Back to Journals » Patient Preference and Adherence » Volume 14
Chinese Hospitalized Cardiovascular Patients’ Attitudes Towards Self-Management: A Qualitative Study
Authors Qiu R ![]() , Schick-Makaroff K
, Schick-Makaroff K ![]() , Tang L
, Tang L ![]() , Wang X
, Wang X ![]() , Zhang Q, Ye Z
, Zhang Q, Ye Z ![]()
Received 30 October 2019
Accepted for publication 1 February 2020
Published 17 February 2020 Volume 2020:14 Pages 287—300
DOI https://doi.org/10.2147/PPA.S236348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Ruolin Qiu, 1 Kara Schick-Makaroff, 2 Leiwen Tang, 3 Xiyi Wang, 1 Qi Zhang, 1 Zhihong Ye 1
1Faculty of Nursing, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Faculty of Nursing, University of Alberta, Edmonton, Alberta, Canada; 3Zhejiang University School of Medicine, Affiliated Sir Run Run Shaw Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Zhihong Ye
Faculty of Nursing, Zhejiang University School of Medicine, #704, Administrative Building, 3 East Qingchun Road, Hangzhou, Zhejiang 310016, People’s Republic of China
Tel +86 136 0661 2119
Email [email protected]
Purpose: This study is aiming to investigate cardiovascular patients’ attitudes towards self-management during hospitalization in China.
Patients and Methods: Twenty-nine individuals living with cardiovascular disease from one designated Cardiology Department in Hangzhou, China, were recruited through a purposive sampling procedure. A qualitative descriptive methodology was used. Semi-structured interviews were also used to gain attitudes toward self-management. The interviews were audio-recorded, transcribed and analyzed by thematic analysis to develop the results.
Results: Four themes were identified from the qualitative data: (1): Responsibilities of self-management; (2): Reflections on self-management; (3): Acknowledgement of self-management support; (4): Challenges in implementing and adherence to self-management. Additionally, interview data were also given to illustrate these main themes emerging during the analysis. Patients gradually took their responsibilities to manage chronic symptoms. During their self-management process, they did reflections to help correct their regiments through supportive interactions. Health system responsiveness, health disparities, social capital, and cultural setting were the main external factors influencing better self-management implementation and adherence.
Conclusion: This study revealed the hospitalized cardiovascular patients’ attitudes towards self-management in China. These findings emphasized the importance of patients’ responsibility, reflections, and various social support receiving and pointed out specific external factors influencing the health outcomes and their quality of life. This study also proves the guide for the policymakers and health system better instructions to develop individually and culturally tailored advanced self-management interventions and programs.
Keywords: attitude, hospitalization, cardiovascular disease, self-management, qualitative research
Introduction
Non-communicable diseases (NCDs), which include chronic diseases, and their ongoing health conditions will result in a high rate of mortality around the world.1 As the World Health Organization projects reported that annual deaths resulting from non-communicable diseases would increase from 40 million in 2016 to 52 million by 2030. Moreover, cardiovascular diseases (CVDs) are several the most prevalent causes worldwide, like ischaemic heart disease, stroke, and hypertensive heart disease.2 Based on previous Chinese statistics, the number living with CVD was increasing, as well as the high rate of mortality, the percentage of which reached 40% in 2010.3,4 Furthermore, chronic diseases including cardiovascular diseases sometimes affect patients’ quality of life and impose heavy financial burdens, especially on the primary health-care system.5 As an essential component of chronic disease management, self-management is widely recognized as a cost-effective intervention to control patients’ ongoing chronic conditions and improve patients’ quality of life.6,7 However, self-management required sufficient focus, resources, and emotional processing to ensure to complete the specific tasks and address kinds of challenges when living with chronic diseases.8 Nevertheless, there is also a diversity of determinants that affect the implementation and maintenance of self-management.9 According to the literature related to the social cognition models of illness belief, individuals holding different views could affect coping strategies and finally the health outcomes both in chronic and acute diseases.10 That is to say, cardiovascular patients’ actions and responses, such as forming self-management strategies, could be shaped by their attitudes.11 It was shown in an earlier study that patients with negative attitudes had worse adherence to lifestyle changes and medication in kinds of chronic conditions.12–14 Moreover, negative attitudes, as well as inadequate knowledge and poor perceptions, have been found as significant challenges in previous studies towards patients’ self-management with chronic disease by quantitative survey.15,16 Besides, there were some qualitative studies have explored the patients’ perceptions and attitudes towards self-management who live with cardiovascular diseases. Fitzpatrick et al17 used photovoice to photograph Asian elders’ perceptions of scenes promoting or acting as barriers to cardiovascular health. Liu et al18 found that different attitudes influenced self-management priority setting and decision-making among Chinese patients with acute coronary syndrome and type 2 diabetes mellitus through deductive directed content analysis. As such, adopting patients’ attitudes can lead to a better understanding of how an individual’s real demands on treatments to achieve the setting-goals, help to tailor individualized self-management strategies and reduce the financial burdens at all levels.
In spite of the importance of the self-management and development of the ongoing intervention as well as the policy, the awareness of self-management is still varied while the improvement strategies were predominantly focused on related professionals.19–21 Unfortunately, to our knowledge, few studies have described how Chinese cardiovascular patients perceive this critical topic, and little is known about how patients think about their self-management process when they are in hospital. Therefore, this study was conducted to investigate cardiovascular patients’ attitudes towards self-management during hospitalization.
Methods
Design
This was a qualitative descriptive study, focusing on cardiovascular patients’ personal experiences of self-management. A phenomenological design using semi-structured interviews was chosen.22 Thematic analysis was used to produce the results, for the study aimed to gain a deeper understanding of the patients’ attitudes towards self-management and perceived challenges when they were engaged in the management.
Setting and Sampling
The study was conducted in the Cardiology Department of Sir Run Run Shaw Hospital (SRRSH) in Hangzhou, China. It was not until the authors obtained permission entering the department from the Nurse Deputy Director and Department Nursing Directors could the study recruitment begin.
A purposive sampling procedure was used to recruit patients with rich information within both genders. People over 18-year-old with cardiovascular disease were included. Other inclusive conditions were as follows: 1) patients participated in the study voluntarily with the informed consent; 2) participants had a clear mind to share their experiences willingly; 3) caregivers could offer vital help with recruitment; 4) participants did not attend other researches at the same time. Nurses in the recruitment site assisted in identifying eligibility, including registration information and medical histories. Potential participants’ names and bed numbers would be collected, and then nurses would inform them or their caregivers about the study.
