Back to Journals » International Journal of Women's Health » Volume 17
Choline Intake and Pelvic Inflammatory Disease Risk: A Cross-Sectional Study Based on NHANES 2013–2018
Received 3 July 2025
Accepted for publication 26 September 2025
Published 6 October 2025 Volume 2025:17 Pages 3499—3509
DOI https://doi.org/10.2147/IJWH.S551450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Hongyu Jin,1 Zhaoyuan Niu,2 Xinyue Zhao1
1Department of Gynecology, Qingdao University Hospital, Qingdao University School of Medicine, Qingdao, People’s Republic of China; 2Department of Gynecology, Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China
Correspondence: Zhaoyuan Niu, Email [email protected]
Background and Aim: Pelvic inflammatory disease (PID), a chronic infection of the female upper genital tract, is a leading cause of morbidity in reproductive-aged women, often resulting in chronic pelvic pain, tubal infertility, and ectopic pregnancy. Choline, an essential nutrient, plays a critical role in various metabolic processes and is known to modulate inflammatory pathways. However, the potential link between dietary choline intake and PID remains largely unexplored. This study aimed to investigate the relationship between dietary choline consumption and PID prevalence.
Methods: We analyzed data from the National Health and Nutrition Examination Survey (NHANES) 2013– 2018. A total of 3204 women were included in the analysis. The association between choline intake and PID was assessed using multivariable logistic regression and smooth curve fitting. Subgroup analyses were performed to explore potential effect modifiers, and threshold effect analysis was used to identify inflection points in the relationship.
Results: Among the 3204 women studied, 208 had PID. In fully adjusted models, higher choline intake was significantly associated with a reduced risk of PID (OR = 0.20, 95% CI: 0.04– 0.92, p = 0.038). Compared to women in the lowest quintile of choline intake, those in the highest quintile had a 45% lower risk of PID (OR = 0.55, 95% CI: 0.30– 0.98, p = 0.044). Smooth curve fitting demonstrated a nonlinear association, with an inflection point at 0.41 g/day overall and at 0.29 g/day for normotensive women. Subgroup analysis suggested that blood pressure status may modify this relationship.
Conclusion: Higher dietary choline intake was associated with a reduced prevalence of PID. These findings highlight the potential role of nutritional factors, particularly adequate choline intake, in reproductive health and support further prospective research to confirm causality.
Keywords: dietary choline intake, pelvic inflammatory disease, NHANES, cross-sectional study
Introduction
PID is a common infectious disorder of the female reproductive system,1 primarily caused by ascending pathogens such as Neisseria gonorrhoeae and Chlamydia trachomatis,2,3 often secondary to untreated sexually transmitted infections or vaginal microbiota imbalance.4–6 The clinical manifestations vary widely, ranging from asymptomatic to severe symptoms including lower abdominal pain, fever, abnormal vaginal discharge, and dyspareunia.7,8 Serious side effects include ectopic pregnancy, chronic pelvic pain, and tubal factor infertility could result from PID if treatment is delayed,9,10 imposing a dual burden on both reproductive health and psychological well-being in women.
Mounting evidence from recent epidemiological investigations has elucidated the substantial impact of nutritional and lifestyle factors on female reproductive health. Contemporary research has specifically identified tobacco use, alcohol consumption patterns, and dietary caffeine exposure as key modifiable risk factors influencing reproductive health trajectories.11 Research suggests that specific dietary patterns or nutrient intake may affect female reproductive health: ketogenic diets may regulate ovarian function in women with polycystic ovary syndrome (PCOS),12 dietary fiber intake is negatively associated with infertility risk,13 and vitamin B6 may reduce the risk of endometriosis.14 The role of nutritional factors in inflammation and immune regulation is also increasingly recognized. Studies have found that certain dietary nutrients have both acute and long-term regulatory effects on inflammation.15 Choline, as an essential nutrient with a recommended daily intake of 0.425 g/day for women, is crucial for methylation support, neurotransmitter synthesis, and cell membrane integrity.16–18 Additionally, it plays a key role in inflammation and immune regulation.19 Its metabolites (such as acetylcholine and betaine) can modulate macrophage activation and cytokine secretion, influencing the host’s immune response to infections.20,21 The relationship between choline consumption and PID susceptibility and clinical outcomes has yet to be fully elucidated.
Based on data from NHANES 2013–2018, this study intends to investigate the association between choline consumption and PID, while exploring potential mechanisms through which choline may influence PID pathogenesis by modulating immune microenvironments or the gut microbiota-reproductive tract axis. The findings may provide novel scientific evidence for PID prevention and nutritional intervention strategies.
Methods
Research Design and Subjects
This study analyzed data from the 2013–2018 NHANES, a nationally representative cross-sectional assessment of health and nutritional status conducted by the CDC’s National Center for Health Statistics (NCHS). NHANES employs standardized interviews, physical examinations, and laboratory tests, with all participants providing written informed consent.
The initial sample comprised 29,400 individuals across three survey cycles. Exclusion criteria were applied sequentially: participants with missing PID data (n = 29,008) or incomplete dietary records (n = 852) were first removed. Further exclusions were made for missing covariate data, including education level (n = 346), poverty-income ratio (n = 340), body mass index (n = 20), hypertension status (n = 2), and vigorous physical activity (n = 1). After these exclusions, the final analytical sample consisted of 3204 participants (Figure 1).
