Back to Journals » Risk Management and Healthcare Policy » Volume 14
Choroid Plexus Cysts: Single Nucleotide Polymorphism Array Analysis of Associated Genetic Anomalies and Resulting Obstetrical Outcomes
Authors Cai M ![]() , Huang H
, Huang H ![]() , Su L, Wu X, Xie X
, Su L, Wu X, Xie X ![]() , Xu L
, Xu L ![]() , Lin N
, Lin N
Received 25 March 2021
Accepted for publication 3 June 2021
Published 15 June 2021 Volume 2021:14 Pages 2491—2497
DOI https://doi.org/10.2147/RMHP.S312813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Meiying Cai,* Hailong Huang,* Linjuan Su, Xiaoqing Wu, Xiaorui Xie, Liangpu Xu, Na Lin
Medical Genetic Diagnosis and Therapy Center, Fujian Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University, Fujian Key Laboratory for Prenatal Diagnosis and Birth Defect, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liangpu Xu; Na Lin Tel +86-0591-87554929
Email [email protected]; [email protected]
Objective: Choroid plexus cysts (CPC) are pseudocysts in the fetal choroid plexus and can be detected during ultrasound examination. However, the etiology of fetuses with CPC is still unknown. This study aimed to evaluate the genetic anomalies of fetuses with CPC using single nucleotide polymorphism (SNP) array analysis, as well as their obstetrical outcomes.
Patients and Methods: Among 201 fetuses, 108, 69, and 24 had isolated CPC (iCPC), CPC with sonographic soft markers, and CPC with sonographic structural malformations, respectively. All fetuses underwent conventional karyotyping analysis and SNP array analysis.
Results: Among 201 fetuses with CPC, 15 had chromosomal abnormalities (7.5%, 15/201), including nine fetuses with trisomy 18. Further, SNP array results were consistent with the conventional karyotype analysis and additionally revealed 6.0% (12/201) abnormal copy number variations (CNVs). The rates of pathogenic CNVs in fetuses with iCPC, CPC combined with sonographic soft markers, and CPC combined with sonographic structural malformations were 6.5%, 6.0%, and 45.8%, respectively, with significant differences among the groups.
Conclusion: The results of the SNP array affected the obstetrical outcomes. CPC is thus associated with pathogenic CNVs in approximately 10.9% of cases. Therefore, SNP array should be offered for prenatal testing of fetuses with CPC.
Keywords: choroid plexus cysts, SNP, cytogenetic abnormalities, sonographic anomalies
Introduction
Choroid plexus cyst (CPC) is a pseudocyst in the fetal choroid plexus. It was first detected on an ultrasound in the second trimester by Chudleigh et al.1 The prevalence of CPC in the second trimester of pregnancy is 1–2%.2,3 The fetal choroid plexus originates from the specific neuroepithelial cells of the neural tube wall during the embryonic period and is an important location for the secretion of cerebrospinal fluid. When the capillary inside the choroid plexus produces a change with a hemangioma appearance, it can wrap up fluid of one part of the cerebrospinal cord, namely the CPC form. If the nodular capillary network is replaced by a well-differentiated wavy fold, the CPC will gradually shrink or even disappear. Because CPCs are not composed of epithelial tissue, they are generally considered pseudocysts, which mostly disappear before 24 to 26 weeks of gestation. CPCs are not thought to cause fetal development abnormalities. However, recent studies indicate certain relationships between CPC and fetal chromosomal abnormalities. For example, the association between CPC and trisomy 18 has been reported previously.4,5
Chromosomal microarray analysis (CMA) can reveal copy number variations (CNVs) and is gradually replacing karyotype analysis in prenatal testing.6–10 CMA can be divided into two categories, array-based comparative genomic hybridization and single nucleotide polymorphism (SNP) arrays. In addition to detecting CNVs, SNP arrays can also reveal uniparental disomy, triploids, and chimerism.11–13 However, the diagnostic yield of SNP arrays in fetuses with CPC has not been determined previously. Therefore, this study aimed to determine whether there is an association between pathogenic CNVs and fetuses with CPC using both conventional karyotype analysis and SNP array.