In total, 32 patients hospitalized in the Cardiology Department were invited, 6 of which was invited by informing their family caregivers, but later only 29 participants were recruited. One female patient refused to talk about her disease, and the other two invitations were rejected by their families. Later, two researchers (R.Q and Q.Z) approached recruited participants accompanied by one on-duty staff and gave a specific introduction about the study, including the purpose, confidentiality, and voluntary principle. Similarly, participants were asked to provide written informed consent. Those who were not convenient or unable to write their name characters were asked to grant oral permissions. In this case, all the voice materials would be recorded and kept. They were invited to have in-depth interviews to share personal experiences. Under the study setting, participants were supposed to undertake the discussions in a quiet place. According to individual preference, they could choose a separate meeting room of the department, or tell researchers to take interviews beside their beds. No one would be present except their caregivers and bed curtains would be pulled up, which could create a quieter and more private area.
Data Collection Procedure
The reported qualitative data were collected from in-depth interviews from April to May 2018, which were mostly conducted by the first author. The first author, R.Q was a Ph.D. candidate with the ability to understand most local dialects. Q.Z. was a master student, and also a research member, helping to take field notes without speaking during eleven interviews. Also, Q.Z conducted three interviews by herself. Both of the researchers were trained about the description of the study and principles of ethics. While the interviews were being conducted, fourteen family caregivers were present. Family members were expected to be present and were supposed to offer necessary help during an emergency. In addition, the authors sometimes needed their interpretation to learn the explicit meaning of participants’ words. Sometime participants would ask their families for details about their activities, but there was no impact on the participants’ statements.
Data collection followed a semi-structured interview guide based on the Chronic Care Model,23 which was piloted with patients with chronic diseases in the hospital for physical examination. After a discussion of the research team, the guideline was translated into understandable words and made some local culture customization. The guideline covered topics including used self-management strategies, the consequences of having chronic diseases, perception of chronic disease self-management, and barriers influencing self-management preference. Several open-ended questions were asked intentionally to explore rich information from patients’ perspectives, and participants could answer using their own words and accents. Some family members helped translate patients’ ideas in mandarin when patients used dialects. Most interviews were conducted next to patients’ beds, lasting between 5 and 115 minutes. Interviews were audiotaped. Two patients (patient #15 and patient #19) stopped the interviews and left for a physical examination in the hospital but their data were still kept for analysis with their permission. Audio materials were all transcribed verbatim in Chinese by the researchers and encoded to guarantee anonymity. Both interview records and text documents were stored in a highly protected research environment or secure computer to ensure confidentiality.
Ethics
The ethical clearance of this study was obtained by The Ethics Committee, Sir Run Run Shaw Hospital, College of Medicine, Zhejiang University (20181203-7). Written informed consent was kept, and the oral permissions were audio-taped from all participants before interviews started, and all the interview materials were securely stored. Participants could refuse to answer any question and withdraw at any time without repercussion. This study was conducted in accordance with the Declaration of Helsinki.
Data Analysis
