Back to Journals » Clinical Ophthalmology » Volume 15
“Chopper Shield” Technique to Protect Corneal Endothelium During Phacoemulsification Surgery for Rock Hard Cataracts
Authors Om Parkash T ![]() , Om Parkash R, Mahajan S, Vajpayee R
, Om Parkash R, Mahajan S, Vajpayee R ![]()
Received 27 February 2021
Accepted for publication 21 April 2021
Published 24 May 2021 Volume 2021:15 Pages 2161—2165
DOI https://doi.org/10.2147/OPTH.S308750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "'Chopper Shield’ technique for Rock Hard Cataracts surgery" [ID 308750].
Views: 4294
Tushya Om Parkash,1 Rohit Om Parkash,1 Shruti Mahajan,1 Rasik Vajpayee2– 4
1Cataract Department, Dr Om Parkash Eye Institute, Amritsar, Punjab, India; 2Eye Department, Vision Eye Institute, Melbourne, Victoria, Australia; 3Eye Department, Royal Victorian Eye and Ear Hospital, Melbourne, Victoria, Australia; 4Department of Surgery, University of Melbourne, Melbourne, Victoria, Australia
Correspondence: Shruti Mahajan
Dr Om Parkash Eye Institute, 117-A, The Mall, Amritsar, Punjab, 143001, India
Tel +91-9872553424
Email [email protected]
Purpose: To describe an innovative technique of using a chopper as a shield for preventing mechanical corneal endothelial trauma that can occur during the phacoemulsification of brunescent cataracts.
Methods: This prospective study included patients with hard cataracts (grade nuclear opalescence 4 and above on LOCS III) who underwent phacoemulsification surgery. The chopper shield technique was performed in 48 eyes of 44 patients. The technique entailed placing the chopper horizontally as a shield anterior to the emulsifying nuclear fragment between the phaco tip and corneal endothelium to prevent nucleus fragments from coming into contact with the corneal endothelium. Outcome measures included cumulative dissipated energy (CDE), corneal edema (day one), CCT (assessed at one day, one week, and one month), and endothelial cell density assessed at three months.
Results: Of the 48 eyes included in the study, 23 were males and 25 were females (mean age: 70.02± 5.98years). Preoperatively, mean central corneal thickness (CCT) was 529.62± 21.70 microns, and endothelial cell counts were 2258.76± 182.22 cells per mm2. Postoperatively on day one, CCT increased to 563.93± 24.53 microns, a 6.47% increase from preoperative central corneal thickness. CCT became 534.83± 22.64 microns on postoperative day seven, a 0.98% increase from preoperative CCT. Endothelial cell loss was 6.77% at three months from the day of surgery.
Conclusion: The chopper shield technique offers continuous protection to the corneal endothelium by minimizing endothelial cell loss during phacoemulsification of dense nuclear cataracts.
Keywords: cataract, phacoemulsification, hard cataract, corneal endothelium, chopper shield
Introduction
Phacoemulsification in rock hard cataracts where the nucleus has achieved maximum density is extremely challenging. The bulk of the nucleus requires the use of more ultrasound energy for emulsification compared to that in early nuclear cataracts. High ultrasound energy and prolonged phacoemulsification time are often associated with predisposition to posterior capsule rupture and increased corneal endothelial trauma.1 Corneal endothelial cell loss can also occur due to mechanical trauma caused by the rebounding of nuclear fragments, air bubbles, irrigating solution turbulence, instrumentation, and IOL contact.2,3
Various modalities used to minimize ultrasound energy and reduce damage to surrounding ocular structures during phacoemulsification include direct phaco chop, crater and chop, power modulations in the form of torsional, variable pulse and burst modes, and phaco tips with decreased amplitude near the incision.4–13 In order to minimize endothelial cell loss associated with mechanical trauma, maneuvers such as endocapsular or deeper plane phacoemulsification of totally separated small nuclear fragments, hypothermic perfusion, employment of fluidics to provide a stable anterior chamber, anterior chamber maintainer, replenishing anterior chamber with ophthalmic viscosurgical device (OVD), and use of femtosecond laser or manual prechopping techniques have been described.2,4,11,14–17 However, these modalities do not ensure the prevention of hard nuclear fragments from coming into physical contact with the corneal endothelium during surgery, thereby causing focal endothelial cell loss and precipitating corneal edema in the early postoperative period.18–20
We describe a new technique that employs the use of a chopper to shield corneal endothelial cells from damage that can occur due to direct contact with hard nuclear fragments.
