Back to Journals » International Medical Case Reports Journal » Volume 13
Chronic, Recurrent Bacterial Endophthalmitis Caused by Achromobacter xylosoxidans: Clinical Features and Management
Authors Lazzarini TA ![]() , Al-khersan H, Patel NA
, Al-khersan H, Patel NA ![]() , Yannuzzi NA, Martinez JD
, Yannuzzi NA, Martinez JD ![]() , Altamirano D, Torres LK, Miller D
, Altamirano D, Torres LK, Miller D ![]() , Batlle JF
, Batlle JF ![]() , Amescua G, Flynn HW Jr
, Amescua G, Flynn HW Jr ![]()
Received 25 April 2020
Accepted for publication 8 June 2020
Published 9 July 2020 Volume 2020:13 Pages 265—269
DOI https://doi.org/10.2147/IMCRJ.S259899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Thomas A Lazzarini,1 Hasenin Al-khersan,1 Nimesh A Patel,1 Nicolas A Yannuzzi,1 Jaime D Martinez,1 Diego Altamirano,1 Lizt K Torres,2 Darlene Miller,1 Juan F Batlle,1,2 Guillermo Amescua,1 Harry W Flynn Jr1
1Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami, Miller School of Medicine, Miami, FL, 33136, USA; 2Laser Center, Santo Domingo, Dominican Republic
Correspondence: Thomas A Lazzarini
Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami, Miller School of Medicine, 900 NW 17th Street, Miami, FL 33136, USA
Tel +1 305 326-6118
Fax +1 305 326-6417
Email [email protected]
Abstract: A 79-year-old man presented to a tertiary referral center from the Dominican Republic with an opaque corneal graft and a diagnosis of chronic, recurrent culture-positive Achromobacter xylosoxidans endophthalmitis of the left eye. The patient had a history of penetrating keratoplasty for Fuchs’ dystrophy and had undergone multiple intraocular surgeries including pars plana vitrectomy and anterior chamber wash out for the diagnosis and management of chronic endophthalmitis. After being referred, the patient underwent a third PKP, removal of his intraocular lens (IOL), capsulectomy, and injection of intravitreal antibiotics. All surgical specimens demonstrated the growth of A. xylosoxidans. Five months after surgery, the graft remained clear without evidence of infection and best-corrected visual acuity was 20/350.
Keywords: endophthalmitis, Achromobacter xylosoxidans, ophthalmlology, postoperative endophthalmitis, ophthalmic infection
Introduction
Chronic postoperative endophthalmitis is diagnostically challenging as patients often present months or years after surgery.1 Achromobacter xylosoxidans is a motile gram-negative rod causing endophthalmitis either acutely or chronically, up to 5 years postoperatively.2–5
A. xylosoxidans is an important ophthalmic pathogen that contaminates surgical fluids and contact lens solution, coating surfaces with biofilm.6,7 The species’ broad antibiotic resistance profile is due to molecular efflux pumps,8 which render most isolates impervious to empiric anti-Pseudomonal therapy.9,10 Achromobacter is difficult to distinguish from Pseudomonas spp. in the laboratory, and misidentification leads to inappropriate treatment.9,11
A. xylosoxidans endophthalmitis case series have demonstrated that intraocular antibiotics alone are often insufficient and that removal of the IOL and lens capsule are frequently needed to achieve resolution of the infection.3,4 The current report describes a patient with chronic A. xylosoxidans endophthalmitis who had undergone pars plana vitrectomy and an anterior chamber washout without resolution of infection, whose infection finally resolved after repeated PKP, removal of his IOL and capsular bag.