According to the method approach recommended by Braun and Clarke,24 a thematic analysis was applied in the study, and the demographic characteristics were presented by description. All the data were only analyzed manually by the first author, R.Q, and memos were used to support to capture the initial ideas about the study questions.
First, the first author immersed in the transcripts and keep repeated reading to get familiar with all aspects of the qualitative data. During the phase, basic notes were taken to obtain an overall picture, while initial ideas related to the study objectives were noted down. Second, the data were reread in more detail, codes were generated, and they were organized into meaningful segments. Third, different codes were collated into potential themes or sub-themes, and other extracts were considered to be reviewed for relation to them. Then, the candidate themes or extracts were all made further decisions of reservation, refinement, combination, abandon, or detachment to reach an accurate representation. Finally, clear definitions and detailed descriptions were conducted to fit determined themes.24
After finishing the analysis process, the first author asked another two researchers (L.W & Q.Z) for opinions and invited an expert (K.S) to discuss the identified themes for further reliability. The following factors enhanced other rigors of the study. Initially, it was essential to emphasize the aim to learn different perspectives from patients about the research questions as well as use the rigors approach without any preliminary judgment during the whole interviewing process. Also, triangulation among participants, researchers, and other reviewers not only determine the credibility and validity25 but also diminished the potential bias. That meant, interviewees share their opinions and provide feedback, while two independent researchers conducted interviews and other reviewers checked the codes and emerging themes.
Findings
Patients
Totally twenty-nine of the participants, comprising twenty-one men and seven women, vary from 32 to 86 years old were interviewed in this study. Participants all had cardiovascular diseases, and some of them had other comorbidities, such as diabetes and cancer. There were supposed to be twenty-nine persons in the analysis; however, during the interview, researchers found that one of the participants had a dialect that was difficult to understand so that the participant was excluded in the analysis. Table 1 provides the details of twenty-eight participants’ demographic characteristics.
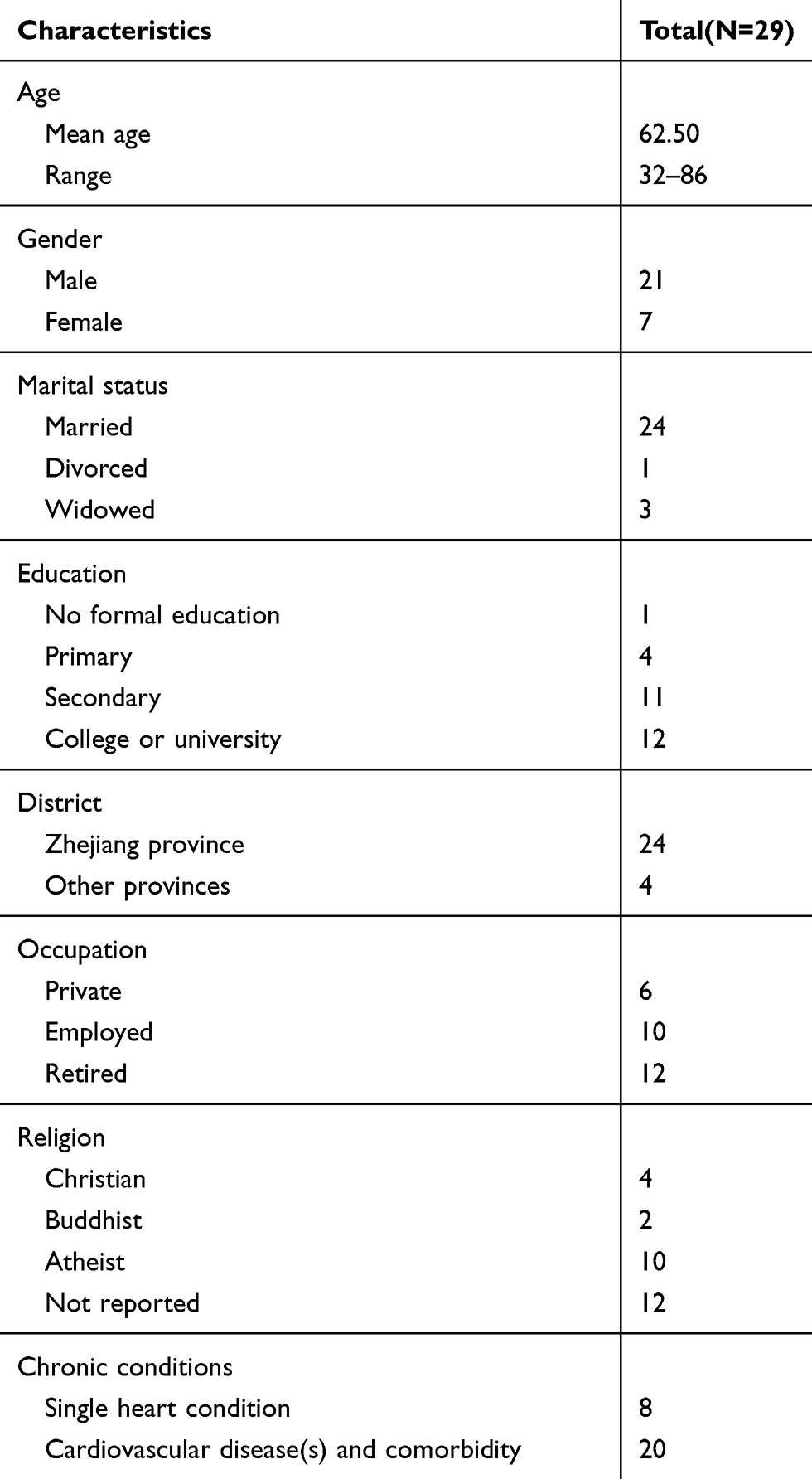 |
Table 1 Patients’ Demographic Characteristics |
Attitude Towards Cardiovascular Disease Self-Management
The attitudes were related to participants’ perspectives and thoughts of self-management, which could also result in their exact reactions as well as behaviors in practicing their strategies. Regarding participants suffering from diverse chronic conditions and different life events so that everyone had described multiple attitudes when answering the question about how they thought about their self-management. As the study aimed to explore the principal attitudes towards self-management, thus only a single attitude was reported in the following. There were four main themes identified: (1): Responsibilities of self-management (four subthemes); (2): Reflections on self-management (four subthemes); (3) Acknowledgement of self-management support (three subthemes); (4) Challenges in implementing and adherence to self-management (four subthemes). Additionally, interview data were also given to illustrate these main themes emerging during the analysis. (See Table 2)
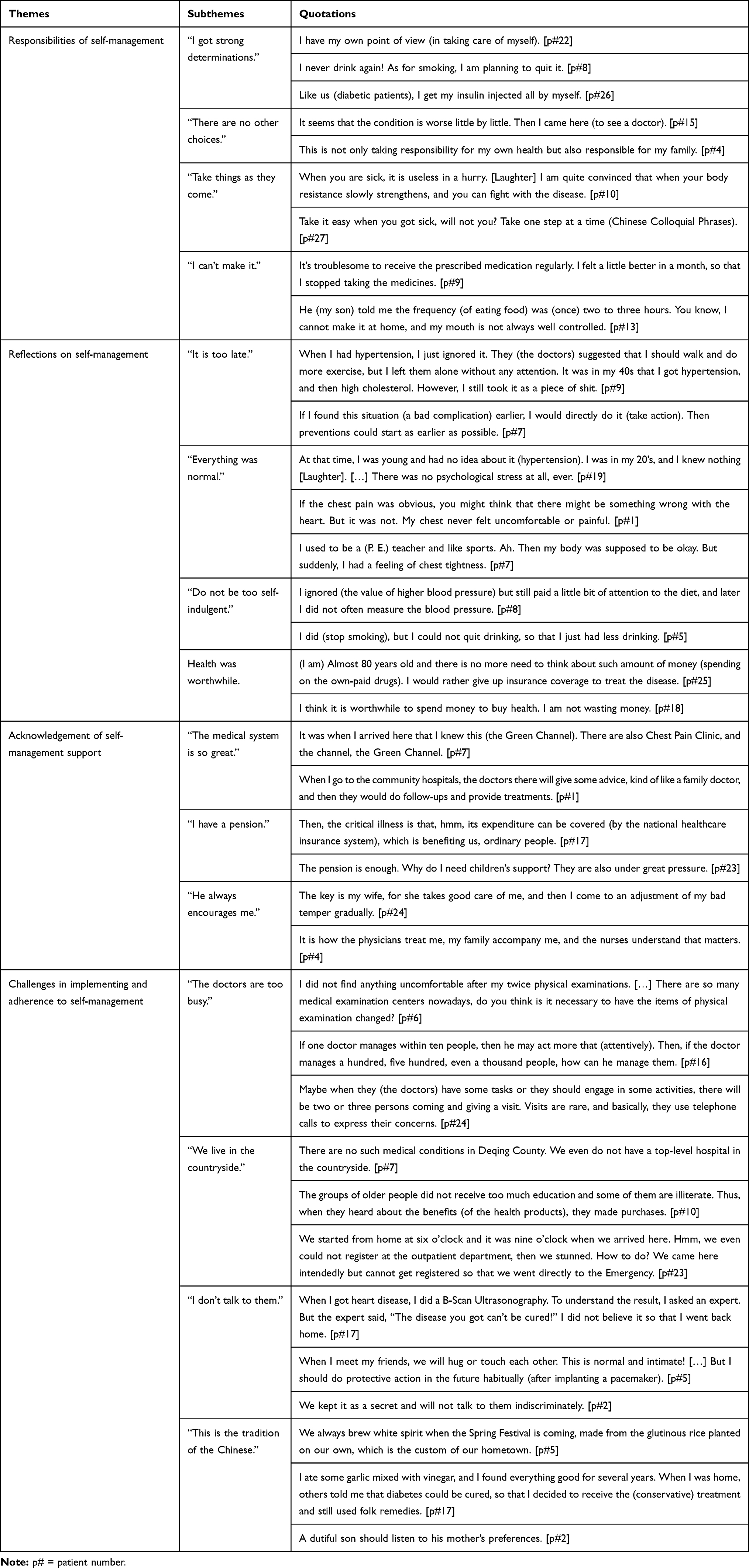 |
Table 2 Themes, Subthemes and Quotations of Attitudes Towards Self-Management |
Theme 1: Responsibilities of Self-Management
Most cardiovascular patients had multiple symptoms. When they perceived their body was in the progress of deterioration, they would take suggested actions to protect themselves away from the risk, or they would even take other alternative treatments to get a better status. They realized they should take responsibility by themselves no matter active or passive.