Patients and Methods
Ethical Statement
The study was approved by the ethics committee at the Fujian Provincial Maternal and Child Health Hospital (2014–042). Informed consent was obtained from all patients. All procedures were applied following the Declaration of Helsinki, international and national laws, guidelines and regulations.
Patient Data
In all, 201 pregnant women who underwent prenatal ultrasound examination for fetal CPC at Fujian Provincial Maternal and Child Health Hospital from January 2016 to June 2020 were included in the study. The pregnant women were 19 to 46 years of age, with an average age of 28 years. The gestational ages for pregnant women were 18–35 weeks, with an average of 24.9 weeks. The inclusion criterion for this study was a fetus with CPC. The exclusion criterion was a fetus without CPC. After the pregnant woman or her family members provided signed informed consent, amniotic fluid or umbilical cord blood was collected for karyotype analysis and SNP array analysis. The 201 cases were divided into three groups as follows: 108 cases of isolated CPC (iCPC), 69 cases of CPC combined with sonographic soft markers, and 24 cases of CPC combined with sonographic structural malformations.
Conventional Karyotype Analysis
According to the routine method established at our center, the cells from the fetal amniotic fluid or cord blood samples were cultured, harvested, lysed, and subjected to G-banding. The karyotype was collected and analyzed using the GSL-120 automatic chromosome scanning platform. The karyotype results were described according to the international naming system of human cytogenetics (ISCN 2016).
SNP Array
The genomic DNA of fetal cells was extracted using the QIAamp DNA Blood Mini Kit (Qiagen). Digestion, amplification, purification, fragmentation, labeling, hybridization, washing, scanning, and data analysis of the sample genomic DNA were carried out according to the operation manual provided by Affymetrix. The Cytoscan 750k chip contains the CNV probes and SNP probes and can detect CNVs, as well as mosaicism (mosaicism ratio > 10%) and loss of heterozygosity. The matching Chromosome Analysis Suite (ChAS) v3.2 was used to analyze the results; the SNP results were further analyzed in combination with the relevant databases to determine the CNV variation properties. The reference databases included our internal database and online public databases. According to the American College of Medical Genetics (ACMG) guidelines,14 CNVs were divided into pathogenic CNVs, likely pathogenic CNVs, uncertain clinical significance (VUS) CNVs, likely benign CNVs, and benign CNVs. Fluorescence in situ hybridization was used to verify the pathogenic CNVs; SNP detection was also carried out using peripheral blood samples from the parents of fetuses with VUS CNVs, and the nature of these CNVs was further determined by inheritance analysis.
Reagents and Instruments
In the karyotyping technique, the fluid was incubated in amniotic fluid cell culture medium (Biosan technology, China). Giemsa staining (Biosan technology, China) was used to detect banding, and a fully automated chromosome image analyzer (AI Cytovision, Great Britain) was used with the GSL-120 (Leica Microsystems, Germany) automatic chromosome scanning platform to analyze the results. In the SNP array technique, the QIAamp DNA Blood Mini Kit (Qiagen, Germany) was used for whole genome DNA extraction. The DNA was treated according to the manufacturer’s instructions using CytoScan™ 750K Suite (Life Technologies, USA) and was hybridized with the CytoScan™ 750K geneChip (Life Technologies, USA), which contains approximately 250,000 SNP and 500,000 CNV probes. Finally, the gene chips were scanned using a GeneChip System GCS 3000 Dx v.2 (Life Technologies, USA).
Statistical Analysis
IBM SPSS statistics 22 software was used to analyze the experimental data. Corrected chi-square tests were used to analyze the detection rate for pathogenic CNVs among the groups. Differences were considered statistically significant at P < 0.05.
Results
Results of Conventional Karyotype Analysis
Conventional karyotype analysis was carried out in 201 samples, and 15 chromosomal abnormalities were detected (7.5%, 15/201). There were 15 cases of chromosomal abnormalities, including nine cases of trisomy 18, one case of trisomy 21, and five cases of chromosomal structural abnormalities (46, XY, add(18)(p11q22), 46, XX, del(14)(p14.3q32.3), 46, X, del(X)(q28), 46, XY, del(5)(q21q31), 46, XY, add(7)(p22q36); Table 1).
