Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Chronic Khat Chewing Induced High-Grade Hemorrhoidal Disease and Post-Operative Bleeding in Yemen
Authors Al-Kubati WR ![]()
Received 19 December 2024
Accepted for publication 12 April 2025
Published 19 April 2025 Volume 2025:21 Pages 489—499
DOI https://doi.org/10.2147/TCRM.S498067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Waheeb Radman Al-Kubati1,2
1Surgical Department, 21st September University, Sana’a, Yemen; 2Physiology Department, Sana’a University, Sana’a, Yemen
Correspondence: Waheeb Radman Al-Kubati, Surgical Department, 21st September University, Physiology department, Sana’a University, Sana’a, Yemen, Email [email protected]
Background: Khat contains alkaloids, tannins, and flavonoids with physiological and pathological effects. In Yemen, anorectal diseases, including hemorrhoids, are prevalent, and hemorrhoidectomy is frequently performed.
Purpose: This study evaluates the relationship between chronic khat chewing and high-grade hemorrhoidal disease, as well as post-operative complications such as bleeding and pain.
Patients and Methods: This prospective cross-sectional study included 1,896 patients aged 16– 85 years, meeting the inclusion criteria were included and followed for three months.
Patients Were Divided Into Two Groups: Chronic khat chewers (n=1,492) and non-khat chewers (n=404) Data included khat habits, clinical assessments, digital rectal exams, anoproctoscopy, intraoperative findings, and post-operative outcomes.
Results: Chronic khat chewing was strongly associated with thrombosed grade IV hemorrhoidal disease. Among khat chewers, 90% had hemorrhoids, with 75% requiring hemorrhoidectomy or hemorrhoidopexy, compared to 25% in non-chewers, where half underwent hemorrhoidopexy. The odds ratio (OR) for hemorrhoids in khat chewers was 27.04. Gender-specific analysis showed a six-fold higher OR for hemorrhoids in khat-chewing females versus non-chewing females. Post-operative complications, including bleeding and severe pain, were significantly higher in male khat chewers (p < 0.05), while no significant differences were observed in females.
Conclusion: Chronic khat chewing is strongly associated with high-grade hemorrhoidal disease and increased post-operative complications. Mechanisms include chronic constipation, increased anal sphincter tone, and prolonged sitting. These findings highlight the need for public health strategies to reduce khat use and tailored clinical approaches to improve outcomes. Future research should focus on establishing causality, identifying confounders, dose-response relationships, and exploring gender-specific management strategies that target both mechanical and pharmacological factors to optimize surgical care and long-term outcomes.
Plain Language Summary: The study investigates how chronic khat chewing affects high-grade hemorrhoidal disease development and post-operative complications such as bleeding and pain in Yemeni patients. The researchers studied 1,896 patients (1,492 khat chewers, 404 non-chewers) aged 16– 85 and evaluated for khat use, symptoms, surgeries, and post-operative outcomes. The study revealed that severe hemorrhoids affected 90% of khat chewers vs 25% of non-chewers. Hemorrhoidectomy was needed in 75% of chewers vs 50% of non-chewers, with significantly higher post-surgical pain and bleeding, particularly in males. Khat use is widespread in Yemen and contributes to chronic constipation, increased anal sphincter tone, and prolonged sitting, heightening the risk of hemorrhoids and surgical complications. These effects make chronic khat use a key risk factor for severe hemorrhoidal disease and post-surgical issues.
Public health efforts should raise awareness of khat-related risks, while surgeons must consider khat habits in hemorrhoidal disease management. Tailored treatment approaches, including dietary adjustments and bowel regulation, can help reduce complications and improve patient outcomes. Addressing this issue requires both reducing khat consumption and enhancing clinical care strategies.
Keywords: khat, hemorrhoids, hemorrhoidectomy, post-operative bleeding
Introduction
Khat, a plant predominantly found in Yemen and East Africa, particularly Somalia and Ethiopia, is widely chewed for its stimulating effects. The primary active compound in khat is the alkaloid cathinone, which acts similarly to amphetamine on the central nervous and peripheral sympathomimetic systems. Khat use is common in countries across Sudan to Madagascar and Yemen containing various alkaloids, tannins, flavonoids, and other substances with both physiological and pathological effects.1–3,
Khat chewing typically begins after lunch, with each individual consuming approximately 400 to 500 grams of fresh leaves for a mean of 4 hours. The leaves are chewed and held in the cheek, and the extract is either swallowed or spit out. In Yemen, anorectal diseases such as constipation, anal fissures, perianal fistulas, abscesses, and hemorrhoids are prevalent, and hemorrhoidectomy is frequently performed in Yemeni hospitals. This study investigates the relationship between chronic khat chewing and high-grade hemorrhoidal disease, with a focus on post-operative bleeding and pain, aiming to uncover potential mechanisms by which khat contributes to these conditions.