“I got strong determinations.” Some patients noticed the major determinant of fighting with the chronic disease was themselves. Once they made their own decisions to practiced self-management and insisted on one behavior independently, they could get benefits from what they have done. There was a quotation showed:
If it benefits my body, I will persist (in eating bitter melons) even though they are unpalatable. [patient #20]
Another one said:
You are the one that you should rely on (when you want to control your symptoms). [patient #2]
“There are no other choices.” Most participants had a tough period struggling to make their body conditions better. And they told that during that time, they were heavily disturbed by those symptoms so that they did practice self-management seriously, like taking medicines regularly or going to consult a professional. As the evidence showed:
When you feel uncomfortable, you have to take medicines and have to go to the doctor’s. Because there is no other way. [patient #3]
Participants also described that they had to take self-management behaviors to get rid of the fear of death. That meant the motivation was that they realized sicknesses were a huge threat to their lives. One participant said:
It is necessary to attach importance to (conduct) them (self-management) at once, rather than “It doesn’t matter.” otherwise you might lose your life. [patient #1]
“Take things as they come.” Several participants admitted the situation that they were older, and their aging organs were naturally getting weaker than ever before, which was an irreversible process. Thus, participants accepted to implement self-management not forced by others but driven by the nature of the world. It is quite natural for a human being to get sick and individuals should take the result as it would be. One participant said:
When you are older, your body will get worse and weaker, and so the aging organs are. Is that right? This illness will be more serious little by little, and it is impossible (to be the same as original). Isn’t it? So, it is a good idea for us to control it well and keep it as the present, right? [patient #3]
“I can’t make it.” This referred to those participants who regarded taking responsibility as a tough task and might not cope with the self-management. They realized the self-management behaviors were good for them once they practiced; however, they could always find reasons to avoid performing better and making a necessary change. As one participant stated:
I do have the idea but without any confidence. [Laughter] Can you imagine how difficult to make up your mind to quit smoking? You need to be confident! [patient #9]
A participant said he was lack of self-discipline, and he always ignored the importance of self-management. He said humorously:
Frankly speaking [Laughter], I only have little self-discipline. For some people, when it comes to the disease, they perform well, because they are afraid of death. But for us, we don’t fear death at all, so that we can’t manage the body well. [patient #1]
Theme 2: Reflections on Self-Management
Many patients have considered why they got their present health status and how they could act to make up for their unhealthy behaviors to reach the expectations. Some of them were regretful to be so dumb in perceiving uncomfortable in the early stage as well as behaving healthier late and were always likely to present their stories in a positive attitude. Some of them gave it an imagination if they could take actions much earlier or more adherent to the physicians’ suggestions no matter it would cost. And others reported that there were too many cardiovascular people without any harmful and visible body damages immediately after being diagnosed. Therefore, they even did not treat those as life-threatening illnesses.
“It is too late.” Patients had the views because they did perceive that their body conditions were in a bad status and were already told by the physicians to manage their diseases. However, they did not pay adequate attention to those considerable suggestions and even ignored them. When looking back, they rued the day. For example, one participant found it too casual and too late to do self-management:
I delayed. I delayed seeing a professional all the time until I felt it painful of my foot. I finally asked a doctor what happened, and the doctor told me to take some medicines. But I have already got the side effect- vomiting, accompanied all the other complications. [patient #2]
“It seems everything is normal.” Symptoms indicated how the patient’s health status was. But as some patients reported, they got a sudden sign like chest pain, and then they found they were in bad health status. Before this, they had few senses about they were under a high risk of getting a worse situation. Otherwise, they would seldom undertake management instructions to prevent the adverse outcomes of the diseases. That is to say, self-perceived “good” condition or “young” body deceived participants, which made them feel “healthy” or “strong” so that they missed the best opportunity to get the suitable treatment to alleviate the ongoing symptoms. A participant said:
I didn’t feel particularly uncomfortable. About ten minutes later or after a break, all was well, and so I didn’t attach any importance to those symptoms. [patient #6]
“Do not be too self-indulgent.” Self-management should take all kinds of healthy behaviors into considerations. But participants only complied with some ways suggested by the professionals and expected to control their conditions through a single strategy. They admitted casual management behaviors did harm their health and cost more money, energy, and time. One participant described:
My daily life is more like to do whatever you want, including entertainment, eating, and drinking, but as for physical exercise, it is casual. [patient #1]
“Health was invaluable.” Some of the participants mentioned that life was only given once, and they were in a stage where they found there was nothing more precious than their body health. Thus, they started to value this kind of treasure, and they used self-management no matter it would cost, especially the money. For instance:
If you do have the (financial) condition, take medicines as good as you can. You know, the body is the essential thing that matters, and the money is not … You see, it’s useless to save money, for your body is consuming your money anyway. [patient #10]
On the other hand, good health could help to improve the quality of life, especially when you were old, and self-management could gather better health. One participant reflected:
After all, you should consider that when people are old, actually the most crucial property is health. There is no guarantee for your life quality with the absence of good health. [patient #27]
Theme 3: Acknowledgement of Self-Management Support
Practicing self-management is a multi-team work, which means when it referrers to conducting participants’ management strategies, they could never complete all the processes by themselves alone. Thus, when answering how they practiced their disease management, participants always expressed their appreciation to those supports from various resources.
“The medical system is great.” As the primary support for all the patients, the medical system provides adequate medical services, both physically and mentally, permeating patients’ every behavior. For example, the regular medication picking-ups and body check-ups in daily life, acute care in emergency events, as well as other health-related consulting and interventions. Some of the interviewed participants had enjoyed these services, and they gave this setting an encouraging affirmation. When a participant mentioned he was sick and accepted the emergency care in the hospital, he got much medical assistance, and he said gratefully:
It is how the physicians treat me, my family accompany me, and the nurses understand that matters. [patient #4]
“I have a pension.” Participants always talked about their costs of treating their diseases. Expenditures on the chronic illness were not a small number, but some retired participants declared that they could still afford the medical bills due to the pension from the government. Besides, the government plays as a backup force on the coverage of the healthcare insurance system, whose policy is aiming to prevent patients from economic difficulties caused by necessary healthcare expenditures. Evidence showed:
I have got the (financial) support from the government. Now we have a good government, as everything is there, and we also can apply to cover most of the medical expenditures. [patient #17]
Except for the supports from the government, the social organization is another source to give a hand to those who have difficulties, for example:
When a family is getting in trouble (due to the disease), oh, the people in the Church will assist them with whatever they have, the money, or the energy. [patient #28]
“He always encourages me.” Participants described some psychological stress when coping with the symptoms or complications and facing challenges. As one of the most cited items in the interviews, good interactions and communications between others and them would help relieve their pressures, like professionals, family, friends, and peers. During these kinds of supportive interactions, they got adequate emotional support. The sentence was:
It may be more uncomfortable for me without his words. [patient #5]
The emotional distress could also come from God, so many participants reported that they would pray depending on their faith and religion when they suffered. The quotation was:
I pray (to Jesus) every day. […] I have been living with the disease peacefully. [patient #17]
Theme 4: Challenges in Implementing and Adherence to Self-Management
Only when the patients planned reasonable self-management strategies individually and complied with the treatments could they control their chronic conditions well. But some of the participants said they had tried their best to put more effort into practicing, but there were various external barriers out of patients’ control during the management processes, which would influence their practicing and adherence. The obstacles appeared to be varied but were very common among patients with cardiovascular diseases as well as other chronic diseases.
