Back to Journals » Psychology Research and Behavior Management » Volume 13
Childhood Maltreatment, Negative Self-Referential Processing, and Depressive Symptoms During Stress
Authors Jopling E ![]() , Tracy A
, Tracy A ![]() , LeMoult J
, LeMoult J
Received 18 September 2019
Accepted for publication 17 December 2019
Published 14 January 2020 Volume 2020:13 Pages 79—87
DOI https://doi.org/10.2147/PRBM.S231505
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ellen Jopling, Alison Tracy, Joelle LeMoult
Department of Psychology, University of British Columbia, Vancouver, BC, Canada
Correspondence: Ellen Jopling
Department of Psychology, University of British Columbia, 2136 West Mall, Vancouver V6T1Z4, BC, Canada
Tel +1-604-916-6269
Email [email protected]
Introduction: Researchers have documented that the impact of childhood maltreatment on later symptoms of depression differs depending on the type(s) of maltreatment experienced, with emotional abuse and neglect being more likely than other forms of childhood maltreatment to increase the risk for depression. It is possible that emotional abuse and neglect are more likely to increase the risk for depression because they promote the development of negative self-referential processing (SRP), but this has not yet been tested empirically. The current study was designed to examine whether negative SRP mediated the association between different forms of childhood maltreatment and symptoms of depression during a time of stress.
Methods: We assessed the experience of different forms of childhood maltreatment (ie, emotional neglect, physical neglect, emotional abuse, physical abuse, and sexual abuse) and negatively biased self-schemas early on in the university semester, among a sample of undergraduate students. We then assessed levels of depressive symptoms 2 months later during a naturalistic stressor (ie, university students’ first final exams).
Results: As expected, negative SRP mediated the relation between both neglect and emotional abuse, but not physical and sexual abuse, and later symptoms of depression.
Discussion: This is the first study to examine SRP as a mechanism underlying the association between forms of childhood maltreatment and symptoms of depression during a time of stress. Results suggest that the development of negative SRP biases may explain why some types of childhood maltreatment are more likely than others to increase an individual’s risk for depression during stressful developmental periods.
Keywords: depression, childhood maltreatment, self-referential processing
Childhood maltreatment is associated with an increased risk for the development of persistent, treatment-resistant depression in adulthood.1 In fact, researchers posit that childhood maltreatment contributes to as many as 50% of depression cases worldwide.2,3 Importantly, current research suggests that certain types of childhood maltreatment are more likely than others to lead to symptoms of depression later in life.1,4 Whereas early studies suggested that individuals exposed to more physical forms of abuse (ie, physical abuse and sexual abuse) were at a higher risk of developing depression than those who experienced other forms of abuse,5 results from more recent meta-analyses suggest that emotional abuse and neglect are most strongly associated with the later development of depression,6–8 particularly during times of stress.9
One reason that emotional abuse and neglect are more likely than other types of maltreatment to increase the risk for depression may be that emotional abuse and neglect are more likely to promote the development of negative self-schemas, negative and stable beliefs and patterns of thinking about oneself.10,11 Importantly, negative self-schemas are distinct from negative cognitive styles more broadly as they specifically involve negative beliefs and attributions regarding the self and are thought to be more strongly associated with depression than other forms of negative cognitive schema.12
Consistent with cognitive models of psychopathology, researchers have documented that childhood maltreatment is associated with negative self-schemas, and as would be expected, this is most commonly observed for forms of maltreatment that are not associated with overt physical threat.13 Sachs-Ericsson, Verona, Joiner, and Preacher argued that victims of emotional abuse receive negative messages about their self-worth, which leads to the creation and maintenance of negative self-schemas.14 Similarly, Steinberg, Gibb, Alloy, and Abramson suggested that negative self-schemas develop in individuals with a history of emotional abuse because they become hypervigilant towards instances of emotional rejection, the internalization of which leads to the expectation that future experiences will be in line with their negative core self-beliefs.15 Importantly, although it has never been explicitly examined, there is also reason to expect that both emotional neglect and physical neglect promote negative self-schemas. Emotional and physical neglect may convey implicit messages that victims are not deserving of care and attention, which in turn, may contribute to the development of negative self-schemas or, at the very least, may prevent the development of positive beliefs about the self.16
In turn, negative cognitive biases relating to the self are thought to be inherently related to the onset and maintenance of depression.10 Indeed, the association between negative self-schemas and depressive symptoms has received empirical support.17–19 For instance, researchers have documented that negative self-schemas predict a more pernicious course of depressive symptoms involving the recurrence of depressive episodes, particularly in the context of stressful life events.19 However, much of this literature is limited by the use of self-report measures (eg, the Young Schema Questionnaire) and cross-sectional designs.20
In sum, there is empirical evidence that some forms of childhood maltreatment lead to the development of negative self-schemas, and in a separate literature, negative self-schemas have been associated with depression. Critically, however, it is unclear whether and to what extent negatively biased self-referential processing (SRP) might be a mechanism through which each form of childhood maltreatment is associated with depressive symptomatology.
