Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Classical Dermatomyositis: A Case Report
Authors Pokhrel S ![]() , Pardhe BD
, Pardhe BD ![]() , Giri N, Pokhrel R, Paudel D
, Giri N, Pokhrel R, Paudel D ![]()
Received 12 October 2019
Accepted for publication 22 January 2020
Published 5 February 2020 Volume 2020:13 Pages 123—126
DOI https://doi.org/10.2147/CCID.S234452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sushant Pokhrel,1,2 Bashu Dev Pardhe,1,3 Nisha Giri,2 Rakesh Pokhrel,2,4 Deliya Paudel2,5
1Department of Laboratory Medicine, Manmohan Memorial Institute of Health Sciences, Kathmandu, Nepal; 2Modern Diagnostic Laboratory and Research Center, Kathmandu, Nepal; 3Department of Life Science and Biochemical Engineering, Sun Moon University, Asan-Si, Chungnam, South Korea; 4Institute of Medicine, Tribhuvan University, Kathmandu, Nepal; 5Manmohan Memorial Medical College and Teaching Hospital, Kathmandu, Nepal
Correspondence: Sushant Pokhrel
Department of Laboratory Medicine, Manmohan Memorial Institute of Health Sciences, PO Box No: 15201, Kathmandu, Nepal
Tel +977-1-4030781
Email [email protected]
Abstract: Dermatomyositis is an idiopathic myopathy involving progressive muscle weakness with skin manifestation. Diagnosis is based upon the progressive muscle weakness, skin rashes, elevated serum muscle enzymes, muscle biopsy, and abnormal electromyogram. The incidence of dermatomyositis is rare. In this case study, we report a case of classical dermatomyositis without incidence of malignancy. Timely diagnosis and administration of steroid led to better prognosis of the patient.
Keywords: dermatomyositis, myopathy, creatinine phosphokinase
Introduction
Dermatomyositis (DM), a connective tissue disorder, is an idiopathic inflammatory myopathy characterized by skin manifestation. It occurs in both juvenile and adult forms. The prevalence of dermatomyositis is 1 in 100,000 while women are more affected than men.1,2 The diagnosis of dermatomyositis is based on rashes on the skin, progressive muscle weakness, elevated serum muscle enzymes, abnormal electromyogram, and abnormal findings on muscle biopsy.3
Dermatomyositis has a typical cutaneous feature such as erythema over the face, neck, and upper trunk as “neck-line V-shaped.”4 Photosensitivity and pruritis are other common cutaneous symptoms. Muscle symptoms include mild to severe weakness, muscle cramps, and fatigue. Dyspnea, dysphagia, and weight loss are frequent signs of disease progression or underlying malignancy.4 To the best of our knowledge no cases are reported from Nepal to date. There are no typical signs and symptoms for the diagnosis of dermatomyositis. We reported a female patient with the features of dermatomyositis.
Case Description
A 44-year-old female patient living in Purano-baneshwor, Kathmandu, Nepal was referred from the National Center for Rheumatic disease (NCRD) for laboratory investigation in the Modern Diagnostic Laboratory and Research Center on 24 July 2019, presenting with hyperpigmented erythematous rash all over her body along with V-shaped rashes on the neckline since 2 months. Initial symptoms as mentioned by the patient included itchy rashes and photosensitivity. She had no history of headache, fever, and weight loss with a normal vital test. In addition, she had no surgical as well as medical history of chronic disease. She had progressed symptoms like muscle pain (especially in the left arm and thigh), unable to walk upstairs, inability to stretch hands, unable to turn neck, and difficulty in swallowing food.
