Back to Journals » International Medical Case Reports Journal » Volume 17
Chlorzoxazone-Induced Fixed Drug Eruption: A Clinical Case Report
Authors Alotaibi H ![]() , Alsergani R, Alharbi AA, Nagshabandi KN
, Alsergani R, Alharbi AA, Nagshabandi KN ![]() , Almubark AA
, Almubark AA
Received 31 May 2024
Accepted for publication 31 August 2024
Published 5 September 2024 Volume 2024:17 Pages 771—775
DOI https://doi.org/10.2147/IMCRJ.S480653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Hend Alotaibi,1 Reem Alsergani,1 Amer Abdulaziz Alharbi,1 Khalid Nabil Nagshabandi,1 Asma Ahmed Almubark2
1Department of Dermatology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2College of Medicine, King Faisal University, Al-Ahsa, Saudi Arabia
Correspondence: Khalid Nabil Nagshabandi, Department of Dermatology, College of Medicine, King Saud University, PJ7C+89Q, Riyadh, 12372, Saudi Arabia, Tel +966-582940888, Email [email protected]
Abstract: Fixed drug eruptions (FDEs) are dermatological manifestations characterized by recurrent lesions at the same site upon re-exposure to the causative drug. We present a novel case of a 32-year-old female who developed bilateral symmetrical erythematous papules on her thighs following the use of chlorzoxazone for chronic back pain. This case is particularly significant as it underscores the potential for this specific drug, which is commonly prescribed, to induce FDE—a reaction previously unreported in the literature. The findings emphasize the necessity for clinicians to maintain a high index of suspicion for drug-induced skin reactions, even with medications considered safe and routinely used. This case serves as a critical reminder of the importance of thorough medication history assessments and the potential implications of drug interactions in dermatological care.
Keywords: acetaminophen, chlorzoxazone, drug-induced fixed eruption, pain management, paracetamol, skin hypersensitivity, symmetrical skin lesions
Introduction
Fixed drug eruption (FDE) is a dermatological response characterized by distinct erythematous patches upon repetitive exposure to a specific drug.1 Clinically, fixed drug eruptions manifest as circular or oval erythematous patches recurring at consistent sites upon drug re-exposure, often accompanied by pruritus and a burning sensation. Diagnosis hinges on the clinical presentation and the patient’s history of drug exposure. Management involves discontinuing the causative drugs and considering alternative medications. Supportive care may encompass the use of topical corticosteroids or antihistamines to alleviate symptoms.2 Preventing recurrence is paramount, necessitating patient education about the specific drugs that triggered the eruption and meticulous documentation in medical records. Although chlorzoxazone, a muscle relaxant, and is commonly prescribed for the management of back pain and many other musculoskeletal conditions, adverse reactions, such as fixed drug eruptions, can manifest due to a hypersensitivity response, eliciting immune cells and inflammatory mediators.3–5 To the best of our knowledge, no instances previously reported chlorzoxazone induced eruption. Herein, we report a novel case of a 32-year-old female who developed a fixed drug cutaneous eruption after commencing chlorzoxazone therapy for chronic back pain.
Case Presentation
A 32-year-old female with no significant past medical history presented with a two-week history of recurrent lesions symmetrically located on both legs. These lesions first appeared a week after she had taken chlorzoxazone for back pain relief. The lesions were non-painful, non-pruritic, and consistently reappeared in the same locations each time she used the drug. The patient did not have any chronic medical or dermatologic conditions other than her back pain. She reported no constitutional symptoms, such as fever, malaise, or systemic involvement. Notably, she had used paracetamol regularly for multiple years without developing any rash, which pointed towards chlorzoxazone as the likely causative agent.
Medication Use and History
The patient had been prescribed a combination of chlorzoxazone and paracetamol for back pain relief. Although she had taken paracetamol for many years without any adverse skin reactions, this was her first exposure to chlorzoxazone. Upon developing the skin lesions, she immediately discontinued both medications. Despite stopping the medication, the lesions persisted for some time before gradually resolving. Subsequently, when she was re-exposed to chlorzoxazone, the lesions recurred in the same locations, further supporting the suspicion that chlorzoxazone was responsible for the fixed drug eruption.
Laboratory Findings
Routine laboratory tests, including complete blood count, liver function tests, renal function tests, and electrolyte levels, were all within normal limits. There were no signs of systemic involvement or any underlying conditions that could have contributed to the skin lesions. The patient’s IgE levels were slightly elevated, suggesting a possible allergic response, but specific allergy testing was not performed as the patient refused further testing.
Causality Assessment
The Naranjo Adverse Drug Reaction Probability Scale was applied to assess the likelihood that chlorzoxazone was the causative agent of the fixed drug eruption. The patient scored 7 on the Naranjo scale, indicating a “probable” adverse drug reaction to chlorzoxazone.