In response to this gap in the literature, the current study was designed to examine whether negative self-schemas mediate the association between each form of childhood maltreatment and symptoms of depression during a time of stress. This question was investigated in a sample of emerging adults, who have the highest cumulative prevalence and incidence rates of depression of any age group.21,22 Further, the impact of self-schemas on wellbeing may be particularly strong in this cohort as emerging adulthood represents a time during which one’s identity is explored and significant development in interpersonal domains occurs.23 We first assessed the experience of different types of childhood maltreatment (ie, emotional neglect, physical neglect, emotional abuse, physical abuse, and sexual abuse) and negatively biased self-schemas early on in the university semester (Time 1). In order to assess self-schemas specifically and to overcome the limitations of self-report measures of self-schemas (including recall, demand and reference biases), negative self-schemas were measured using the well-validated self-referential encoding task,24 which provides an index of negatively biased SRP. Given evidence of a robust association between stressful life events and the development of depression, we assessed symptoms of depression during a particularly stressful and ecologically valid period: university students’ first final exams (Time 2).25,26 We expected that the relation between childhood maltreatment and symptoms of depression would be mediated by negatively biased SRP for neglect (both emotional and physical) and emotional abuse, but not for physical abuse and sexual abuse.
Method
Participants
Using GPower 3.1, it was determined via a power analysis based on a moderate effect size of f2 =0.15 that a sample of 99 participants would be required to detect differences at α = 0.05 and power = 90%. However, given the longitudinal nature of the study design (with the potential for attrition), recruitment remained active across the entire first 3 weeks of the university semester. Therefore, the current sample consisted of 160 undergraduate students (85.6% female) who were entering their first year of university. Participants were recruited during the first 3 weeks of the semester via the University of British Columbia’s Human Subject Pool. Written informed consent was obtained from all participants included in the study, and all study procedures were conducted in accordance with the Declaration of Helsinki. The mean age of the sample was 18.29 years (SD = 0.86). Participants self-identified as the following ethnicities: 59.4% Asian, 25.6% Caucasian, 3.8% Latino, 0.6% Canadian Indigenous, and 0.6% Native Hawaiian/Pacific Islander.
Cognitive Task
Self-Schemas
We assessed participants negative self-schemas using the SRET presented via E-Prime 2.0.24 The SRET consisted of 40 adjectives, 20 of which were positively valenced and 20 of which were negatively valenced. Each trial began with the phrase “Describes me?” presented for 500 ms in the middle of the screen. Next, a blank screen appeared for 250 ms, following which an adjective was presented in the middle of the screen. Adjectives were presented in random order, and participants pressed the key corresponding to “yes” or “no” to indicate whether or not the word described them. Finally, a fixation cross was presented for 1000 ms in the middle of the screen. Immediately following, participants worked on a distractor task for 3 mins. Lastly, participants were asked to write down as many words as they could recall from the SRET, regardless of whether or not the word was endorsed as self-descriptive.
Four variables were obtained based on participants’ performance on the SRET: the number of positive and negative words endorsed as self-descriptive, and the number of endorsed positive and negative adjectives that were recalled. In line with previous research,19,27,28 we computed an SRP bias score based on the number of negative words endorsed and recalled as a proportion of the total number of words endorsed and recalled in order to control for individual differences in overall rates of endorsement and recall.