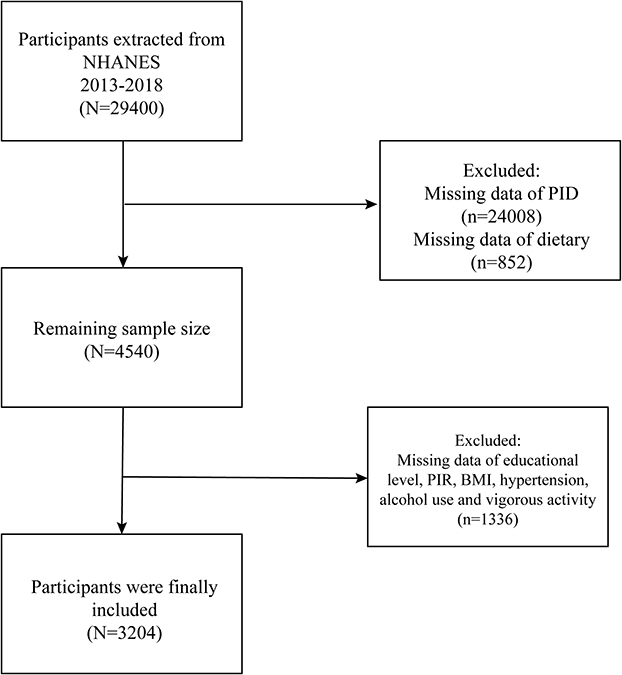 |
Figure 1 Flow chart for participant inclusion and exclusion. Abbreviations: NHANES, National Health and Nutrition Examination Survey; PID, pelvic inflammatory disease; PIR, poverty income ratio; BMI, body mass index. |
Assessment of Choline Intake
Choline intake was assessed using two 24-hour dietary recall interviews. The first interview was conducted in person at the Mobile Examination Centers (MEC), followed by a telephone interview 3–10 days later. The average of both recalls was used to estimate total choline intake.22,23 The choline intake assessed in this study was limited to dietary sources and excluded intake from supplements.
Assessment of Pelvic Inflammatory Disease
We diagnosed PID through self-reported responses to the reproductive health questionnaire (variable name: RHQ078). In the survey, researchers asked participants whether they had ever received treatment for PID, with the question: “Have you ever received treatment for PID?” If participants answered “yes”, it indicated a past PID infection. This diagnostic approach has been previously validated for reliability.24,25
Covariates
The analysis adjusted for: demographic characteristics (age, race, education, marital status), socioeconomic indicators [poverty income ratio (PIR)], clinical measures [body mass index (BMI), hypertension], lifestyle factors (alcohol use, vigorous activity), and reproductive health characteristics (regular period). Variance inflation factor (VIF) analysis confirmed all covariates had VIF < 10, indicating no multicollinearity concerns.
Statistical Analysis
Data normality was assessed using the Shapiro–Wilk test prior to applying parametric methods. Normally distributed continuous variables are presented as mean ± standard error (SE) and compared with t tests, while non-normal variables are summarized as median (interquartile range, IQR) and compared with Mann–Whitney U-tests. Categorical variables are expressed as n (%) and compared with chi-square tests.