Materials and Methods
This prospective study included patients with hard cataracts (grade nuclear opalescence 4 and above on LOCS III) who underwent phacoemulsification surgery. An informed consent was taken from all patients prior to the surgery and the study followed the principles of the Declaration of Helsinki. Approval was taken from the Dr Om Parkash Eye Institute’s ethics committee. All surgeries were performed by three surgeons (ROP, SM, and TOP). Patients with previous ocular surgery or trauma, corneal dystrophies, pseudo exfoliation syndrome, zonulopathy, low baseline endothelial cell count (ECC), poorly dilating pupil of size less than 6.5 mm, and inability to come for follow-up were excluded from the surgery.
The chopper shield technique was performed in 48 eyes of 44 patients between July 2018 and March 2020. One patient had transient diffuse corneal edema because of conversion to manual small incision cataract surgery (MSICS), and the second patient had posterior capsule rupture. Intraoperative cumulative dissipated energy (CDE) was recorded. The postoperative outcome measures were corneal edema on day one, central corneal thickness (CCT) assessed at one day, one week, and one month, and ECC assessed at three months.
Surgery was performed under topical anesthesia using proparacaine eye drops and complete aseptic precautions. A large capsulorhexis measuring about 5.5 mm was fashioned with a capsulorhexis forceps following trypan blue staining. A combination of sodium hyaluronate 3% w/v with chondroitin sulphate 4% w/v (Auro Laboratories Limited, India) was used as OVD. The Centurion phacoemulsification system (Alcon, Fort Worth, TX, USA) was used for the surgery with a balanced tip and power at 75% in the longitudinal mode, vacuum of 650 mmHg and an aspiration flow rate of 42 cc/min for the chopping maneuvers. Vertical chopping was used to achieve nuclear disassembly into smaller fragments with complete separation between individual fragments. After chopping, individual fragments were mobilized and brought in the central area and emulsified at 90% power in torsion mode with 600 mmHg vacuum and aspiration flow rate of 50 cc/min. The chopper was placed between phaco needle and posterior surface of cornea, creating a mechanical barrier between the nuclear fragments and the corneal endothelium. Surgical technique (Video 1):
The appropriate placement of the chopper between the phaco tip and the corneal endothelium prevented the chattering nuclear fragments from bouncing upwards and striking the endothelium (Figure 1). The chopper was intermittently used to rotate the nucleus and maneuver the fragments towards the phaco tip while it maintained the protective scaffolding function above the phaco needle during actual emulsification. Once emulsification was complete, routine irrigation and aspiration of the residual cortex was completed and a foldable, single piece, Tecnis 1 monofocal IOL (Model no ZCB00, Johnson and Johnson Vision) was implanted in the bag and the wounds sealed with stromal hydration.
 |
Figure 1 Chopper shield: parts of the chopper such as the tip, shaft-tip junction, and the shaft lie horizontally shielding the endothelium from nuclear fragments during emulsification. |
Results
Phacoemulsification surgery using the chopper shield technique was performed in 48 eyes of 44 patients between July 2018 and March 2020 having grade 4 or grade 5 nuclear sclerosis. Two patients were excluded from the study. One patient in the study had transient diffuse corneal edema because conversion to MSICS was done, and the second patient had posterior capsule rupture. Of the 48 eyes included in the study, 23 were males and 25 were females with a mean age of 70.02±5.98 years.. CDE was 34.16±3.18% seconds. Preoperatively, mean CCT was 529.62±21.70 microns and ECC was 2258±182.22 cells per mm2.