There is significant evidence that individuals at risk of developing depression and those who have already developed depression are characterized by negative schemas that are activated by negative events or negative mood.29,30 Thus, because cognitive biases can remain latent until they are triggered (for example, by a negative mood state), a negative mood was induced immediately before participants completed the SRET.31 Specifically, participants were instructed to watch one of three randomly assigned six-minute film clips using procedures described in LeMoult et al:19 My Girl, which depicts an adolescent girl learning that her best friend has died;32 Stepmom, which depicts a young son and daughter saying goodbye to their terminally ill mother;33 and Dead Poets Society, which depicts an adolescent boy learning that his best friend has completed suicide.34 To ensure the efficacy of the negative mood induction, self-reported negative affect was assessed via the Positive and Negative Affect Scale (PANAS) immediately prior and following the viewing of the film clip.35 The PANAS has good internal consistency (α = 0.85) and test–retest reliability (r = 0.87). Internal consistency was also acceptable in the present study (αs > 0.79).
Self-Report Measures
Childhood Trauma
Participants completed the Childhood Trauma Questionnaire to assess history of childhood maltreatment.36 The CTQ is a 28-item questionnaire consisting of five subscales (five items each assessing emotional neglect, physical neglect, emotional abuse, physical abuse, and sexual abuse) and three validity items. Items for each form of maltreatment were summed to yield five subscale scores, which in turn were summed to create a total score. The CTQ is one of the most commonly used scales to assess experiences of childhood maltreatment, and it has excellent internal consistency (α = 0.96) and good test–retest reliability (r = 0.85) among university populations.37 There was also excellent internal consistency in the current study (α = 0.91).
Symptoms of Depression
Participants completed the 21-item Beck Depression Inventory-II to assess the severity of their depressive symptoms during the past 2 weeks.38 The BDI-II is one of the most widely used assessment tools for self-reported symptoms of depression, and has excellent internal consistency (α = 0.91) and test–retest reliability.38–40 There was also good internal consistency in the current study (α = 0.88).
Covariates
Consistent with recent publications,41 in order to provide a more rigorous test of the relations among childhood maltreatment, negative self-schemas, and symptoms of depression, in all models we included age, sex, and depression history as covariates. Depression history was assessed via participants’ self-report of having ever received a diagnosis of depression from a health professional.
Procedures
Participants came to the laboratory to complete an initial study session within the first 3 weeks of beginning university. After providing informed consent, participants completed a negative mood induction, followed immediately by the SRET. A positive mood clip, Milo and Otis,42 which depicts puppies and kittens playing in a field, was shown after the completion of the SRET and prior to the completion of the questionnaires. Participants then reported on their history of childhood maltreatment (CTQ) and relevant covariates including age, sex, and history of depression. To examine whether these variables could predict symptoms of depression during a time of increased stress, participants reported on their level of depressive symptoms (BDI-II) during their first final exam period, approximately 2 months later, online via Qualtrics.
Results
Descriptive Statistics and Preliminary Analyses
Of the 160 participants who completed the Time 1 session, 6 were lost to follow-up. These individuals did not differ from those who completed Time 2 with respect to age, sex, racial group, depression history, or experience of childhood maltreatment, ps > 0.05. Bivariate correlations between all variables are presented in Supplemental Table 1.
Mood Induction
To examine the effectiveness of the mood induction, a repeated-measures analysis of variance (ANOVA) was conducted on self-reported negative affect, as measured by the PANAS. As expected, results indicated a significant main effect of time, F(1, 157) = 54.08, p < 0.001, with participants reporting an increase in their negative affect from before (M = 15.32, SD = 4.85) to after watching the negative film clip (M = 18.56, SD = 6.55).