Recent epidemiological studies highlight an increasing prevalence of hemorrhoidal disease in regions with high khat consumption. Chronic khat chewers develop hemorrhoidal disease via dual pathways—mechanical (eg, constipation) and pharmacological (vascular effects), supporting our findings.4 Khat’s gastrointestinal effects stem from its tannins and cathinone content, which inhibit peristalsis causing hypomotility and straining, increase anal sphincter resting pressure, and cause constipation—key risk factors for hemorrhoids. Additionally, cathinone’s vasoconstrictive properties on the vascular system. This effect can lead to increased heart rate, blood pressure, peripheral and anal vascular constriction, and elevated sphincter tone, exacerbating hemorrhoidal disease and potentially worsening postoperative outcomes.4,5
Prolonged sedentary chewing (4–8 hours) further worsens these effects. Constipation prevalence ranges from 23–48% (Al-Hadrani AM, 2000, Burkitt DP, 1972; Hizawa K, 1994).1,6,7 Chronic khat use is also linked to systemic inflammation, hematological changes, and undernutrition (Leminie et al, 2021) with poor dietary habits worsening gastrointestinal symptoms (Hailesellasie et al, 2024).8,9 Further research is needed to confirm causality and long-term effects.
Methods
This prospective cross-sectional study was conducted in private hospitals across Yemen from January 2009 to January 2023. A total of 1,896 patients aged 16 to 85 years were enrolled, including 1,492 khat chewers (Group 1) and 404 non-khat chewers (Group 2).
Inclusion Criteria
The non-khat chewer control group comprised patients presenting with anorectal diseases other than hemorrhoids, which may introduce confounding factors. This limitation was acknowledged, and future studies are encouraged to match control and intervention groups on broader baseline characteristics.
Data Collection
Data collected included demographic details, khat chewing habits (self-reported using a structured questionnaire detailing frequency and duration of chewing sessions), presenting symptoms, clinical assessments, and intraoperative outcomes. Post-operative outcomes, including bleeding and pain, were quantified using patient-reported outcome measures (PROMs), specifically:
Pain: Assessed using the Visual Analog Scale (VAS), rated from 0 (no pain) to 10 (worst pain). The Visual Analog Scale (VAS) was used for pain assessment due to its simplicity and validated use in post-surgical pain evaluation.
Bleeding: Evaluated using a graded scale (none, mild, moderate, severe) during post-operative follow-ups at 1 week, 1 month, and 3 months.
Diagnostic Criteria for Hemorrhoidal Disease
High-grade hemorrhoidal disease was diagnosed based on patient history, and clinical evaluation for location, size, and extent of hemorrhoidal tissue through digital rectal examinations and anoproctoscopy using the Goligher classification, which categorizes them as follows:
- Grade I: Hemorrhoids that bleed but do not prolapse.
- Grade II: Hemorrhoids that prolapse during defecation but spontaneously reduce.
- Grade III: Hemorrhoids that prolapse and require manual reduction.
- Grade IV: Hemorrhoids that are prolapsed and cannot be manually reduced.
Surgical Intervention
Laser excisional hemorrhoidectomy was the predominant surgical procedure (95%), while laser hemorrhoidopexy was performed in 5% of cases. Surgical indications were determined by standardized clinical criteria and patient preferences, as recorded during clinical consultations.
Statistical Analysis
- Descriptive Statistics: Mean and standard deviation (SD) were used for continuous variables (eg, age), and percentages for categorical variables (eg, sex, khat chewing status).
- Chi-Square and Fisher’s Exact Test: These were employed to evaluate associations between khat chewing and outcomes such as hemorrhoids, surgical intervention, and complications. Fisher’s exact test was used for low-frequency categories.
- Multivariable Logistic Regression: Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to control for confounders such as age, sex, dietary habits, and lifestyle factors.
- Power Analysis: A post hoc power analysis confirmed sufficient sample size for detecting significant associations, although the imbalance between groups was acknowledged as a limitation.
- Addressing Sample Size Imbalance: Future studies are recommended to apply propensity score matching or stratified analysis to minimize the impact of this limitation.
Ethical Considerations
This Study Complies With the Principles Outlined in the Declaration of Helsinki
Written informed consent was obtained from all participants before participation. For participants under 18 years of age, parental or guardian consent was obtained in accordance with the ethical guidelines set by the Institutional Review Board (IRB) of the 21 of September University of Medical & Applied Sciences, Faculty of Medicine, Sana’a, Yemen. All data were anonymized to ensure confidentiality.
Results
Demographics and Baseline Characteristics
A total of 1,896 patients were included in the study, with 1,492 chronic khat chewers and 404 non-khat chewers. The mean age was similar between the groups (khat chewers: 42.3 ± 10.5 years; non-khat chewers: 41.8 ± 11.1 years; p = 0.08). Males constituted a higher proportion in both groups (66.7% in khat chewers vs 75.2% in non-khat chewers). Table 1 summarizes the baseline characteristics of the participants.
