Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 17
Chronic Obstructive Pulmonary Disease in People with HIV: an Evidence-Based Review
Authors Read AT ![]() , Akodu J, Barber TJ, Brown JP, Burns FM, Hurst JR
, Akodu J, Barber TJ, Brown JP, Burns FM, Hurst JR ![]() , Miller RF
, Miller RF ![]() , Lipman MCI
, Lipman MCI
Received 11 March 2025
Accepted for publication 1 June 2025
Published 12 June 2025 Volume 2025:17 Pages 153—174
DOI https://doi.org/10.2147/HIV.S496211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Andrew T Read,1 Jane Akodu,2 Tristan J Barber,2,3 James P Brown,1 Fiona M Burns,2,3 John R Hurst,1,4 Robert F Miller,2,3 Marc CI Lipman1,2,4
1Respiratory Medicine, Royal Free London NHS Foundation Trust, London, UK; 2Ian Charleson Day Centre, Royal Free London NHS Foundation Trust, London, UK; 3Institute for Global Health, University College London, London, UK; 4UCL Respiratory, University College London, London, UK
Correspondence: Andrew T Read, Royal Free Hospital, Pond Street, London, NW3 2QG, UK, Email [email protected]
Abstract: HIV co-infection is a risk factor for the development of COPD. HIV enhances the deleterious effects of exposures such as tobacco smoking, as well as interacting with other drivers of COPD such as pulmonary tuberculosis, air pollution and biomass fuel burning. Recent work demonstrates that HIV also contributes independently to COPD pathogenesis by promoting oxidative stress, chronic inflammation, abnormal innate and adaptive immune responses, microbial dysbiosis, and epigenetic alterations within the lung. Consequently, people with HIV develop COPD younger, more often, and with faster rates of lung function decline compared to seronegative individuals. They may also have distinct patterns of lung function abnormalities compared to other etiotypes of COPD. Understanding the natural and pathogenetic history of HIV-associated COPD is important as its assessment, prevention and treatment are currently extrapolated from the general population. Whilst smoking cessation remains vital, further understanding may help guide unique management strategies for HIV-associated COPD. In this review, we explore its epidemiology and pathophysiology and discuss prevention and treatment approaches in this increasingly common disease.
Keywords: smoking, emphysema, lung function, airflow obstruction, air pollution, antiretroviral therapy
Introduction
Effective antiretroviral therapy (ART) has moved the focus of HIV care away from acute, opportunistic infections, towards chronic, age-associated comorbidities. Of these, people with HIV appear particularly susceptible to the development of Chronic Obstructive Pulmonary Disease (COPD).1–5
COPD is defined as a “heterogeneous lung condition characterised by chronic respiratory symptoms due to abnormalities of the airway and/or alveoli that cause persistent, often progressive, airflow obstruction”.6 COPD accounted for 3.3 million deaths globally in 20197 and is one of the top three causes of death worldwide.8 The global prevalence of COPD is increasing, driven by a complex interaction of different risk factors which, in general, represent systemic disadvantage across the life-course.7 Traditionally, at least in high-income settings, tobacco smoking is regarded as the most important risk factor and is still the most prevalent.7 However, in 2023 the Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy proposed a new taxonomy for COPD based on the contribution of multiple factors driving disease pathogenesis.9 The development of these “etiotypes” (that is, the primary cause of the resulting COPD) importantly emphasises the heterogeneity of COPD, and highlights the influence of other risk exposures on the lung, such as infections (Table 1).
 |
Table 1 Proposed Taxonomy (Etiotypes) of COPD |
More recently, HIV co-infection has been recognised as a novel risk factor for COPD. People with HIV develop COPD younger, more often, and with faster rates of lung function decline than seronegative individuals.3,5,10–12 HIV-associated COPD may be associated with distinct lung function abnormalities, compared to other “etiotypes” of COPD,13 and with significant gas exchange impairment.14 Even in the setting of suppressive ART, HIV persists within the lung.15 By promoting immune senescence and impairing epithelial integrity, HIV augments the effects of other drivers such as tobacco smoke to promote oxidative stress and low-grade inflammation in the alveolar compartment.16
Understanding the relationship between HIV and the other exposures that contribute to COPD pathogenesis is key to the development of specific strategies to mitigate these risks. This review will summarise recent advancements in our understanding of the epidemiology of COPD and HIV co-occurrence in different settings. It will explore the interaction between HIV and different risk factors, how HIV infection contributes to COPD pathogenesis, the emerging paradigm of HIV-associated COPD as an independent “etiotype” of COPD, and the approaches that can be taken to impact this.
Methodology
Our goal was to review the epidemiology of COPD in people living with HIV in different settings, to discuss the interactions between HIV and other drivers of COPD, to highlight pathways by which HIV may influence the development and natural history of COPD and discuss interventions that clinicians may use now or in the future, to mitigate the effects of HIV on the development of COPD. The broad nature of the review precluded the use of systematic review methods, and our findings are presented as a narrative review.
References for this review were identified through searches of PubMed articles published from January 1st, 2020, to Febuary 28th, 2025, containing the terms “HIV and COPD” and “HIV, COPD and smoking” yielding 280 results. Articles were screened by title and abstract and, if felt relevant to the above broad themes, read in more detail before being included. Studies were excluded if felt not relevant to the research themes above. Other publications were subsequently identified through cited reference searching and papers known to authors.
The Epidemiology of the Co-Occurrence of HIV and COPD in Different Settings
For people with HIV, COPD is one of the most common co-morbidities.1,17 The prevalence is higher than in the general population, though estimates vary widely amongst different cohorts.1,3,12 A recent meta-analysis estimated the global prevalence of COPD in people with HIV as 10.5% (95% CI: 6.2–15.7%),3 with highest prevalence in northern Europe and populations with higher incomes – although this likely reflects significant under-diagnosis of COPD in many global south settings.18
Depending on geographical location, cohort, and study design, prevalence estimates of HIV-associated COPD range from 3.4% to over 40%.12 This may reflect the variation in methods used to establish COPD diagnoses: self-reporting, International Classification of Disease-9 (ICD-9) coding, computed tomography (CT)-proven emphysema and spirometry have all been used in different studies.12 Generally, self-reporting of symptoms and radiological methods find higher rates of obstructive lung disease than spirometry,12 which is obligatory for the diagnosis of COPD.6
Most prevalence studies have been conducted in high-income countries (HICs),3 where tobacco smoking is the predominant risk factor for the development of COPD. Here, longitudinal analysis of large cohorts of people with HIV has helped estimate COPD incidence and prevalence. The biggest of these to date was the Veteran Ageing Cohort Study (VACS), where health records of over 33,000 military veterans with HIV were compared to demographically matched seronegative controls.1 ICD-9 codes were extracted from health records to analyse the co-occurrence of HIV with COPD. Veterans with HIV were significantly more likely to have incident diagnoses of COPD than those without HIV. HIV infection was associated with a greater incident risk of COPD in veterans under the age of 50 (Incident Risk Ratio [IRR] 1.17; 95% CI: 1.11–1.24), than those over the age of 50 (IRR 1.08 95% CI: 1.01–1.15), with the prevalence of COPD gradually increasing with age amongst both veterans with and without HIV. These effects were independent of smoking status.
It is imperative to understand how trends in the prevalence and incidence of obstructive lung disease in people with HIV develop over time. In a recent study by Rowell Consola et al, administrative health records from three hospitals in greater New York were retrospectively analysed for data on inpatient admissions over a 10-year period. Amongst >19,000 people with HIV, chronic lung diseases were the most prevalent recorded co-morbidity (25.3%), significantly higher than in the HIV negative population (14.0%; Prevalence Ratio [PR] 1.8; 95% CI: 1.8–1.8).4 Between 2006 and 2016, the prevalence of chronic lung diseases in people with HIV increased from just over 20% to nearly 35%. The study did not delineate between different forms of chronic lung diseases but suggests the burden of non-communicable lung disease is rising for people with HIV.
The development of COPD in people with HIV is a heterogeneous process and will depend on the interaction of different risk exposures and different HIV-related factors in different settings. Most people with HIV reside in African countries,19 where rates of tobacco use are rising,20 but where tuberculosis (TB) and biomass fuel burning also markedly contribute to COPD development.21 Across the African continent, prevalence estimates of HIV-associated COPD vary, for example, from 3.7–10.4% in Uganda22 to 15.4%-22.2% in Nigeria.23 Generally, studies report HIV-associated COPD prevalence at a lower frequency in LMICs than HICs,12 though this may reflect reduced access to CT imaging or spirometry. Interestingly, a recent meta-analysis found the odds of developing obstructive lung disease for people with HIV were higher in Africans (Odds Ratio [OR]: 1.56, 13 studies), than Americans (OR: 0.93, 15 studies) or Europeans (OR 1.36; p<0.01, 10 studies), though studies in Africa lacked gas exchange and CT scan data, and there was significant inconsistency between study design.5
Most reports have assessed COPD in men with HIV, though recent work has explored the impact of biological sex. In the general population, being female has been associated with the development of more severe, early onset COPD,24 and females may be more susceptible than men to harmful effects of smoking.25 Analysis of the Women’s Interagency HIV study found that women with HIV have lower baseline forced expiratory volume in one second (FEV1) and diffusing capacity for carbon monoxide (DLCO) than seronegative women.26 However, subsequent studies have failed to demonstrate an association between airflow obstruction and HIV status in women.27 Interestingly, a US study suggests women with HIV may have lower baseline DLCO and slower rates of decline of FEV1 than men with HIV,13 though this may be a reflection of the equations used to calculate lung function values in people of different sex and ethnicities.
Differences between sexes are also reported in studies from African countries with high HIV prevalence, where the leading risk factor for the development of obstructive lung disease in women is exposure to household air pollution.21 In a cohort of non-smoking women with HIV in Uganda, faster rates of FEV1 decline were noted compared to male counterparts and individuals without HIV.28 These differences may be due to cultural behaviours that result in different exposures to indoor cooking fumes: in Ugandan women with HIV but not men, higher exposure to carbon monoxide (CO) was associated with increased odds of reporting respiratory symptoms.29 However, this may not explain the entire association. In a cohort of Ugandan adults with HIV who had recently completed treatment for pneumonia, women with HIV had 3.44 increased odds of obstructive lung disease on spirometry than men (95% CI: 1.1–12.0; p=0.04), a result that persisted when adjusted for exposure to TB and biomass fuel burning.30 Whether sex-based differences in immune responses help to explain these differential patterns of lung function abnormalities in women with HIV is under investigation.
Risk Factors for COPD in People with HIV
Smoking
Globally, smoking is the most prevalent risk factor for COPD.21 In the US, up to 40% of people with HIV smoke compared to 21% of the general population.31 In China, studies suggest that over 50% of people with HIV are cigarette smokers,32 increasing to 65% in men with HIV who have sex with men.33 In LMICs, tobacco consumption is less prevalent but is still statistically higher than in people without HIV.19 Cultural practices contribute to differences between sexes: in an analysis of tobacco use in people with HIV in 28 LMICs, 24.4% of men with HIV were active tobacco smokers, compared to just 1.3% of women with HIV.34 In a recent prospective cohort study of over 500,000 adults in China, 74.3% of men had ever “smoked regularly” compared to just 3.2% of women.35
Despite declining smoking rates in people with HIV in the US (from 37.6% to 33.6% between 2009 and 2014), rates remain almost twice as high when compared to seronegative individuals, and people with HIV are less likely to quit compared to the general population.36 In China, rates of tobacco use remain high,35 and in many African countries, prevalence of tobacco use is rising.19
Tuberculosis
Previous pulmonary TB is an independent risk factor for the development of COPD.37 This is particularly significant considering an estimated 10 million people develop TB annually, and in 2020, there were over 150 million people who had survived TB.38 A recent meta-analysis including 23 studies37 found that TB increases the odds of developing fixed-airflow obstruction, meeting the spirometry criteria for COPD (by 2.59 CI: 2.12–3.15; P<0.001).38 The risk is also higher for people with HIV on ART. In a Ugandan population of people with well-controlled HIV, pulmonary tuberculosis was the strongest predictor of COPD risk and reduced lung function.39 This association was also seen in a study of urban centres in Uganda, where the prevalence of COPD in people with HIV was associated with previous tuberculosis and a BMI of <21/Kg/m2.40
Biomass Fuel Burning
Approximately 3 billion people around the world cook and heat their homes by burning solid fuels in open fires and stoves.41 In a recent report from the Global Burden of Disease collaborators, household air pollution from the burning of solid fuels was the primary risk factor responsible for disability adjusted life years from chronic respiratory diseases in southern Africa.21 A recent meta-analysis estimated exposure to burning of solid biomass fuels increased the risk of COPD by 2.65 (95% CI: 2.31–3.31) compared to the use of non-biomass fuels.42 COPD from household air pollution may differ from tobacco-related COPD in several ways, including greater airway involvement but less emphysema.42 Understanding how this relates to or differs from HIV remains under investigation.
