.cjtee.2016.04.006
28. Song C, Li J, Wang T, et al. CT and MRI findings of intraorbital wooden foreign bodies. Clin Radiol. 2025;84:106859. doi:10.1016/j.crad.2025.106859
29. You YY, Shi BJ, Wang XY, et al. Intraorbital wooden foreign bodies: case series and literature review. Int J Ophthalmol. 2021;14(10):1619–1627. doi:10.18240/ijo.2021.10.21
30. Hwang K, Park CY. Intraorbital Wooden Foreign Body in a Soldier. J Craniofac Surg. 2023;34(6):e592–e593. doi:10.1097/SCS.0000000000009482
31. Grewal AM, Singh M, Yadav D, et al. Long-term ophthalmic anatomical and functional outcomes after surgical removal of intraorbital foreign bodies. Eur J Ophthalmol. 2021;31(1):263–270. doi:10.1177/1120672119885587
32. Gao YZ, Zhang YF, Zhang M, Xu HY, Jin XR. Clinical characteristics and prognostic factors for visual outcome in 669 patients with intraocular foreign bodies. Int J Ophthalmol. 2021;14(5):759–765. doi:10.18240/ijo.2021.05.18
33. Xing X, Liu F, Qi Y, Li J, Yu B, Wan L. Clinical characteristics and prognostic factors of patients with intraocular foreign bodies from a tertiary eye center in North China. Clin Ophthalmol. 2024;18:3635–3643. doi:10.2147/OPTH.S492986
34. Khanam S, Agarwal A, Goel R, et al. Clinical presentation and management strategies in intraorbital foreign bodies. Case Rep Ophthalmol Med. 2021;2021:6645952. doi:10.1155/2021/66459
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.