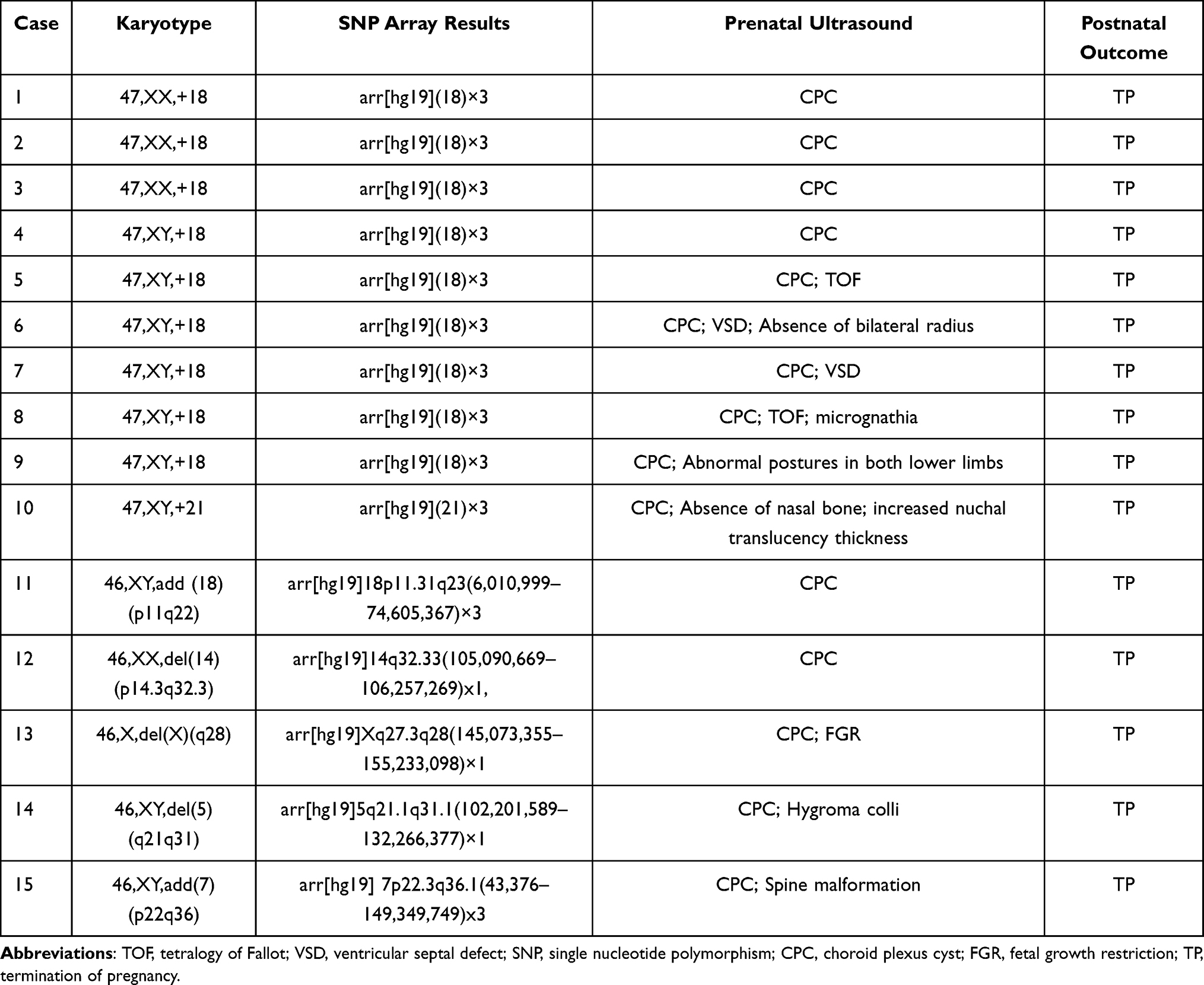 |
Table 1 Abnormal Karyotyping Analysis Results of Fetuses with CPC |
Results of SNP Array Analysis
SNP array analysis was performed for all 201 fetuses with CPC. The results of 15 cases were consistent with the results of karyotype analysis; further, 12 cases of abnormal CNVs were detected using the SNP array (the additional detection rate was 6.0%, 12/201). The sizes of CNVs ranged from 0.3 MB to 4.1 MB. Of the 12 abnormal CNVs, seven were pathogenic and five were of VUS. The seven cases of pathogenic CNVs included two cases of 22q11.21 microdeletion, one case of 2q13 microdeletion, 17q12 microdeletion, 1p31.3 microdeletion, and 15q11.2 microdeletion, and one case of 1q21.1q21.2 microduplication. The five cases of VUS CNVs included the 20q13.2 microduplication, 15q13.3 microduplication, 8p23.2 microduplication, 1q31.1 microduplication, and 14q21.2q21.3 microdeletion (Table 2).