Ambient Air Pollution
Air pollution is second only to tobacco smoke as globally the most attributed risk factor for deaths and disability adjusted life years lost from chronic respiratory disease.21 The development of COPD has been directly linked to exposure to air pollutants,43 with recent estimates suggesting as much as 50% of the total attributable risk of COPD may come from exposure to gaseous and particulate components of air pollution.44 There is no safe “threshold” for air pollution; the relationship between respiratory events and air pollution is supra-linear: there are more adverse effects per unit change in air pollution at lower concentrations, compared to higher concentrations.44 High levels of air pollution increase the risk of COPD exacerbations, hospitalisations and death.45 People with HIV may be particularly susceptible to the effects of air pollution: in a cohort study of >250 adults in rural Uganda, people with HIV were more likely to report chronic cough, dyspnoea or wheeze when exposed to unsafe levels of CO measured by 48-hour ambulatory CO monitoring, compared to adults without HIV.29 In people with HIV, elevated concentrations of ambient air pollutants are associated with suppressed antibody responses to Pneumocystis jirovecii surface glycoproteins in serum and bronchoalveolar lavage (BAL), though so far no correlation with adverse clinical outcomes has been demonstrated.46,47
HIV as an Independent Risk Factor for Lung Disease
In meta-analyses, after adjusting for cigarette smoking, the prevalence of COPD is significantly higher in people with HIV than in those without HIV,3 suggesting an independent effect of HIV on lung health. In people with HIV, CD4+ T-cell counts <200 cells/µL are associated with reduced pulmonary diffusing capacity.48 Low nadir CD4+ cell count is independently and negatively correlated with the development of COPD,49 and with gas exchange impairment in people with HIV.50 In the AIDS linked to the Intravenous Experience (ALIVE) cohort in the US, (a cohort of people who inject drugs) people with an HIV load of >75,000 copies/mL and CD4+ T cell counts <100 cells/mm3 had faster FEV1 and FVC declines compared to individuals without HIV.51
The impact of HIV control on lung function decline is not completely understood. In the AGEhIV study, a longitudinal cohort study which followed over 900 people in Amsterdam with virally suppressed HIV over almost 8 years, treated HIV infection was associated with greater adjusted yearly declines in FEV1 and FVC over time compared to those without HIV: even in the setting of viral control, lung function decline is faster than in the general population.52 Although rates of FEV1 and FVC decline between people with HIV and the general population were even faster in smokers, these changes persisted after controlling for smoking and other risk behaviours. Statistically higher C-reactive protein (CRP) concentrations during follow-up were associated with accelerated declines in FEV1 and FVC among those with HIV, but not in participants without HIV, suggesting low-grade inflammation could be contributing to this.
Moreover, in the VACS cohort, ART use was not associated with a lower incidence of COPD after adjusting for smoking status.1 To specifically examine the impact of ART on lung function decline, the Strategic Timing of Antiretroviral Treatment (START) trial enrolled ART-naïve adults with HIV who had CD4+ T-cell counts >500 cells/mm3 and a median time since HIV diagnosis of 1.2 years. Participants were randomised to begin ART immediately or deferred until CD4+ T-cell counts were <350 cells/mm3 or AIDS developed. After nearly 4 years of follow-up, there was no difference between immediate or deferred ART initiation on rates of post-bronchodilator FEV1 decline or incident COPD risk.53 This suggests that at least for those early in their disease course with CD4+ cell counts >500 cells/mm3, use of ART does not affect FEV1 decline. However, this study did not assess other lung function measures (eg DLCO) or radiographic markers of COPD, and the effects of HIV control on the development of COPD may become apparent after a longer follow-up period.
HIV Acts Synergistically with Other Risk Exposures
As well as causing an independent effect on lung health, HIV interacts with and augments other risk exposures to contribute to COPD pathogenesis (Figure 1). Perhaps, the most important of these is the synergistic effect of HIV and tobacco smoke on the lung. Smokers living with HIV are more susceptible to the development of emphysema than seronegative smokers.54 A recent prospective matched cohort study of >1000 people in Denmark and the US with virally suppressed HIV found an 8.5mL/year faster decline in FEV1 for people with HIV compared to those without. This effect was augmented by smoking: smokers with HIV experienced 16.8mL/year faster decline in FEV1 than smokers without HIV.10
 |
Figure 1 Drivers and implications of HIV-associated COPD. HIV interacts directly and indirectly with different factors to contribute to COPD pathogenesis with negative implications for patients. |
Tobacco smoking appears to impair the effectiveness of ART: smoking is associated with a greater risk of virological rebound in women with HIV on ART and a higher risk of developing AIDS when adjusted for other confounders.55 Moreover, in a cohort of ART-naïve men living with HIV in South Africa, current smokers had 3 times higher odds (95% CI: 1.3–7.9, P = 0.01) for developing pulmonary tuberculosis than non-smokers,56 suggesting smoking and HIV combine to enhance susceptibility to other infections. Smoking is also a risk factor for the development of bacterial pneumonia, an effect that is reduced when people stop smoking.57 Given the synergistic effect of HIV and tobacco smoke on the lungs, understanding how to address tobacco dependence in people with HIV is critical.
How Does HIV Co-Infection Influence the Natural History of COPD?
The recent proposal of a new taxonomy for COPD, with “etiotypes” of COPD grouped by underlying causative factors reflects the observation that some disease entities show distinct clinical features.9 Although there are many cross-sectional studies reporting the prevalence of COPD among people with HIV,40,41,48,58,59 our understanding of the natural history of HIV-associated COPD is more limited. HIV infection accelerates lung function decline but may also contribute to impaired gas exchange before, or independently of airflow obstruction developing (Figure 1).
Effects on Gas Exchange
The diffusing capacity of the lungs for carbon monoxide is a measure of the ability of gas to transfer from the alveoli into red blood cells. People with HIV have a higher risk of gas exchange impairment,5 with reduced DLCO measurements among the most prevalent findings on lung function testing in people with HIV.14,26,48 Low DLCO is associated with low nadir CD4+ T cell counts and detectable viraemia.50,60 Importantly, both impairments of DLCO and FEV1 have been identified as independent risk factors for mortality in people with HIV.13,61
Discerning which factors contribute to lung function and gas exchange impairment, and the relationship between these measures in HIV-associated COPD is complex. Analysis of the Pittsburgh HIV Lung Cohort found that older age, male sex and GOLD stage 1 COPD at baseline were all associated with faster rates of decline of post-bronchodilator FEV1 & FVC.62 Interestingly, viral load, CD4 T+ cell levels and ART use were not associated with rates of decline. In a separate analysis of the same cohort, measurements of DLCO, FEV1 and FVC were recorded in conjunction with symptoms and serum immune markers. Specific patterns of lung function decline were associated with specific symptoms. Elevated serum CRP & endothelin-1 (ET-1) levels were associated with faster rates of decline in FEV1 and the FEV1/FVC ratio.13 Detectable viraemia, however, was associated with impaired DLCO at baseline. This might suggest that distinct mechanistic pathways lead to airflow obstruction or gas exchange impairment in people with HIV.
In one of the largest reported studies recording lung function in men with HIV (The Multicenter AIDS Cohort Study), HIV status was not correlated with impaired FEV1.50 However, men living with HIV had a 1.6x increased risk of DLCO <80% predicted (95% CI: 1.18–1.28, p=0.002), and a 3.0x increased risk of DLCO <60% predicted (95% CI: 1.36–6.47, p=0.006) compared to men without HIV. Lower DLCO was associated with lower nadir CD4+ counts. Isolated impairments in DLCO in the presence of normal spirometry (iso↓DLCO) have also been reported in cohorts of women living with HIV,26,27 where they were again associated with lower nadir CD4 counts. Iso↓DLCO is associated with worse ratings on health quality of life indexes,63 and worse respiratory symptom scores, an association which strengthens as gas exchange worsens.14
If specific immunological mechanisms drive iso↓DLCO, they are not well understood. Lower DLCO levels are associated with increased CD25+/CD4+ and CD25+/CD8+ T cells, as well as higher IL-6 and CRP levels in people with HIV that have high rates of concurrent tobacco use.64 This suggests that adaptive immune activation may contribute to gas exchange impairment, though the relative contribution of regulatory CD4+ T cells was not assessed. Perturbations in innate immunity may also contribute. In longitudinal analyses, reduced DLCO in people with HIV was associated with elevated plasma markers of monocyte/macrophage activation such as Interleukin-2 (IL-2) and soluble CD163 (sCD163) as well as markers of endothelial dysfunction such as ET-1.65
In the Inflammation, Ageing, Microbes and Obstructive Lung Disease (I AM OLD) Study, done in two US cities, elevated plasma levels of the pneumoproteins pulmonary and activation-regulated chemokine (PARC)/CCL-18 and Clara cell secretory protein (CC-16) were more strongly associated with low DLCO than low FEV1 in people with HIV.66 Further work by the same group characterised biomarkers specifically associated with an iso↓DLCO phenotype in people with HIV, including soluble CD14 (sCD14), sCD163, interferon gamma-induced protein 10 (IP10), soluble tumour necrosis factor (TNF) receptors sTNFR-I, and sTNFR-II.67 In addition, two studies demonstrate that people with HIV with low DLCO preferentially express different genes compared to people without HIV or those with normal gas exchange. Impairments in DLCO are associated with activation of processes involved in inflammation, immunity, apoptosis68 and interferon signalling.69 Understanding the mechanisms by which HIV causes distinct abnormalities in lung function and gas exchange is imperative to understanding HIV-associated COPD as its own etiotype. However, DLCO impairment is non-specific and can be the result of infections;70 abnormalities in lung structure such as emphysema or fibrosis; pulmonary vascular disease such as pulmonary hypertension or congestive cardiac failure.71 Further studies which control for these co-morbidities are required to delineate the significance of impaired gas exchange in people with HIV.
Emphysema
Emphysema on chest imaging is common in people with HIV, with a recent systematic review estimating a weighted average prevalence of emphysema in those with HIV of 23% (95% CI: 16–30%).72 High rates of tobacco and marijuana use are associated with the development of emphysema in people with HIV,73 but HIV infection is a risk factor for the development of emphysema independent of smoking.54,74 In a single centre study from Italy, emphysema was reported in 18% of people with HIV that had never smoked.75 Emphysema in people with HIV is often more diffuse on chest imaging than in those without and has been independently associated with CD4+ cell counts <200/mm3, high sCD14 levels,74 high TNFα and IL-1B levels,76 and low CD4+/CD8+ T cell ratios.77 For people with HIV, radiological emphysema is associated with worse symptoms such as cough and mucus production and shorter six-minute walking distances, compared to those without HIV.77 An emphysema burden of >10% on CT also carries a 2.4x increased risk of mortality (95% CI: 1.1–5.5), compared to people with </=10% emphysema, an effect which is independent of smoking pack-years.61
Identifying people with HIV at greatest risk for progressive emphysema is therefore important, as it offers the possibility of intervening early, ie prior to significant morbidity and mortality occurring. Low DLCO and a combination of CT-proven centrilobular and paraseptal emphysema have been identified as factors associated with radiological progression of emphysema in people with HIV.78 Interestingly, a recent prospective cohort study from Atlanta of more than 160 people with HIV followed up over a 6-year period, found that traditional metrics of airflow limitation (FEV/FVC ratio <0.7) were not the most effective measures with which to predict the presence of radiological emphysema.79 In this cohort, these were a FEV1/FVC cut-off of 0.78 and a residual lung volume of 116% predicted.
Further work is required to determine the optimal thresholds for identifying patients with HIV associated emphysema. Although emphysema and COPD often coexist, one does not necessarily imply the other; airflow limitation on spirometry is required for a diagnosis of COPD. While high rates of emphysema may in part explain the high frequency of gas exchange impairment in people with HIV, in the multi-center study of HIV in the Etiology of Lung disease (SHIELD) the association between HIV and low DLCO were independent of emphysema severity, suggesting that this relationship is complex.80
Symptom Burden, Morbidity & Mortality
People with HIV may report more respiratory problems than their seronegative counterparts (Figure 1). Even in individuals without overt lung disease, HIV infection is associated with reduced exercise tolerance and worse respiratory symptoms reported by questionnaire.81 Independent of the effect of antiretroviral therapy, people with HIV are more likely to have respiratory symptoms,82 and these are likely to be more severe and result in healthcare seeking behaviour.83
People with HIV-associated COPD may be particularly affected. In the ALIVE cohort, HIV was an independent risk factor for moderate breathlessness on the MRC scale, and when HIV and COPD were present together, this association was worse than with either disease alone.58 In other cohorts, more chronic cough and decreased exercise tolerance are present in people with HIV compared to negative individuals.84 Moreover, people with HIV who have a diagnosis of COPD are more likely to report depressive symptoms and have a lower quality of life than those without COPD.85
HIV has also been identified as an independent risk factor for exacerbations of COPD. In the ALIVE cohort, HIV was associated with 2.47 increased odds of COPD exacerbation (95% CI: 1.22-5.00).86 How this relates to CD4+ cell count and immune function is not clear. The ALIVE study found there was an increased risk of COPD exacerbation for people with HIV with undetectable viral loads, and CD4+ cell counts >350 cells/mm3, but this was not seen with CD4+ counts <350 cells/mm3. By contrast, in the VACS study, lower baseline CD4+ cells counts, higher HIV RNA levels and lack of ART were all associated with increased risk of acute exacerbation.87 While these observations may in part be explained by differences in how COPD exacerbations are reported or differences in health seeking behaviours between the two cohorts, the relationship between viral control and exacerbation risk requires further clarification.