Laboratory Findings
Physical examination showed signs of inflammation supported by laboratory findings, i.e. erythrocyte sedimentation rate (ESR) done by Wintrobe’s method found to be 30 mm/1st hour (normal 0–20 mm/1st hour), leukocytosis (14,920 cells/µL) with neutrophilia 13,080 cells/µL (normal range 2500–8000 cells/µL), and carbohydrate reactive protein (CRP) done by nephelometry found to be 25.3 mg/L (normal <3 mg/L). Hematological parameters were measured using Sysmex XN-350 and are presented in Table 1. Biochemical parameters (Table 2) were measured by a fully automated Dimension RxL Max integrated chemistry analyzer that revealed an elevated level of serum creatinine kinase 17,160 IU/L (normal 26–192 IU/L), and normal plasma glucose level and renal function test. Her liver enzymes revealed an elevated level of alanine aminotransferase (ALT), i.e. 370 IU/L (normal 5–45 IU/L), and aspartate aminotransferase (AST) 616 IU/L (normal 5–45 IU/L). Nailfold capillaroscopy of 8 fingers findings showed variant and simple Raynaud's. Urine analysis, chest X-ray, and thyroid function test were normal. Serum lactate dehydrogenase (LDH) 1657 IU/L (reference 25–250 IU/L), Jo-1 antibodies, and dsDNA antibodies were negative while anti-Mi-2 antibody was positive. Raynaud’s phenomenon and anti-Mi-2 antibody are highly specific to dermatomyositis. Based on the above findings, a diagnosis of dermatomyositis was made.
 |
Table 1 Hematological Parameters of the Dermatomyositis Patient During Diagnostic Work-Up |
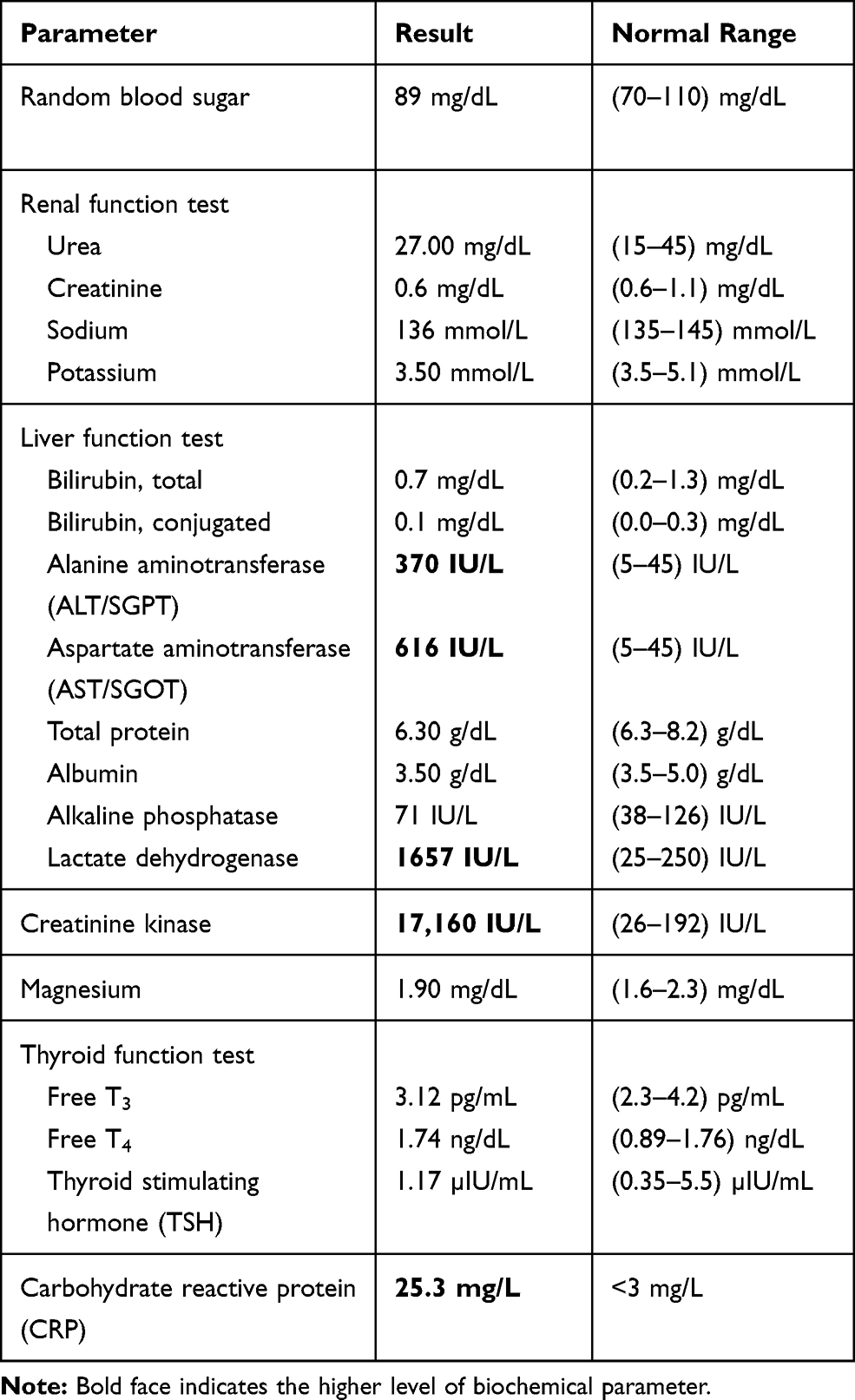 |
Table 2 Biochemical Parameters of the Dermatomyositis Patient During Diagnosis |
She was administered with 50 mg prednisolone with a significant improvement of muscular activities within a month; with a modest fall in serum creatinine kinase level as shown in Table 3 and 25 mg azathioprine once a day as immunosuppressive drugs. At present, she is orally administered 50 mg prednisolone therapy for maintenance therapy and still being followed up.
 |
Table 3 CPK Level After Treatment |
Discussion
Dermatomyositis is classified into classical dermatomyositis, amyopathic dermatomyositis, juvenile dermatomyositis, hypomyopathic dermatomyositis, clinically amyopathic dermatomyositis, and clinical lyamyopathic evolving into classic.5 The patient showed cutaneous manifestation with evidence of myalgia occurring within 1 month after the onset of skin disease, which is classical dermatomyositis. In the older age group, the incidence of malignancy is higher in dermatomyositis. The common malignancies are ovarian cancer, colon cancer, melanoma, breast cancer, and non-Hodgkin’s lymphoma, while in the Asian population nasopharyngeal cancer is common.6