Physical Examination
On cutaneous examination, multiple targeted erythematous papules and plaques with central hemorrhagic crusts were observed symmetrically over the thighs and knees (Figure 1). The lesions were well-demarcated, non-tender, and showed no signs of secondary infection. There were no palmar or plantar lesions, and no mucous membrane involvement.
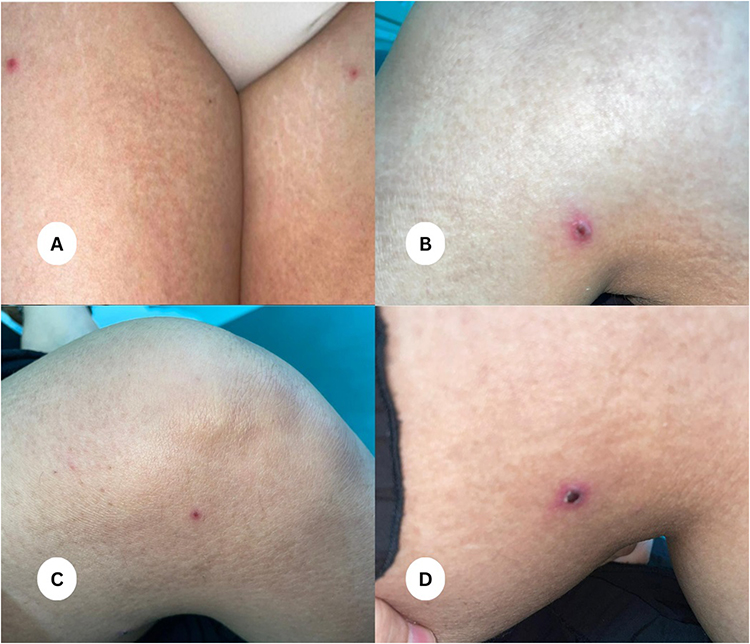 |
Figure 1 (A–D) Bilateral symmetric targeted erythematous papules with central hemorrhagic crusts on the skin of both thighs and knees. |
Histopathological Findings
A punch biopsy of the right thigh revealed parakeratosis, focal skin erosion, crust formation, and fibrin deposition, which were consistent with excoriation or itching. The epidermis showed acanthosis, spongiosis, and lymphocytic exocytosis, along with an interface reaction around the area of erosion. The dermis contained superficial and deep perivascular lymphocytic aggregates with accompanying eosinophils, findings suggestive of an allergic reaction, most likely drug-induced (Figure 2). These histopathological findings confirmed the diagnosis of a fixed drug eruption secondary to the use of chlorzoxazone.
 |
Figure 2 (A) (Hematoxylin & eosin, ×40), (B) (Hematoxylin & eosin, ×100) Histopathological examination revealed signs of parakeratosis, localized skin erosion, crusts, and fibrin material consistent with skin irritation and itching. Changes in epidermis exhibited acanthosis, spongiosis, and lymphocytic exocytosis, with an interface reaction around the erosion. In the dermis, there were clusters of lymphocytes arranged perivascularly, along with eosinophils, indicating a probable allergic reaction, likely triggered by medication. |
Discussion
Fixed Drug Eruptions (FDEs) are dermatological reactions associated with drug exposure, predominantly occurring in previously affected areas upon re-exposure to the causative drug. FDEs, in contrast to exanthematous skin reactions that constitute up to 95% of all cutaneous reactions, are comparatively less frequent and consequently prone to underdiagnosis. Furthermore, the existence of various FDE variants poses challenges in accurate diagnosis, particularly when clinicians are unfamiliar with the diverse manifestations of this condition.1 In individuals undergoing pharmacological treatment, the occurrence of a symmetric cutaneous eruption should prompt consideration of a potential drug-induced reaction.1,6 In our case, the histopathological findings of interface reaction around the erosion, along with perivascular lymphocyte aggregates and eosinophils in the dermis, aligns with an allergic reaction due to drug-induced hypersensitivity reactions underscoring the role of eosinophils in inflammatory reactions.7 On the other hand, the revealed parakeratosis, focal skin erosion, and fibrin material are consistent with excoriation and itching, indicating a secondary response to the skin lesions rather than a primary pathological process.