Perhaps most importantly, the presence of COPD increases risk of death for people with HIV: airflow obstruction, gas exchange impairment and emphysema are all independently associated with increased risk of all-cause mortality.61,88 The negative implications of HIV-associated COPD are outlined in Figure 1.
How Does HIV Influence the Development of COPD?
In individuals without HIV, COPD is typically the result of a genetic susceptibility to a modified inflammatory response to chronic irritants such as cigarette smoke, though the mechanisms that cause this are not fully understood.6 HIV infection contributes to COPD pathogenesis by further modifying the alveolar immune response to noxious stimuli.
HIV Persistence within the Lung
HIV can directly infect a range of cell types within the lung. These include bronchial epithelial cells89 and, when blood CD4+ T cell levels are low, alveolar macrophages.90 Alveolar macrophages are the most plentiful cells within bronchoalveolar (BAL) fluid, and the primary innate cells within the lung. In the presence of CD4+ T cells in vitro, HIV infection of alveolar macrophages isolated from BAL fluid is enhanced, and HIV may be transmitted from infected CD4+ T cells to alveolar macrophages via direct contact.91
HIV infection alters the immune response of alveolar macrophages, impairing phagocytic activity92,93 and skewing macrophages towards a pro-inflammatory, protease producing phenotype. In vitro, monocyte-derived macrophages infected with HIV demonstrate activation of pathways associated with the pathogenesis of COPD such as activation of the NLRP3 inflammasome.94 HIV therefore appears to promote lung inflammation by influencing the ability of alveolar macrophages to respond to external stimuli.
As described in other anatomical sites within the body,95 HIV may persist within cellular reservoirs in the lung. As long-lived cells, tissue macrophages represent a compelling cellular reservoir for HIV. Initial studies demonstrating in vivo infection of alveolar macrophages from BAL fluid samples were complicated by the fact that donors were not treated with ART and may subsequently have had co-existent inflammatory processes occurring within their lungs.93 It is therefore difficult to understand if the infected macrophages isolated represent recruitment of short-lived inflammatory cells rather than chronic immune reservoirs within the lung. HIV nucleic acids have, however, been isolated from the BAL fluid alveolar macrophages of individuals on ART with undetectable plasma viral loads.92
Further evidence for a cellular reservoir within the lungs is provided by animal models. Cellular labelling experiments in rhesus macaques demonstrate infection and destruction of short-lived interstitial macrophages but reduced cell death of longer-lived HIV-infected alveolar macrophages.96 In murine models, HIV infection of tissue macrophages is rapidly suppressed by ART, but delayed viral rebound occurs in around one-third of animals, suggesting persistence of HIV infection within macrophages.97
In lung samples from people with HIV who died and were on ART, significant levels of viral DNA were regularly isolated at post-mortem suggesting viral persistence despite ART.98 It is unclear if this represents replication competent virus. Further studies suggest that bronchial epithelial cells,89 CD4−CD8− T cells,99 and bronchial pericytes100 may contribute to a cellular reservoir for HIV in the lung. The contribution of such reservoirs to the pathogenesis of COPD is likely indirect, though HIV persistence within the lung may contribute to chronic, low-grade inflammation within the alveolar space.
Altered Adaptive Immune Responses
The lung is continually exposed to inhaled pathogens, allergens and toxins. To counter these, a robust adaptive immune response requires a broad population of CD4+ and CD8+ T cells. HIV infection may reduce the effectiveness of the adaptive response by inducing immune senescence, and the recruitment of terminally differentiated exhausted cells into the alveolar compartment.
For example, chronic HIV infection results in the accumulation of CD8+ T cells exhibiting high levels of exhaustion markers, such as programmed cell death protein-1 (PD-1), and low proliferative capacity.101 In people with HIV not on antiretroviral therapy, there appears to be a profound influx of dysfunctional CD8+ T cells into the lung, with a resulting lymphocytic alveolitis.102 These cells again demonstrate decreased proliferation markers and higher expression of PD-1. People with HIV also appear to have low CD4+/CD8+ T cell ratios in peripheral blood even after CD4+ T cell population recovery following ART.103 High levels of terminally differentiated, activated CD8+ T cells may represent a marker of persistent immune dysfunction in the T cell compartment, even after viral suppression.
HIV infection may also induce senescence of CD4+ T cells. Cell sorting studies comparing peripheral blood and lung mucosal T cell populations in HIV positive and negative individuals with COPD demonstrated qualitative and quantitative lung mucosal CD4+ T cell depletion in people with HIV, which was not replicated in peripheral blood, or people without HIV.104 This was again associated with raised levels of exhaustion markers Fas-1 and PD-1. People on long-term ART also experience persistent depletion in the diversity of their T-cell receptor repertoire.105 Thus, the inflammation associated with chronic HIV infection may result in immune senescence of the adaptive response and deplete the diversity of the response to external stimuli.
Changes to the Airway Epithelium
HIV infection reduces the integrity of the airway epithelium, the main physical and immunological barrier protecting the lung from external insults. HIV can infect bronchial epithelial cells which express HIV co-receptors CD4, CCR5 and CXCR4.106 Following infection, HIV decreases expression of E-cadherin, an adhesion molecule produced by airway epithelial cells which is important for barrier function,107 thus increasing epithelial cellular permeability to harmful inhalants.
The cystic fibrosis transmembrane regulator protein (CTFR) is a key component of airway clearance, ciliogenesis and epithelial cell differentiation. In vitro, the HIV protein Tat impairs transcription of CFTR,106 and cigarette smoke acts synergistically with Tat to impair both CFTR transcription and mucociliary clearance.108 In the macaque model, Simian adapted HIV (SHIV) infection results in goblet cell metaplasia and loss of tight junction proteins in the airway epithelium.109 SHIV infection generates significant numbers of HIV-gp120+ epithelial cells in small airways, an effect doubled when macaques are exposed to cigarette smoke regularly.
HIV also promotes cellular senescence in airway epithelial cells. Small airway epithelial cells taken from people with HIV have shorter telomere lengths compared with HIV-negative controls even after accounting for cigarette smoke exposure and age.110 These changes are also seen in basal progenitor cells, the multipotent progenitor cells that regenerate the airway epithelium following damage. HIV infection results in the expression of higher levels of matrix metalloproteinase-9 (MMP-9),111 decreased differentiation capacity and shortened telomere length in these cells.112
HIV and Smoking Act Synergistically within the Lung
HIV infection may render cells more susceptible to the harmful effects of cigarette smoke by increasing the expression of pro-inflammatory mediators that cause lung damage. In alveolar macrophages taken from BAL fluid of HIV-1 transgenic rats, exposure to cigarette smoke increases expression of MMP-9, and this is increased further when cells are exposed to the HIV protein Tat in vitro.113 Alveolar macrophages taken from BAL fluid of people with HIV more frequently exhibit pro-inflammatory markers of differentiation (CD163− CCR7+), compared to seronegative controls. In smokers, these macrophages also have increased expression of the HIV co-receptor CXCR4, and Toll-like receptor-4 (TLR-4).114
By inducing expression of HIV co-receptors on alveolar macrophages, smoking may potentiate HIV infection within cells of the lung. Cigarette smoke enhances HIV entry into bronchial epithelial cells in vitro, via up-regulation of CCR5.108 Also, exposure of alveolar macrophages in vitro to the carcinogen benzo(a)pyrene, a component of cigarette smoke, enhances HIV-1 replication in these cells.115
Synergistic effects may also occur via modulation of miRNA pathways. The lactoperoxidase system (LPO) is an important part of the innate immune response, mitigating oxidative stress in the lung by reducing levels of hydrogen peroxidase (H2O2). Bronchial epithelial cells exposed to TGF-B1, which is upregulated in COPD and HIV infection, and cigarette smoke express decreased LPO levels via transcriptional silencing of miRNAs. Decreased LPO led to increased H2O2 expression, and a subsequent oxidative stress response.116 In vitro, Tat also impairs mucociliary clearance by modulating the miRNAome in the presence of cigarette smoke.117
Few studies have linked immunological changes with radiographic or spirometric outcomes. Corleis et al found increased numbers of CD8+ T cells in the airway mucosa of smokers with HIV, and these were inversely correlated with lung aeration measured by CT imaging, suggesting smoking may cause recruitment of CD8+ T cells which results in structural changes within the lung.118 In a retrospective study of 82 people from the Pittsburgh Lung HIV study cohort who were virally suppressed on ART, both current smoking and intensity of smoking were correlated with higher HIV DNA and cell-associated RNA levels in peripheral blood mononuclear cells (PBMCs). Whilst this may suggest that smoking promotes HIV persistence despite systemic viral suppression, there was no relationship between these markers of HIV persistence and impairments in FEV1% predicted, FVC % predicted, FEV1/FVC or DLCO % predicted.119
Dysbiosis in the Lung Microbiome
The effects of HIV on the gut microbiome are well-established,120 though its impact on the lung microbiome is less so. Compared to other mucosal surfaces, the lungs must maintain a relatively lower bacterial burden to effectively facilitate gas exchange at the alveoli.121 HIV driven perturbations in lung microbial populations, resulting in an overabundance of pathogenic species, may contribute to COPD pathogenesis.
Pneumocystis jirovecii is disproportionately found in airways of people with HIV with COPD, regardless of CD4+ T cell count.122 A multicentre study identified bacterial gene sequences representing the gut pathogen Tropheryma whipplei more frequently in BAL fluid of some individuals with HIV compared to seronegative controls.123 However, this has also been demonstrated in BAL fluid taken from healthy smokers and non-smokers so may not be unique to the HIV population.124 Other studies conducted as part of the Lung HIV microbiome project failed to identify a significant difference in bacterial populations in BAL fluid between people with HIV on ART, and those without HIV, though changes have been demonstrated at the level of the oral mucosa.125
Microbial dysbiosis may be exaggerated in advanced HIV infection as immunosuppression limits the ability of the immune system to restrict colonisation of the respiratory tract. Twigg et al took BAL samples from 30 people with HIV with a baseline mean CD4+ T cell count of 262 cells/mm3.126 The relative abundance of Prevotella and Veillonella, species previously associated with lung inflammation, was higher in people with HIV than seronegative controls. These differences reduced but did not completely resolve after a year on ART. In a UK cohort study, there was no difference in the core airway microbiome depending on HIV status, but pathogenic respiratory taxa such as Staphylococcus, Pseudomonas and Klebsiella were significantly more frequent in sputum samples of people with HIV, and this was correlated to the duration of HIV infection, and the timing of ART introduction.127
Airway inflammation may result from translocation of oral bacteria into the lung. Alterations in the oral microbiome have been associated with increased airflow obstruction and lower DLCO in people with HIV but not negative controls.128 Detection of supraglottic taxa of bacteria in BAL fluid is correlated with detection of proinflammatory cytokines and deficits in lung function in people with HIV,129 linking micro-aspiration of bacteria from the oral cavity to COPD pathogenesis. However, multiple studies have also demonstrated enrichment of the lung microbiome by commensal gut bacteria.123,126–128 In the setting of advanced HIV infection, breakdown of the gut mucosal barrier may result in translocation of bacteria from the gut, resulting in alteration of the lung microbiome.
A recent study compared respiratory microbiota between virologically suppressed adults in Uganda and the United Kingdom, stratified by HIV and COPD status.130 Reduced bacterial diversity and significant enrichment of induced sputum samples with Campylobacter species was found in people with both HIV and COPD, compared to people with just one of these conditions. Comparisons between the two groups revealed significant differences in the sputum microbiome composition, irrespective of viral suppression, suggesting geographical differences may also play a role.