“The doctors are too busy.” Though the participants had appreciated what they had received from the health system overall, but some of them still expressed they were not that satisfied with the present health system, such as the setting of various medical institutions, like basic community hospitals, higher-level hospitals and medical exam centers, the attitudes and the qualifications of the professionals, and the effects of treatments. Several patients described their terrible experiences in the outpatient department. For example:
When you go to see a doctor, you have to wait for a long time, maybe half an hour. After thirty minutes, it is your turn, but the inquiry lasts three minutes, and then it is over. [patient #1]
“We live in the countryside.” Some participants always talked about the difficulties of access to better medical services because of the long distances from those high-quality medical institutions. Most participants mentioned they wanted to find a hospital with a good reputation and seek better medical care conditions, including more professional health providers, more advanced pieces of equipment and better treatments. It was strongly related to the fundamental conditions when the patients want to manage their disease well. But as participants stated, in the low-developed areas, there was a lack of educational opportunities and financial support. One patient described:
In our community hospital, there is a doctor who used to be a barefoot doctor. […] Professionals are all in high-quality here. Oh, equipment is also better here. Yes, of course, the medical conditions are great. [patient #10]
Nevertheless, participants had praised the rural environment surroundings. They said they preferred to exercise in a place with more green areas. There was the evidence going:
Differently, here are tall (buildings). […] It is a big city without a place to walk. But we are in small cities, and the air is very fresh all around. So along the river, we could walk along the riverside. [patient #14]
“I won’t talk to them.” Some participants said that they did not have too many friends and solid interpersonal friendships to discuss with their recent conditions. Someone revealed that it was personal self-protective intention to avoid contacting or being touched by others. Or patients were passively refused to get close to people after experiencing negative emotions and bad interactions, like stigmatization and denial, which badly influenced individuals’ dignity and the trust among individuals and groups. Under these situations, they preferred to stay alone rather than ask for support, do prays or search online information by themselves. For example:
Because I always think that I am in poor health, so I should keep away from other people. I am afraid of being infected. [patient #24]
“This is the tradition of the Chinese.” Interviewed participants were from different provinces of China. They reported that some diet habits were shaped by local cuisine characteristics and kept all the time. But due to the career change, business and moving, they take internal migration so that they might live with local diet habits. Furthermore, the Chinese had a variety of festivals and special moments, and different places had diverse customs to celebrate linking with diet patterns. As a participant said:
[Laughter] As soon as I arrived Chengdu at the Qingming Festival, I told my buddies I wanted to eat something delicious, so that we went to for the food, good smelling, heavily oily, salty and spicy. [patient #1]
They also had a lot point of views in traditional values which related to the decision-making. For instance, several patients believed that Traditional Chinese Medicine and some folk remedies had their strengths. However, one patient thought Traditional Chinese Medicine should be used scientifically, not blindly. And the patient said:
Regarding treatments (of chronic disease), Chinese medicine is sometimes more scientific than Western medicine. […] If one hundred patients had the same problem, Chinese medicine doctors could give one hundred different prescriptions accordingly, but Western medicine works conversely, only five treatment plans for these people and then the patients try them one by one. [patient #12]
Another example was about family authority. Regarding filial piety, an old female patient wanted her son to obey her wishes, while a young man refused to bother her mother, and preferred to afford his family rather than take sick leave. Another male patient thought his wife should respect his decision about maintaining an unhealthy lifestyle because he was a man. He said:
I thought she was a short-sighted woman, and her views could not be taken seriously. [patient #1]
Discussion
This study provides some new insights into Chinese cardiovascular patients’ attitudes towards self-management. The findings emphasized that the responsibility of self-management should be shifted to the individual, which was also highlighted in a previous systematic review and qualitative synthesis from the perspective of patients with obesity, type 2 diabetes mellitus and chronic obstructive pulmonary disease.26 As stated by Statfield,27 the individual acted as the “responsible stewardship of one’s health.” Some recent studies demonstrated that these responsibilities referred to taking control of the disease management by themselves and were acquired by learning, teaching or empowerment, such as improving self-efficacy, accepting social identity, problem-solving, and adaptive coping.28–33 What showed by this study was that one participant could both reported active and passive attitudes based on specific conditions personally. This might potentially be related to their current situation — receiving acute care in the hospital. Another possible explanation was that the knowledge related to their disease conditions has been accumulated but still inadequate, which could help to develop the awareness of self-responsibility and lead to their situational self-management practices.
Compared with a mixed-methods study in adults with heart failure using intentionally guided reflection, this study showed that participants would make active reflections on their actions before this hospitalization caused by cardiovascular disease exacerbations.34 Meanwhile, several participants appeared to be happy when doing reflections on their self-management, which helped them rethink and then correct their self-management regiments. This study revealed that patients’ behavior self-regulation might be related to their metacognition,35 which could be verified by empirical researches in the future. And it is possible to apply guided reflection in the later interventions.
This study elucidated the inner voices of patients for their acknowledgment of the social support received from various kinds of resources. Patients with cardiovascular diseases, especially those with comorbidities or complications, usually access different levels of healthcare facilities and use a variety of medical supplies. For the participants in this study, treating and managing cardiovascular diseases caused enormous economic burdens, such as high health expenditures on medical visits and hospitalizations, or other spending on food, transportation, and work productivity and activity impairment.36,37 Thus, financial support from the government, such as the healthcare system, pension, and allowance, or other information sources, like charity, community, and personal, made it much more affordable for patients to deal with chronic conditions.36,38 Even though those participants with high salaries did not pay much attention to this kind of support since they were able to pay for those medical bills, it was even better to have healthcare insurance coverage. As such, all the participants appreciated the financial support from the government.
Participants expressed intense demands on emotional support.39–41 Health professionals are expected more to value empathy, understanding, and reassurance on what patients are suffering because they are trained to be so.42,43 Offered with peers’ experiences, patients could absorb practical knowledge from peers to meet their own self-management needs.44 Family members re-organized themselves to support patients cope with challenges and keep normality, leading a subsequent adaption for families.45 Many participants in this study expressed thanks to their family members but also delivered apologies for being such a burden.46
Conversely, some of the participants in this study had experienced stigmatization, denial, blame, and other negative interactions, for instance, time-limited communication with physician, made these people reluctant to disclose themselves and start to avoid people, even self-isolated.26,47 Under these situations, some participants would rather believe in their faiths to exclude psychological distress.48,49 Or others would prefer to use electronic devices to get access to mobile health (mHealth) approaches.50,51 It might be explained that mHealth intervention made participants more engaged in the interaction and strengthen mutual relationships, and online information helps them exchange real-time feelings and receive online peer support, which created stability when life transition occurred.51,52 Sometimes, it could help patients do more reflective thinking on acquiring knowledge and insights about their situations.53,54 Furthermore, more evidence needs to support the function of the mHealth approaches when patients are suffering from negative events about self-management.