SRET (Time 1)
Participants endorsed as self-referential an average of 13.39 (SD = 4.50) positive words and 7.13 (SD = 3.56) negative words on the SRET. Following the filler task, participants recalled an average of 5.58 (SD = 2.48) of the positive words that were endorsed and 2.36 (SD = 1.66) of the negative words that were endorsed, yielding an average negative SRP score of 0.30 (SD = 0.21; using the formula put forth by Gotlib et al).43
Childhood Trauma (Time 1)
The average total CTQ maltreatment score within our sample was 30.89 (SD = 9.00). 114 participants (71%) endorsed having experienced some degree of maltreatment during childhood. Of these 114 participants, 39% endorsed having experienced some degree of emotional neglect; 13.8% endorsed having experienced some degree of physical neglect; 57.5% endorsed having experienced some degree of emotional abuse; 37% endorsed having experienced some degree of physical abuse; and 6.3% endorsed having experienced some degree of sexual abuse. These prevalence rates are in line with previous findings in the university population.37
Symptoms of Depression (Time 2)
The average score on the BDI-II was 14.31 (SD=10.98). Of the 154 participants who completed the T2 session, 90 (58.44%) had depressive symptoms within the minimal range (score of 0–13), 21 (13.64%) within the mild range (score of 14–19), 26 (16.88%) within the moderate range (score of 20–28), and 17 (11.04%) within the severe range (score of 29–63) based on cut-offs defined by Beck, Steer, and Brown.38
Main Analyses
To examine whether performance on the SRET mediated the association between childhood maltreatment and later symptoms of depression, we conducted a series of bias-corrected bootstrapped mediation analyses using CTQ total score as well as each of the CTQ subscales as predictors, SRP bias as the mediator, and depressive symptomatology as the outcome. Age, sex, and depression history were included as covariates in all analyses, as is consistent with previous research. Exploratory analyses indicated that these variables did not significantly interact with negative SRP bias to predict variance in later symptoms of depression, R2change = 0.044, p > 0.05. Thus, moderated mediation models were not pursued.
Continuous variables were z-scored, and mediation analyses were performed using the PROCESS macro for SPSS. All PROCESS commands are presented in the supplement. Estimates include bootstrapped standard errors and 95% bootstrapped confidence intervals (CI; based on 5000 bootstrap samples). To quantify the relative magnitude of effects, percent mediation (a measure of effect size) was calculated for all mediation models following guidelines set forth by Preacher and Kelley and is interpreted as the percent of the total effect accounted for by the indirect effect.44 Direct and indirect effects for all models are presented in Table 1, and beta coefficients can be found in Supplemental Table 2 and in Supplemental Figures 1–6.