Oxidative Stress
HIV infection promotes oxidative stress within the alveoli by disturbing the normal oxidant/antioxidant balance.15,16 HIV indirectly inhibits synthesis of the compound glutathione, the main endogen antioxidant.131 Glutathione protects alveolar cells by reducing reactive oxygen species. Non-smokers with HIV on ART have significantly higher glutathione levels in BAL than those not taking antiretroviral therapy,132 suggesting ART may protect the lung from oxidative stress. Smoking in people with HIV is associated with lower glutathione levels than non-smokers,133 and smokers with HIV experience falling glutathione levels over time.134 Decreased glutathione means that lung defence against oxidative species is impaired. Data suggest that this is the case even for people with HIV taking ART.132,135 Compared to uninfected controls, alveolar macrophages isolated from people with HIV on ART have higher levels of H2O2, and the proteins Nox1, Nox2, Nox4 and TGF-β1, proteins that contribute to oxidative stress and immune dysfunction.136
Developments at the Epigenetic Level
DNA methylation regulates gene expression by recruiting or inhibiting proteins involved in transcription. Recent epigenome-wide association studies have investigated whether differential DNA methylation influences lung function variability in people with HIV. People with HIV in the START trial underwent annual spirometry testing over a median 5-year period. Airflow obstruction (FEV1/FVC <0.7) in these people was associated with almost 1400 differentially methylated positions in DNA isolated from peripheral blood samples. These methylation signatures were enriched for biological pathways associated with chronic viral infections. Individuals with airflow obstruction were globally hypomethylated compared to those without.137 Subsequent studies have also identified distinct DNA methylation profiles in bronchial epithelial cells in people with HIV with COPD and higher levels of epigenetic biomarkers associated with ageing.138 Epigenetic changes that result in ageing of the airway epithelium in people with HIV may contribute to the heightened risk of COPD in this population.
Even with HIV suppression, infection with HIV promotes low level chronic inflammation in the lung. Impairments in, and senescence of, innate and adaptive immune cells, oxidative stress, dysbiosis of the lung microbiome and disordered epithelial barrier integrity may all contribute to increased susceptibility to environmental exposures such as cigarette smoke, and subsequent COPD pathogenesis.
How Might We Influence the Development and Natural History of COPD?
Screening & Case Finding
Studies suggesting that lung function declines fastest in the incipient stages of COPD139 highlight the importance of early diagnosis and raise questions about optimal approaches for early COPD detection in HIV clinics. This is particularly complicated given the heterogeneity of COPD, where the presence of symptoms and objective lung function changes do not often correlate.140
Screening, the process of identifying asymptomatic participants who have an increased risk of developing a disease, for COPD in the general population is controversial. The US Preventative Services Task Force currently recommends against screening asymptomatic people for COPD on the basis that early detection does not affect disease course and has no treatment other than exposure reduction, which should proceed irrespective of COPD status.141 GOLD, however, argues that this should not apply to high-risk populations6 and advocates for case finding, ie performing spirometry in patients with respiratory symptoms or risk factors, in the general population.6 The European AIDS Clinical Society142 also advocates for case finding of COPD in people with HIV.
The best way to do this is not yet determined. Lambert et al employed a questionnaire-based screening tool in an outpatient HIV clinic to screen over 1500 people with HIV for COPD.143 Only 64% of participants successfully completed the questionnaire. Two hundred and four participants met criteria for spirometry, but it was performed in only 64, resulting in just 5 people with objective evidence of COPD.
In an urban HIV clinic in New York, Shirley et al screened all people aged >35 with same day peak flow measures and a respiratory symptom questionnaire.144 Those with either abnormal questionnaire responses or abnormal peak flow (<70% predicted), as well as one-third of people with normal screens were offered spirometry. Five of 89 (6%) who completed spirometry were diagnosed with COPD. In this study, abnormal peak flow was more sensitive (sensitivity of 80%) than either the questionnaire or a combination or both peak flow and questionnaire, in the diagnosis of COPD.
A single centre study in Italy combined a questionnaire approach with hand-held spirometry in over 1450 participants.145 Twenty percent (282) qualified for same day spirometry based on questionnaire scores, and of the 190 who completed it, 65 (34%) had impaired spirometry. They were referred for formal lung function testing, which was completed in only 33 people. Twenty-two (67%) had COPD. In each of these studies, large dropout rates, poor attendance at spirometry appointments, and/or the low specificity of tools for the detection of COPD highlight the difficulty of creating a screening tool for HIV-associated COPD in an outpatient setting.
Formal spirometry-based techniques may not be applicable for use in LMIC where access is often limited, or for the screening of large cohorts of people in outpatient settings. In LMICs, micro-spirometers may be useful and are generally more sensitive than questionnaire-based approaches.146 Novel methods that incorporate questionnaires combined with peak flow, such as the COPD Assessment in Primary care To identify Undiagnosed Respiratory disease and Exacerbation risk (CAPTURE) tool, are currently being evaluated, though not specifically in people with HIV.147 To date, this has demonstrated only limited sensitivity in the diagnosis of COPD,148 though this may improve in patients who require treatment because of increased risk of exacerbations or hospitalisation.149 Techniques that also incorporate clinically relevant exposures to particular risk factors have been tested in Uganda.150 Studies that validate the CAPTURE tool and other such techniques in HIV populations are required. Currently, no conclusive recommendations on screening and case-finding can be made.
The Timing & Type of Antiretroviral Therapy
Work identifying low nadir CD4+ T cell counts and high HIV RNA levels as risk factors for impaired lung function48,51 contributed to the hypothesis that early initiation of ART may reduce the rate of lung function decline in people with HIV. However, in the START trial, after a median of 3.9 years follow-up in a relatively young population (median age 36 years; IQR 30–44), there appeared to be no difference in rates of decline of airflow obstruction, or COPD incident risk, whether ART were started immediately or deferred.53
Conversely, data from early observational studies suggested that ART use may be associated with an increased risk of COPD.151,152 This led to the hypothesis that certain subtypes of ART could have a direct toxic effect on the lung. However, in the sub-group analysis of the START trial, different drug classes of antiretroviral therapy had no clear effect on declines in lung function, even though only small numbers of people were taking integrase inhibitors – which limits what we can conclude about this particular drug class.153
Key Considerations When Managing COPD in People with HIV
People with HIV have been historically excluded from large, randomised controlled trials of treatments for COPD. Management strategies for COPD in HIV populations are extrapolated from the general population. However, there are a few specific areas of note when considering treatment for COPD in people with HIV (Figure 2).
 |
Figure 2 Key considerations in the assessment and management of HIV-associated COPD. |
Initial COPD strategies including exposure reduction, vaccinations and pulmonary rehabilitation are important irrespective of HIV status. Recent guideline updates in chronic pharmacological COPD management promote the use of inhaled therapies with dual bronchodilators (LABA-LAMA) as the background therapy recommended for all but those with minimal symptoms and low exacerbation risk.6 Inhaled corticosteroids are also recommended for people with relatively higher blood eosinophilia (>/= 300 cells/μL) and/or more than two COPD exacerbations per year. This is particularly important in the context of HIV, where co-infection increases the risk of exacerbations. Long-term inhaled corticosteroid use in COPD is associated with modest but increased risk of fractures,154 bacterial pneumonia155 and tuberculosis,156 conditions for which HIV co-infection also confers a heightened risk.
Another consideration is the interaction between protease inhibitor-boosted ART regimens, such as those containing ritonavir or cobicistat, and inhaled steroid therapies. Ritonavir and cobicistat both inhibit the hepatic CYP3A4 isoenzyme, resulting in increased concentrations of corticosteroids. There are numerous reports of the development of hypercortisolism (Cushing’s syndrome) due to co-administration of ritonavir and inhaled fluorinated corticosteroids.157 Beclomethasone is considered to have the lowest adverse effect profile of inhaled steroids,158 and European HIV guidelines recommend against the co-administration of steroid inhalers with some boosted ART regimens.159 Key clinically relevant drug interactions between COPD medications and ART are outlined in Figure 3.
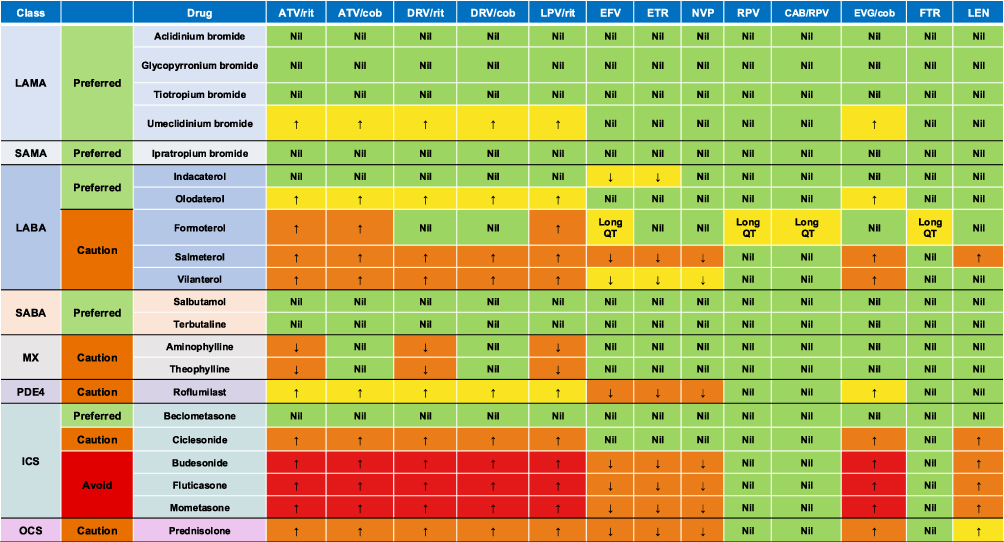 |
Figure 3 Clinically relevant drug interactions between COPD medications and selected antiretrovirals. For detailed drug interactions, dose adjustments, and alternative options, refer to the Liverpool HIV Drug Interactions Database: https://www.hiv-druginteractions.org.Other ARTs: There are no known clinically relevant drug interactions between any of the COPD medications listed in the table and the following antiretrovirals: ABC, FTC, 3TC, TAF, TDF, ZDV, DOR, MVC, BIC, Oral CAB, DTG & RAL. Abbreviations: LAMA, Long-acting muscarinic antagonists; LABA, Long-acting β agonists; SABA, Short-acting β agonists; MX, Methylxanthines; PDE4, Phosphodiesterase 4 inhibitors; ICS, Inhaled corticosteroids; OCS, Oral corticosteroids; ABC, Abacavir; ATV, Atazanavir; BIC, Bictegravir; CAB, Cabotegravir; Cob, Cobicistat; DOR, Doravirine; DRV, Darunavir; DTG, Dolutegravir; EFV, Efavirenz; ETR, Etravirine; EVG, Elvitegravir; FTC, Emtricitabine; 3TC, Lamivudine; FTR, Fostemsavir; LEN, Lenacapavir; LPV, Lopinavir; MVC, Maraviroc; NVP, Nevirapine; RAL, Raltegravir; Rit, Ritonavir; RPV, Rilpivirine; TAF, Tenofovir Alafenamide; TDF, Tenofovir Disoproxil; ZDV, Zidovudine. Notes: ↑: increased serum concentration of COPD medication; ↓: decreased serum concentration of COPD medication; Long QT: drug combination may prolong QT interval; Green: Preferred drug combination – No significant interactions; Yellow: Potential weak interaction – No additional monitoring and/or dose adjustment required; Orange: Likely interaction – Monitor carefully, consider alternatives or dose adjustment; Red: Significant interaction – Avoid drug combination. Use alternatives. |
Smoking Cessation
Smoking cessation is vital for people with HIV given their disproportionately high rates of tobacco use,31,36 and the fact smoking cessation reduces the risk of subsequent bacterial pneumonia,57 myocardial infarction,160 lung cancer and strokes161 in people with HIV.
How to promote smoking cessation in this setting is an active area of research. Mobile phone-based approaches and interventions administered at clinic level, such as training staff to administer smoking cessation advice or electronic processes that result in automatic referral to smoking cessation clinics, are generally more effective at achieving cessation than patient-level interventions such as counselling and pharmacotherapy.162 However, these may only achieve short-term cessation.163 A recent Cochrane review assessing the effectiveness of different smoking cessation techniques in people with HIV found that the nicotinic receptor agonist varenicline likely helps people stop smoking for at least 6 months more effectively than other methods, with no evidence of serious adverse events.164 This conclusion was only based on two studies. A systematic review found no increase in neuropsychiatric events associated with varenicline use, other than sleep disorders.165
Even when smoking cessation is achieved in people with HIV, there are high rates of relapse.31,166 This may be due to more withdrawal symptoms and co-consumption of alcohol and illicit drugs.166 Other barriers to cessation include lower rates of employment causing financial instability, significant lifetime psychiatric diagnoses and the fact that peer support networks for people with HIV often include other smokers.36,167 Randomised controlled trials specifically comparing smoking cessation interventions in people with HIV are required.
Modulation of Non-Tobacco Related Risk Factors
Globally, 97% of major cities currently fail to meet the WHO’s recommended annual concentrations of ambient air pollution levels.168 This highlights the size and global nature of the challenge required to reduce environmental exposures that contribute to COPD. Change is required at every level from individual protective methods and the modification of cultural practices to population level policy-based approaches. New technologies such as high efficiency portable air cleaners, which when placed in people’s houses reduce respiratory symptoms and risks of moderate exacerbations of COPD,169 must be combined with global initiatives such as the Clean Cooking Alliance that aims to make clean cooking practices accessable in LMICs.170 Further research is needed to address gaps in our understanding of how to best reduce risk exposures in those with HIV, particularly in LMICs.