Paracetamol is a commonly utilized over-the-counter analgesic-antipyretic agent, recognized for its established safety profile characterized by a notably low frequency of adverse effects. Adverse cutaneous reactions caused by paracetamol are infrequent and typically manifest as fixed pigmentary eruptions.8 The incidence of Paracetamol-induced Fixed Drug Eruption is documented in fewer than 1.5% of all FDE cases. Such reactions may manifest as a maculopapular rash, bullous reaction, cellulitis-like reaction, pigmenting type or skin necrosis.9 Muscle relaxants such as carisoprodol has been reported to cause a fixed drug eruption in combination with meprobamate (anxiolytic).10 But only a single suspected case, documented in 1970, originating from St John’s Hospital reported that a patient experiencing the onset of a fixed drug rash subsequent to the administration of a chlormezanone, a muscle relaxant, and paracetamol combination therapy.5 Our case highlights a rare development of fixed drug cutaneous eruption caused solely by chlorzoxazone therapy, excluding paracetamol involvement as a potential cause, as the patient regularly took paracetamol without any rash development. FDEs are generally believed to be a type IV hypersensitivity reaction (cell-mediated immunity). The drug or its metabolite acts as a hapten, binding to epidermal cells and eliciting an immune response. Upon first exposure to the drug, T cells sensitized to the drug or its metabolites are generated. These memory T cells persist in the affected skin areas. On re-exposure to the drug, these T cells are rapidly activated, leading to inflammation and damage in the same skin sites.1,2
The Implications of this case, underscore the importance of heightened vigilance among clinicians when encountering dermatological presentations with overlapping features. Clinicians should consider a detailed medication history, paying particular attention to drugs known to be associated with cutaneous reactions, such as chlorzoxazone,11 which puts chlorzoxazone in the list of potential drugs causing such cutaneous reactions. The accumulation of such knowledge would not only enhance our ability to diagnose and manage these reactions effectively but also contribute to the development of preventive strategies and personalized medicine in the field of dermatology.
Conclusion
This case highlights chlorzoxazone as the causative agent of fixed drug eruptions, independent of the regular use of paracetamol. This is significant as it underscores the importance of detailed medication histories in identifying the true culprit of drug-induced skin reactions. We contribute to a more precise understanding of the mechanisms behind such eruptions, ultimately improving diagnostic accuracy and management strategies in dermatology.
Declaration of Patient Consent
Written informed consent was obtained from the patient for publication of the details of their medical case and any accompanying images.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Statement of Ethics
Ethical approval is not required to publish the case details in accordance with local or national guidelines.
Funding
There is no funding to report.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Shaker G, Mehendale T, De La Rosa C. Fixed drug eruption: an underrecognized cutaneous manifestation of a drug reaction in the primary care setting. Cureus. 2022;14(8):e28299. PMID: 36034061; PMCID: PMC9397151. doi:10.7759/cureus.28299
2. Crisafulli G, Franceschini F, Caimmi S, et al. Mild cutaneous reactions to drugs. Acta Biomed. 2019;90(3–S):36–43. PMID: 30830060; PMCID: PMC6502176. doi:10.23750/abm.v90i3-S.8159
3. Patel HD, Uppin RB, Naidu AR, Rao YR, Khandarkar S, Garg A. Efficacy and safety of combination of NSAIDs and muscle relaxants in the management of acute low back pain. Pain Ther. 2019;8(1):121–132. PMID: 30652262; PMCID: PMC6513919. doi:10.1007/s40122-019-0112-6
4. Böhm R, Proksch E, Schwarz T, Cascorbi I. Drug Hypersensitivity. Dtsch Arztebl Int. 2018;115(29–30):501–512. PMID: 30135011; PMCID: PMC6121083. doi:10.3238/arztebl.2018.0501
5. Wilson HT. A fixed drug eruption due to paracetamol. Br J Dermatol. 1975;92(2):213–214. PMID: 125095. doi:10.1111/j.1365-2133.1975.tb03061.x
6. Iannini P, Mandell L, Felmingham J, Patou G, Tillotson GS. Adverse cutaneous reactions and drugs: a focus on antimicrobials. J Chemother. 2006;18(2):127–139. PMID: 16736880. doi:10.1179/joc.2006.18.2.127
7. Caro-Chang LA, Fung MA. The role of eosinophils in the differential diagnosis of inflammatory skin diseases. Hum Pathol. 2023;140:101–128. PMID: 37003367. doi:10.1016/j.humpath.2023.03.017
8. HireRC SS, Dakhale GN, KambleA K. Paracetamol induced fixed drug eruption: a case report. Int J Basic Clin Pharmacol. 2014;3:
9. Kimmatkaar P, Das S, Gandhi A, Taneja V. Paracetamol-induced fixed drug eruption presenting as eyelid skin necrosis. Indian J Ophthalmol. 2018;66(11):1627–1629. PMID: 30355885; PMCID: PMC6213702. doi:10.4103/ijo.IJO_448_18
10. Honeycutt WM, Curtis AC. Fixed drug eruption to carisoprodol and cross reaction with meprobamate. JAMA. 1962;180:691–692. PMID: 13908692. doi:10.1001/jama.1962.03050210053017a
11. Popiołek I, Piotrowicz-Wójcik K, Porebski G. Hypersensitivity reactions in serious adverse events reported for paracetamol in the eudravigilance database, 2007⁻2018. Pharmacy. 2019;7(1):12. PMID: 30658389; PMCID: PMC6473647. doi:10.3390/pharmacy7010012
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.