 |
Table 1 Descriptive Statistics of Patient Demographics by Group |
Prevalence of Hemorrhoids
Hemorrhoids were significantly more prevalent among khat chewers (90%) compared to non-khat chewers (25%), with an odds ratio (OR) of 27.04 (95% CI: 20.40–35.84, p < 0.00001; Table 2, Figure 1). Gender-specific analysis revealed that male khat chewers had a slightly higher prevalence (87.1%) compared to female khat chewers (81.4%) (p = 0.03). These findings were further supported by logistic regression analysis (Table 3), indicating that khat chewing independently increased the odds of hemorrhoids (adjusted OR = 25.96; 95% CI: 20.45–32.98).
 |
Table 2 Odds Ratios For Hemorrhoids And Hemorrhoidectomy in Khat Chewers Vs Non-Chewers |
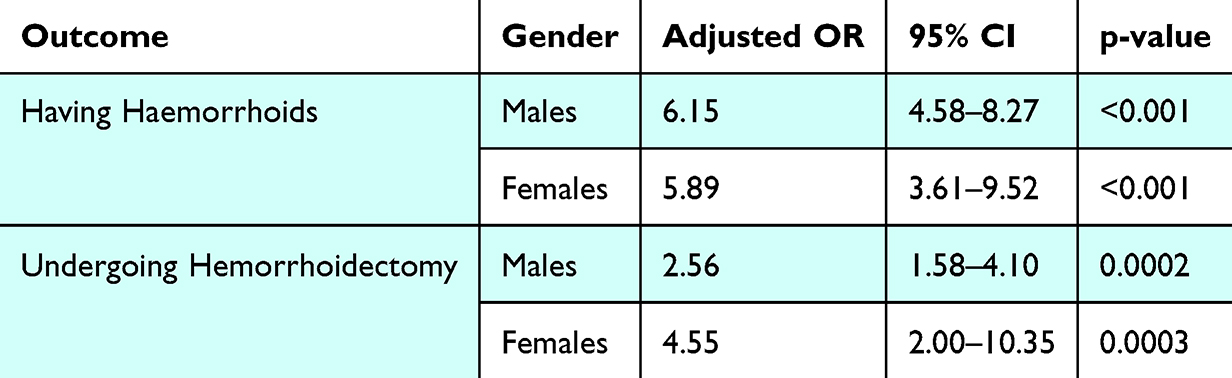 |
Table 3 Logistic Regression Adjusted Odds Ratios for Haemorrhoids and Hemorrhoidectomy by Gender |
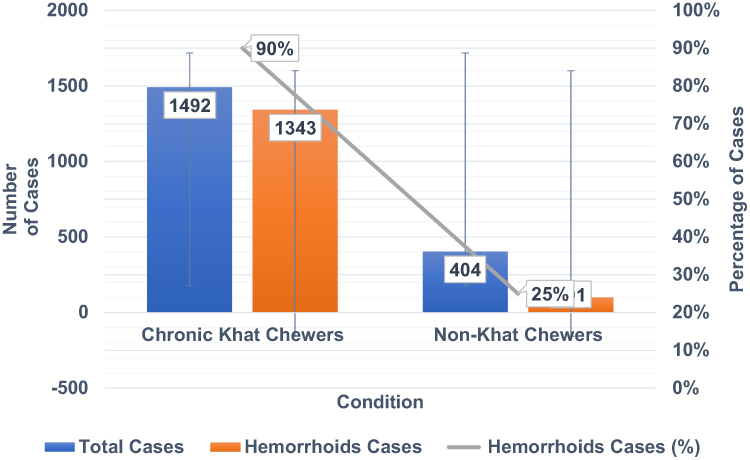 |
Figure 1 Hemorrhoids Cases by Group in Khat Chewers vs Non-Khat Chewers. |
Surgical Intervention: Hemorrhoidectomy
The need for hemorrhoidectomy was significantly higher among khat chewers (75%) compared to non-khat chewers (50%), with an OR of 3.06 (95% CI: 2.03–4.60, p < 0.00001; Table 2, Figure 2). Gender-specific analysis showed that females had a higher likelihood of undergoing hemorrhoidectomy (OR = 4.80; 95% CI: 2.10–10.98, p = 0.000176) compared to males (OR = 2.64; 95% CI: 1.62–4.29, p = 0.000168) (Table 4).