Modulation of Chronic Inflammation
HIV increases COPD risk through activation of inflammatory pathways. The exact pathways by which this happen are not fully elucidated and there are no current HIV specific strategies to modulate chronic inflammation to mitigate HIV-related COPD risk. Nevertheless, several trials have looked at interventions that may reduce inflammation in the lung to slow rates of lung function decline.
TGF-B is implicated in the development of emphysema in murine models.171 In the general population, use of angiotensin receptor blockers (ARBs) has been associated with slower emphysema development, potentially due to effects on TGF-B.172 However, in a randomised controlled trial of people with HIV, the use of the ARB losartan was not associated with decreased levels of lung inflammation compared to placebo.173
The use of statins has also been investigated given their pleiotropic effects as potent systemic immune modulators. In a small pilot study of 22 people with HIV, participants were randomised to receive placebo or 24 weeks of daily rosuvastatin therapy, and lung function was recorded over time. People receiving rosuvastatin demonstrated stability in serial FEV1 measurements and improved DLCO, compared to people who received placebo, but this effect was not statistically significant.174
Pharmacological therapies aiming to reduce lung inflammation have also been studied in paediatric populations with HIV. In the double blinded Bronchopulmonary Function in Response to Azithromycin Treatment for Chronic Lung Disease in HIV-Infected Children (BREATHE) trial, 347 children and adolescents from Zimbabwe and Malawi were randomised to receive either weekly azithromycin or placebo for 48 weeks.175 Azithromycin use was associated with reduced rates of exacerbation of respiratory symptoms, but in subsequent analysis at 72 weeks, there was no observed effect of azithromycin on FEV1 decline.176
Other Co-Morbidities
Key considerations regarding the investigation, management and risk mitigation of HIV-associated COPD as previously discussed are outlined in Figure 2. Further consideration should be given to the fact that HIV-associated COPD almost always exists in conjunction with other co-morbidities, many of which are also related to tobacco smoking. Cardiovascular risk assessment is vital given HIV confers an increased risk of cardiovascular disease,177 and COPD in people with HIV has been shown to increase the risk of both type 1 and type 2 myocardial infarction by 2.5–3x, after adjusting for smoking and other typical cardiovascular risk factors.178 Statins reduce the risk of major adverse cardiovascular events even in people with HIV with low-to-moderate cardiovascular risk,179 and are now recommended by the British HIV Association (BHIVA) for all people with HIV over the age of 40 irrespective of lipid profile or cardiovascular risk.180
Compared to seronegative individuals, the incidence of lung cancer may be twice as high for people with HIV.181 It may also present at a younger age and be less curable.182 Current or former smokers with HIV should be considered a target population for lung cancer screening.183,184 Sleep disordered breathing is also common in people with HIV,185 and may present with symptoms that mimic COPD.
What are the Key Research Policy Questions for Now and in the Future?
Whilst there have been recent advances in our understanding of HIV-associated COPD as its own etiotype, there needs to be wider recognition among the global scientific community of the independent risk HIV poses to the lung. HIV should be considered as an independent risk factor for obstructive lung disease in screening tools. This would improve identification of HIV-associated COPD as well as related co-morbidities such as cardiovascular disease and lung cancer. People with HIV should be included in major clinical trials for the treatment of COPD, including assessment of non-pharmacological measures, exercise and pulmonary rehabilitation. Heightened surveillance of respiratory problems in people with HIV is also needed irrespective of smoking status.
Like other etiotypes of COPD, HIV-associated COPD rarely exists in isolation. Further prospective longitudinal cohort studies that control for different risk behaviours and measure symptoms, lung function, imaging, and inflammatory and immune activation biomarkers will help us better understand the natural history of HIV-associated COPD, and the relative contributions made by the different (often interacting) risks. These studies must occur in a variety of different settings and involve populations with different risk exposures including occupational exposures, for example silica dust exposure in miners living with HIV, which may be associated with development of both COPD and TB.186 This will help to better understand the synergistic effect HIV has with other drivers of COPD. Understanding how these factors together impact on lung function and gas exchange will guide future diagnostic technologies and management strategies, which in turn need to be easily deployable in LMICs where the burden of HIV-associated COPD is often under appreciated.
Ultimately, a better understanding of the molecular mechanisms that allow HIV persistence and subsequent inflammation in the lung, and the contribution of HIV-related factors such as immune reconstitution and timing of ART may further the development of HIV-specific strategies to mitigate COPD risk and improve outcomes for the increasing number of people with HIV-associated COPD.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Crothers K, Huang L, Goulet JL, et al. HIV infection and risk for incident pulmonary diseases in the combination antiretroviral therapy era. Am J Respir Crit Care Med. 2011;183(3):388–395. doi:10.1164/rccm.201006-0836OC
2. Gershon AS, Warner L, Cascagnette P, Victor JC, To T. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study. Lancet. 2011;378(9795):991–996. doi:10.1016/S0140-6736(11)60990-2
3. Bigna JJ, Kenne AM, Asangbeh SL, Sibetcheu AT. Prevalence of chronic obstructive pulmonary disease in the global population with HIV: a systematic review and meta-analysis. Lancet Glob Heal. 2018;6(2):e193–e202. doi:10.1016/S2214-109X(17)30451-5
4. Rowell-Cunsolo TL, Hu G, Bellerose M, Liu J. Trends in comorbidities among human immunodeficiency virus–infected hospital admissions in New York city from 2006–2016. Clin Infect Dis. 2020;73(7):e1957–e1963. doi:10.1093/cid/ciaa1760
5. Konstantinidis I, Zou RH, Papageorgiou SN, et al. Effect of human immunodeficiency virus on lung function and structure: a systematic review and meta-analysis. Ann Am Thorac Soc. 2025;22(2):274–284. doi:10.1513/AnnalsATS.202404-384OC
6. Global initiative for obstructive lung disease 2025 report:1-193. Available from: https://goldcopd.org/wp-content/uploads/2024/11/GOLD-2025-Report-v1.0-15Nov2024_WMV.pdf.
7. Collaborators G 2019 CRD; Momtazmanesh S, Moghaddam SS, Ghamari S-H, et al. Global burden of chronic respiratory diseases and risk factors, 1990–2019: an update from the global burden of disease study 2019. eClinicalMedicine. 59;2023:101936. doi:10.1016/j.eclinm.2023.101936
8. Halpin DMG, Celli BR, Criner GJ, et al. The GOLD Summit on chronic obstructive pulmonary disease in low- and middle-income countries. Int J Tuberc Lung Dis. 2019;23(11):1131–1141. doi:10.5588/ijtld.19.0397
9. Global initiative for obstructive lung disease 2023 report. Available from: https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf.
10. Thudium RF, Ronit A, Afzal S, et al. Faster lung function decline in people living with HIV despite adequate treatment: a longitudinal matched cohort study. Thorax. 2023;78(6):535–542. doi:10.1136/thorax-2022-218910
11. Gingo MR, Morris A, Crothers K. Human immunodeficiency virus–associated obstructive lung diseases. Clin Chest Med. 2013;34(2):273–282. doi:10.1016/j.ccm.2013.02.002
12. Byanova K, Kunisaki KM, Vasquez J, Huang L. Chronic obstructive pulmonary disease in HIV. Expert Rev Respir Med. 2021;15(1):71–87. doi:10.1080/17476348.2021.1848556
13. Konstantinidis I, Qin S, Fitzpatrick M, et al. Pulmonary function trajectories in people with HIV: analysis of the Pittsburgh HIV lung cohort. Ann Am Thorac Soc. 2022;19(12):2013–2020. doi:10.1513/AnnalsATS.202204-332OC
14. Byanova KL, Fitzpatrick J, Jan AK, et al. Isolated abnormal diffusing capacity for carbon monoxide (iso↓DLco) is associated with increased respiratory symptom burden in people with HIV infection. PLoS One. 2023;18(7):e0288803. doi:10.1371/journal.pone.0288803
15. Cribbs SK, Crothers K, Morris A. Pathogenesis of HIV-related lung disease: immunity, infection, and inflammation. Physiol Rev. 2020;100(2):603–632. doi:10.1152/physrev.00039.2018
16. Konstantinidis I, Crothers K, Kunisaki KM, et al. HIV-associated lung disease. Nat Rev Dis Primers. 2023;9(1):39. doi:10.1038/s41572-023-00450-5
17. Brown J, Smith C, Johnson M, Lipman M, Abubakar I. Respiratory co-morbidities in people with HIV. Lancet Infect Dis. 2016;16(1):21. doi:10.1016/S1473-3099(15)00468-5
18. Siddharthan T, Pollard SL, Quaderi SA, et al. Discriminative accuracy of chronic obstructive pulmonary disease screening instruments in 3 low- and middle-income country settings. JAMA. 2022;327(2):151–160. doi:10.1001/jama.2021.23065
19. Peprah E, Armstrong-Hough M, Cook SH, et al. An emerging syndemic of smoking and cardiopulmonary diseases in people living with HIV in Africa. Int J Environ Res Public Heal. 2021;18(6):3111. doi:10.3390/ijerph18063111
20. Collaborators G 2015 T; Reitsma MB, Fullman N, Ng M, et al. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: a systematic analysis from the global burden of disease study 2015. Lancet. 2017;389(10082):1885–1906. doi:10.1016/S0140-6736(17)30819-X
21. Collaborators GCRD; Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
22. Mugisha JO, Schatz EJ, Randell M, et al. Chronic disease, risk factors and disability in adults aged 50 and above living with and without HIV: findings from the wellbeing of older people study in Uganda. Glob Heal Action. 2016;9(1):31098. doi:10.3402/gha.v9.31098
23. Akanbi MO, Taiwo BO, Achenbach CJ, et al. HIV associated chronic obstructive pulmonary disease in Nigeria. J AIDS Clin Res. 2015;06(05). doi:10.4172/2155-6113.1000453
24. Foreman MG, Zhang L, Murphy J, et al. Early-onset chronic obstructive pulmonary disease is associated with female sex, maternal factors, and African American race in the COPDGene study. Am J Respir Crit Care Med. 2011;184(4):414–420. doi:10.1164/rccm.201011-1928OC
25. Amaral AFS, Strachan DP, Burney PGJ, Jarvis DL. Female smokers are at greater risk of airflow obstruction than male smokers. UK biobank. Am J Respir Crit Care Med. 2017;195(9):1226–1235. doi:10.1164/rccm.201608-1545OC
26. Fitzpatrick ME, Gingo MR, Kessinger C, et al. HIV infection is associated with diffusing capacity impairment in women. JAIDS J Acquir Immune Defic Syndr. 2013;64(3):284–288. doi:10.1097/QAI.0b013e3182a9213a
27. Wang RJ, Nouraie M, Kunisaki KM, et al. Lung function in women with and without human immunodeficiency virus. Clin Infect Dis. 2022;76(3):e727–e735. doi:10.1093/cid/ciac391
28. McNeill J, Okello S, Sentongo R, et al. Chronic human immunodeficiency virus infection is associated with accelerated decline of forced expiratory volume in 1 second among women but not among men: a longitudinal cohort study in Uganda. Ann Am Thorac Soc. 2022;19(10):1779–1783. doi:10.1513/AnnalsATS.202111-1275RL
29. North CM, MacNaughton P, Lai PS, et al. Personal carbon monoxide exposure, respiratory symptoms, and the potentially modifying roles of sex and HIV infection in rural Uganda: a cohort study. Environ Heal. 2019;18(1):73. doi:10.1186/s12940-019-0517-z
30. Abelman RA, Fitzpatrick J, Zawedde J, et al. Sex modifies the risk of HIV-associated obstructive lung disease in Ugandans postpneumonia. AIDS. 2023;37(11):1683–1692. doi:10.1097/QAD.0000000000003626