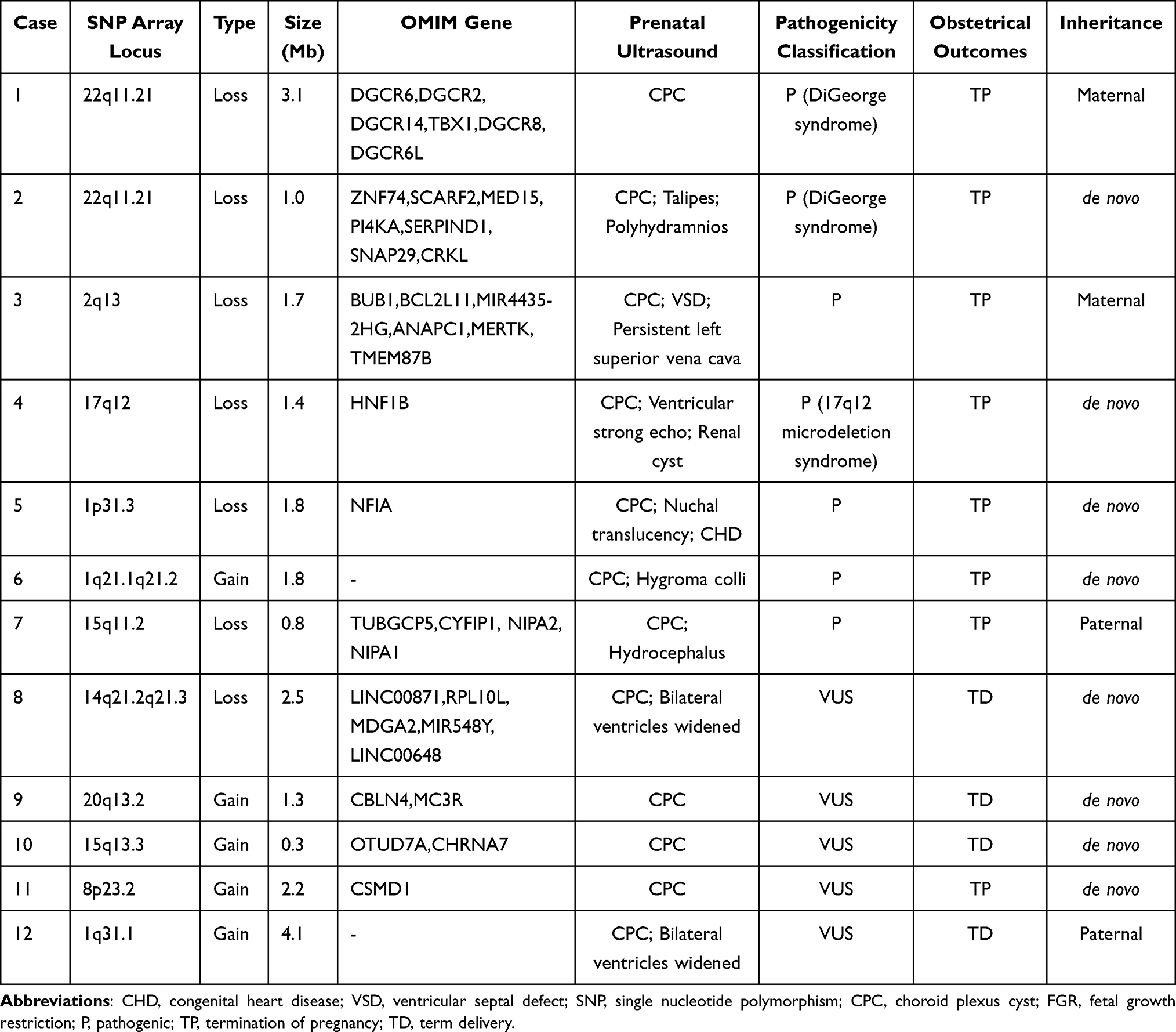 |
Table 2 SNP Results of Fetal CPCs with Normal Karyotype Analysis |
Comparison of Positive Rate of Different CPC Types and Pregnancy Outcome
In the iCPC group, seven cases of pathogenic CNVs were associated with termination of the pregnancy and the remaining 101 cases grew well after birth. Four cases of pathogenic CNVs of CPC with sonographic soft markers were associated with terminated pregnancy and 65 cases grew well after birth. There were 11 cases of pathogenic CNVs detected in CPC with sonographic structural malformations; their parents also chose to terminate the pregnancy. Others in these groups continued with the pregnancy, and the newborns were followed up after birth. There were significant differences among the three groups (χ2 = 34.054, P = 0.000) (Table 3).