Associations between dietary choline intake and PID were evaluated using multivariable logistic regression, treating choline both as a continuous variable and in quintiles, with results reported as odds ratios (ORs) and 95% confidence intervals (CIs). Three models were constructed: Model 1 (unadjusted); Model 2 (adjusted for age, race, education, and marital status); and Model 3 (further adjusted for PIR, BMI, hypertension, alcohol use, vigorous activity, regular period, and dietary energy intake). Nonlinearity was examined using restricted cubic splines, and potential thresholds were explored using piecewise logistic models. Prespecified subgroup analyses were performed with multiplicative interaction terms. As an additional analysis within hypertensive participants, we stratified by current antihypertensive medication use and formally tested the choline × medication interaction. All analyses were performed using R (version 4.2) and EmpowerStats (version 4.2). A two-sided p < 0.05 was considered statistically significant.
Results
Baseline Characteristics of Participants
Table 1 presents demographic and clinical characteristics of the study population. The final analytical cohort comprised 3204 participants aged 20–59 years (mean age 39.76 ± 11.43 years), including 208 PID cases and 2996 controls. The PID patients were older on average, had a higher percentage of non-Hispanic White people, and had a higher BMI than the non - PID group. However, they consumed less total energy and dietary choline.
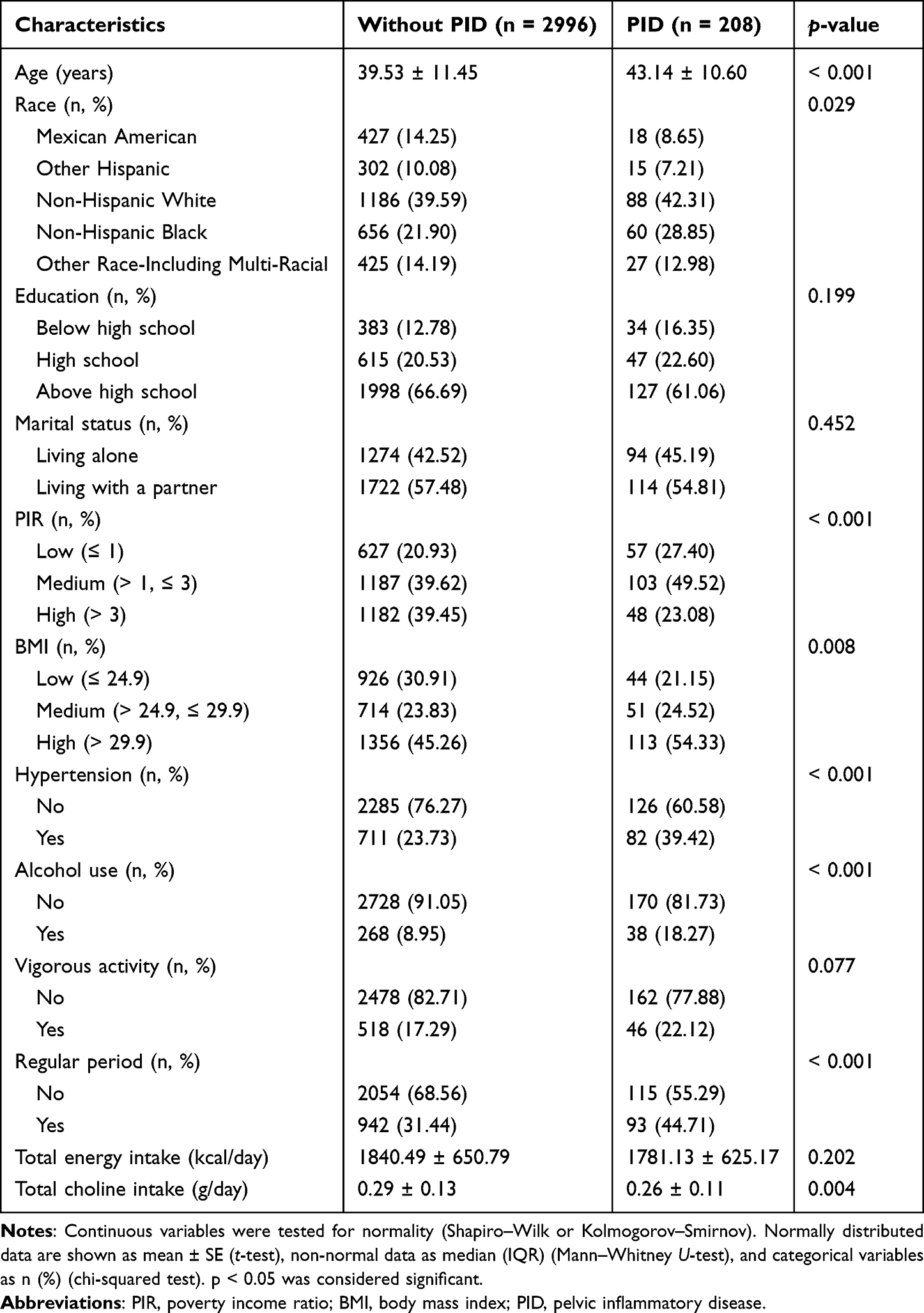 |
Table 1 Demographic and Clinical Characteristics Stratified by Pelvic Inflammatory Disease Status |
Relationships Between Dietary Choline and PID
Multivariable logistic regression analysis was performed to examine the association between choline intake and PID (Table 2). When treated as a continuous variable, choline intake was consistently associated with a lower risk of PID across all models. The odds ratios (OR) for Models 1, 2, and 3 were 0.17 (95% CI: 0.05–0.57), 0.24 (95% CI: 0.07–0.79), and 0.20 (95% CI: 0.04–0.92), respectively, indicating that higher choline consumption was inversely related to PID risk. Each 1 g/day increase in choline intake was associated with a significant reduction in PID prevalence. Smoothing curve fitting revealed a nonlinear relationship between choline intake and PID (Figure 2). In the quintile analysis, after full adjustment, women in the highest quintile (Q5) had a 45% lower risk of PID compared with those in the lowest quintile (Q1) (OR = 0.55, 95% CI: 0.30–0.98, p = 0.044).