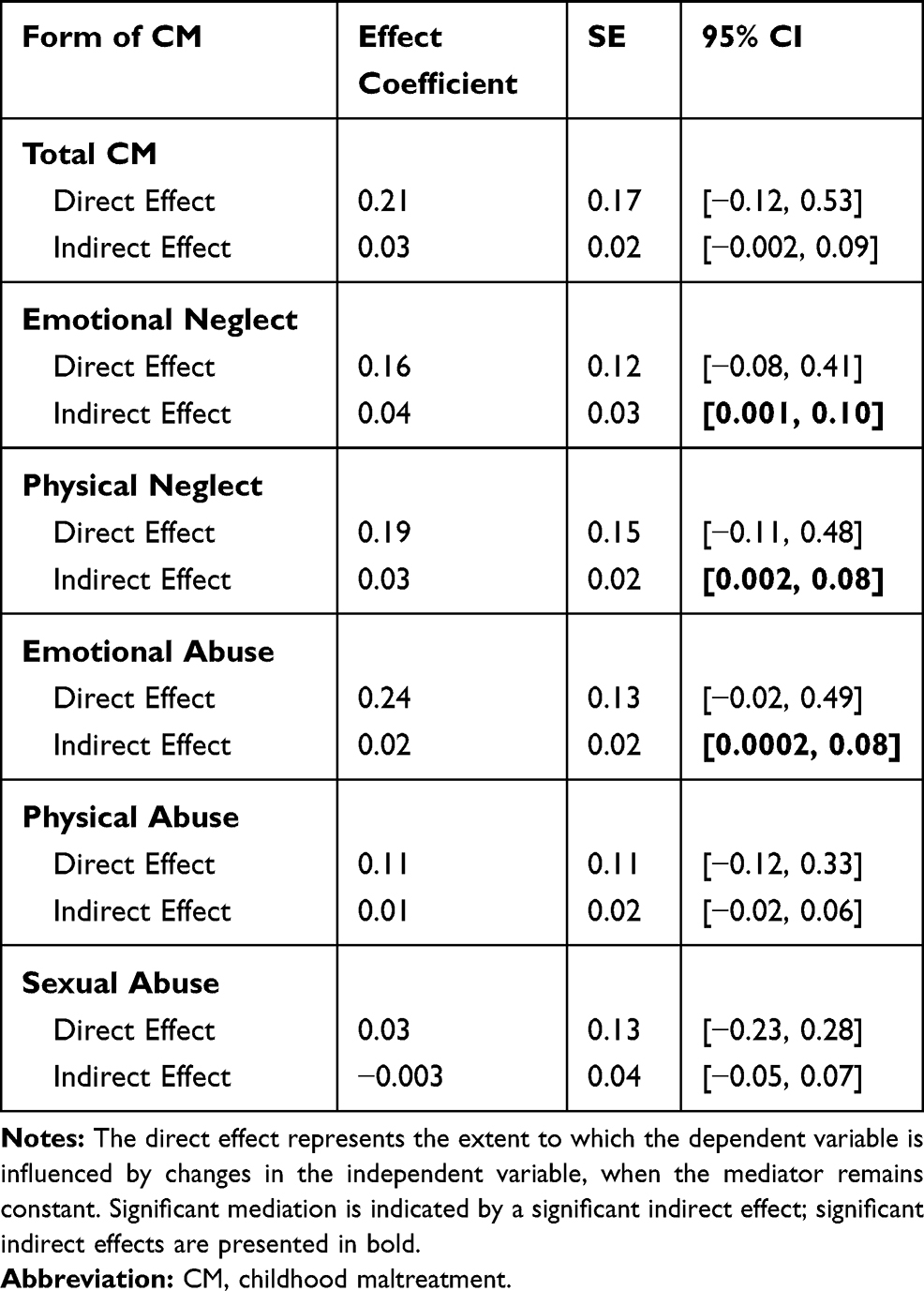 |
Table 1 Direct and Indirect Effects of Forms of Childhood Maltreatment on Symptoms of Depression for All Mediation Models |
As expected, SRP biases mediated the association between both forms of neglect and emotional abuse, but not physical and sexual abuse, and later symptoms of depression. Specifically, SRP fully mediated the association between emotional neglect and symptoms of depression, indirect effect = 0.04, SE = 0.03, 95% CI [0.001, 0.10]. When negative SRP biases were included in the model, the association between emotional neglect and symptoms of depression was no longer significant, β = 0.16, SE = 0.12, t(148) = 1.33, p = 0.185. Effect size analyses indicated that SRP biases accounted for approximately 19% of the total effect between emotional neglect and later symptoms of depression, PM = 0.186.
SRP also fully mediated the association between physical neglect and symptoms of depression, indirect effect = 0.03, SE = 0.02, 95% CI [0.002, 0.08]. When negative SRP biases were included in the model, the association between physical neglect and symptoms of depression was no longer significant, β = 0.19, SE = 0.15, t(149) = 1.26, p = 0.209. SRP biases accounted for approximately 14% of the total effect between physical neglect and later symptoms of depression, PM = 0.144.
SRP also mediated the association between emotional abuse and symptoms of depression, indirect effect = 0.02, SE = 0.02, 95% CI [0.0002, 0.08]. When negative SRP biases were included in the model, the association between emotional abuse and symptoms of depression was significant at a trend level, β = 0.24, SE = 0.13, t(149) = 1.80, p = 0.073. SRP biases accounted for approximately 9% of the total effect between emotional abuse and later symptoms of depression, PM = 0.092.
In contrast, SRP biases did not mediate the relation between total level of childhood maltreatment and later symptoms of depression, indirect effect = 0.03, SE = 0.02, 95% CI [−0.002, 0.09]. When negative SRP biases were included in the model, the association between total level of childhood maltreatment and symptoms of depression was not significant, β = 0.21, SE = 0.17, t(148) = 1.24, p = 0.216. SRP biases accounted for approximately 12% of the total effect between total level of childhood maltreatment and symptoms of depression, PM = 0.092.
SRP biases also did not mediate the relation between childhood physical abuse and later symptoms of depression, indirect effect = 0.01, SE = 0.02, 95% CI [−0.02, 0.06]. When negative SRP biases were included in the model, the association between childhood physical abuse and symptoms of depression was not significant, β = 0.11, SE = 0.11, t(149) = 0.94, p = 0.347. SRP biases accounted for approximately 9% of the total effect between physical abuse and symptoms of depression, PM = 0.089.