 |
Table 4 Odds Ratios By Gender For Hemorrhoids and Postoperative Complications |
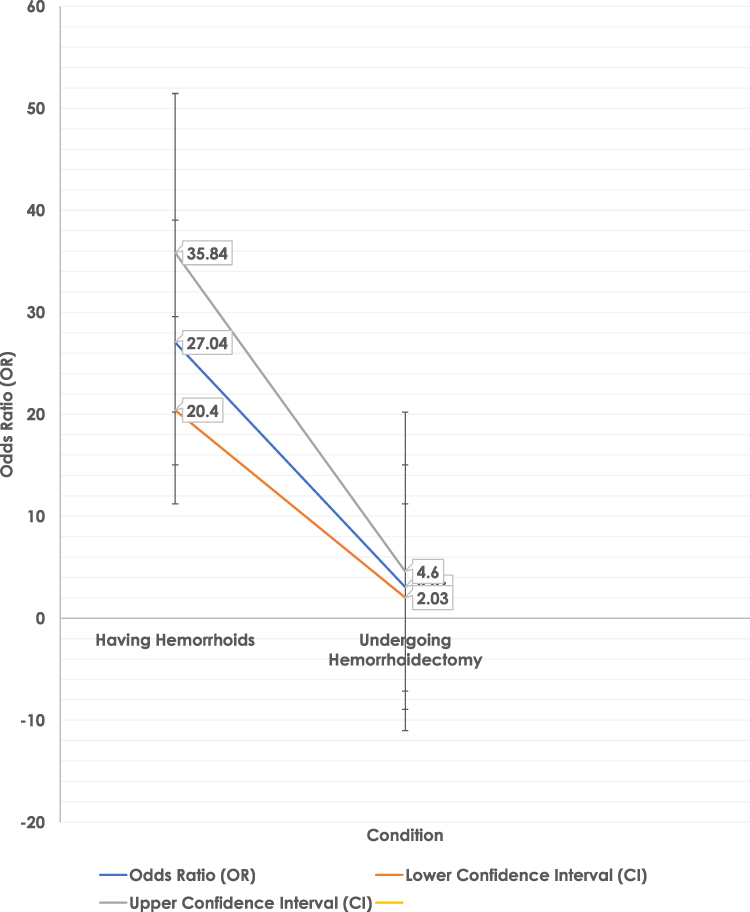 |
Figure 2 Odds Ratios for Developing Hemorrhoids and Requiring Hemorrhoidectomy in Khat Chewers vs Non-Khat Chewers. |
Postoperative Complications
Postoperative complications, including bleeding and severe pain, were more frequent among khat chewers (12.5%) compared to non-khat chewers (4.2%; p < 0.001). Gender-specific analysis indicated that males were more likely to experience severe postoperative pain (OR = 3.89; 95% CI: 0.92–16.53, p = 0.047), while the odds were not statistically significant in females (OR = 5.95; 95% CI: 0.29–84.46, p = 0.233) (Table 4, Figure 3).
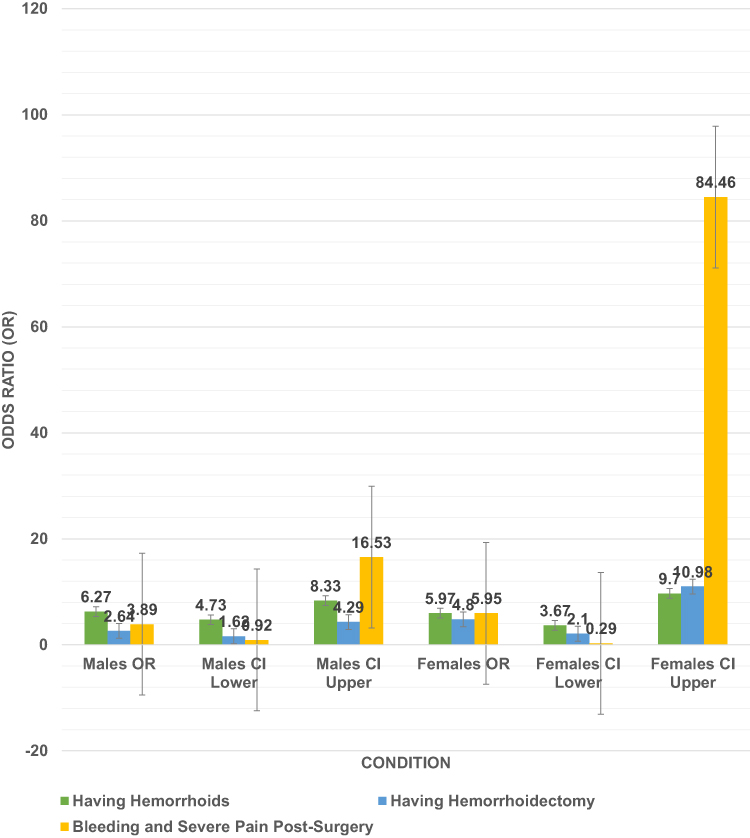 |
Figure 3 Gender-Based Odds Ratios for Hemorrhoids, Hemorrhoidectomy, and Postoperative Complications. |
Statistical Analysis
Chi-square and Fisher’s exact tests confirmed the significant association between khat chewing and hemorrhoidal outcomes (p < 0.00001 for both hemorrhoid prevalence and hemorrhoidectomy rates; Table 5). Multivariable logistic regression (Table 3) demonstrated that khat chewing was an independent risk factor for hemorrhoidal disease and surgical intervention, even after adjusting for age, sex, and dietary factors.