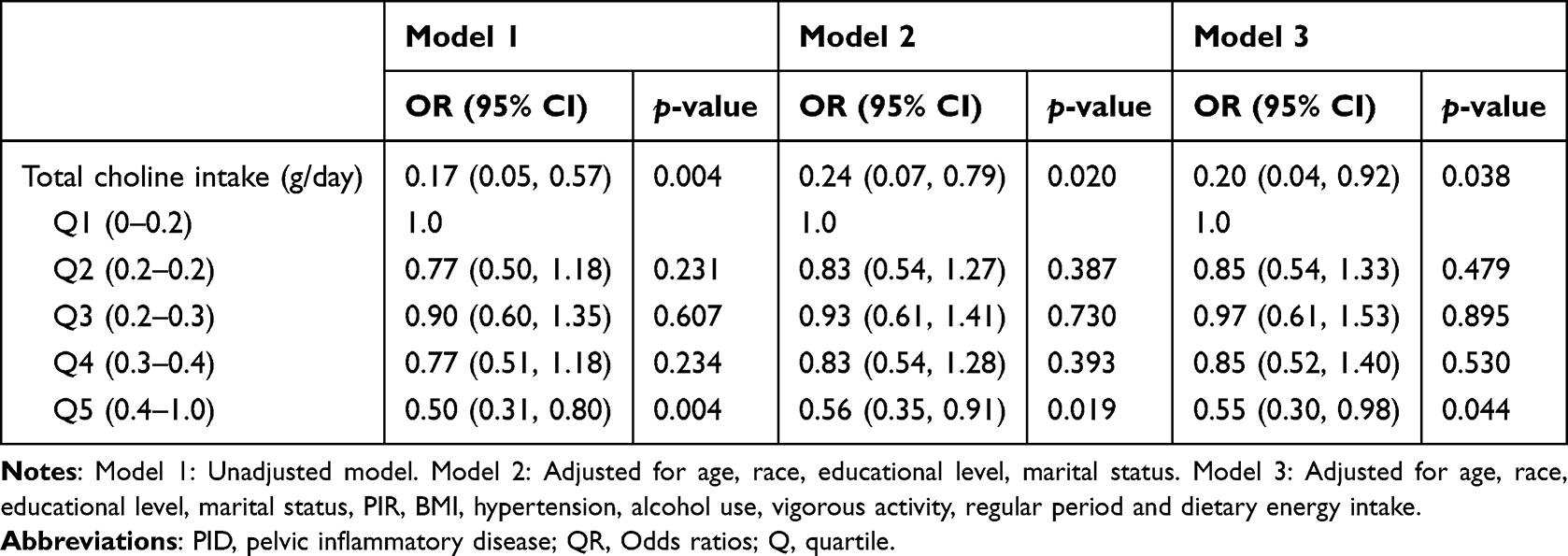 |
Table 2 Logistic Regression Analysis of the Association Between Choline and PID |
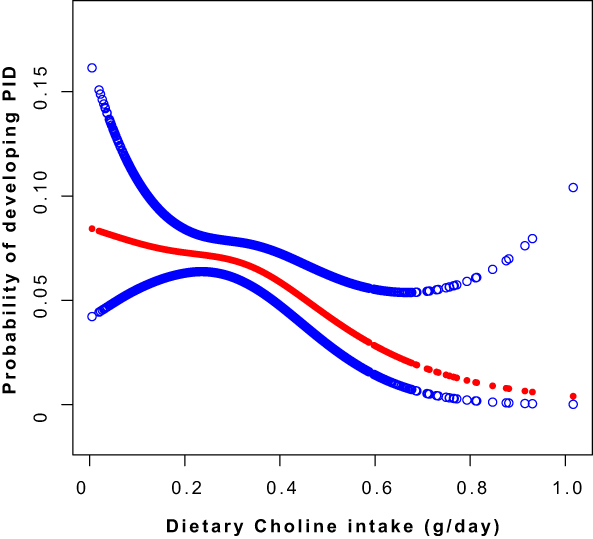 |
Figure 2 Smooth curve fitting between dietary choline intake and PID. The association between dietary choline intake and the probability of PID was modeled using restricted cubic spline regression. The red solid line represents the adjusted probability of PID, and the blue bands represent the 95% confidence intervals (CIs). The Y-axis displays the probability on a logarithmic scale, while the X-axis shows dietary choline intake (g/day). The model was adjusted for age, race, BMI, PIR, educational level, marital status, hypertension, alcohol use, vigorous activity, regular period, and dietary energy intake. Abbreviations: PID, pelvic inflammatory disease; PIR, poverty income ratio; BMI, body mass index. |
Subgroup Analysis
We conducted subgroup analyses and tested interactions across demographic and behavioral characteristics (Table 3). A significant interaction by hypertension status was observed (p for interaction < 0.05). Among participants with hypertension, higher choline intake was associated with lower odds of PID (OR = 0.03, 95% CI: 0.00–0.35); among those without hypertension, the association was weaker and not statistically significant (OR = 0.46, 95% CI: 0.08–2.54). Stratified restricted cubic spline analyses further suggested a non-linear association in non-hypertensive participants (Figure 3).
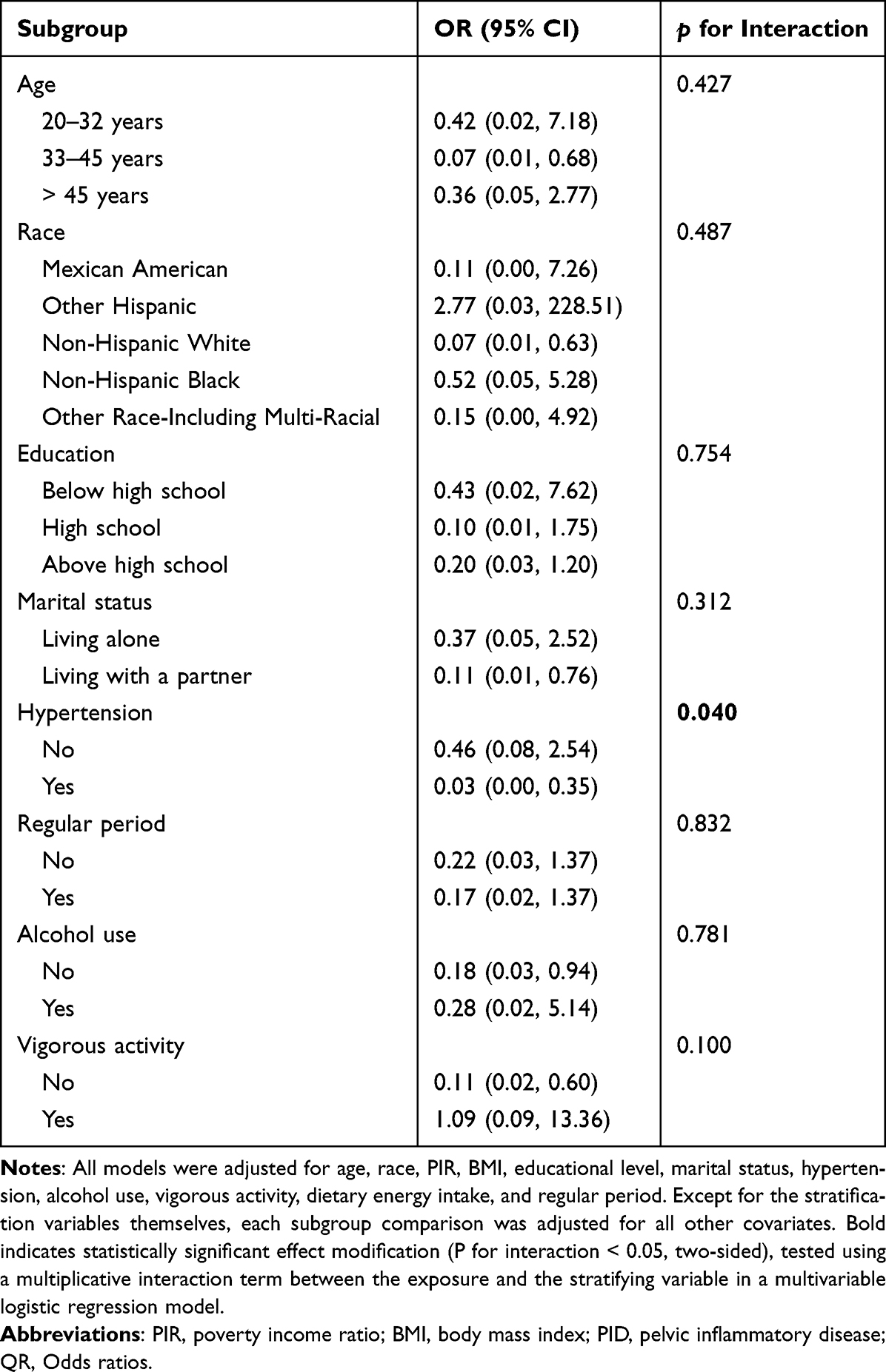 |
Table 3 Subgroup Analysis of the Relationship Between Dietary Choline Intake and PID |
 |
Figure 3 Smooth curve fitting of dietary choline intake in relation to PID stratified by hypertension status. The association between dietary choline intake and the probability of developing pelvic inflammatory disease (PID) stratified by hypertension status, modeled using restricted cubic spline regression. The blue solid line represents participants with hypertension, and the red solid line represents those without hypertension. The Y-axis displays the probability on a logarithmic scale, and the X-axis shows dietary choline intake (g/day). The model was adjusted for age, race, BMI, PIR, educational level, marital status, alcohol use, vigorous activity, regular period, and dietary energy intake. Abbreviations: PID, pelvic inflammatory disease; PIR, poverty income ratio; BMI, body mass index. |