Finally, SRP biases did not mediate the association between childhood sexual abuse and symptoms of depression, indirect effect = −0.003, SE = 0.04, 95% CI [−0.05, 0.07]. When negative SRP biases were included in the model, the association between childhood physical abuse and symptoms of depression was not significant, β = 0.03, SE = 0.13, t(149) = 0.19, p = 0.850. The direct effect (c’-path) was larger than the total effect (c-path), suggestive of a suppression effect. Therefore, following guidelines put forth by Shrout and Bolger, percent mediation was not computed.45
Discussion
This is the first study to examine SRP as a mechanism underlying the association between multiple forms of childhood maltreatment and later symptoms of depression during a time of stress. Importantly, we found differential effects of SRP biases based on the type of childhood maltreatment experienced. Whereas negative SRP biases mediated the relation between emotional neglect, physical neglect, emotional abuse, and symptoms of depression, SRP biases did not significantly mediate the relation between physical abuse or sexual abuse and symptoms of depression. These findings are critical to furthering our understanding of the mechanisms through which different forms of childhood maltreatment increase the risk for later depressive symptoms, and to helping us to understand why some forms of childhood maltreatment are more likely than others to increase the risk for depression.
The extant literature suggests that emotional forms of childhood maltreatment may be more likely than physical forms of childhood maltreatment to increase the risk for later symptoms of depression, though it should be noted that physical and sexual abuse are often less frequently endorsed, which can artificially attenuate the strength of their association with depression.6 Although little is known about the mechanisms through which different forms of maltreatment confer risk for depression, findings from the current study support the proposition that negative self-schemas serve as a mechanism through which emotional abuse and neglect are associated with symptoms of depression. Our findings are consistent with evidence from Crawford and Wright, who found that the experience of psychological maltreatment (ie, emotional abuse and neglect) during childhood was associated with later schemas of low self-esteem and self-deprecation.46 Our findings are also consistent with past studies that have documented that maladaptive schemas considered more broadly (eg, schemas regarding loss and danger) are associated cross-sectionally with both childhood trauma and depressive symptoms.47
One possible reason that negative self-schemas mediate the association between emotional abuse and neglect and later symptoms of depression is that emotional abuse and neglect during childhood promote feelings of shame. Although Loader argued that children who are abused are likely to experience a “pervasive, and often life-long, sense of shame” regardless of the form of mistreatment, evidence suggests that emotional maltreatment is most likely to encourage the development of a deeply rooted sense of shame because it produces negative feelings about ones global, stable self– similar cognitions to those that are associated with a negative SRP bias.48,49 Consistent with this theory, children with rejecting parents (ie, emotionally abusive and/or neglectful) or a history of childhood psychological maltreatment are more prone to the experience of shame, which in turn is associated with higher levels of depression during the adolescent period.50 Evidence suggests that emotional forms of maltreatment promote the development of shame because negative cognitions are communicated to the child either verbally (in the case of emotional abuse) or non-verbally (in the case of neglect).51 Shame may, in turn, contribute to the manifestation of negative self-schemas because it promotes the development of an ingrained, negative view of the self.49 However, other forms of childhood maltreatment (eg, childhood sexual abuse) have also been linked to feelings of shame among survivors and, as such, future work ought to examine the complex associations between forms of childhood maltreatment, shame, SRP biases, and depression.
In the present study, the indirect effects of childhood physical abuse and childhood sexual abuse on symptoms of depression were not significant. We also found that the first-order correlations between these forms of childhood maltreatment and symptoms of depression were not significant (see Supplemental Table 1). Although earlier work has documented that individuals exposed to physical abuse or sexual abuse are at higher risk of developing depression than those who experienced other forms of abuse,5 more recent work has been mixed. For example, recent meta-analyses showed that emotional abuse and neglect were associated with greater risk for depression than were physical and sexual abuse,7,52 and other studies have reported nonsignificant associations between both physical and sexual abuse with depressive symptoms.53,54 That being said, as noted above, physical abuse and sexual abuse are often less frequently endorsed than other forms of maltreatment, and lower prevalence rates can attenuate the strength of their association with depression. Researchers have also posited that among individuals with a history of physical abuse and sexual abuse, distress may manifest in other ways, as these forms of abuse increase risk for other forms of psychopathology, namely posttraumatic stress disorder (PTSD) or sexual promiscuity, particularly in younger samples.52,55 Clearly, further work is required to further elucidate these complex associations.