31. Mdodo R, Frazier EL, Dube SR, et al. Cigarette smoking prevalence among adults with hiv compared with the general adult population in the United States: cross-sectional surveys. Ann Intern Med. 2015;162(5):335–344. doi:10.7326/M14-0954
32. Wang Y, Chen X, Li X, et al. Cigarette smoking among Chinese PLWHA: an exploration of changes in smoking after being tested HIV positive. AIDS Care. 2016;28(3):365–369. doi:10.1080/09540121.2015.1090536
33. Berg CJ, Nehl EJ, Wong FY, et al. Prevalence and correlates of tobacco use among a sample of MSM in Shanghai, China. Nicotine Tob Res. 2011;13(1):22–28. doi:10.1093/ntr/ntq193
34. Mdege ND, Shah S, Ayo-Yusuf OA, Hakim J, Siddiqi K. Tobacco use among people living with HIV: analysis of data from demographic and health surveys from 28 low-income and middle-income countries. Lancet Glob Heal. 2017;5(6):e578–e592. doi:10.1016/S2214-109X(17)30170-5
35. Chan KH, Wright N, Xiao D, et al. Tobacco smoking and risks of more than 470 diseases in China: a prospective cohort study. Lancet Public Heal. 2022;7(12):e1014–e1026. doi:10.1016/S2468-2667(22)00227-4
36. Frazier EL, Sutton MY, Brooks JT, Shouse RL, Weiser J. Trends in cigarette smoking among adults with HIV compared with the general adult population, United States - 2009–2014. Prev Med. 2018;111:231–234. doi:10.1016/j.ypmed.2018.03.007
37. Zaniku HR, Connolly E, Aron MB, et al. Prevalence and associated factors of chronic obstructive pulmonary disease among adults in Neno District, Malawi: a cross-sectional analytical study. Int J Chronic Obstr Pulm Dis. 2024;19:389–401. doi:10.2147/COPD.S444378
38. Dodd PJ, Yuen CM, Jayasooriya SM, van der Zalm MM, Seddon JA. Quantifying the global number of tuberculosis survivors: a modelling study. Lancet Infect Dis. 2021;21(7):984–992. doi:10.1016/S1473-3099(20)30919-1
39. Fan H, Wu F, Liu J, et al. Pulmonary tuberculosis as a risk factor for chronic obstructive pulmonary disease: a systematic review and meta-analysis. Ann Transl Med. 2021;9(5):390. doi:10.21037/atm-20-4576
40. Kayongo A, Wosu AC, Naz T, et al. Chronic obstructive pulmonary disease prevalence and associated factors in a setting of well-controlled HIV, A cross-sectional study. COPD J Chronic Obstr Pulm Dis. 2020;17(3):297–305. doi:10.1080/15412555.2020.1769583
41. Ddungu A, Semitala FC, Castelnuovo B, Sekaggya-Wiltshire C, Worodria W, Kirenga BJ. Chronic obstructive pulmonary disease prevalence and associated factors in an urban HIV clinic in a low income country. PLoS One. 2021;16(8):e0256121. doi:10.1371/journal.pone.0256121
42. Pathak U, Gupta NC, Suri JC. Risk of COPD due to indoor air pollution from biomass cooking fuel: a systematic review and meta-analysis. Int J Environ Heal Res. 2020;30(1):75–88. doi:10.1080/09603123.2019.1575951
43. Park J, Kim HJ, Lee CH, Lee CH, Lee HW. Impact of long-term exposure to ambient air pollution on the incidence of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Environ Res. 2021;194:110703. doi:10.1016/j.envres.2020.110703
44. Sin DD, Doiron D, Agusti A, et al. Air pollution and COPD: GOLD 2023 committee report. Eur Respir J. 2023;61(5):2202469. doi:10.1183/13993003.02469-2022
45. Li J, Sun S, Tang R, et al. Major air pollutants and risk of COPD exacerbations: a systematic review and meta-analysis. Int J Chronic Obstr Pulm Dis. 2016;11:3079–3091. doi:10.2147/COPD.S122282
46. Blount RJ, Djawe K, Daly KR, et al. Ambient air pollution associated with suppressed serologic responses to pneumocystis jirovecii in a prospective cohort of HIV-infected patients with pneumocystis pneumonia. PLoS One. 2013;8(11):e80795. doi:10.1371/journal.pone.0080795
47. Blount RJ, Daly KR, Fong S, et al. Effects of clinical and environmental factors on bronchoalveolar antibody responses to Pneumocystis jirovecii: a prospective cohort study of HIV+ patients. PLoS One. 2017;12(7):e0180212. doi:10.1371/journal.pone.0180212
48. Crothers K, McGinnis K, Kleerup E, et al. HIV infection is associated with reduced pulmonary diffusing capacity. JAIDS J Acquir Immune Defic Syndr. 2013;64(3):271–278. doi:10.1097/QAI.0b013e3182a9215a
49. Risso K, Guillouet-de-Salvador F, Valerio L, et al. COPD in HIV-infected patients: CD4 cell count highly correlated. PLoS One. 2017;12(1):e0169359. doi:10.1371/journal.pone.0169359
50. Kunisaki KM, Nouraie M, Jensen RL, et al. Lung function in men with and without HIV. AIDS. 2020;34(8):1227–1235. doi:10.1097/QAD.0000000000002526
51. Drummond MB, Merlo CA, Astemborski J, et al. The effect of HIV infection on longitudinal lung function decline among IDUs. AIDS. 2013;27(8):1303–1311. doi:10.1097/QAD.0b013e32835e395d
52. Verboeket SO, Boyd A, Wit FW, et al. Changes in lung function among treated HIV-positive and HIV-negative individuals: analysis of the prospective AGEhIV cohort study. Lancet Heal Longev. 2021;2(4):e202–e211. doi:10.1016/S2666-7568(21)00033-7
53. Kunisaki KM, Niewoehner DE, Collins G, et al. Pulmonary effects of immediate versus deferred antiretroviral therapy in HIV-positive individuals: a nested substudy within the multicentre, international, randomised, controlled strategic timing of antiretroviral treatment (START) trial. Lancet Respir Med. 2016;4(12):980–989. doi:10.1016/S2213-2600(16)30319-8
54. Diaz PT, King MA, Pacht ER, et al. Increased susceptibility to pulmonary emphysema among HIV-seropositive smokers. Ann Intern Med. 2000;132(5):369. doi:10.7326/0003-4819-132-5-200003070-00006
55. Feldman JG, Minkoff H, Schneider MF, et al. Association of cigarette smoking with HIV prognosis among women in the HAART era: a report from the women’s interagency HIV study. Am J Public Heal. 2011;96(6):1060–1065. doi:10.2105/AJPH.2005.062745
56. Murrison LB, Martinson N, Moloney RM, et al. Tobacco smoking and tuberculosis among men living with HIV in Johannesburg, South Africa: a case-control study. PLoS One. 2016;11(11):e0167133. doi:10.1371/journal.pone.0167133
57. De P, Farley A, Lindson N, Aveyard P. Systematic review and meta-analysis: influence of smoking cessation on incidence of pneumonia in HIV. BMC Med. 2013;11(1):15. doi:10.1186/1741-7015-11-15
58. Drummond MB, Kirk GD, Ricketts EP, et al. Cross sectional analysis of respiratory symptoms in an injection drug user cohort: the impact of obstructive lung disease and HIV. BMC Pulm Med. 2010;10(1):27. doi:10.1186/1471-2466-10-27
59. Kendall CE, Wong J, Taljaard M, et al. A cross-sectional, population-based study measuring comorbidity among people living with HIV in Ontario. BMC Public Heal. 2014;14(1):161. doi:10.1186/1471-2458-14-161
60. Islam M, Ramesh N, Kolman S, et al. Association between CD4+, viral load, and pulmonary function in HIV. Lung. 2017;195(5):635–642. doi:10.1007/s00408-017-0030-5
61. Triplette M, Justice A, Attia EF, et al. Markers of chronic obstructive pulmonary disease are associated with mortality in people living with HIV. AIDS. 2018;32(4):487–493. doi:10.1097/QAD.0000000000001701
62. Li Y, Nouraie SM, Kessinger C, et al. Factors associated with progression of lung function abnormalities in HIV-infected individuals. JAIDS J Acquir Immune Defic Syndr. 2018;79(4):501–509. doi:10.1097/QAI.0000000000001840
63. Abdo M, Kunisaki KM, Morris A, et al. Pulmonary function and quality of life in aging men with and without HIV from the multicenter AIDS cohort study. AIDS Res Hum Retroviruses. 2023;39(12):621–632. doi:10.1089/aid.2023.0001
64. Fitzpatrick ME, Singh V, Bertolet M, et al. Relationships of pulmonary function, inflammation, and T-cell activation and senescence in an HIV-infected cohort. AIDS. 2014;28(17):2505–2515. doi:10.1097/QAD.0000000000000471
65. Fitzpatrick ME, Nouraie M, Gingo MR, et al. Novel relationships of markers of monocyte activation and endothelial dysfunction with pulmonary dysfunction in HIV-infected persons. AIDS. 2016;30(9):1327–1339. doi:10.1097/QAD.0000000000001092
66. Jeon D, Chang EG, McGing M, et al. Pneumoproteins are associated with pulmonary function in HIV-infected persons. PLoS One. 2019;14(10):e0223263. doi:10.1371/journal.pone.0223263
67. Jan AK, Moore JV, Wang RJ, et al. Markers of inflammation and immune activation are associated with lung function in a multi-center cohort of persons with HIV. AIDS. 2021;35(7):1031–1040. doi:10.1097/QAD.0000000000002846
68. Crothers K, Petrache I, Wongtrakool C, Lee PJ, Schnapp LM, Gharib SA. Widespread activation of immunity and pro‐inflammatory programs in peripheral blood leukocytes of HIV‐infected patients with impaired lung gas exchange. Physiol Rep. 2016;4(8):e12756. doi:10.14814/phy2.12756
69. Zhang M, Dai G, Smith DL, et al. Interferon-signaling pathways are upregulated in people with HIV with abnormal pulmonary diffusing capacity (DLCO). AIDS. 2024;38(10):1523–1532. doi:10.1097/QAD.0000000000003946
70. Morris AM, Huang L, Cchetti P, et al. Permanent declines in pulmonary function following pneumonia in human immunodeficiency virus-infected persons. Am J Respir Crit Care Med. 2012;162(2):612–616. doi:10.1164/ajrccm.162.2.9912058
71. Neder JA, Berton DC, Muller PT, O’Donnell DE. Incorporating lung diffusing capacity for carbon monoxide in clinical decision making in chest medicine. Clin Chest Med. 2019;40(2):285–305. doi:10.1016/j.ccm.2019.02.005
72. Ringheim H, Thudium RF, Jensen JUS, Rezahosseini O, Nielsen SD. Prevalence of emphysema in people living with human immunodeficiency virus in the current combined antiretroviral therapy era: a systematic review. Front Med. 2022;9:897773. doi:10.3389/fmed.2022.897773
73. Wenger D, Triplette M, Shahrir S, et al. Associations of marijuana with markers of chronic lung disease in people living with HIV. HIV Med. 2021;22(2):92–101. doi:10.1111/hiv.12966
74. Attia EF, Akgün KM, Wongtrakool C, et al. Increased risk of radiographic emphysema in HIV is associated with elevated soluble CD14 and Nadir CD4. Chest. 2014;146(6):1543–1553. doi:10.1378/chest.14-0543
75. Besutti G, Santoro A, Scaglioni R, et al. Significant chronic airway abnormalities in never‐smoking HIV‐infected patients. HIV Med. 2019;20(10):657–667. doi:10.1111/hiv.12785
76. Thudium RF, Ringheim H, Ronit A, et al. Independent associations of tumor necrosis factor-alpha and interleukin-1 beta with radiographic emphysema in people living with HIV. Front Immunol. 2021;12:668113. doi:10.3389/fimmu.2021.668113
77. Triplette M, Attia EF, Akgün KM, et al. A low peripheral blood CD4/CD8 ratio is associated with pulmonary emphysema in HIV. PLoS One. 2017;12(1):e0170857. doi:10.1371/journal.pone.0170857
78. Leung JM, Malagoli A, Santoro A, et al. Emphysema distribution and diffusion capacity predict emphysema progression in human immunodeficiency virus infection. PLoS One. 2016;11(11):e0167247. doi:10.1371/journal.pone.0167247
79. Auld SC, Harrington KRV, Nguyen MLT, Colasanti JA, Marconi VC, Staitieh BS. Brief report: alternative pulmonary function measures of emphysema in people with HIV. JAIDS J Acquir Immune Defic Syndr. 2024;97(3):282–285. doi:10.1097/QAI.0000000000003490
80. Raju S, Astemborski J, Drummond MB, et al. Brief report: HIV is associated with impaired pulmonary diffusing capacity independent of emphysema. JAIDS J Acquir Immune Defic Syndr. 2022;89(1):64–68. doi:10.1097/QAI.0000000000002818
81. Robertson TE, Nouraie M, Qin S, et al. HIV infection is an independent risk factor for decreased 6-minute walk test distance. PLoS One. 2019;14(4):e0212975. doi:10.1371/journal.pone.0212975
82. Brown J, Roy A, Harris R, et al. Respiratory symptoms in people living with HIV and the effect of antiretroviral therapy: a systematic review and meta-analysis. Thorax. 2017;72(4):355. doi:10.1136/thoraxjnl-2016-208657
83. Brown J, Pickett E, Smith C, et al. The effect of HIV status on the frequency and severity of acute respiratory illness. PLoS One. 2020;15(5):e0232977. doi:10.1371/journal.pone.0232977
84. Triplette M, Attia E, Akgün K, et al. The differential impact of emphysema on respiratory symptoms and 6-minute walk distance in HIV infection. JAIDS J Acquir Immune Defic Syndr. 2017;74(1):e23–e29. doi:10.1097/QAI.0000000000001133
85. Byun JY, Lambert CC, Fazeli PL, Iyer AS, Batey DS, Vance DE. Symptomatology and quality of life of older people with HIV and comorbid chronic obstructive pulmonary diseases from an HIV clinic in Birmingham, Alabama. J Assoc Nurses AIDS Care. 2024;35(2):91–103. doi:10.1097/JNC.0000000000000452