Postoperatively on day one, the CCT increased to 563.93±24.53 microns, a 6.47% increase from preoperative central corneal thickness. The CCT became 534.83±22.64 microns on a postoperative day seven, a 0.98% increase from preoperative CCT. The endothelial cell loss was 6.77% evaluated postoperatively at three months from the day of surgery. The median endothelial cell loss was 6.49%,the range of endothelial loss was 4–16.23%, and the interquartile range of endothelial cell loss was 1.23% (Figure 2). The two patients who had endothelial cell loss in excess of 15% involved conversion to MSICS in one patient and posterior capsule rupture in the second patient.
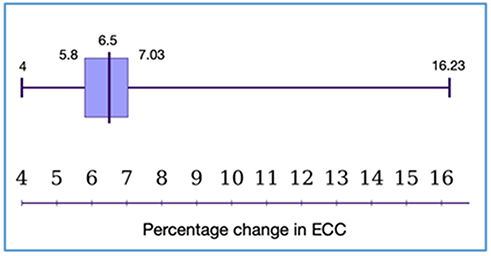 |
Figure 2 Box and whisker plot showing percentage change in endothelial cell count. |
Discussion
Phacoemulsification surgery in rock hard cataracts is associated with high propensity to corneal endothelial cell damage because of prolonged phaco time, high phaco energy, and mechanical contact by hard nuclear fragments.1,21 Surgeons employ various ultrasound power delivery modulations, innovative phaco tips, use deeper plane phacoemulsification of nuclear fragments and coat corneal endothelium with viscodispersive OVDs to protect corneal endothelium.6,8–11,14,18,21 However, the rigid and irregular nuclear fragments do not mold well at the phaco tip leading to a much greater chatter and poor followability. In addition, high fluidic use during phacoemulsification predisposes increased chatter. The resultant turbulence in the anterior chamber along with chatter leads to small or large fragments with sharp edges being dislodged from the phaco tip and striking the corneal endothelial surface. Repeated mechanical trauma to the endothelium along with the collateral damage caused by the high ultrasound energy itself increases the risk of endothelial decompensation and development of bullous keratopathy in these eyes.22
Our technique where the chopper is used as a protective shield during nuclear fragment removal offers a highly potent mechanical barrier and protects the corneal endothelium. In our technique, the large distance between the emulsification plane and the corneal endothelium facilitated an easy atraumatic placement of the chopper away from the corneal endothelium. During the emulsification the chattering occurs of the totally separated small nuclear nuclear fragments and tiny swirling fragments. We repositioned the chopper continuously, anterior to the nuclear fragments between the phaco tip and the corneal endothelium. The anteriorly bouncing nuclear fragments are kept close to the phaco tip by the closely placed chopper shield. The close proximity of the chopper shield with the phaco tip, along with slow nuclear emulsification and deeper plane of emulsification, does not allow unrestricted anterior propagation of the chattering nuclear fragments. The strategic positioning of the chopper provides a manual barrier to the chattering and mobile nuclear fragments by remarkably preventing the upward movement of sharp-edged fragments, thereby minimizing mechanical trauma to the endothelium. While the chopper shield prevents mechanical trauma, it does not advocate the prevention of damage due to ultrasound energy. Posterior capsular protection in phacoemulsification of hard nuclear fragments is not compromised while using the chopper as a shield in a high fluidic environment in the postocclusion phase. In the initial stages of nuclear emulsification, the nuclear mass provides posterior capsular protection. Prior to emulsifying the last nuclear fragment, the posterior capsule is protected by refilling capsular the bag with an OVD, slow pacing of emulsification, lowering of fluid parameters, and the slightly anterior direction of the phaco tip.
The prechopping techniques including the miLOOP (Carl Zeiss Meditec, Dublin, USA) technique fragment the hard nucleus into smaller fragments, thereby reducing the phaco time and energy used.23 However, there are challenges involved in fragmenting the brunescent nucleus into six or eight smaller fragments. Furthermore, the movement of large nuclear fragments in the anterior chamber to cause mechanical trauma to the corneal endothelium still continues.