The information pathways mentioned above were based on the patients’ social capital.55 Social capital could exert effects on patients through knowledge diffusion, informal social control of healthy behavior, healthcare services and amenities access, and emotional or material support and mutual respect receiving.56 Except for social capital, other contextual characteristics would also be the external obstacles that could influence self-management strategies and health outcomes, for example, factors related to health disparities57 (economic considerations, education opportunity and so on) and health system responsiveness58,59 (environmental features, characteristics of the population and so on). It turned out that highly educated participants in this study expressed more fluently and gave more information about their perspectives. As a consequence, patients from rural areas with low socioeconomic status had lower social capital to get access to top-class medical resources as urban citizens did.60 And they could have more inferior self-monitoring effects on their symptoms.61 Due to the shortage of health resources, barefoot doctors with low-educational level and informal identity recognition still served as community health workers in the rural areas,62 which accounted for some complaints in the study about their incompetent professional.63 Besides, owning less awareness to seek appropriate self-management strategies, people in such areas were easily trapped in a health-product sale scheme.64
Cultural setting, including cuisines culture, traditional norms, and values, is another implication that should be highlighted.65 Recommendations for treatment or self-management sometimes were juxtaposed or contrasted with the traditional Chinese values and views when patients made decisions, but they would decide to use the integrated approaches or prefer traditional one accordingly.66–68 Patients usually made the final decisions after consulting with family members.69 The other is that gender power and masculine norms in Chinese family accounts for male patients’ unwillingness of following their wives’ suggestions about lifestyle adjustment.70 Both of the reasons caused family caregivers’ burden. More researches are required on the relationship between the self-management process, family value, and family adaptability. Chinese food always uses much oil, sauce, and salt which are significantly related to cardiovascular disease.71 And the cuisines vary from different district parts, with some regional featured food eating account from the traditional geographical customs and for social functions.72 Nevertheless, when some patients move up from one to another place with different cuisines, the immigrations might live with local healthy food habits to be integrated into the new environment and to get a better interpersonal relationship.72 But it might be tough for older people to change their minds since they thought they might lose their quality of life and happiness, which was the same finding in the study by Shen.68
What was interesting was that attitudes could be directly or indirectly formed from a person’s past life experiences and various present situations, and some participants had changed their attitudes and coping approaches towards self-management after experiencing special event.73 For instance, support based on social capital could be restricted due to internal migration, even intercultural immigration,74,75 and then social networks would influence their health outcomes. But the relationship between diverse life events and patients’ coping approaches was not identified by the current study and needed further investigation.
Conclusion and Implications
In conclusion, these findings revealed the cardiovascular patients’ attitudes and perceptions towards the self-management process under the context of hospitalization, and highlighted that attitudes significantly influenced self-management behaviors. This study emphasized the importance of self-responsibility undertaken to manage chronic symptoms, reflections to enhance knowledge, regulation of self-management strategies during the self-management process, and the supports as well as the main challenges that prevented better self-management implementations. Policymakers, health practitioners, nurses, and other professionals may consider all these challenges to better understand cardiovascular patients’ attitudes, and consider how they may influence the outcomes of patients’ self-management and further, their quality of life. Hospitalization may be an opportune time for professionals to guide patients in proactive self-reflection, and to boost awareness of the importance of enhancing responsibility towards self-management. More situationally, individually, and culturally tailored interventions and programs could be developed to verify the effectiveness of self-management in the future. Further, policymakers may facilitate policy development to reduce the disparities for those living in underdeveloped regions with fewer inherent social supports.
Limitations
This study had a few limitations. All the results were based on the data provided by twenty-eight individuals with cardiovascular diseases during hospitalization, and most of them were from Zhejiang Province and might have been restricted within the districts. Further studies could be conducted to explore district as well as gender differences. Therefore, their opinions reflected by the context and living environment, as well as the psychological status, cannot be generalized to otherChinese people. The diversity of the representative patients in our data set could be increased by maximum variation sampling, which could help to cover the patients in the community, with other kinds of chronic diseases, from different provinces, etc. There was only one person who did the primary data analysis, but there were two other researchers, and an expert reviewed the themes regarding the interpretation of the data, which strengthen the reliability of this study. Furthermore, during the study, the places of interviewing were not too ideal for conducting private interviews, for noisy surroundings not only influenced the quality of records but sometimes interrupted participants’ thinking. A much quieter and private place was required to obtain sufficient information.
Acknowledgments
The authors would like to express thanks to the funder and all the group members in the research team, as well as those who had provided their assistance during the research process. The authors also especially acknowledge all the participants for their contribution to the narrative data and cooperation. The study was supported by grants from the Department of Health of Zhejiang Province (2019ZD034). Funders provide financial support during the data collection process.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bratzke LC, Muehrer RJ, Kehl KA, et al. Self-management priority setting and decision-making in adults with multimorbidity: a narrative review of literature. Int J Nurs Stud. 2015;52:744–755. doi:10.1177/1753193414567012
2. WHO. Projections of mortality and causes of death, 2016 to 2060. 2018. Available from: https://www.who.int/healthinfo/global_burden_disease/projections/en/. Accessed on 3 October 3, 2019.
3. Yang G, Kong L, Zhao W, et al. Emergence of chronic non-communicable diseases in China. Lancet. 2008;1697–1705.
4. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990–2010: findings from the global burden of disease study 2010. Lancet. 2013:381:1987–2015.
5. Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet. 2017;390:2584–2594.
6. Allegrante JP, Wells MT, Peterson JC. Interventions to Support Behavioral Self-Management of Chronic Diseases. Annu Rev Public Health. 2019;40(1):127–146. doi:10.1146/annurev-publhealth-040218-044008
7. Guo P, Harris R. The effectiveness and experience of self-management following acute coronary syndrome: a review of the literature. Int J Nurs Stud. 2016;61:29–51.