Additional Analysis in Hypertensive Participants
Among hypertensive participants, we conducted a stratified analysis according to current antihypertensive medication use (BPQ050A: “Now taking prescribed medicine for HBP”) and formally tested the choline × medication interaction. Of the hypertensive subgroup, 496 women reported current use of antihypertensive medication, 159 reported no use, and 138 had missing data. The stratified results were directionally consistent with the main analyses, and the interaction term was not statistically significant (p for interaction > 0.05). These findings suggest that antihypertensive medication use did not materially modify the observed association between choline intake and PID (Table 4).
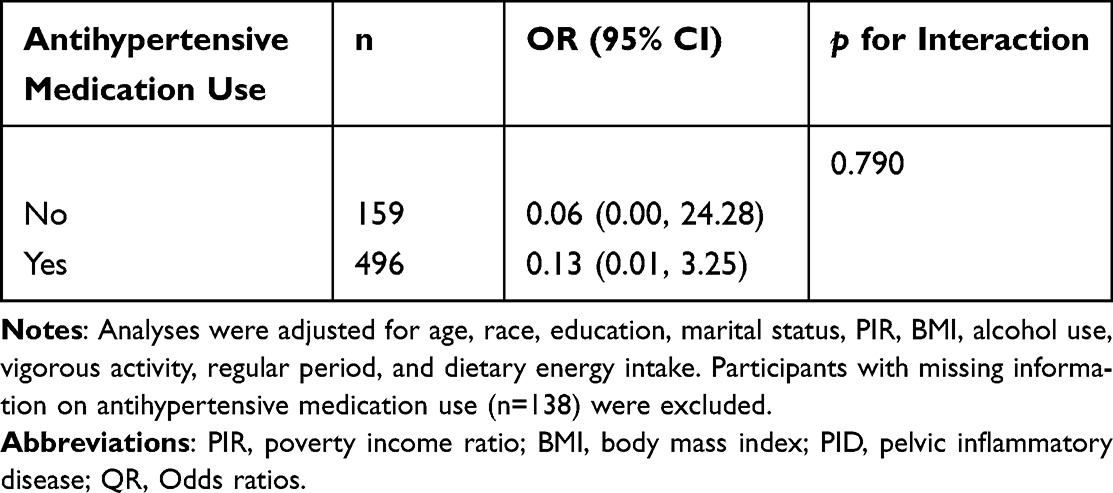 |
Table 4 Association Between Dietary Choline Intake and PID Among Hypertensive Participants, Stratified by Antihypertensive Medication Use |
Threshold Effect Analysis
Threshold analysis indicated a piecewise (threshold) relationship between choline intake and the odds of PID (Table 5). The overall model identified a threshold at 0.41 g/day (likelihood-ratio test, p = 0.026). Below this threshold, the association was not statistically significant (per 0.1 g/day increase: OR = 0.73, 95% CI: 0.10–5.18; p = 0.755). Above the threshold, higher intake was associated with a substantial decrease in the odds of PID (per 0.1 g/day increase: OR ≈ <0.01, 95% CI: <0.01–0.31; p = 0.019).
 |
Table 5 Analysis of Threshold and Saturation Effects Between Dietary Choline Intake and PID |
Hypertension-stratified analyses (Table 6) suggested a lower threshold among non-hypertensive participants (0.29 g/day; likelihood-ratio test, p = 0.014). In this subgroup, choline showed no significant association at intakes below 0.29 g/day (OR = 16.87, 95% CI: 0.40–713.20; p = 0.139), whereas at or above the threshold, a stronger protective association was observed (OR = 0.02, 95% CI: <0.01–0.52; p = 0.018), suggesting that a minimum intake level may be required before a preventive effect is evident.