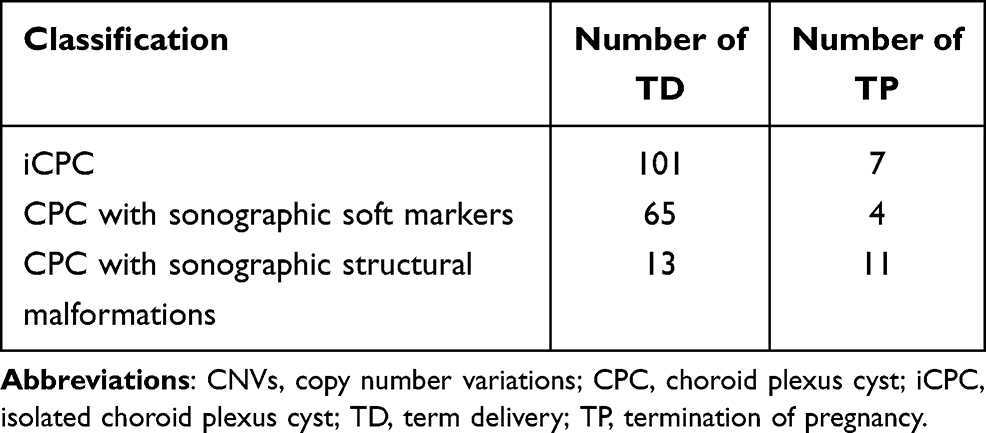 |
Table 3 Obstetrical Outcomes of 201 Fetuses with CPC |
Discussion
CPC is an important sonographic soft marker in the fetus. It is mainly manifested in the anechoic area with a clear boundary in the lateral ventricle. It usually appears as a single cyst on one side or multiple cysts on one or both sides. Fetal CPC originates from the specific neural epithelial cells on the neural tube wall during the embryonic period, which is an important place for cerebrospinal fluid secretion. As the association between CPC and abnormal CNVs is unclear, karyotype analysis and SNP arrays were performed for fetuses with CPC to explore the relationship between CPC and abnormal CNVs in this study.