8. Schulman-Green D, Jaser S, Martin F, et al. Processes of self-management in chronic illness. J Nurs Scholarship. 2012;44(2):136–144. doi:10.1111/jnu.2012.44.issue-2
9. Bidwell JT, Vellone E, Lyons KS, et al. Determinants of heart failure self-care maintenance and management in patients and caregivers: a dyadic analysis. Res Nurs Health. 2015;38(5):392–402. doi:10.1002/nur.21675
10. Hurt CS, Burn DJ, Hindle J, et al. Thinking positively about chronic illness: an exploration of optimism, illness perceptions and well-being in patients with Parkinson’s disease. Br J Health Psychol. 2014;19(2):363–379. doi:10.1111/bjhp.12043
11. Wingham J, Harding G, Britten N, et al. Heart failure patients’ attitudes, beliefs, expectations and experiences of self-management strategies: a qualitative synthesis. Chronic Illn. 2014;10(2):135–154. doi:10.1177/1742395313502993
12. Alefishat EA, Abu Farha RK, Al-Debei M. Self-reported adherence among individuals at high risk of metabolic syndrome: effect of knowledge and attitude. Med Princ Pract 2017;26:157–163. doi:10.1177/1753193416669262
13. Jaam M, Hadi MA, Kheir N, et al. A qualitative exploration of barriers to medication adherence among patients with uncontrolled diabetes in Qatar: integrating perspectives of patients and health care providers. Patient Prefer Adherence. 2018;12:2205. doi:10.2147/PPA
14. Hartayu TS, Mi MI, Suryawati S. Improving of type 2 diabetic patients’ knowledge, attitude and practice towards diabetes self-care by implementing community-based interactive approach-diabetes mellitus strategy. BMC Res Notes. 2012;5(1):315. doi:10.1186/1756-0500-5-315
15. Mosleh SM, Almalik MMA. Illness perception and adherence to healthy behaviour in Jordanian coronary heart disease patients. Eur J Cardiovasc Nurs. 2016;15(4):223–230. doi:10.1177/1474515114563885
16. Zou H, Chen Y, Fang W, et al. Identification of factors associated with self-care behaviors using the COM-B model in patients with chronic heart failure. Eur J Cardiovasc Nurs. 2017;16(6):530–538. doi:10.1177/1474515117695722
17. Fitzpatrick AL, Steinman LE, Tu S-P, et al. Using photovoice to understand cardiovascular health awareness in Asian elders. Health Promot Pract. 2012;13(1):48–54. doi:10.1177/1524839910364381
18. Liu X-L, Willis K, Fulbrook P, et al. Factors influencing self-management priority setting and decision-making among Chinese patients with acute coronary syndrome and type 2 diabetes mellitus. Eur J Cardiovasc Nurs. 2019;18:700–710.
19. Aamodt IT, Lycholip E, Celutkiene J, et al. Health care professionals’ perceptions of home telemonitoring in heart failure care: cross-sectional survey. J Med Internet Res. 2019;21:e10362. doi:10.2196/10362
20. King AJL, Johnson R, Cramer H, et al. Community case management and unplanned hospital admissions in patients with heart failure: a systematic review and qualitative evidence synthesis. J Adv Nurs. 2018;74(7):1463–1473. doi:10.1111/jan.2018.74.issue-7
21. Sezgin D, Mert H, Özpelit E, et al. The effect on patient outcomes of a nursing care and follow-up program for patients with heart failure: a randomized controlled trial. Int J Nurs Stud. 2017;70:17–26.
22. Masupe TK, Ndayi K, Tsolekile L, et al. Redefining diabetes and the concept of self-management from a patient’s perspective: implications for disease risk factor management. Health Educ Res. 2018;33(1):40–54. doi:10.1093/her/cyx077
23. Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving chronic illness care: translating evidence into action. Health Aff. 2001;20(6):64–78. doi:10.1377/hlthaff.20.6.64
24. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
25. Creswell JW, Miller DL. Determining validity in qualitative inquiry. Theory Pract. 2000;39(3):124–130. doi:10.1207/s15430421tip3903_2
26. Franklin M, Lewis S, Willis K, et al. Patients’ and healthcare professionals’ perceptions of self-management support interactions: systematic review and qualitative synthesis. Chronic Illn. 2018;14(2):79–103. doi:10.1177/1742395317710082
27. Starfield B, Hyde J, Gervas J, et al. The concept of prevention: a good idea gone astray? J Epidemiol Community Health. 2008;62(7):580–583. doi:10.1136/jech.2007.071027
28. Andrew S, Blumenthal JA, Koch GG, et al. Effects of coping skills training on quality of life, disease biomarkers, and clinical outcomes in patients with heart failure. Circulation. 2017;10(1):e003410.
29. Ha Dinh TT, Bonner A, Clark R, et al. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: a systematic review. JBI Database Syst Rev Implement Rep. 2016;14(1):210–247. doi:10.11124/jbisrir-2016-2296
30. Harkness K, Spaling MA, Currie K, et al. A systematic review of patient heart failure self-care strategies. J Cardiovasc Nurs. 2015;30(2):121–135.
31. Li -C-C, Shun S-C. Understanding self care coping styles in patients with chronic heart failure: a systematic review. Eur J Cardiovasc Nurs. 2016;15(1):12–19. doi:10.1177/1474515115572046
32. Lilly CL, Bryant LL, Leary JM, et al. Evaluation of the effectiveness of a problem-solving intervention addressing barriers to cardiovascular disease prevention behaviors in 3 underserved populations: Colorado, North Carolina, West Virginia, 2009. Prev Chronic Dis. 2014;11:E32. doi:10.5888/pcd11.130249
33. Warren N, Canaway R, Unantenne N, et al. Taking control: complementary and alternative medicine in diabetes and cardiovascular disease management. Health (London). 2013;17(4):323–339. doi:10.1177/1363459312460699
34. Sethares KA, Asselin ME. The effect of guided reflection on heart failure self-care maintenance and management: a mixed methods study. Heart Kung. 2017;192–198. doi:10.3389/fphys.2017.00192
35. Miller MM, Rohan JM, Delamater A, et al. Changes in executive functioning and self-management in adolescents with type 1 diabetes: a growth curve analysis. J Pediatr Psychol. 2012;38(1):18–29. doi:10.1093/jpepsy/jss100
36. Jeon Y-H, Essue B, Jan S, et al. Economic hardship associated with managing chronic illness: a qualitative inquiry. BMC Health Serv Res. 2009;9(1):182. doi:10.1186/1472-6963-9-182
37. Terauchi Y, Ozaki A, Zhao X, et al. Humanistic and economic burden of cardiovascular disease related comorbidities and hypoglycaemia among patients with type 2 diabetes in Japan. Diabetes Res Clin Pract. 2019;149:115–125.
38. Palaya J, Pearson S, Nash T. Perception of social support in individuals living with a diabetic foot: a qualitative study. Diabetes Res Clin Pract. 2018;146:267–277.
39. Clayton C, Motley C, Sakakibara B. Enhancing social support among people with cardiovascular disease: a systematic scoping review. Curr Cardiol Rep. 2019;21(10):123. doi:10.1007/s11886-019-1216-7
40. Lee CS, Gelow JM, Mudd JO, et al. Profiles of self-care management versus consulting behaviors in adults with heart failure. Eur J Cardiovasc Nurs. 2015;14(1):63–72. doi:10.1177/1474515113519188
41. Wierenga KL, Lehto RH, Given B. Emotion regulation in chronic disease populations: an integrative review. Res Theory Nurs Pract. 2017;31(3):247–271. doi:10.1891/1541-6577.31.3.247
42. Delea S, Buckley C, Hanrahan A, et al. Management of diabetic foot disease and amputation in the Irish health system: a qualitative study of patients’ attitudes and experiences with health services. BMC Health Serv Res. 2015;15(1):251. doi:10.1186/s12913-015-0926-9
43. Frith CD, Frith U. How we predict what other people are going to do. Brain Res. 2006;1079:36–46.
44. Welstand J, Carson A, Rutherford P. Living with heart failure: an integrative review. Int J Nurs Stud. 2009;46:1374–1385.