86. Lambert AA, Kirk GD, Astemborski J, Mehta SH, Wise RA, Drummond MB. HIV infection is associated with increased risk for acute exacerbation of COPD. JAIDS J Acquir Immune Defic Syndr. 2015;69(1):68–74. doi:10.1097/QAI.0000000000000552
87. Depp TB, McGinnis KA, Kraemer K, et al. Risk factors associated with acute exacerbation of chronic obstructive pulmonary disease in HIV-infected and uninfected patients. AIDS. 2016;30(3):455–463. doi:10.1097/QAD.0000000000000940
88. Gingo MR, Nouraie M, Kessinger CJ, et al. Decreased lung function and all-cause mortality in HIV-infected individuals. Ann Am Thorac Soc. 2018;15(2):192–199. doi:10.1513/AnnalsATS.201606-492OC
89. Devadoss D, Singh SP, Acharya A, et al. HIV-1 productively infects and integrates in bronchial epithelial cells. Front Cell Infect Microbiol. 2021;10:612360. doi:10.3389/fcimb.2020.612360
90. Joseph SB, Arrildt KT, Swanstrom AE, et al. Quantification of entry phenotypes of macrophage-tropic HIV-1 across a wide range of CD4 densities. J Virol. 2013;88(4):1858–1869. doi:10.1128/JVI.02477-13
91. Schiff AE, Linder AH, Luhembo SN, et al. T cell-tropic HIV efficiently infects alveolar macrophages through contact with infected CD4+ T cells. Sci Rep. 2021;11(1):3890. doi:10.1038/s41598-021-82066-x
92. Cribbs SK, Lennox J, Caliendo AM, Brown LA, Guidot DM. Healthy HIV-1-infected individuals on highly active antiretroviral therapy harbor HIV-1 in their alveolar macrophages. AIDS Res Hum Retroviruses. 2015;31(1):64–70. doi:10.1089/aid.2014.0133
93. Jambo KC, Banda DH, Kankwatira AM, et al. Small alveolar macrophages are infected preferentially by HIV and exhibit impaired phagocytic function. Mucosal Immunol. 2014;7(5):1116–1126. doi:10.1038/mi.2013.127
94. Hernandez JC, Latz E, Urcuqui-Inchima S. HIV-1 induces the first signal to activate the NLRP3 inflammasome in monocyte-derived macrophages. Intervirology. 2013;57(1):36–42. doi:10.1159/000353902
95. Churchill MJ, Deeks SG, Margolis DM, Siliciano RF, Swanstrom R. HIV reservoirs: what, where and how to target them. Nat Rev Microbiol. 2016;14(1):55–60. doi:10.1038/nrmicro.2015.5
96. Cai Y, Sugimoto C, Arainga M, et al. Preferential destruction of interstitial macrophages over alveolar macrophages as a cause of pulmonary disease in simian immunodeficiency virus–infected rhesus macaques. J Immunol. 2015;195(10):4884–4891. doi:10.4049/jimmunol.1501194
97. Honeycutt JB, Thayer WO, Baker CE, et al. HIV persistence in tissue macrophages of humanized myeloid-only mice during antiretroviral therapy. Nat Med. 2017;23(5):638–643. doi:10.1038/nm.4319
98. Lamers SL, Rose R, Maidji E, et al. HIV DNA is frequently present within pathologic tissues evaluated at autopsy from combined antiretroviral therapy-treated patients with undetectable viral loads. J Virol. 2016;90(20):8968–8983. doi:10.1128/JVI.00674-16
99. Meziane O, Salahuddin S, Pham TNQ, et al. HIV infection and persistence in pulmonary mucosal double negative T cells in vivo. J Virol. 2020;94(24). doi:10.1128/jvi.01788-20
100. Stephenson SE, Wilson CL, Bond NG, et al. Pericytes as novel targets for HIV/SIV infection in the lung. Am J Physiol Lung Cell Mol Physiol. 2020;319(5):L848–L853. doi:10.1152/ajplung.00296.2020
101. Trautmann L, Janbazian L, Chomont N, et al. Upregulation of PD-1 expression on HIV-specific CD8+ T cells leads to reversible immune dysfunction. Nat Med. 2006;12(10):1198–1202. doi:10.1038/nm1482
102. Neff CP, Chain JL, MaWhinney S, et al. Lymphocytic alveolitis is associated with the accumulation of functionally impaired HIV-specific t cells in the lung of antiretroviral therapy–naive subjects. Am J Respir Crit Care Med. 2015;191(4):464–473. doi:10.1164/rccm.201408-1521OC
103. Serrano-Villar S, Sainz T, Lee SA, et al. HIV-infected individuals with low CD4/CD8 ratio despite effective antiretroviral therapy exhibit altered t cell subsets, heightened CD8+ T cell activation, and increased risk of non-AIDS morbidity and mortality. PLoS Pathog. 2014;10(5):e1004078. doi:10.1371/journal.ppat.1004078
104. Popescu I, Drummond MB, Gama L, et al. Activation-induced cell death drives profound lung CD4+ T-cell depletion in HIV-associated chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;190(7):744–755. doi:10.1164/rccm.201407-1226OC
105. Turner CT, Brown J, Shaw E, et al. Persistent T cell repertoire perturbation and T cell activation in HIV after long term treatment. Front Immunol. 2021;12:634489. doi:10.3389/fimmu.2021.634489
106. Chinnapaiyan S, Parira T, Dutta R, et al. HIV infects bronchial epithelium and suppresses components of the mucociliary clearance apparatus. PLoS One. 2017;12(1):e0169161. doi:10.1371/journal.pone.0169161
107. Brune KA, Ferreira F, Mandke P, et al. HIV impairs lung epithelial integrity and enters the epithelium to promote chronic lung inflammation. PLoS One. 2016;11(3):e0149679. doi:10.1371/journal.pone.0149679
108. Chinnapaiyan S, Dutta R, Bala J, et al. Cigarette smoke promotes HIV infection of primary bronchial epithelium and additively suppresses CFTR function. Sci Rep. 2018;8(1):7984. doi:10.1038/s41598-018-26095-z
109. Chand HS, Vazquez-Guillamet R, Royer CM, et al. Cigarette smoke and HIV synergistically affect lung pathology in cynomolgus macaques. J Clin Investig. 2018;128(12):5428–5433. doi:10.1172/JCI121935
110. Xu S, Vucic EA, Shaipanich T, et al. Decreased telomere length in the small airway epithelium suggests accelerated aging in the lungs of persons living with human immunodeficiency virus (HIV). Respir Res. 2018;19(1):117. doi:10.1186/s12931-018-0821-0
111. Chung NPY, Ou X, Khan KMF, Salit J, Kaner RJ, Crystal RG. HIV reprograms human airway basal stem/progenitor cells to acquire a tissue-destructive phenotype. Cell Rep. 2017;19(6):1091–1100. doi:10.1016/j.celrep.2017.04.026
112. Chung NPY, Khan KMF, Andreoli M, Kaner RJ, O’Beirne SL, Crystal RG. Impaired differentiation of small airway basal stem/progenitor cells in people living with HIV. Sci Rep. 2022;12(1):2966. doi:10.1038/s41598-022-06373-7
113. Staitieh BS, Malik S, Auld SC, et al. HIV increases the risk of cigarette smoke-induced emphysema through MMP-9. JAIDS J Acquir Immune Defic Syndr. 2023;92(3):263–270. doi:10.1097/QAI.0000000000003125
114. Neff CP, Atif SM, Logue EC, et al. HIV infection is associated with loss of anti-inflammatory alveolar macrophages. J Immunol. 2020;205(9):2447–2455. doi:10.4049/jimmunol.2000361
115. Ranjit S, Sinha N, Kodidela S, Kumar S. Benzo(a)pyrene in cigarette smoke enhances HIV-1 replication through NF-κB activation via CYP-mediated oxidative stress pathway. Sci Rep. 2018;8(1):10394. doi:10.1038/s41598-018-28500-z
116. Santiago MJ, Chinnapaiyan S, Panda K, et al. MicroRNA mediated suppression of airway lactoperoxidase by TGF-β1 and cigarette smoke promotes airway inflammation. J Inflamm. 2024;21(1):31. doi:10.1186/s12950-024-00405-x
117. Panda K, Santiago MJ, Rahman M, et al. HIV-1 tat protein and cigarette smoke mediated ADAM17 upregulation can lead to impaired mucociliary clearance. Cells. 2024;13(23):2009. doi:10.3390/cells13232009
118. Corleis B, Cho JL, Gates SJ, et al. Smoking and human immunodeficiency virus 1 infection promote retention of CD8 + T cells in the airway mucosa. Am J Respir Cell Mol Biol. 2021;65(5):513–520. doi:10.1165/rcmb.2021-0168OC
119. Cyktor J, Qin S, Staines B, et al. Associations of HIV persistence, cigarette smoking, inflammation, and pulmonary dysfunction in people with HIV on antiretroviral therapy. Medicine. 2022;101(27):e29264. doi:10.1097/MD.0000000000029264
120. Liu J, Williams B, Frank D, Dillon SM, Wilson CC, Landay AL. Inside out: HIV, the gut microbiome, and the mucosal immune system. J Immunol. 2017;198(2):605–614. doi:10.4049/jimmunol.1601355
121. Natalini JG, Singh S, Segal LN. The dynamic lung microbiome in health and disease. Nat Rev Microbiol. 2023;21(4):222–235. doi:10.1038/s41579-022-00821-x
122. Cui L, Lucht L, Tipton L, et al. Topographic diversity of the respiratory tract mycobiome and alteration in HIV and lung disease. Am J Respir Crit Care Med. 2015;191(8):932–942. doi:10.1164/rccm.201409-1583OC
123. Lozupone C, Cota-Gomez A, Palmer BE, et al. Widespread colonization of the lung by tropheryma whipplei in HIV infection. Am J Respir Crit Care Med. 2013;187(10):1110–1117. doi:10.1164/rccm.201211-2145OC
124. Morris A, Beck JM, Schloss PD, et al. Comparison of the respiratory microbiome in healthy nonsmokers and smokers. Am J Respir Crit Care Med. 2013;187(10):1067–1075. doi:10.1164/rccm.201210-1913OC
125. Beck JM, Schloss PD, Venkataraman A, et al. Multicenter comparison of lung and oral microbiomes of HIV-infected and HIV-uninfected individuals. Am J Respir Crit Care Med. 2015;192(11):1335–1344. doi:10.1164/rccm.201501-0128OC
126. Twigg HL, Knox KS, Zhou J, et al. Effect of advanced HIV Infection on the respiratory microbiome. Am J Respir Crit Care Med. 2016;194(2):226–235. doi:10.1164/rccm.201509-1875OC
127. Rofael SAD, Brown J, Pickett E, et al. Enrichment of the airway microbiome in people living with HIV with potential pathogenic bacteria despite antiretroviral therapy. EClinicalMedicine. 2020;24:100427. doi:10.1016/j.eclinm.2020.100427
128. Yang L, Dunlap DG, Qin S, et al. Alterations in oral microbiota in HIV are related to decreased pulmonary function. Am J Respir Crit Care Med. 2019;201(4):445–457. doi:10.1164/rccm.201905-1016OC
129. Zhou JJ, Zhai J, Zhou H, et al. Supraglottic lung microbiome taxa are associated with pulmonary abnormalities in an HIV longitudinal cohort. Am J Respir Crit Care Med. 2020;202(12):1727–1731. doi:10.1164/rccm.202004-1086LE
130. Kayongo A, Bartolomaeus TUP, Birkner T, et al. Sputum microbiome and chronic obstructive pulmonary disease in a rural Ugandan cohort of well-controlled HIV infection. Microbiol Spectr. 2023;11(2):e02139–21. doi:10.1128/spectrum.02139-21
131. Martin JA, Sastre J, De la asunción JG, Pallardó FV, Viña J. Hepatic γ-cystathionase deficiency in patients with AIDS. JAMA. 2001;285(11):1444–1445. doi:10.1001/jama.285.11.1444
132. Cribbs SK, Guidot DM, Martin GS, Lennox J, Brown LA. Anti-retroviral therapy is associated with decreased alveolar glutathione levels even in healthy HIV-infected individuals. PLoS One. 2014;9(2):e88630. doi:10.1371/journal.pone.0088630
133. Cole SB, Langkamp‐Henken B, Bender BS, Findley K, Herrlinger‐Garcia KA, Uphold CR. Oxidative stress and antioxidant capacity in smoking and nonsmoking men with HIV/acquired immunodeficiency syndrome. Nutr Clin Pr. 2005;20(6):662–667. doi:10.1177/0115426505020006662
134. Pacht ER, Diaz P, Clanton T, Hart J, Gadek JE. Alveolar fluid glutathione decreases in asymptomatic HIV-seropositive subjects over time. Chest. 1997;112(3):785–788. doi:10.1378/chest.112.3.785
135. Mandas A, Iorio EL, Congiu MG, et al. Oxidative Imbalance in HIV‐1 Infected Patients Treated with Antiretroviral Therapy. BioMed Res Int. 2009;2009(1):749575. doi:10.1155/2009/749575
136. Yeligar SM, Ward JM, Harris FL, Brown LAS, Guidot DM, Cribbs SK. Dysregulation of alveolar macrophage PPARγ, NADPH oxidases, and TGFβ1 in otherwise healthy HIV-infected individuals. AIDS Res Hum Retroviruses. 2017;33(10):1018–1026. doi:10.1089/aid.2016.0030
137. Cordero AIH, Yang CX, Obeidat M, et al. DNA methylation is associated with airflow obstruction in patients living with HIV. Thorax. 2021;76(5):448–455. doi:10.1136/thoraxjnl-2020-215866
138. Cordero AIH, Yang CX, Yang J, et al. Airway aging and methylation disruptions in HIV-associated chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2022;206(2):150–160. doi:10.1164/rccm.202106-1440OC
139. Drummond MB, Hansel NN, Connett JE, Scanlon PD, Tashkin DP, Wise RA. Spirometric predictors of lung function decline and mortality in early chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;185(12):1301–1306. doi:10.1164/rccm.201202-0223OC
140. Csikesz NG, Gartman EJ. New developments in the assessment of COPD: early diagnosis is key. Int J Chronic Obstr Pulm Dis. 2014;9:277–286.