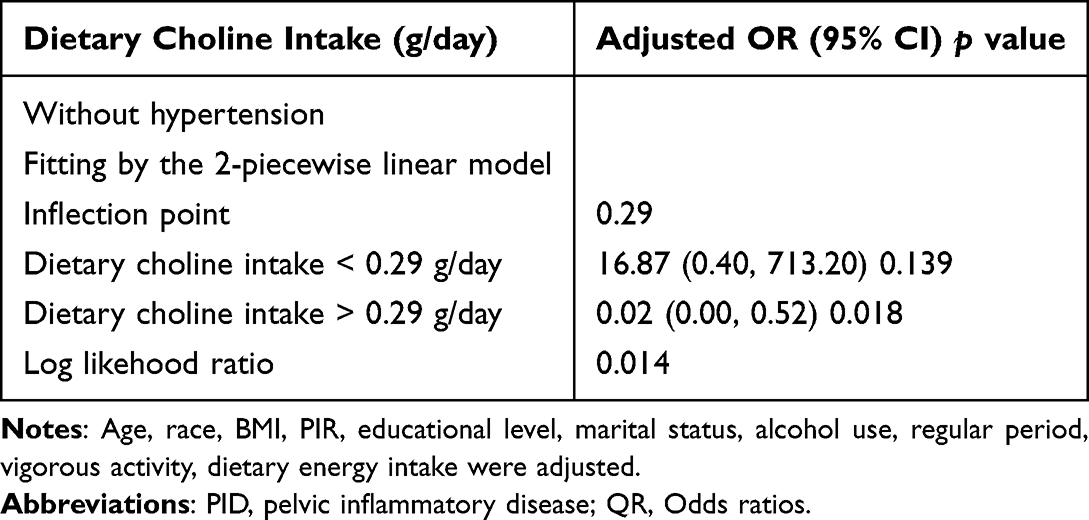 |
Table 6 Threshold Effect Analysis of Choline Intake (g/Day) on PID Using the Two-Piecewise Linear Regression Model |
Discussion
Multivariable-adjusted logistic regression revealed a significant inverse association between dietary choline consumption and PID risk (p < 0.05), which persisted after comprehensive covariate adjustment. The results from the smooth curve fitting further validated this negative relationship. Notably, blood pressure status emerged as a significant effect modifier (interaction p < 0.05), with distinct patterns observed between hypertensive and non-hypertensive subgroups. The smooth curve fitting results stratified by blood pressure revealed a threshold-like (piecewise) relationship between the two in the non-hypertensive population. Threshold analysis determined an overall choline intake inflection point at 0.41 g/day, with normotensive subjects showing a lower threshold of 0.29 g/day.
This groundbreaking study establishes the first evidence base for the choline - PID relationship, an association never before examined in epidemiological or mechanistic research. Therefore, we attempt to review and analyze the existing literature to explain the possible mechanisms. Choline, as a precursor of anti-inflammatory metabolites such as acetylcholine, may reduce the release of pro-inflammatory cytokines (eg, TNF-α, IL-6) through cholinergic anti-inflammatory pathways, including the vagus nerve–immune regulatory axis, thereby lowering the risk of pelvic inflammatory disease (PID).26–28 In daily diets, eggs, red meat, milk, and cheese are among the richest sources of choline.29 Previous studies have shown that individuals with higher intakes of choline and betaine tend to have lower levels of inflammatory markers, such as C-reactive protein, homocysteine, IL-6, and TNF-α.17 Animal experiments have also confirmed that a high-choline diet can reduce inflammatory damage in mice with bacterial peritonitis.30 Furthermore, acetylcholine can activate the nAChR/ERK pathway to promote the secretion of IL-10 from monocytic-derived suppressive granulocytes (M-MDSCs), thus inhibiting inflammation.31 The choline metabolite betaine can enhance the expression of intestinal tight junction proteins and inhibit inflammatory pathways, directly protecting the intestinal mucosal barrier function.32 At the same time, betaine increases the abundance of beneficial gut microbiota (such as bifidobacteria and lactobacilli),33,34 while choline deficiency may lead to intestinal barrier disruption and dysbiosis.35,36 These mechanisms may collectively contribute to intestinal immune dysregulation, potentially serving as underlying triggers or aggravating factors for PID.
Our findings further suggest that blood pressure status may modify the association between choline intake and PID. Among hypertensive individuals, higher choline consumption was associated with markedly lower odds of PID (OR = 0.03, 95% CI: 0.00–0.35). A plausible explanation is that choline’s anti-inflammatory properties may alleviate hypertension-related chronic low-grade inflammation and endothelial dysfunction.37–40 In contrast, non-hypertensive participants exhibited a nonlinear dose–response relationship, with significant risk reduction only when choline intake exceeded the threshold of 0.29 g/day, suggesting a minimum requirement for protective effects. To further examine the potential influence of medication, an additional sensitivity analysis restricted to hypertensive participants and stratified by current antihypertensive use (BPQ050A) found no significant interaction, with directionally consistent estimates across strata. These findings suggest that the observed association is unlikely to be driven by medication use.
This study presents several notable strengths. First, the use of a large, nationally representative sample from the NHANES database (n = 3204) enhances the generalizability and statistical power of the findings. Second, the application of multivariable models adjusting for a wide range of demographic, lifestyle, and clinical covariates improves the robustness of the observed associations. Third, the use of restricted cubic spline models and subgroup analyses allows for a more comprehensive exploration of potential nonlinear relationships and effect modifications.
Several limitations should be acknowledged. First, the cross-sectional design limits causal inference between dietary choline intake and PID. Second, residual confounding cannot be excluded due to unmeasured factors such as genetic predisposition, detailed sexual behaviors, and environmental exposures. Third, both choline intake and PID status were self-reported, which may introduce recall bias and misclassification despite standardized questionnaires; moreover, NHANES does not collect information on PID treatment history, which could improve diagnostic accuracy. Fourth, laboratory biomarkers (eg, plasma choline, TNF-α, IL-6) were unavailable in these survey cycles, precluding direct assessment of anti-inflammatory pathways. Fifth, dietary data were obtained from two 24-hour recalls and did not capture choline from dietary supplements, potentially underestimating total exposure and failing to fully reflect habitual intake. Sixth, although NHANES collects information on prescription medication use, including antihypertensive therapy, these data are self-reported, lack details on drug class, dose, duration, and adherence, and contain substantial missing values. To avoid overstratification, antihypertensive medication was not included in the primary models. In a hypertension-restricted additional analysis stratified by current medication use (BPQ050A), the interaction was not statistically significant and estimates were directionally consistent with the main results; nonetheless, class-specific drug effects and residual confounding cannot be entirely excluded. Finally, as NHANES represents the US noninstitutionalized population, generalizability to other settings with different dietary patterns and health-care access may be limited. Prospective studies with detailed biomarker and medication data are warranted to validate these associations and clarify causal mechanisms.