Papp et al15 found that CPC was the most common ultrasound change in in fetuses with trisomy 18, with an incidence of 38.7%. Most fetuses with trisomy 18 were accompanied by abnormal anatomical structures, and approximately 1/3 of them had CPC.16 In this study, 201 fetuses were assessed by karyotype analysis, 15 cases with chromosomal abnormalities were detected, and the abnormality rate was 7.5%. Trisomy 18 was the most common chromosome abnormality in 15 cases (nine cases in total). Among these, four fetuses with trisomy 18 showed only iCPC, suggesting that fetuses with iCPC had a higher risk of trisomy 18. One fetus with CPC was detected with trisomy 21. In addition to CPC, the ultrasound findings of this case also included the absence of a nasal bone and increased nuchal translucency thickness. These two indicators are common ultrasound indicators of trisomy 21. Current studies suggest that the increased risk of trisomy in fetuses with CPC might be coincidental.5 In addition, five cases of chromosomal unbalanced translocation were detected, indicating that the abnormality in the large segment chromosome altered the genetic material and disturbed the balance between genes, leading to fetal development abnormalities.17
In this study, abnormal CNVs were detected in 12 fetuses with CPC, and seven of these were pathogenic CNVs. The 22q11 Deletion Syndrome (22q11DS) involves multiple systems and organs.18 In our study, 22q11DS was detected in two fetuses with CPC, including one fetus with iCPC. This suggests that fetuses with 22q11DS might also present only with CPC. The SNP array showed a 1.8 Mb microduplication at 1q21.1q21.2 in one fetus with CPC and hygroma colli. This region is a susceptible site for neurocognitive impairment, which might lead to growth retardation, fine and large motor retardation, cardiac malformation, autism, and schizophrenia.19,20 One fetus with CPC, ventricular echo, and a renal cyst had a 1.4 Mb microdeletion at 17q12, which could lead to 17q12 deletion syndrome.21,22 One fetus with CPC and hydrocephalus had a microdeletion of 0.8 Mb at 15q11.2, which could manifest as growth retardation, difficult feeding, and abnormal behavior.23 One fetus with CPC, nuchal translucency, and congenital heart disease had a 1.8 Mb microdeletion at 1p31.3, which is associated with brain dysplasia.24 One fetus with CPC, ventricular septal defect, and persistent left superior vena cava had a 1.7 Mb microdeletion at 2q13, which could manifest as growth retardation and abnormal behavior.25 In total, seven cases with pathogenic CNVs showed CPC phenotypes, which enriched the clinical phenotypes of these pathogenic CNVs.
As SNP arrays have a strong diagnostic ability for fetuses with chromosome abnormalities, many VUS CNVs associated with clinical phenotypes have been detected.26,27 Many related studies have reported that VUS CNVs account for less than 5% of all detected cases.28,29 In this study, five fetuses with VUS CNVs were detected among 201 fetuses, with a detection rate of 2.5%, consistent with literature reports. A case of VUS CNV was found in chromosome 1q31.1 with a fragment size of 4.1 Mb. One fetus had a 0.3 Mb copy number duplication in chromosome 15q13.3. The penetrance of a duplication in chromosome 15q13.3 in the ClinGen database is approximately 5–10%.30 These five VUS CNVs could be related to nervous system development, but whether they are pathogenic remains to be clarified.
The results of the SNP array analysis did affect the obstetrical outcomes. In our study, the parents of 22 fetuses with pathogenic CNVs and one fetus with VUS CNVs chose to terminate the pregnancy. The parents of the remaining fetuses with normal CNVs chose to continue the pregnancy, and the newborns were followed up after birth. SNP array analysis can thus provide an objective theoretical basis for correctly evaluating fetal prognosis and helping pregnant women decide whether to continue their pregnancy. However, the remaining fetuses with normal CNVs should further be used with increasingly advanced technology to identify mutations or other factors involved in CPC etiology.
SNP array is a recently developed molecular karyotype analysis method with advantages such as a short experimental cycle, lack of cell culture, low sample requirement, and high resolution. SNP arrays have been applied for prenatal diagnosis in many laboratories as they can assess the whole genome only through sampled DNA, overcoming the shortcomings of conventional karyotype analysis, and facilitating the rapid detection of microdeletions or microduplications in the whole genome. In this study, the SNP array results of 15 cases were consistent with the results of conventional karyotype analysis; further, 12 cases of chromosomal microdeletion and microduplication were detected by SNP array. The additional detection rate was 6.0% (12/201). SNP arrays are thus more sensitive to detect chromosomal abnormalities in fetuses with CPC and could be a useful and necessary supplement to traditional karyotype analysis. The detection rate of pathogenic CNV was the highest for CPC with abnormal ultrasonic structure (45.8%), followed by iCPC and CPC with abnormal ultrasonic soft index (6.5% and 6.0%, respectively). Therefore, SNP array analysis is highly recommended for fetuses with CPC and abnormal ultrasound structure. Due to the small number of samples in this study, the deficiency point was only seven pathogenic CNVs. In the future, we will expand the sample size and conduct further studies.