141. Recommendation: chronic obstructive pulmonary disease: screening | United States preventive services taskforce. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/chronic-obstructive-pulmonary-disease-screening.
142. Chronic lung disease — EACS guidelines. Available from: https://eacs.sanfordguide.com/eacs-part2/chronic-lung-disease/chronic-lung-disease-in-hiv.
143. Lambert AA, Drummond MB, Kisalu A, et al. Implementation of a COPD screening questionnaire in an outpatient HIV clinic. COPD J Chronic Obstr Pulm Dis. 2016;13(6):767–772. doi:10.3109/15412555.2016.1161016
144. Shirley DK, Kaner RJ, Glesby MJ. Screening for chronic obstructive pulmonary disease (COPD) in an urban HIV clinic: a pilot study. AIDS Patient Care STDs. 2015;29(5):232–239. doi:10.1089/apc.2014.0265
145. Quiros-Roldan E, Pezzoli MC, Berlendis M, et al. A COPD case-finding program in a large cohort of HIV-infected persons. Respir Care. 2019;64(2):169–175. doi:10.4187/respcare.06247
146. Schnieders E, Ünal E, Winkler V, et al. Performance of alternative COPD case-finding tools: a systematic review and meta-analysis. Eur Respir Rev. 2021;30(160):200350. doi:10.1183/16000617.0350-2020
147. Yawn BP, Han M, Make BM, et al. Protocol summary of the COPD assessment in primary care to identify undiagnosed respiratory disease and exacerbation risk (CAPTURE) validation in primary care study. Chronic Obstr Pulm Dis. 2021;8(1):60–75.
148. Martinez FJ, Han MK, Lopez C, et al. Discriminative accuracy of the CAPTURE tool for identifying chronic obstructive pulmonary disease in US primary care settings. JAMA. 2023;329(6):490–501. doi:10.1001/jama.2023.0128
149. Li Y, Wen F, Ma Q, et al. Use of CAPTURE to identify individuals who may or may not require treatment for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;208(4):435–441. doi:10.1164/rccm.202303-0504OC
150. Siddharthan T, Wosu AC, Pollard SL, et al. A novel case-finding instrument for chronic obstructive pulmonary disease in low- and middle-income country settings. Int J Chronic Obstr Pulm Dis. 2020;15:2769–2777. doi:10.2147/COPD.S268076
151. George MP, Kannass M, Huang L, Sciurba FC, Morris A. Respiratory symptoms and airway obstruction in HIV-infected subjects in the HAART era. PLoS One. 2009;4(7):e6328. doi:10.1371/journal.pone.0006328
152. Gingo MR, George MP, Kessinger CJ, et al. Pulmonary function abnormalities in HIV-infected patients during the current antiretroviral therapy era. Am J Respir Crit Care Med. 2010;182(6):790–796. doi:10.1164/rccm.200912-1858OC
153. Kunisaki KM, Baker JV, Collins G, et al. Lung function decline in early HIV infection: impact of antiretroviral drug timing and drug regimen. Am J Respir Crit Care Med. 2020;201(6):739–741. doi:10.1164/rccm.201911-2266LE
154. Loke YK, Cavallazzi R, Singh S. Risk of fractures with inhaled corticosteroids in COPD: systematic review and meta-analysis of randomised controlled trials and observational studies. Thorax. 2011;66(8):699. doi:10.1136/thx.2011.160028
155. Miravitlles M, Auladell-Rispau A, Monteagudo M, et al. Systematic review on long-term adverse effects of inhaled corticosteroids in the treatment of COPD. Eur Respir Rev. 2021;30(160):210075. doi:10.1183/16000617.0075-2021
156. Brassard P, Suissa S, Kezouh A, Ernst P. Inhaled corticosteroids and risk of tuberculosis in patients with respiratory diseases. Am J Respir Crit Care Med. 2012;183(5):675–678. doi:10.1164/rccm.201007-1099OC
157. Saberi P, Phengrasamy T, Nguyen D. Inhaled corticosteroid use in HIV‐positive individuals taking protease inhibitors: a review of pharmacokinetics, case reports and clinical management. HIV Med. 2013;14(9):519–529. doi:10.1111/hiv.12039
158. Boyd SD, Hadigan C, Mcmanus M, et al. Influence of low-dose ritonavir with and without darunavir on the pharmacokinetics and pharmacodynamics of inhaled beclomethasone. JAIDS J Acquir Immune Defic Syndr. 2013;63(3):355–361. doi:10.1097/QAI.0b013e31829260d6
159. Boyd SD, Hadigan C, Mcmanus M, et al. EACS Guidelines. Available from: https://eacs.sanfordguide.com/eacs-part1/drug-drug-interactions-other-prescribing-issues/drug-drug-interactions/eacs-bronchodilators-for-copd-arvs-interactions.
160. Petoumenos K, Worm S, Reiss P, et al. Rates of cardiovascular disease following smoking cessation in patients with HIV infection: results from the D:A:D study*. HIV Med. 2011;12(7):412–421. doi:10.1111/j.1468-1293.2010.00901.x
161. D’Couto H, Thielking AM, Sewpaul R, et al. The impact of tobacco smoking and smoking cessation on lung cancer and stroke incidence among people with HIV on antiretroviral therapy in South Africa: a simulation modeling study. BMJ Global Health. 2024;9(12):e017049. doi:10.1136/bmjgh-2024-017049
162. Mann-Jackson L, Choi D, Sutfin EL, et al. A qualitative systematic review of cigarette smoking cessation interventions for persons living with HIV. J Cancer Educ. 2019;34(6):1045–1058. doi:10.1007/s13187-019-01525-2
163. Uthman O, Nduka C, Abba M, et al. Does mode of delivery matter for smoking cessation interventions? A meta-analysis of mHealth versus face-to-face interventions for smoking cessation among people living with HIV (Preprint). JMIR mHealth uHealth. 2017;7(1):e203. doi:10.2196/mhealth.9329
164. Mdege ND, Shah S, Dogar O, et al. Interventions for tobacco use cessation in people living with HIV. Cochrane Database Syst Rev. 2024;2024(8):CD011120.
165. Thomas KH, Martin RM, Knipe DW, Higgins JPT, Gunnell D. Risk of neuropsychiatric adverse events associated with varenicline: systematic review and meta-analysis. BMJ. 2015;350(mar12 8):h1109. doi:10.1136/bmj.h1109
166. Zyambo CM, Burkholder GA, Cropsey KL, et al. Mental health disorders and alcohol use are associated with increased likelihood of smoking relapse among people living with HIV attending routine clinical care. BMC Public Heal. 2019;19(1):1409. doi:10.1186/s12889-019-7705-1
167. Humfleet GL, Delucchi K, Kelley K, Hall SM, Dilley J, Harrison G. Characteristics of HIV-positive cigarette smokers: a sample of smokers facing multiple challenges. AIDS Educ Prev. 2009;21(3_supplement):54–64. doi:10.1521/aeap.2009.21.3_supp.54
168. WHO global air quality guidelines. Available from: https://iris.who.int/bitstream/handle/10665/345329/9789240034228-eng.pdf?sequence=1&isAllowed=y.
169. Hansel NN, Putcha N, Woo H, et al. Randomized clinical trial of air cleaners to improve indoor air quality and chronic obstructive pulmonary disease health: results of the CLEAN AIR study. Am J Respir Crit Care Med. 2022;205(4):421–430. doi:10.1164/rccm.202103-0604OC
170. Batchelor S, Brown E, Scott N, Leary J. Two birds, one stone—reframing cooking energy policies in Africa and Asia. Energies. 2019;12(9):1591. doi:10.3390/en12091591
171. Bonniaud P, Kolb M, Galt T, et al. Smad3 null mice develop airspace enlargement and are resistant to TGF-β-mediated pulmonary fibrosis. J Immunol. 2004;173(3):2099–2108. doi:10.4049/jimmunol.173.3.2099
172. Parikh MA, Aaron CP, Hoffman EA, et al. Angiotensin-converting inhibitors and angiotensin II receptor blockers and longitudinal change in percent emphysema on computed tomography. the multi-ethnic study of atherosclerosis lung study. Ann Am Thorac Soc. 2017;14(5):649–658. doi:10.1513/AnnalsATS.201604-317OC
173. MacDonald DM, Collins G, Wendt CH, et al. Short communication: a pilot study of the effects of losartan versus placebo on pneumoproteins in HIV: a secondary analysis of a randomized double blind study. AIDS Res Hum Retroviruses. 2022;38(2):127–130. doi:10.1089/aid.2020.0285
174. Morris A, Fitzpatrick M, Bertolet M, et al. Use of rosuvastatin in HIV-associated chronic obstructive pulmonary disease. AIDS. 2017;31(4):539–544. doi:10.1097/QAD.0000000000001365
175. Ferrand RA, McHugh G, Rehman AM, et al. Effect of once-weekly azithromycin vs placebo in children with HIV-associated chronic lung disease. JAMA Network Open. 2020;3(12):e2028484. doi:10.1001/jamanetworkopen.2020.28484
176. Madanhire T, McHugh G, Simms V, et al. Longitudinal lung function trajectories in response to azithromycin therapy for chronic lung disease in children with HIV infection: a secondary analysis of the BREATHE trial. BMC Pulm Med. 2024;24(1):339. doi:10.1186/s12890-024-03155-x
177. Currier JS, Taylor A, Boyd F, et al. Coronary heart disease in HIV-infected individuals. JAIDS J Acquir Immune Defic Syndr. 2003;33(4):506–512. doi:10.1097/00126334-200308010-00012
178. Crothers K, Nance RM, Whitney BM, et al. Chronic obstructive pulmonary disease and the risk for myocardial infarction by type in people with HIV. AIDS. 2023;37(5):745–752. doi:10.1097/QAD.0000000000003465
179. Grinspoon SK, Fitch KV, Zanni MV, et al. Pitavastatin to prevent cardiovascular disease in HIV Infection. N Engl J Med. 2023;389(8):687–699. doi:10.1056/NEJMoa2304146
180. BHIVA rapid guidance on the use of statins for primary prevention of cardiovascular disease in people living with HIV v2. Available from: https://bhiva.org/wp-content/uploads/2024/10/BHIVA-rapid-guidance-on-the-use-of-statins.pdf.
181. Haas CB, Engels EA, Horner MJ, et al. Trends and risk of lung cancer among people living with HIV in the USA: a population-based registry linkage study. Lancet HIV. 2022;9(10):e700–e708. doi:10.1016/S2352-3018(22)00219-3
182. Bhikoo R, Allwood BW, Irusen EM, Koegelenberg CFN. Lung cancer presents at a younger age and is less likely to be curable in people living with HIV. Respiration. 2024;103(1):47–50. doi:10.1159/000534464
183. Díaz-álvarez J, Roiz P, Gorospe L, et al. Implementation of a lung cancer screening initiative in HIV-infected subjects. PLoS One. 2021;16(12):e0260069. doi:10.1371/journal.pone.0260069
184. Januszewski AP, Bower M. Lung cancer in people living with HIV. Lancet HIV. 2022;9(10):e670–e672. doi:10.1016/S2352-3018(22)00252-1
185. Punjabi NM, Brown TT, Aurora RN, et al. Prevalence and predictors of sleep-disordered breathing in men participating in the multicenter AIDS cohort study. Chest. 2023;163(3):687–696. doi:10.1016/j.chest.2022.10.030
186. Lalloo UG, Pillay S, Mngqibisa R, Abdool-Gaffar S, Ambaram A. HIV and COPD: a conspiracy of risk factors. Respirology. 2016;21(7):1166–1172. doi:10.1111/resp.12806
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.