45. Whitehead L, Jacob E, Towell A, et al. The role of the family in supporting the self-management of chronic conditions: a qualitative systematic review. J Clin Nurs. 2018;27(1–2):22–30. doi:10.1111/jocn.2018.27.issue-1pt2
46. Brittain K, Taylor JY, Wu CY. Family adaptability and cohesion and high blood pressure among urban African American women. J Nurse Pract. 2010;6(10):786–793. doi:10.1016/j.nurpra.2010.02.005
47. Currie K, Strachan PH, Spaling M, et al. The importance of interactions between patients and healthcare professionals for heart failure self-care: a systematic review of qualitative research into patient perspectives. Eur J Cardiovasc Nurs. 2015;14(6):525–535. doi:10.1177/1474515114547648
48. Dyer J. How does spirituality affect physical health?: a conceptual review. Holist Nurs Pract. 2007;21(6):324–328. doi:10.1097/01.HNP.0000298617.27008.be
49. Unantenne N, Warren N, Canaway R, et al. The strength to cope: spirituality and faith in chronic disease. J Relig Health. 2013;52(4):1147–1161. doi:10.1007/s10943-011-9554-9
50. Free C, Phillips G, Galli L, et al. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: a systematic review. PLoS Med. 2013;10(1):e1001362–e1001362. doi:10.1371/journal.pmed.1001362
51. Piette JD, List J, Rana GK, et al. Mobile health devices as tools for worldwide cardiovascular risk reduction and disease management. Circulation. 2015;132(21):2012–2027. doi:10.1161/CIRCULATIONAHA.114.008723
52. Piette JD, Striplin D, Marinec N, et al. A mobile health intervention supporting heart failure patients and their informal caregivers: a randomized comparative effectiveness trial. J Med Internet Res. 2015;17(6):e142. doi:10.2196/jmir.4550
53. Nordin C, Michaelson P, Eriksson MK, et al. It’s about me: patients’ experiences of patient participation in the web behavior change program for activity in combination with multimodal pain rehabilitation. Int Med Internet Res. 2017;19:e22.
54. Petersen M, Hempler NF. Development and testing of a mobile application to support diabetes self-management for people with newly diagnosed type 2 diabetes: a design thinking case study. BMC Med Inform Decis Mak. 2017;17(1):91. doi:10.1186/s12911-017-0493-6
55. Putnam RD. Bowling alone: America’s declining social capital. In: Crothers L, Lockhart C, editors. Culture and Politics: A Reader. New York: Palgrave Macmillan US; 2000:223–234.
56. Hu F, Hu B, Cehn R, et al. A systematic review of social capital and chronic non-communicable diseases. Biosci Trends. 2014;8(6):290–296. doi:10.5582/bst.2014.01138
57. Winkleby MA, Jatulis DE, Frank E, et al. Socioeconomic status and health: how education, income, and occupation contribute to risk factors for cardiovascular disease. Am J Public Health. 1992;82(6):816–820. doi:10.2105/AJPH.82.6.816
58. Liu X, Lu H, Wang Y, et al. Factors affecting patient satisfaction with ecdemic medical care: a cross-sectional study in nanchang, china. Patient Prefer Adherence. 2018;12:1373. doi:10.2147/PPA.S167244
59. Röttger J, Blümel M, Linder R, et al. Health system responsiveness and chronic disease care – what is the role of disease management programs? An analysis based on cross-sectional survey and administrative claims data. Social Sci Med. 2017;185:54–62.
60. Zhu W, Li H, Xia H, et al. Inequalities in structural social capital and health between migrant and local hypertensive patients. Ann Global Health. 2019;85(1):48. doi:10.5334/aogh.2398
61. Zeng Y, Wu J, Han Y, et al. Educational disparities in the associations between self-monitoring of blood glucose and glycemic control in type 2 diabetes patients in Xiamen, China. J Diabetes. 2018;10(9):715–723. doi:10.1111/jdb.2018.10.issue-9
62. Hu D, Zhu W, Fu Y, et al. Development of village doctors in China: financial compensation and health system support. Int J Equity Health. 2017;16(1):9. doi:10.1186/s12939-016-0505-7
63. He X, Li L, Bian Y. Satisfaction survey among primary health care outpatients in the backward region: an empirical study from rural Western China. Patient Prefer Adherence. 2018;12:1989. doi:10.2147/PPA.S172021
64. Wang C, Lang J, Xuan L, et al. The effect of health literacy and self-management efficacy on the health-related quality of life of hypertensive patients in a western rural area of China: a cross-sectional study. Int J Equity Health. 2017;16(1):58. doi:10.1186/s12939-017-0551-9
65. Long E, Ponder M, Bernard S. Knowledge, attitudes, and beliefs related to hypertension and hyperlipidemia self-management among African-American men living in the southeastern United States. Patient Educ Couns. 2017;100:1000–1006.
66. Davidson PM, Daly J, Leung D, et al. Health-seeking beliefs of cardiovascular patients: a qualitative study. Int J Nurs Stud. 2011;48:1367–1375.
67. Manderson L, Canaway R, Unantenne N, et al. Care seeking, use of complementary therapies and self management among people with type 2 diabetes and cardiovascular disease. CAMELOT Phase I: an ethnographic approach. Aust J Herbal Med. 2012;24(1):10–18.
68. Shen H, Edwards H, Courtney M, et al. Barriers and facilitators to diabetes self-management: perspectives of older community dwellers and health professionals in China. Int J Nurs Pract. 2013;19(6):627–635. doi:10.1111/ijn.12114
69. Lamore K, Montalescot L, Untas A. Treatment decision-making in chronic diseases: what are the family members’ roles, needs and attitudes? A systematic review. Patient Educ Couns. 2017;100:2172–2181. doi:10.3389/fmicb.2017.02172
70. Mao A, Bristow K, Robinson J. Caught in a dilemma: why do non-smoking women in China support the smoking behaviors of men in their families? Health Educ Res. 2012;28(1):153–164. doi:10.1093/her/cys078
71. Du S, Neiman A, Batis C, et al. Understanding the patterns and trends of sodium intake, potassium intake, and sodium to potassium ratio and their effect on hypertension in China. Am J Clin Nutr. 2013;99(2):334–343. doi:10.3945/ajcn.113.059121
72. Ma G. Food, eating behavior, and culture in Chinese society. J Ethnic Foods. 2015;2:195–199.
73. Albarracín D, Wyer RSJ. The cognitive impact of past behavior: influences on beliefs, attitudes, and future behavioral decisions. J Pers Soc Psychol. 2000;79(1):5–22. doi:10.1037/0022-3514.79.1.5
74. Chun KM, Chesla CA, Kwan CML. “So We Adapt Step by Step”: acculturation experiences affecting diabetes management and perceived health for Chinese American immigrants. Social Sci Med. 2011;72:256–264.
75. Zhang L, Liu S, Zhang G, et al. Internal migration and the health of the returned population: a nationally representative study of China. BMC Public Health. 2015;15(1):719. doi:10.1186/s12889-015-2074-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.