Conclusion
Higher dietary choline intake (> 0.41 g/day) was associated with a lower prevalence of PID, suggesting that adequate choline consumption may contribute to prevention in women at risk. Given the limitations of this cross-sectional design, these findings should be interpreted with caution, and prospective studies are needed to confirm causality and elucidate underlying mechanisms.
Abbreviations
PID, Pelvic inflammatory disease; PCOS, Polycystic Ovary Syndrome; NHANES, National Health and Nutrition Examination Survey; NCHS, National Center for Health Statistics; CDC, Centers for Disease Control and Prevention; MEC, Mobile Examination Center; VIF, Variance inflation factor; PIR, Poverty income ratio; BMI, Body mass index; Q1, The lowest quintile group; Q5, The highest quintile group; OR, Odds ratios; M-MDSCs, Monocytic-derived suppressive granulocytes.
Data Sharing Statement
The survey data are publicly available at www.cdc.gov/nchs/nhanes/.
Ethical Statement
This study is a secondary analysis of publicly available, de-identified data from the National Health and Nutrition Examination Survey (NHANES) 2013–2018. All NHANES protocols are approved by the National Center for Health Statistics Research Ethics Review Board (NCHS ERB), and written informed consent is obtained from all participants. The Institutional Review Board of the Affiliated Hospital of Qingdao University determined that the present secondary analysis is exempt from further review because it uses de-identified public data. The present study was conducted in accordance with the principles of the Declaration of Helsinki. No additional informed consent was required for this analysis.
Acknowledgments
We gratefully acknowledge all study participants for their involvement.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no external funding was received for this study.
Disclosure
All authors declare that they have no competing financial interests.
References
1. Mitchell C, Prabhu M. Pelvic inflammatory disease: current concepts in pathogenesis, diagnosis and treatment. Infect Dis Clin N Am. 2013;27(4):793–809. doi:10.1016/j.idc.2013.08.004
2. Haggerty CL, Ness RB. Epidemiology, pathogenesis and treatment of pelvic inflammatory disease. Exp Rev Anti-Infective Ther. 2006;4(2):235–247. doi:10.1586/14787210.4.2.235
3. Curry A, Williams T, Penny ML. Pelvic inflammatory disease: diagnosis, management, and prevention. Am Fam Physician. 2019;100(6):357–364.
4. Greydanus DE, Cabral MD, Patel DR. Pelvic inflammatory disease in the adolescent and young adult: an update. Disease-a-Month. 2022;68(3):101287. doi:10.1016/j.disamonth.2021.101287
5. Sweet RL. Sexually transmitted diseases, Pelvic inflammatory disease and infertility in women. Infect Dis Clin N Am. 1987;1(1):199–215. doi:10.1016/S0891-5520(20)30103-3
6. Turpin R, Tuddenham S, He X, Klebanoff MA, Ghanem KG, Brotman RM. Bacterial vaginosis and behavioral factors associated with incident pelvic inflammatory disease in the longitudinal study of vaginal flora. J Infect Dis. 2021;224(12 Suppl 2):S137–s144. doi:10.1093/infdis/jiab103
7. Gradison M. Pelvic inflammatory disease. Am Fam Physician. 2012;85(8):791–796.
8. Yang SF, Wu TF, Tsai HT, Lin LY, Wang PH. New markers in pelvic inflammatory disease. Clin Chim Acta. 2014;431:118–124. doi:10.1016/j.cca.2014.02.004