In conclusion, it is difficult to judge whether CPC is pathological based on prenatal ultrasound alone. CPC was determined to be associated with pathogenic CNVs in approximately 10.9% of fetuses subjected to SNP array analysis. The SNP array can thus be used as a supplement to karyotype analysis to improve the accuracy of prenatal testing, so as to avoid the omission of pathogenic microdeletions or microduplications. Therefore, the results of this study indicate that SNP array analysis should be offered in prenatal testing for fetuses with CPC.
Acknowledgments
We thank the patients that participated in this study. This study was supported by the Fujian Provincial Natural Science Foundation (grant nos. 2017J01238) and the training project of young and middle-aged talents in health system of Fujian Province (grant nos. 2020GGA020).
Disclosure
The authors declare no conflicts of interest.
References
1. Chudleigh P, Pearce JM, Campbell S. The prenatal diagnosis of transient cysts of the fetal choroid plexus. Prenat Diagn. 1984;4(2):135–137. doi:10.1002/pd.1970040207
2. Tayyar AT, Tayyar M. Multiple Choroid Plexus Cysts: a case report. Int Med J. 2016;5(4):1–8. doi:10.5455/medscience.2016.05.8468
3. Sullivan A, Giudice T, Vavelidis F, et al. Choroid plexus cysts: is biochemical testing a valuable adjunct to targeted ultrasonography? Am J Obstet Gynecol. 1999;181(2):260–265. doi:10.1016/s0002-9378(99)70545-4
4. Sharma A, Dadhwal V, Rana A, et al. Isolated large bilateral choroid plexus cysts associated with trisomy 18. BMJ Case Rep. 2019;12(3):1–10. doi:10.1136/bcr-2019-229216
5. Shah N. Prenatal Diagnosis of Choroid Plexus Cyst: what Next? J Obstet Gynaecol India. 2017;68(3):366–368. doi:10.1007/s13224-017-1047-7
6. Wang Y, Cao L, Liang D, et al. Prenatal chromosomal microarray analysis in fetuses with congenital heart disease: a prospective cohort study. Am J Obstet Gynecol. 2018;218(2):
7. Zhu X, Li J, Ru T. Identification of copy number variations associated with congenital heart disease by chromosomal microarray analysis and next-generation sequencing. Prenat Diagn. 2016;36(4):321–327. doi:10.1002/pd.4782
8. Sukenik-Halevy R, Sukenik S, Koifman A. Clinical aspects of prenatally detected congenital heart malformations and the yield of chromosomal microarray analysis. Prenat Diagn. 2016;36(13):1185–1191. doi:10.1002/pd.4954
9. Xia Y, Yang Y, Huang S, et al. Clinical application of chromosomal microarray analysis for the prenatal diagnosis of chromosomal abnormalities and copy number variations in fetuses with congenital heart disease. Prenat Diagn. 2018;38(6):406–413. doi:10.1002/pd.5249
10. Wou K, Levy B, Wapner RJ. Chromosomal Microarrays for the Prenatal Detection of Microdeletions and Microduplications. Clin Lab Med. 2016;36(2):261–276. doi:10.1016/j.cll.2016.01.017
11. Brady PD, Vermeesch JR. Genomic microarrays: a technology overview. Prenat Diagn. 2012;32(4):336–343. doi:10.1002/pd.2933
12. Zhang Y, Zhong M, Zheng D. Chromosomal mosaicism detected by karyotyping and chromosomal microarray analysis in prenatal diagnosis. J Cell Mol Med. 2020;25(1):358–366. doi:10.1111/jcmm.16080
13. Xiang J, Ding Y, Song X, et al. Clinical Utility of SNP Array Analysis in Prenatal Diagnosis: a Cohort Study of 5000 Pregnancies. Front Genet. 2020;11:571219. doi:10.3389/fgene.2020.571219