Case Report
A 79-year-old man with a history of Fuch’s dystrophy presented to a tertiary referral center with chronic, recurrent Achromobacter xylosoxidans endophthalmitis of the left eye. The patient presented to his ophthalmologist in the Dominican Republic five months after penetrating keratoplasty with pain and reduced vision several days after freshwater exposure while on a hike in the forest. He was found to have inferior edema of his corneal graft without ulceration or hypopyon and was started on topical moxifloxacin, fortified vancomycin and fortified gentamicin every two hours. After two weeks of topical therapy, he developed an anterior chamber hypopyon with fibrin deposition. His ocular ultrasound (Figure 1A) and examination were consistent with endophthalmitis.
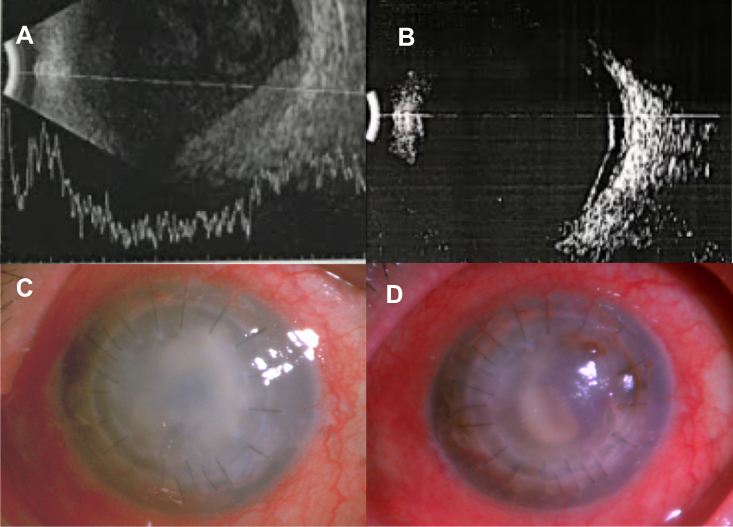 |
Figure 1 Clinical images of Achromobacter xylosoxidans endophthalmitis. (A) Ultrasonography performed when the patient presented with anterior chamber hypopyon revealed preretinal membranes suggestive of endophthalmitis which prompted pars plana vitrectomy. (B) Post-vitrectomy ultrasonography revealed improvement in vitreous membranes and vitiritis but demonstrated a retinal detachment. The retinal detachment was repaired with a second vitrectomy with the use of silicone oil tamponade. (C) Four months following initial vitrectomy for endophthalmitis, the patient presented with an opacified corneal graft and anterior chamber membranes suggestive of recurrent infection. The patient underwent anterior chamber washout with empiric intracameral injection of vancomycin (1mg/0.1cc) and amphotericin B (5mcg/0.1cc). Anterior chamber fluid samples submitted to microbiology grew Achromobacter xylosoxidans. (D) Following the anterior chamber washout and intracameral antimicrobial injections, the corneal haze and anterior chamber membranes improved, but there was recurrence of a corneal endoplaque indicating persistent infection. |
He underwent pars plana vitrectomy with intravitreal injection of vancomycin (1mg/0.1cc) and ceftazidime (2.25mg/0.1cc). The infection appeared to resolve and his topical antibiotics were tapered. His postoperative course was complicated by retinal detachment, which was detected on ultrasound three weeks postoperatively (Figure 1B), so he underwent repeated vitrectomy with injection of silicone oil (SO). One month after his initial vitrectomy, he was found to have a new endothelial plaque in his corneal graft which resolved within two weeks on fortified vancomycin and gentamicin eyed drops. After another two weeks, the endothelial deposits recurred and did not resolve with additional topical therapy. Six weeks later and a total of four months after his initial vitrectomy for endophthalmitis, the patient developed pain and was observed to have inflammatory membranes in the anterior chamber (Figure 1C), which prompted anterior chamber washout and intracameral injection of vancomycin (1mg/0.1cc) and Amphotericin B (5mcg/0.1cc). His anterior chamber paracentesis sample grew Achromobacter xylosoxidans, and despite targeted topical therapy, the endothelial plaque returned (Figure 1D) and the patient was referred for evaluation at a tertiary referral center.