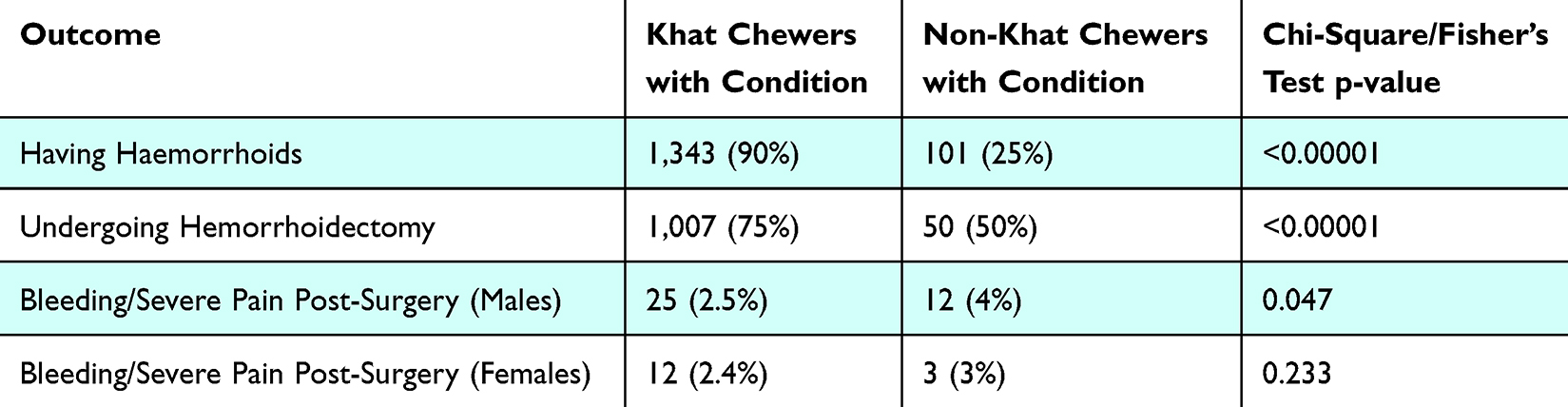 |
Table 5 Chi-Square/Fisher’s Exact Test Results for Association Between Khat Chewing and Haemorrhoids Outcomes |
Discussion
This study explores the association between chronic khat chewing and the development of high-grade hemorrhoidal disease, as well as its impact on post-operative complications in Yemen. Our findings reveal a significantly higher prevalence of advanced hemorrhoidal disease among chronic khat chewers. Specifically, 90% of khat chewers presented with third- or fourth-degree hemorrhoids, with 75% requiring hemorrhoidectomy. In contrast, only 25% of non-khat chewers were diagnosed with hemorrhoids, and only half of these cases required surgical intervention. Statistical analysis demonstrated a robust correlation between khat chewing and the prevalence of hemorrhoidal disease requiring treatment (p < 0.05). Post-operative complications such as pain and bleeding were also more common among khat chewers, underscoring the clinical impact of chronic khat use.1,2,10
Key Findings and Broader Implications
Chronic khat chewing was identified as a significant and independent risk factor for hemorrhoidal disease, with khat chewers exhibiting a substantially higher prevalence, severity, and need for surgical intervention compared to non-khat chewers. Gender-specific differences were evident, as male khat chewers were more likely to experience postoperative complications, such as severe pain and bleeding, while females had higher odds of undergoing hemorrhoidectomy. These findings emphasize the importance of targeted public health interventions to address khat use as a modifiable risk factor for hemorrhoidal disease. Future research should focus on identifying additional confounders, improving sample size balance, and exploring tailored, gender-specific management strategies to optimize care and outcomes.
Physiological and Pathological Effects of Khat Chewing
Prolonged khat chewing introduces a range of physiological and pathological effects that contribute to hemorrhoidal disease. The contracting effects of tannins and the sympathomimetic actions of cathinone, the main active alkaloid in khat, play pivotal roles. These compounds inhibit intestinal peristalsis, increase anal sphincter tone, and lead to chronic constipation and straining. These mechanisms not only aggravate haemorrhoid formation but also contribute to complications such as post-operative bleeding. Additionally, khat chewing sessions, which often last for hours, lead to prolonged sitting, increasing vascular filling and resting anal pressure, further exacerbating haemorrhoid development.6,7,11
Among the Proposed Mechanisms for Hemorrhoidal Pathogenesis Are
1. Deterioration of Connective Tissue: The weakening of connective tissue that anchors hemorrhoids results in the bulging and “sliding” of hemorrhoids into the anal canal, leading to progressive symptoms.12
2. Hypertrophy or Increased Tone of the Internal Anal Sphincter: During defecation, the fecal bolus forces the hemorrhoidal plexus against the internal anal sphincter, causing vessel enlargement and symptomatic hemorrhoids.13
3. Abnormal Distension of the Arteriovenous Anastomoses: Hemorrhoidal cushions may become abnormally distended due to increased arterial flow. This is supported by the observation that hemorrhoids regress following hemorrhoidal artery ligation.14,15
Theories regarding hemorrhoidal development suggest that factors such as the absence of portal venous valves, the upright human posture, and the breakdown of elastic support within the anal cushions are significant contributors.16–18 These theories are consistent with our findings, which highlight chronic constipation, straining, and prolonged sitting as primary contributors to hemorrhoidal development among khat chewers.