We would like to note several limitations of our research. First, we relied on participants’ self-reported history of childhood maltreatment. Although it has been documented that individuals may deny instances of childhood abuse and neglect or may have difficulty remembering early maltreatment, on the whole, research has shown that adults’ recall of childhood events is reasonably accurate.56 Further, despite evidence that mood state may influence self-reported memory of experienced events, this effect is likely much smaller than has been suggested previously.56 Second, while the inclusion of a university sample was advantageous insofar as we were able to take advantage of a naturalistic and ecologically valid stressor, it is important to acknowledge the limitations associated with the study of depression in this population. In particular, our sample may represent a high-functioning cohort, and as such our findings may not generalize to emerging adults more broadly. However, given the prevalence of childhood maltreatment in the population and of depression among university students,57,58 it remains important to examine mechanisms through which childhood maltreatment contributes to depression in this population. Nonetheless, future research should replicate the present study in a community sample of emerging adults. Third, symptoms of PTSD were not assessed in the present study. Given documented associations between depression and PTSD,59 it will be important for future work to consider the impact of PTSD symptomatology on the observed associations between childhood maltreatment, SRP biases, and symptoms of depression during stress. Finally, though history of depression was controlled for in all mediation analyses, the absence of a formal assessment of depressive symptoms at Time 1 limits our ability to assess changes in depression across the first university semester. Future studies examining the impact of childhood maltreatment and SRP biases on changes in depression would help to further elucidate associations among these variables.
Despite these limitations, the current study offers an important contribution to theoretical models of psychopathology. This study connects several important areas of literature, both emerging (negative SRP and depression) and well-established (childhood maltreatment and the later development of symptoms of depression) in nature. Specifically, the present study suggests negatively biased SRP is a mechanism through which particular forms of childhood maltreatment influence individual differences in symptoms of depression during a stressful developmental period among a sample of emerging adults. Further, the current study extends past work by assessing self-schemas in particular, which we measured using a well-validated cognitive task, rather than negative cognitive styles or maladaptive schemas more generally. Doing so provides a more fine-grained understanding of the mechanisms through which childhood maltreatment influences the experience of depression later in life. Importantly, this fine-grained understanding is critical to the development of treatment protocols targeting mechanisms underlying depressive symptoms in the context of a history of childhood maltreatment.
Ethical Approval and Informed Consent
All procedures performed in the present study were approved by the University of British Columbia’s Behavioural Research Ethics Board (Study ID: H17-01585) and were conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study.
Data Sharing Statement
The raw data, analysis code, and materials used in this study are not openly available but are available upon request to the corresponding author.
Funding
This study was funded by the Social Sciences and Humanities Research Council (Grant N.: 430-2017-00408) awarded to Dr. Joelle LeMoult. The funding source was not involved in any stage of the research.
Disclosure
Dr Joelle LeMoult reports grants from the University of British Columbia. The authors report no other conflicts of interest in this work.
References
1. Teicher MH, Samson JA, Polcari A, McGreenery CE. Sticks, stones, and hurtful words: relative effects of various forms of childhood maltreatment. Am J Psychiatry. 2006;163(6):993–1000.
2. Li M, D’Arcy C, Meng X. Maltreatment in childhood substantially increases the risk of adult depression and anxiety in prospective cohort studies: systematic review, meta-analysis, and proportional attributable fractions. Psychol Med. 2016;46:717–730.
3. McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, Kessler RC. Childhood adversities and first onset of psychiatric disorders in a national sample of US adolescents. Arch Gen Psychiatry. 2012;69:1151.
4. Wells TT, Vanderlind WM, Selby EA, Beevers CG. Childhood abuse and vulnerability to depression: cognitive scars in otherwise healthy young adults. Cogn Emot. 2014;28(5):821–833.
5. Schraedley PK, Gotlib IH, Hayward C. Gender differences in correlates of depressive symptoms in adolescents. J Adolesc Health. 1999;25(2):98–108.
6. Infurna MR, Reichl C, Parzer P, Schimmenti A, Bifulco A, Kaess M. Associations between depression and specific childhood experiences of abuse and neglect: a meta-analysis. J Affect Disord. 2016;190:47–55.