Upon presentation to our center, the patient had light perception only visual acuity and an intraocular pressure (IOP) of 45 mmHg in the left eye. His anterior segment exam revealed an opacified corneal graft with paracentral thinning, no corneal epithelial defects, a retrocorneal plaque, and no view into the anterior chamber (Figure 2A and B). He denied pain and had minimal conjunctival injection. The patient underwent removal of his graft, IOL and capsular bag removal, and repeat PKP in the left eye. SO was prolapsed forward from the vitreous cavity through the open-sky by manipulating the pars plana infusion cannula. The SO did not appear infected, so the remainder was left in place. The patient received intravitreal vancomycin (1.0 mg/0.1cc) and ceftazidime (2.25mg/0.1cc) and Sub-Tenons Triamcinolone (40mg/cc).
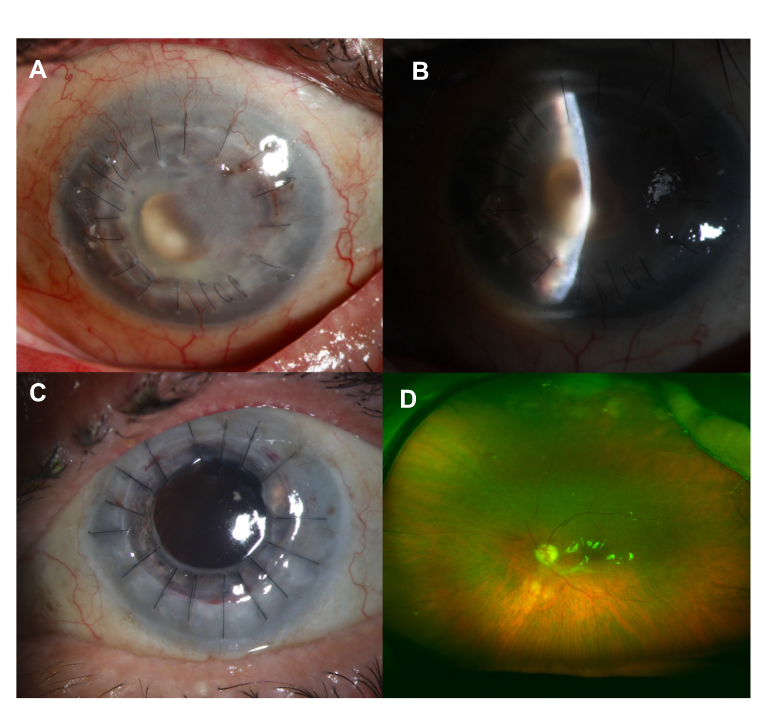 |
Figure 2 Clinical images of chronic, recurrent Achromobacter xylosoxidans endophthalmitis. (A) At the time of presentation to a tertiary center, slit lamp photography demonstrated minimal conjunctival injection and an opacified corneal graft with an endoplaque, which is highlighted with a narrowed beam (B). (C) Five months after repeat penetrating keratoplasty, removal of intraocular lens and lens capsule, and intravitreal injection of antibiotics, the patient’s corneal graft remained clear. (D) The patient’s retina remained attached under silicone oil with a focus of fibrovascular proliferation at the inferotemporal margin of the optic disc. |
Pathological evaluation of the cornea button, lens capsule, and IOL demonstrated inflammation but no organisms. Samples of each were initially reported to grow Pseudomonas fluorescens. On day thirteen, the pathogen was identified as multidrug resistant A. xylosoxidans (Table 1). Five months following surgery, the patient’s visual acuity improved to 20/350 with aphakic correction and his IOP was 10 mmHg. His graft has remained clear and there was no evidence of infection or intraocular inflammation (Figure 2C and D).