The patient showed typical features for diagnosis of dermatomyositis such as progressive muscle weakness, elevated muscle enzyme, dysphagia, and erythematous rashes all over the body with positive anti-Mi-2 antibody, which is specific to dermatomyositis. Treatment is based on high-dose prednisolone until clinical and biochemical remission is obtained. Initially, CPK levels were higher; however, on treatment with steroid, the patient responded well and the CPK level reduced significantly,7 which is similar to our study represented in Table 3. Decrease in the level of CPK is a good prognostic factor in dermatomyositis patients.8
Mi-2 antigen, nuclear helicase protein, forms part of the nucleosome remodeling deacetylase (NuRD) complex involved in transcription regulation.9 Mi-2 is expressed highly in developing hair follicles and embryonic ectoderm, which plays a critical role in the development of epidermis.10 Mi-2 is also essential for differentiation and renewal of the basal epidermis.11 Immune response to Mi-2 protein leads to the development of skin rashes and production of anti-mi-2 antibody.12 Anti-Mi-2 is associated with typical skin manifestation where ultraviolet radiation intensity may have an important role in initiating the disease. Sunlight plays a significant role in anti-Mi-2 production through subcellular distribution, expression, and metabolism of the components of Mi-2 antigens.13 Mi-2 expression is regulated by UV radiation through protein translation and stability.14 A patient with anti-Mi-2 antibody presents cutaneous lesions and mild to moderate muscle involvement and responds well to glucocorticoid therapy. Our patient did not have any evidence of malignancy and showed better prognosis. However, recurrence of disease is rare but rashes on skin and retractable myositis can occur, and monitoring and follow-up are needed for the patients.15
This dermatomyositis patient showed typical clinical manifestation with increased muscle enzymes along with increased liver enzymes. Anti-Mi-2 antibody positive, the patient showed less evidence of malignancy. Proper management and therapy leads to better prognosis of the disease.