9. Soper DE. Pelvic inflammatory disease. Obstetrics Gynecol. 2010;116(2 Pt 1):419–428. doi:10.1097/AOG.0b013e3181e92c54
10. Crossman SH. The challenge of pelvic inflammatory disease. Am Fam Physician. 2006;73(5):859–864.
11. Bala R, Singh V, Rajender S, Singh K. Environment, lifestyle, and female infertility. Reprod Sci. 2021;28(3):617–638. doi:10.1007/s43032-020-00279-3
12. Magagnini MC, Condorelli RA, Cimino L, et al. Does the ketogenic diet improve the quality of ovarian function in obese women? Nutrients. 2022;14(19):4147. doi:10.3390/nu14194147
13. Cai Q, Chen T. Association between dietary fiber and female fertility: a NHANES-based study. Reprod Sci. 2023;30(5):1555–1564. doi:10.1007/s43032-022-01103-w
14. Sheng J, Chen L, Yan H, Nie J. Study of the association of niacin and vitamin B6 intake with endometriosis: evidence from NHANES 2003–2006. Int J Gynecol Obstet. 2025;169(2):773–780. doi:10.1002/ijgo.16096
15. Fabozzi G, Verdone G, Allori M, et al. Personalized nutrition in the management of female infertility: new insights on chronic low-grade inflammation. Nutrients. 2022;14(9):1918. doi:10.3390/nu14091918
16. Gao Y, Mao K, Yang C, et al. The causal relationship between choline metabolites and acute acalculous cholecystitis: identifying ABCG8 as colocalized gene. Nutrients. 2024;16(21):3588. doi:10.3390/nu16213588
17. Zeisel SH, da Costa KA. Choline: an essential nutrient for public health. Nutr Rev. 2009;67(11):615–623. doi:10.1111/j.1753-4887.2009.00246.x
18. Fischer LM, daCosta KA, Kwock L, et al. Sex and menopausal status influence human dietary requirements for the nutrient choline. Am J Clin Nutr. 2007;85(5):1275–1285. doi:10.1093/ajcn/85.5.1275
19. Huang SY, Yang ZJ, Cheng J, et al. Choline alleviates cognitive impairment in sleep-deprived young mice via reducing neuroinflammation and altering phospholipidomic profile. Redox Biol. 2025;81:103578. doi:10.1016/j.redox.2025.103578
20. Sanchez-Lopez E, Zhong Z, Stubelius A, et al. Choline uptake and metabolism modulate macrophage IL-1β and IL-18 production. Cell Metab. 2019;29(6):1350–1362.e1357. doi:10.1016/j.cmet.2019.03.011
21. Snider SA, Margison KD, Ghorbani P, et al. Choline transport links macrophage phospholipid metabolism and inflammation. J Biol Chem. 2018;293(29):11600–11611. doi:10.1074/jbc.RA118.003180
22. Lin H, Zhong Z, Zhang C, Jin X, Qi X, Lian J. An inverse association of dietary choline with atherosclerotic cardiovascular disease among US adults: a cross-sectional NHANES analysis. BMC Public Health. 2024;24(1):1460. doi:10.1186/s12889-024-18837-8
23. Gong H, Jiang J, Choi S, Huang S. Sex differences in the association between dietary choline intake and total bone mineral density among adolescents aged 12–19 in the United States. Front Nutr. 2024;11:1459117. doi:10.3389/fnut.2024.1459117
24. Chen Z, Wu Z, Zhang Y. Association between dietary magnesium intake and pelvic inflammatory disease in US women: a cross-sectional study of NHANES. Front Nutr. 2024;11:1430730. doi:10.3389/fnut.2024.1430730
25. Hu P, Zhang S, Li H, Yan X, Zhang X, Zhang Q. Association between dietary trace minerals and pelvic inflammatory disease: data from the 2015–2018 National Health and Nutrition Examination Surveys. Front Nutr. 2023;10:1273509.
26. Bonaz B, Sinniger V, Pellissier S. Anti-inflammatory properties of the vagus nerve: potential therapeutic implications of vagus nerve stimulation. J Physiol. 2016;594(20):5781–5790. doi:10.1113/JP271539
27. Rosas-Ballina M, Tracey KJ. Cholinergic control of inflammation. J Internal Med. 2009;265(6):663–679. doi:10.1111/j.1365-2796.2009.02098.x
28. Uwada J, Nakazawa H, Muramatsu I, Masuoka T, Yazawa T. Role of muscarinic acetylcholine receptors in intestinal epithelial homeostasis: insights for the treatment of inflammatory bowel disease. Int J Mol Sci. 2023;24(7):6508.
29. Vallianou NG, Kounatidis D, Psallida S, et al. The interplay between dietary choline and cardiometabolic disorders: a review of current evidence. Curr Nutr Rep. 2024;13(2):152–165.
30. Luo S, Lin H, Wu C, et al. Cholinergic macrophages promote the resolution of peritoneal inflammation. Proc Natl Acad Sci USA. 2024;121(27):e2402143121. doi:10.1073/pnas.2402143121
31. Zheng W, Song H, Luo Z, et al. Acetylcholine ameliorates colitis by promoting IL-10 secretion of monocytic myeloid-derived suppressor cells through the nAChR/ERK pathway. Proc Natl Acad Sci USA. 2021;118(11).
32. Thomes PG, Osna NA, Bligh SM, Tuma DJ, Kharbanda KK. Role of defective methylation reactions in ethanol-induced dysregulation of intestinal barrier integrity. Biochem Pharmacol. 2015;96(1):30–38. doi:10.1016/j.bcp.2015.04.018
33. Du J, Zhang P, Luo J, et al. Dietary betaine prevents obesity through gut microbiota-drived microRNA-378a family. Gut Microbes. 2021;13(1):1–19.
34. Perumal SK, Arumugam MK, Osna NA, Rasineni K, Kharbanda KK. Betaine regulates the gut-liver axis: a therapeutic approach for chronic liver diseases. Front Nutr. 2025;12:1478542.
35. Arias N, Arboleya S, Allison J, et al. The relationship between choline bioavailability from diet, intestinal microbiota composition, and its modulation of human diseases. Nutrients. 2020;12(8):2340.
36. Eslami M, Alibabaei F, Babaeizad A, et al. The importance of gut microbiota on choline metabolism in neurodegenerative diseases. Biomolecules. 2024;14(11):1345. doi:10.3390/biom14111345
37. Boulanger CM. Secondary endothelial dysfunction: hypertension and heart failure. J Mol Cell Cardiol. 1999;31(1):39–49. doi:10.1006/jmcc.1998.0842
38. Mordi I, Mordi N, Delles C, Tzemos N. Endothelial dysfunction in human essential hypertension. J Hypertens. 2016;34(8):1464–1472. doi:10.1097/HJH.0000000000000965
39. Zhang Z, Zhao L, Zhou X, Meng X, Zhou X. Role of inflammation, immunity, and oxidative stress in hypertension: new insights and potential therapeutic targets. Front Immunol. 2022;13:1098725. doi:10.3389/fimmu.2022.1098725
40. Edwards JM, McCarthy CG, Wenceslau CF. The obligatory role of the acetylcholine-induced endothelium-dependent contraction in hypertension: can arachidonic acid resolve this inflammation? Curr Pharm Des. 2020;26(30):3723–3732. doi:10.2174/1381612826666200417150121
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.