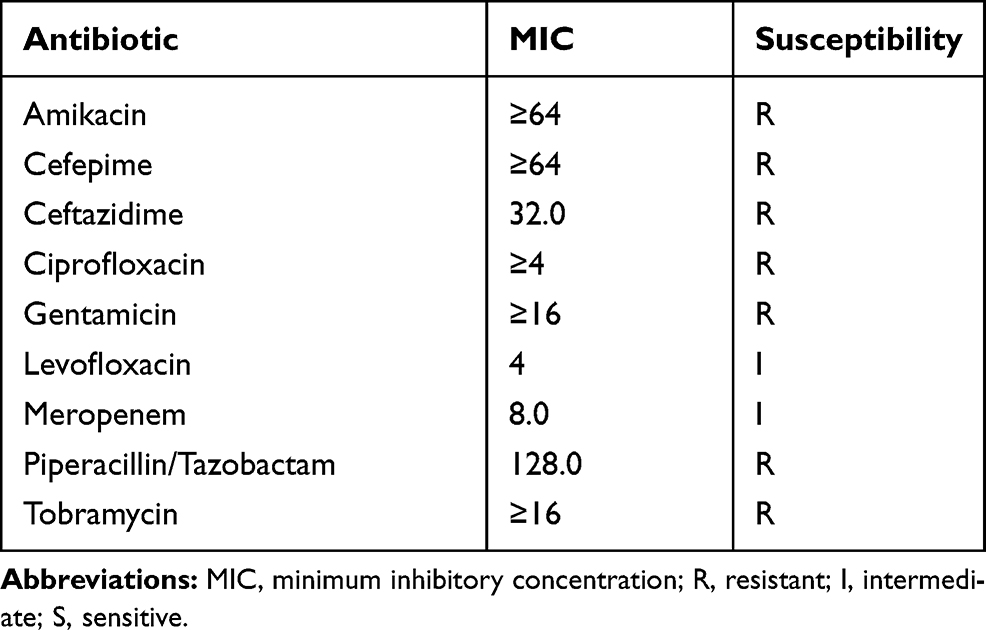 |
Table 1 Antibiotic Susceptibility Profile of Clinical Achromobacter xylosoxidans Isolate |
Discussion
Herein, we report an atypical case of chronic exogenous Achromobacter xylosoxidans endophthalmitis in the left eye of a patient with a complicated ophthalmic history. His clinical course highlights unique challenges in the diagnosis and management of chronic endophthalmitis. The patient presented to our tertiary referral clinic with marked vision loss, but there was no view into the anterior chamber through his opaque graft to assess for the most common features seen in chronic endophthalmitis – hypopyon, keratic precipitates, or a plaque associated with the capsular bag.1 In light of his clinical course marked by recurrent endophthalmitis and a recent positive anterior chamber culture from the referring site, surgical management was elected to achieve definitive diagnosis and visual rehabilitation.
Chronic A. xylosoxidans endophthalmitis most often occurs after cataract surgery3,4,12 and has never been reported as a complication of infectious keratitis. The patient’s most recent ophthalmic surgery was penetrating keratoplasty, and his graft had remained clear for five months without evidence of infection, suggesting the infection was unlikely to be related to the surgery, though donor rim cultures were not available. The most likely etiology of the patient’s infection was contamination through fresh water exposure given the ubiquitous presence of A. xylosoxidans in the environment,13–15 and the development of corneal findings days after the exposure. Therefore, this likely represents the first reported case of A. xylosoxidans keratitis progressing to endophthalmitis. A. xylsoxidans is known to deeply infiltrate the cornea16 through which it could have directly entered the anterior chamber, or the organism could have migrated along a corneal suture.
This case additionally highlights that current automated microbiology kits have difficulty in rapidly differentiating between Achromobacter xylosoxidans and Pseudomonas species recovered from clinical infections.17 This patient’s isolate was initially identified as Pseudomonas fluorescens (99%-Vitek2, BioMeriuex, Raliegh, NC, USA) but ultimately identified as Achromobacter xylsoxidans (99%-Vitek2) upon repeat testing and confirmation with a manual commercial kit (APINE, BioMeriuex, Raleigh, NC, USA).