Mechanisms Specific to Khat-Induced Hemorrhoids
The pathogenesis of hemorrhoids in chronic khat chewers appears multifactorial. Prolonged sitting during khat chewing exacerbates haemorrhoid formation by increasing vascular filling and resting anal pressure. These physiological impacts align with established theories on hemorrhoidal pathogenesis, emphasizing the role of elastic tissue breakdown, increased anal pressure, and the impact of straining and hard stools.19,20
Tannins in khat inhibit intestinal peristalsis, increase internal anal sphincter tone, and cause chronic constipation and straining.2 The sympathomimetic effects of cathinone further exacerbate these issues by inhibiting detrusor muscle activity, leading to urinary retention and increased intra-abdominal pressure. These factors collectively contribute to the development of high-grade hemorrhoids and subsequent complications.21,22
Gender and Hemorrhoidal Disease
Our findings did not show a significant association between gender and haemorrhoid prevalence in either the khat-chewing or non-chewing groups. However, the higher prevalence of hemorrhoidectomy among males may be linked to the greater proportion of male khat chewers. This finding is consistent with previous research and underscores the need for further studies to evaluate additional factors such as dietary habits and lifestyle influences.2
Perioperative and Postoperative Implications of Khat Chewing
Khat consumption has notable perioperative and postoperative implications. The sympathomimetic effects of cathinone increase anal sphincter tone, contributing to heightened straining and exacerbating hemorrhoidal disease. Furthermore, the prolonged sitting associated with khat chewing heightens intra-abdominal pressure and resting anal pressure, increasing the likelihood of post-operative bleeding and pain. These findings suggest that chronic khat chewing poses significant challenges in the surgical management of hemorrhoids, necessitating tailored perioperative care strategies.7
Khat chewing can delay gastric emptying and reduce intestinal motility, increasing the risk of aspiration during anesthesia. Additionally, the astringent properties of tannins in khat may lead to chronic constipation and straining, contributing to the development or exacerbation of hemorrhoids.22
Understanding the multifaceted effects of khat is vital for optimizing perioperative care and minimizing potential complications in patients who use this substance.
Khat consumption is associated with increase heart rate, vasoconstriction and elevated blood pressure which could attribute to increased postoperative bleeding.23
These effects are primarily due to the sympathomimetic action of cathinone its main amphetamine-like ingredient.
Moreover, khat’s sympathomimetic effects extend to the urinary system, where it inhibits detrusor muscle activity, leading to urinary retention. This urinary retention can result in increased intra-abdominal pressure and straining during defecation, thereby exacerbating hemorrhoid development.24
Erectile Dysfunction and Khat Chewing
Interestingly, erectile dysfunction (ED) were noted in some male patients undergoing hemorrhoidectomy, potentially linked to khat’s sympathomimetic effects on erectile mechanisms. Psychological and cultural factors may also contribute to this observation. Studies in regions with prevalent khat chewing, such as Yemen, have highlighted the association between khat and ED, suggesting that chronic use may exacerbate vascular and neurological factors underlying erectile function.25,26 Psychological and cultural factors may also play a role and warrant further investigation.
Minimally Invasive Techniques and Wound Healing in Hemorrhoidal Surgery
Most studies examining the relationship between khat chewing and hemorrhoidal disease are observational, with limited experimental or longitudinal data available. Additionally, there is a lack of studies examining the dose-response relationship between chewing duration and hemorrhoid severity.
Minimally invasive techniques like laser hemorrhoidoplasty (LHP) have been developed to reduce postoperative pain, improve wound healing, and enhance recovery. A study by Gambardella et al (2023)27 comparing LHP to Milligan-Morgan hemorrhoidectomy (MM) in grade III hemorrhoidal disease found that LHP resulted in significantly lower pain, reduced analgesic use, and faster return to daily activities (2.1 vs 5.8 days). LHP also required only basic wound care, unlike MM, which necessitated frequent dressing changes. However, LHP showed higher recurrence rates for symptoms (21.6% vs 8.1%) and prolapse (18.9% vs 1.1%), indicating a trade-off between short-term comfort and long-term durability.27
Brusciano et al (2019)28 emphasized the role of pelvic floor dynamics in anorectal conditions, suggesting that dysfunction in the chest, abdomen, vertebral column, or perineum may affect surgical outcomes. Addressing these biomechanical factors could help refine minimally invasive approaches. In rectal prolapse management, Brusciano et al (2023)29 found that stapled transanal rectal resection (STARR) effectively alleviates obstructed defecation while minimizing tissue trauma, supporting the broader goal of sphincter preservation.28,29 While LHP offers superior perioperative recovery, excisional techniques like MM may provide better long-term symptom control. Further research is needed to optimize minimally invasive methods, balancing wound healing benefits with long-term efficacy.
Limitations
This study has several limitations that should be acknowledged. First, the imbalance in sample size between khat chewers (1,492) and non-chewers (404) may have introduced bias. However, this distribution reflects the actual prevalence of khat consumption in the study population and provides sufficient statistical power. Second, the study was cross-sectional, limiting the ability to infer causality between chronic khat chewing and hemorrhoidal disease. Third, confounding factors such as dietary habits, lifestyle differences, and socioeconomic status were not fully addressed, which could influence the observed associations. Lastly, the reliance on patient-reported outcomes for post-operative pain and bleeding may have introduced reporting bias.