14. Hanemaaijer NM, Sikkema-Raddatz B, Vries GVD, et al. Practical guidelines for interpreting copy number gains detected by high-resolution array in routine diagnostics. Eur J Hum Genet. 2012;20(2):161–165. doi:10.1038/ejhg.2011.174
15. Papp C, Szigeti Z, Tóth-Pál E, Hajdú J, Joó JG, Papp Z. Ultrasonographic findings of fetal aneuploidies in the second trimester--our experiences. Fetal Diagn Ther. 2007;23(2):105–113. doi:10.1159/000111588
16. Bronsteen R, Lee W, Vettraino IM, et al. Second-Trimester Sonography and Trisomy 18. J Ultrasound Med. 2004;23(2):241–245. doi:10.7863/jum.2004.23.2.233
17. Hsiao CC, Tsao LY, Chen HN, et al. Changing Clinical Presentations and Survival Pattern in Trisomy 18. Pediatr Neonatol. 2009;50(4):147–151. doi:10.1016/S1875-9572(09)60053-X
18. Sullivan KE. Chromosome 22q11.2 deletion syndrome and DiGeorge syndrome. Immunol Rev. 2019;287(1):186–201. doi:10.1111/imr.12701
19. BenítezBurraco A, BarcosMartínez M, Espejoportero I, et al. Narrowing the Genetic Causes of Language Dysfunction in the 1q21.1 Microduplication Syndrome. Front Pediatr. 2018;16:163–169. doi:10.3389/fped.2018.00163
20. Zhang H, Yue F, Zhang X, et al. Prenatal detection of distal 1q21.1q21.2 microduplication with abnormal ultrasound findings: two cases report and literature review. Medicine. 2021;100(1):e24227. doi:10.1097/MD.0000000000024227
21. Natascha R, Hanna H, Friedrich S, et al. 17q12 Deletion Syndrome as a Rare Cause for Diabetes Mellitus Type MODY5. J Clin Endocrinol Metab. 2018;103(10):3601–3610. doi:10.1210/jc.2018-00955
22. Siolos A, Merkoviti M, Georgiou I, et al. Congenital anomaly of the kidney and urinary tract and mody 5 due to 17Q12 deletion syndrome; a case report. Endocrine Abstracts. 2020. doi:10.1530/endoabs.70.AEP450
23. Butler MG. Clinical and genetic aspects of the 15q11.2 BP1–BP2 microdeletion disorder. J Intellect Disabil Res. 2017;61(6):568–579. doi:10.1111/jir.12382
24. Petti M, Samanich J, Pan Q, et al. Molecular characterization of an interstitial deletion of 1p31.3 in a patient with obesity and psychiatric illness and a review of the literature. Am J Med Genet A. 2011;155(4):825–832. doi:10.1002/ajmg.a.33869
25. Wolfe K, Mcquillin A, Alesi V, et al. Delineating the psychiatric and behavioral phenotype of recurrent 2q13 deletions and duplications. Am J Med Genet B Neuropsychiatr Genet. 2018;177(4):397–405. doi:10.1002/ajmg.b.32627
26. Oneda B, Rauch A. Microarrays in prenatal diagnosis. Best Pract Res Clin Obstet Gynaecol. 2017;42:53–63. doi:10.1016/j.bpobgyn.2017.01.003
27. Hillman SC, McMullan DJ, Hall G, et al. Use of prenatal chromosomal microarray: prospective cohort study and systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2013;41(6):610–620. doi:10.1002/uog.12464
28. Papoulidis I, Sotiriadis A, Siomou E, et al. Routine use of array comparative genomic hybridization (aCGH) as standard approach for prenatal diagnosis of chromosomal abnormalities. Clinical experience of 1763 prenatal cases. Prenat Diagn. 2015;35(13):1269–1277. doi:10.1002/pd.4685
29. Wapner RJ, Martin CL, Levy B, et al. Chromosomal Microarray versus Karyotyping for Prenatal Diagnosis. N Engl J Med. 2012;367(23):2175–2184. doi:10.1056/NEJMoa1203382
30. Zhou D, Gochman P, Broadnax DD, et al. 15q13.3 duplication in two patients with childhood‐onset schizophrenia. Am J Med Genet B Neuropsychiatr Genet s. 2016;171(6):777–783. doi:10.1002/ajmg.b.32439
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.