Amir-Asgari et al have described that tiny swirling fragments had a significant role in endothelial insult.24 Presently, to prevent corneal endothelium during hard nuclear cataract emulsification, the tiny swirling fragments are inhibited from hitting the corneal endothelium by performing a slow, deeper plane of emulsification, and repeated coating of corneal endothelium by dispersive OVD. The use of the chopper as a shield provides additional protection to the corneal endothelium in hard cataracts when we compare it to the previous studies.
The femtosecond laser helps in partial fragmentation and softening, thereby decreasing phaco time and energy compared to the manual technique. However, while doing the nuclear emulsification no barrier exists between the nuclear fragments and the corneal endothelium. Our initial experience has yielded pristine clear corneas in the immediate postoperative period and endothelial cell loss of approximately 6% at the end of three months which is comparable to the endothelial cell loss associated with femtosecond laser-assisted cataract surgery. The change in CCT on day one in our study was less than the conventional phaco in the hard cataracts but comparable to the corresponding FLACS studies.25
In conclusion, we describe a simple technique that is very easy to adopt and helps protect the corneal endothelium during phacoemulsification in rock hard cataracts. In our technique, we use a thin chopper that does not obscure the vision of the surgical field at any point in time. This simple step that can be easily incorporated by the surgeon for safe phacoemulsification of rock hard cataracts.
What is known?
What this paper adds?
Funding
No funding was provided for this study.
Disclosure
Presented at
- American Society of Cataract & Refractive Surgery (Virtual Meeting) May 16–17, 2020.
- American Academy of Ophthalmology virtual conference, 2020.
No financial interest or benefit has arisen from the direct applications of this research. The authors report no conflicts of interest in this work.
References
1. Foster GJL, Allen QB, Ayres BD, et al. Phacoemulsification of the rock-hard dense nuclear cataract: options and recommendations. J Cataract Refract Surg. 2018;44(7):905–916. doi:10.1016/j.jcrs.2018.03.038
2. Hwang HB, Lyu B, Yim HB, Lee NY. Endothelial cell loss after phacoemulsification according to different anterior chamber depths. J Ophthalmol. 2015;2015:210716. doi:10.1155/2015/210716
3. Yi DH, Reza Dana M. Corneal edema after cataract surgery: incidence and etiology. Semin Ophthalmol. 2002;17(3–4):
4. Chen G, Wang D, Du Y, Huang H. Effect of continuous ultrasonic phacoemulsification with anterior chamber maintainer on corneal endothelial damage in hard nuclear cataract. Eur J Ophthalmol. 2015;25(3):198–201. doi:10.5301/ejo.5000537
5. Vanathi M, Vajpayee RB, Tandon R, Titiyal JS, Gupta V. Crater-and-chop technique for phacoemulsification of hard cataracts. J Cataract Refract Surg. 2001;27(5):659. doi:10.1016/S0886-3350(00)00702-1
6. Park J, Yum HR, Kim MS, Harrison AR, Kim EC. Comparison of phaco-chop, divide-and-conquer, and stop-and-chop phaco techniques in microincision coaxial cataract surgery. J Cataract Refract Surg. 2013;39(10):1463–1469. doi:10.1016/j.jcrs.2013.04.033
7. Vajpayee RB, Kumar A, Dada T, Titiyal JS, Sharma N, Dada VK. Phaco-chop versus stop-and-chop nucleotomy for phacoemulsification. J Cataract Refract Surg. 2000;26(11):1638–1641. doi:10.1016/S0886-3350(00)00544-7
8. Chen D, Tang Q, Yu F, Cai X, Lu F. Consecutive drilling combined with phaco chop for full thickness segmentation of very hard nucleus in coaxial microincisional cataract surgery. BMC Ophthalmol. 2019;19(1):20. doi:10.1186/s12886-019-1033-1
9. Falabella P, Yogi MS, Teixeira A, Jopetibe F, Sartori J, Schor P. Retrochop technique for rock-hard cataracts. J Cataract Refract Surg. 2013;39(6):826–829. doi:10.1016/j.jcrs.2013.03.015
10. Kim DY, Jang JH. Drill and chop: modified vertical chop technique for hard cataract. Ophthalmic Surg Lasers Imaging. 2012;43(2):169–172. doi:10.3928/15428877-20111222-01
11. Chang DF. Phaco Chop: Mastering Techniques, Optimizing Technology, and Avoiding Complications. Thorofare, NJ: SLACK Incorporated; 2004.