Future Research Directions
While this study provides strong evidence of the association between chronic khat chewing and high-grade hemorrhoidal disease, several areas require further investigation. First, a structured approach to future research is recommended, including prospective cohort studies that control for confounders such as diet, hydration, and bowel habits to clarify the causal link between chronic khat chewing and high-grade hemorrhoidal disease.
Further investigations should examine the dose-response relationship between chewing duration/frequency and hemorrhoidal severity, as well as explore gender-specific differences in disease progression and post-operative complications. Additionally, longitudinal studies are needed to assess the potential role of khat’s sympathomimetic effects in post-hemorrhoidectomy erectile dysfunction. Expanding research efforts in khat-prevalent regions is essential to develop evidence-based interventions including minimally invasive hemorrhoidal procedures, such as LHP and STARR, to improve outcomes and mitigate its public health impact by addressing both mechanical and pharmacological factors.
Conclusion
This study demonstrates a strong association between chronic khat chewing and the development of high-grade hemorrhoidal disease, with significantly higher prevalence, severity, and postoperative complications among khat chewers compared to non-chewers. Chronic khat chewing exacerbates hemorrhoidal disease through multifactorial mechanisms, including the physiological effects of tannins and cathinone, which induce chronic constipation, increased anal sphincter tone, and straining during defecation and urination. Additionally, prolonged sitting associated with khat chewing amplifies vascular filling and resting anal pressure, further predisposing individuals to hemorrhoidal development and exacerbating existing conditions.
These findings underscore the urgent need for targeted public health strategies to reduce khat use and mitigate its adverse health impacts. Educational campaigns and clinical interventions should raise awareness about khat’s role in gastrointestinal and surgical complications, while tailored perioperative strategies are essential to improve outcomes for hemorrhoidectomy patients with a history of khat use. Future research should adopt prospective cohort designs to establish causality, address confounding factors such as diet and lifestyle, and explore gender-specific management approaches to optimize care and outcomes. Expanding research efforts will be critical to developing evidence-based interventions and mitigating the burden of hemorrhoidal disease in populations where khat use is prevalent.
Acknowledgments
The authors would like to thank the Surgery Department of 21st September University, Sana’a, Yemen, for their support during the study. Special thanks to the medical staff in the involved hospitals for their invaluable assistance in data collection and patient management over the 14-year study period.
Disclosure
The authors declare no competing interests related to this study.
References
1. Al-Hadrani AM. Khat induced hemorrhoidal disease in Yemen. Saudi Med J. 2000;21(5):475–477. PMID: 11500685.
2. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology. 1990;98(2):380–386. PMID: 2295392. doi:10.1016/0016-5085(90)90828-o
3. Alshoabi S Abdulwadoud, Hamid A M, Gameraddin M B, Suliman A G, Omer A M, Alsultan K D, Binmodied A A and Alhamadi M A. (2022). Risks of khat chewing on the cardiovascular, nervous, gastrointestinal, and genitourinary systems. Journal of Family Medicine and Primary Care, 11(1), 32–36. 10.4103/jfmpc.jfmpc_1254_21
4. Oberi IA, Omar Y, Alfaifi AJ, et al. Prevalence of hemorrhoids and their risk factors among the adult population in Jazan, Saudi Arabia. Cureus. 2023;15(9):e45919. doi:10.7759/cureus.45919
5. Nigussie T, Gobena T, Mossie A. Association between khat chewing and gastrointestinal disorders: a cross sectional study. Ethiop J Health Sci. 2013;23(2):123–130. PMID: 23950628; PMCID: PMC3742889.
6. Burkitt DP. Varicose veins, deep vein thrombosis, and hemorrhoids: epidemiology and suggested aetiology. Br Med J. 1972;2(5813):556–561. PMID: 5032782; PMCID: PMC1788140. doi:10.1136/bmj.2.5813.556
7. Hizawa K, Iida M, Suekane H, et al. Mucosal prolapse syndrome: diagnosis with endoscopic US. Radiology. 1994;191(2):527–530. PMID: 8153334. doi:10.1148/radiology.191.2.8153334
8. Leminie AA, Dugul TT, Eshetu EM. Melka DS. catha edulis forsk and ascorbic acid effects on hematological indices in rat. J Blood Med. 2021;12:855–862. PMID: 34602828; PMCID: PMC8480916. doi:10.2147/JBM.S328703
9. Hailesellasie G, Oumer A, Asfaw A. Determinants of undernutrition among khat chewing and non-khat chewing male adults in Addis Ababa, Ethiopia: a comparative cross-sectional study. Sci Rep. 2024. 14(1):4679. PMID: 38409396; PMCID: PMC10897126. doi:10.1038/s41598-024-54471-5
10. Johanson JF. Association of hemorrhoidal disease with chronic constipation. Gastroentrrology. 1990;98:380–486. doi:10.1016/0016-5085(90)90828-O
11. Noorani A, Carapeti E. Hemorrhoids: anatomy, pathophysiology and presentation. In: Cohen R, Windsor A, editors. Anus. London: Springer; 2014:pp. 157–167doi:10.1007/978-1-84882-091-3_13
12. Haas PA, Ta F Jr, Haas GP. The pathogenesis of hemorrhoids. Dis Colon Rectum. 1984;27(7):442–450. PMID: 6745015. doi:10.1007/BF02555533
13. Arabi Y, Alexander-Williams J, Keighley MR. Anal pressures in hemorrhoids and anal fissure. Am J Surg. 1977;134(5):608–610. PMID: 920890. doi:10.1016/0002-9610(77)90445-7
14. Thomson WH. The nature of hemorrhoids. Br J Surg. 1975;62(7):542–552. PMID: 1174785. doi:10.1002/bjs.1800620710
15. Morinaga K, Hasuda K, Ikeda T. A novel therapy for internal hemorrhoids: ligation of the hemorrhoidal artery with a newly devised instrument (Moricorn) in conjunction with a doppler flowmeter. Am J Gastroenterol. 1995;90(4):610–613. PMID: 7717320.