Roberts et al published a case series describing 5 patients with acute postoperative A. xylosoxidans endophthalmitis following cataract surgery by the same surgeon on the same day.18 A contamination investigation revealed “massive colonization of the phacoemulsifier irrigation channels by Pseudomonas fluorescens.” The authors concluded that the source of the patients’ infections was unknown because the bacteria isolated from the phacoemulsifier device was different from the identical strains isolated from the patients.
Our case and other reports of Achromobacter xylosoxidans misidentification in the literature raise the possibility that the “Pseudomonas fluorescens” contaminant was misidentified and that the contaminated phacoemulsifier served as the reservoir for the Achromobacter xylsoxidans endophthalmitis outbreak. The frequent confusion between Achormobacter xylosoxidans and Pseudomonas spp. has significant clinical import. Clinical isolates of Achromobacter xylosoxidans are typically resistant to aminoglycosides, fluoroquinolones, and cephalosporins, which are mainstays of empiric antipseudomonal therapy.9 Misidentification, therefore, leads to inappropriate antimicrobial therapy and a delay in clinical resolution of infection.
Available data from case reports and small case series suggest that surgical management of chronic Achromobacter xylosoxidans endophthalmitis, including IOL and capsular bag removal, is critical to achieve resolution of the infection as a result of biofilm formation.3,4,12 This is consistent with management recommendations for chronic postoperative endophthalmitis caused by other organisms.1 In this case, the corneal graft was removed in addition to the IOL and capsule complex. Due the antimicrobial properties of silicone oil,19 silicone oil was left in the vitreous cavity.
Recent evidence suggests that A. xylosoxidans infections may be on the rise.20,21 This unique case demonstrates the importance of developing better molecular diagnostics to rapidly distinguish between Pseudomonas species and Achromobacter xylosoxidans as well as the need for surgical intervention with removal of donor tissues and implanted prosthetics to adequately treat chronic endophthalmitis.
Abbreviations
PKP, penetrating keratoplasty; SO, silicone oil; IOL, intraocular lens; IOP, intraocular pressure.
Ethics Approval and Consent to Participate
The need for ethics approval for this case report was waived. The patient provided written consent allowing the use of clinical images and information for the purposes of publication.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors declare there is no conflict of interest, including financial, in this work.
References
1. Shirodkar AR, Pathengay A, Flynn HW
2. Reddy AK, Garg P, Shah V, Gopinathan U. Clinical, microbiological profile and treatment outcome of ocular infections caused by Achromobacter xylosoxidans. BMJ Case Rep. 2018;11(1).
3. Villegas VM, Emanuelli A, Flynn HW
4. Park JH, Lee EK, Lee SY, Kim DY, Kim JY. Recurrent endophthalmitis caused by achromobacter xylosoxidans: importance of aggressive surgical removal of capsular bag. Korean J Ophthalmol. 2018;32(2):160–162. doi:10.3341/kjo.2017.0143
5. Al-Mezaine HS, Al-Assiri A, Al-Rajhi AA. Incidence, clinical features, causative organisms, and visual outcomes of delayed-onset pseudophakic endophthalmitis. Eur J Ophthalmol. 2009;19(5):804–811. doi:10.1177/112067210901900519