12. Yang W-J, Wang X-H, Zhao F, Mei Z-M, Li S, Xiang Y. Torsional and burst mode phacoemulsification for patients with hard nuclear cataract: a Randomized Control Study. Medicine (Baltimore). 2019;98(22):e15870. doi:10.1097/MD.0000000000015870
13. Davison JA. Results of endocapsular phacofracture debulking of hard cataracts. Clin Ophthalmol. 2015;9:1233–1238. doi:10.2147/OPTH.S85939
14. Wan W, Jiang L, Ji Y, et al. Effect of hypothermic perfusion on phacoemulsification in eyes with hard nuclear cataract: randomized trial. J Cataract Refract Surg. 2019;45(12):1717–1724. doi:10.1016/j.jcrs.2019.07.029
15. Li X, He Y, Su T, et al. Comparison of clinical outcomes between cystotome-assisted prechop phacoemulsification surgery and conventional phacoemulsification surgery for hard nucleus cataracts: a CONSORT-compliant article. Medicine (Baltimore). 2018;97(46):e13124. doi:10.1097/MD.0000000000013124
16. Zhao Y, Yang K, Li J, Zhu S. Comparison between the prechopping method with a reverse chopper and the routine stop-and-chop method in treating cataract with grade IV hard nucleus. J Fr Ophtalmol. 2018;41(4):315–320. doi:10.1016/j.jfo.2017.11.011
17. Chang DF. Strategies for handling the hard nucleus. In: Boyd S, editor. New Outcomes in Cataract Surgery. Panama: Highlights of Ophthalmology; 2005.
18. O’Brien PD, Fitzpatrick P, Kilmartin DJ, Beatty S. Risk factor for endothelial cell loss after phacoemulsification surgery by a junior resident. J Cataract Refract Surg. 2004;30(4):839–843. PMID: 15093647. doi:10.1016/S0886-3350(03)00648-5
19. Ganekal S, Nagarajappa A. Comparison of morphological and functional endothelial cell changes after cataract surgery: phacoemulsification versus manual small-incision cataract surgery. Middle East Afr J Ophthalmol. 2014;21(1):56–60. PMID: 24669147. doi:10.4103/0974-9233.124098
20. Maggon R, Bhattacharjee R, Shankar S, Kar RC, Sharma V, Roy S. Comparative analysis of endothelial cell loss following phacoemulsification in pupils of different sizes. Indian J Ophthalmol. 2017;65(12):
21. Khokhar S, Aron N, Sen S, Agarwal E, Agarwal E. Effect of balanced phacoemulsification tip on the outcomes of torsional phacoemulsification using an active-fluidics system. J Cataract Refract Surg. 2017;43(1):22–28. doi:10.1016/j.jcrs.2016.11.034
22. Pricopie S, Istrate S, Voinea L, Leasu C, Paun V, Radu C. Pseudophakic bullous keratopathy. Rom J Ophthalmol. 2017;61(2):
23. Ianchulev T, Chang DF, Koo E, MacDonald S, Calvo E, Tyson FT. A microinterventional endocapsular nucleus disassembly: novel technique and results of first-in-human randomised controlled study. Br J Ophthalmol. 2019;103(2):176–180. doi:10.1136/bjophthalmol-2017-311766
24. Amir-Asgari S, Hirnschall N, Findl O. Using continuous intraoperative optical coherence tomography to classify swirling lens fragments during cataract surgery and to predict their impact on corneal endothelial cell damage. J Cataract Refract Surg. 2016;42(7):1029–1036. doi:10.1016/j.jcrs.2016.04.029
25. Chen X, Yu Y, Song X, Zhu Y, Wang W, Yao K. Clinical outcomes of femtosecond laser-assisted cataract surgery versus conventional phacoemulsification surgery for hard nuclear cataracts. J Cataract Refract Surg. 2017;43(4):486–491. doi:10.1016/j.jcrs.2017.01.010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.