16. Gupta K. Anal Cushions and Pathophysiology of Hemorrhoids. In: Lasers in Proctology. Singapore: Springer; 2022. doi:10.1007/978-981-19-5825-0_3.
17. Welling DR, Rich NM. Hemorrhoid veins, the forgotten realm of the vascular surgeon. J Vasc Surg Venous Lymphat Disord. 2014;2(2):226–229. doi:10.1016/j.jvsv.2012.07.009
18. Michalik M, Pawlak M, Bobowicz M, Witzling M. Long-term outcomes of stapled hemorrhoidopexy. Wideochir Inne Tech Maloinwazyjne. 2014;9(1):18–23. Epub 2013 Nov 26. PMID: 24729805; PMCID: PMC3983538. doi:10.5114/wiitm.2011.35784
19. Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J Gastroenterol. 2012;18(17):2009–2017. PMID: 22563187; PMCID: PMC3342598. doi:10.3748/wjg.v18.i17.2009
20. Romaguera VP, Sancho-Muriel J, Alvarez-Sarrdo E, Millan M, Garcia-Granero A, Frasson M. Postoperative complications in hemorrhoidal disease and special conditions. Rev Recent Clin Trials. 2021;16(1):67–74. PMID: 32250228. doi:10.2174/1574887115666200406114218
21. Al-Motarreb A, Baker K, Broadley KJ. Khat: pharmacological and medical aspects and its social use in Yemen. Phytother Res. 2002;16(5):403–413. PMID: 12203257. doi:10.1002/ptr.1106
22. Silva B, Soares J, Rocha-Pereira C, Mladěnka P, Remião F. on behalf of The OEMONOM researchers. khat, a cultural chewing drug: a toxicokinetic and toxicodynamic summary. Toxins. 2022;14(2):71. doi:10.3390/toxins14020071
23. Al-Habori M. The potential adverse effects of habitual use of Catha edulis (khat). Expert Opin Drug Saf. 2005;4(6):1145–1154. PMID: 16255671. doi:10.1517/14740338.4.6.1145
24. Valente MJ, Guedes de Pinho P, de Lourdes Bastos M, Carvalho F, Carvalho M. Khat and synthetic cathinones: a review. Arch Toxicol. 2014;88(1):15–45. PMID: 24242878. doi:10.1007/s00204-013-1163-9
25. Warfa N, Klein A, Bhui K, Leavey G, Craig T, Alfred Stansfeld S. Khat use and mental illness: a critical review. Soc Sci Med. 2007;65(2):309–318. Epub 2007 Jun 1. PMID: 17544193. doi:10.1016/j.socscimed.2007.04.038
26. Nassar OH, Aklan HM. Erectile dysfunction among yemenis: does chewing khat play a role? Eurasian J Med. 2014;46(2):69–73. PMID:25610301; PMCID:PMC4261453]. doi:10.5152/eajm.2014.18
27. Gambardella C, Brusciano L, Brillantino A, et al. Mid-term efficacy and postoperative wound management of laser hemorrhoidoplasty (LHP) vs conventional excisional hemorrhoidectomy in grade III hemorrhoidal disease: the twisting trend. Langenbecks Arch Surg. 2023;408(1):140. PMID: 37020091; PMCID: PMC10076349. doi:10.1007/s00423-023-02879-4
28. Brusciano L, Gambardella C, Tolone S, et al. An imaginary cuboid: chest, abdomen, vertebral column and perineum, different parts of the same whole in the harmonic functioning of the pelvic floor. Tech Coloproctol. 2019;23(6):603–605. Epub 2019 May 7. PMID: 31065825. doi:10.1007/s10151-019-01996-x
29. Brusciano L, Gambardella C, Falato A, et al. Rectal prolapse pathological features: findings in patients with outlet obstruction treated with stapled transanal rectal resection. Dis Colon Rectum.;66(8):e826–e833. Epub 2022 Feb 28. PMID: 35239529. doi:10.1097/DCR.0000000000002269
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.