6. Holmes B, Snell JJS, Lapage SP. Strains of Achromobacter xylosoxidans from clinical material. J Clin Pathol. 1977;30(7):595–601. doi:10.1136/jcp.30.7.595
7. Wiley L, Bridge DR, Wiley LA, Odom JV, Elliott T, Olson JC. Bacterial biofilm diversity in contact lens-related disease: emerging role of Achromobacter, Stenotrophomonas, and Delftia. Invest Ophthalmol Vis Sci. 2012;53(7):3896–3905. doi:10.1167/iovs.11-8762
8. Alvarez-Ortega C, Olivares J, Martinez JL. RND multidrug efflux pumps: what are they good for? Front Microbiol. 2013;4:7. doi:10.3389/fmicb.2013.00007
9. Spierer O, Miller D, O’Brien TP. Comparative activity of antimicrobials against Pseudomonas aeruginosa, Achromobacter xylosoxidans and Stenotrophomonas maltophilia keratitis isolates. Br J Ophthalmol. 2018;102(5):708–712. doi:10.1136/bjophthalmol-2017-311751
10. Spierer O, Monsalve PF, O’Brien TP, Alfonso EC, Gologorsky D, Miller D. Clinical features, antibiotic susceptibility profiles, and outcomes of infectious keratitis caused by Achromobacter xylosoxidans. Cornea. 2016;35(5):626–630. doi:10.1097/ICO.0000000000000798
11. Hogardt M, Ulrich J, Riehn-Kopp H, Tummler B. EuroCareCF quality assessment of diagnostic microbiology of cystic fibrosis isolates. J Clin Microbiol. 2009;47(11):3435–3438. doi:10.1128/JCM.01182-09
12. Swart J, Voker-Dieben HJ, Reichert-Thoen JWM. Alcaligenes xylosoxidans endophthalmitis 8 months after cataract extraction. Am J Ophthalmol. 1999;127(3):345–346. doi:10.1016/S0002-9394(98)00339-0
13. Amoureux L, Bador J, Fardeheb S, et al. Detection of Achromobacter xylosoxidans in hospital, domestic, and outdoor environmental samples and comparison with human clinical isolates. Appl Environ Microbiol. 2013;79(23):7142–7149. doi:10.1128/AEM.02293-13
14. Jha P, Kumar A. Characterization of novel plant growth promoting endophytic bacterium Achromobacter xylosoxidans from wheat plant. Microb Ecol. 2009;58(1):179–188. doi:10.1007/s00248-009-9485-0
15. Spear JB, Fuhrer J, Kirby BD. Achromobacter xylosoxidans (Alcaligenes xylosoxidans subsp. xylosoxidans) bacteremia associated with a well-water source: case report and review of the literature. J Clin Microbiol. 1988;26(3):598–599. doi:10.1128/JCM.26.3.598-599.1988
16. Lee B, Cai CX, Srikumaran D, Woreta FA. Severe Achromobacter xylosoxidans keratitis with deep corneal involvement. Am J Ophthalmol Case Rep. 2018;11:128–130. doi:10.1016/j.ajoc.2018.06.006
17. Zbinden A, Bottger EC, Bosshard PP, Zbinden R. Evaluation of the colorimetric VITEK 2 card for identification of gram-negative nonfermentative rods: comparison to 16S rRNA gene sequencing. J Clin Microbiol. 2007;45(7):2270–2273. doi:10.1128/JCM.02604-06
18. Robert PY, Chainier D, Garnier F, et al. Alcaligenes xylosoxidans endophthalmitis following phacoemulsification and intraocular lens implantation. Ophthalmic Surg Lasers Imaging. 2008;39(6):500–504. doi:10.3928/15428877-20081101-15
19. Chrapek O, Vecerova R, Koukalova D, et al. The in vitro antimicrobial activity of silicone oils used in ophthalmic surgery. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2012;156(1):7–13. doi:10.5507/bp.2011.060
20. De Baets F, Schelstraete P, Van Daele S, Haerynck F, Vaneechoutte M. Achromobacter xylosoxidans in cystic fibrosis: prevalence and clinical relevance. J Cyst Fibros. 2007;6(1):75–78. doi:10.1016/j.jcf.2006.05.011
21. Davies JC, Rubin BK. Emerging and unusual gram-negative infections in cystic fibrosis. Semin Respir Crit Care Med. 2007;28(3):312–321. doi:10.1055/s-2007-981652
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.