Consent
The patient had given written informed consent for the publication of her clinical details. Institutional approval is not required for this case study.
Acknowledgment
We thank the patient for participating in the study. Our special thanks go to all the laboratory staff, management, and officials of the Modern Diagnostic Laboratory and Research Center, Kathmandu for providing the opportunity to carry out the case report work.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kalyan M, Kanitkar S, Gaikwad A, Kumar H. Dermatomyositis: a case report. J Mahatma Gandhi Inst Med Sci. 2016;21(1):53–55. doi:10.4103/0971-9903.178107
2. Marvi U, Chung L, Fiorentino DF. Clinical presentation and evaluation of dermatomyositis. Indian J Dermatol. 2012;57(5):375–381. doi:10.4103/0019-5154.100486
3. Bohan A, Peter JB. Polymyositis and dermatomyositis (Second of two parts). N Engl J Med. 1975;292(8):403–407. doi:10.1056/NEJM197502202920807
4. Papakonstantinou E, Kapp A, Raap U. A mild form of dermatomyositis as a prodromal sign of lung adenocarcinoma: a case report. J Med Case Rep. 2016;10(1):34. doi:10.1186/s13256-016-0816-8
5. Gerami P, Schope JM, McDonald L, Walling HW, Sontheimer RD. A systematic review of adult-onset clinically amyopathic dermatomyositis (dermatomyositis sine myositis): a missing link within the spectrum of the idiopathic inflammatory myopathies. J Am Acad Dermatol. 2006;54(4):597–613. doi:10.1016/j.jaad.2005.10.041
6. Dalakas MC. Polymyositis, dermatomyositis and inclusion-body myositis. In: Braunwald ELD, Fauci AS, Kasper DL, et al., editors. Harrison’s Principles of Internal Medicine,
7. Petri MH, Satoh M, Martin-Marquez BT, et al. Implications in the difference of anti-Mi-2 and -p155/140 autoantibody prevalence in two dermatomyositis cohorts from Mexico City and Guadalajara. Arthritis Res Ther. 2013;15(2):R48. doi:10.1186/ar4207
8. Fudman EJ, Schnitzer TJ. Dermatomyositis without creatine kinase elevation. A poor prognostic sign. Am J Med. 1986;80(2):329–332.
9. Ghirardello A, Zampieri S, Iaccarino L, et al. Anti-Mi-2 antibodies. Autoimmunity. 2005;38(1):79–83. doi:10.1080/08916930400022681
10. Mammen AL, Casciola-Rosen LA, Hall JC, Christopher-Stine L, Corse AM, Rosen A. Expression of the dermatomyositis autoantigen Mi-2 in regenerating muscle. Arthritis Rheum. 2009;60(12):3784–3793. doi:10.1002/art.v60:12
11. Kashiwagi M, Morgan BA, Georgopoulos K. The chromatin remodeler Mi-2beta is required for establishment of the basal epidermis and normal differentiation of its progeny. Development. 2007;134(8):1571–1582. doi:10.1242/dev.001750
12. Fujimoto M. Dermatomyositis: myositis‐specific autoantibodies and skin manifestations. Clin Exp Neuroimmunol. 2012;3.
13. Okada S, Weatherhead E, Targoff IN, Wesley R, Miller FW. Global surface ultraviolet radiation intensity may modulate the clinical and immunologic expression of autoimmune muscle disease. Arthritis Rheum. 2003;48(8):2285–2293. doi:10.1002/(ISSN)1529-0131
14. Burd CJ, Kinyamu HK, Miller FW, Archer TK. UV radiation regulates Mi-2 through protein translation and stability. J Biol Chem. 2008;283(50):34976–34982. doi:10.1074/jbc.M805383200
15. Hamaguchi Y, Kuwana M, Hoshino K, et al. Clinical correlations with dermatomyositis-specific autoantibodies in adult japanese patients with dermatomyositis: a multicenter cross-sectional study. JAMA Dermatol. 2011;147(4):391–398. doi:10.1001/archdermatol.2011.52
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.