7. Mandelli L, Petrelli C, Serretti A. The role of specific early trauma in adult depression: a meta-analysis of published literature. Childhood trauma and adult depression. Eur Psychiatry. 2015;30:665–680.
8. Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med. 2012;9:e1001349.
9. Shapero BG, Black SK, Liu RT, et al. Stressful life events and depression symptoms: the effect of childhood emotional abuse on stress reactivity. J Clin Psychol. 2014;70:209–223.
10. Beck AT. Depression: clinical, experimental, and theoretical aspects. JAMA. 1967.
11. Rose DT, Abramson LY. Developmental predictors of depressive cognitive style: research and theory. In
12. Phillips WJ, Hine DW, Thorsteinsson EB. Implicit cognition and depression: a meta-analysis. Clin Psychol Rev. 2010;30:691–709.
13. Segal ZV. Appraisal of the self-schema construct in cognitive models of depression. Psychol Bull. 1988;103(2):147–162.
14. Sachs-Ericsson N, Verona E, Joiner T, Preacher KJ. Parental verbal abuse and the mediating role of self-criticism in adult internalizing disorders. J Affect Disord. 2006;93(1–3):71–78.
15. Steinberg JA, Gibb BE, Alloy LB, Abramson LY. Childhood emotional maltreatment, cognitive vulnerability to depression, and self-referent information processing in adulthood: reciprocal relations. J Cogn Psychother. 2003;17(4):347–358.
16. Soffer N, Gilboa–Schechtman E, Shahar G. The relationship of childhood emotional abuse and neglect to depressive vulnerability and low self–efficacy. Int J Cogn Ther. 2008;1(2):151–162.
17. Disner SG, Shumake JD, Beevers CG. Self-referential schemas and attentional bias predict severity and naturalistic course of depression symptoms. Cogn Emot. 2017;31(4):632–644.
18. Kiang M, Farzan F, Blumberger DM, et al. Abnormal self-schema in semantic memory in major depressive disorder: evidence from event-related brain potentials. Biol Psychol. 2017;126:41–47.
19. LeMoult J, Kircanski K, Prasad G, Gotlib IH. Negative self-referential processing predicts the recurrence of major depressive episodes. Clin Psychol Sci. 2017;5(1):174–181.
20. Young JE, Brown G. Young schema questionnaire. In: Young JE, editor. Cognitive Therapy for Personality Disorders: A Schema-Focused Approach. 2nd ed. New York: Professional Resource Press/Professional Resource Exchange; 1994;63–76.
21. Kessler RC, Walters EE. Epidemiology of DSM-III-R major depression and minor depression among adolescents and young adults in the National Comorbidity Survey. Depress Anxiety. 1998;7:3–14.
22. Klerman GL, Weissman MM. Increasing rates of depression. JAMA. 1989;261:2229.
23. Arnett JJ. Emerging adulthood: what is it, and what is it good for? Child Dev Perspect. 2007;1:68–73.
24. Derry PA, Kuiper NA. Schematic processing and self-reference in clinical depression. J Abnorm Psychol. 1981;90(4):286–297.
25. Hammen CL. Stress and depression: old questions, new approaches. Curr Opin Psychol. 2014;4:2–7.
26. Tennant C. Life events, stress and depression: a review of recent findings. Aust N Z J Psychiatry. 2002;36:173–182.
27. Fritzsche A, Dahme B, Gotlib IH, et al. Specificity of cognitive biases in patients with current depression and remitted depression and in patients with asthma. Psychol Med. 2010;40:815–826.
28. Kircanski K, Mazur H, Gotlib IH. Behavioral activation system moderates self-referent processing following recovery from depression. Psychol Med. 2013;43:1909–1919.
29. Gilboa E, Gotlib IH. Cognitive biases and affect persistence in previously dysphoric and never-dysphoric individuals. Cogn Emot. 1997;11(5–6):517–538.
30. Teasdale JD, Dent J. Cognitive vulnerability to depression: an investigation of two hypotheses. Br J Clin Psychol. 1987;26(2):113–126.
31. Teasdale JD. Cognitive vulnerability to persistent depression. Cogn Emot. 1988;2(3):247–274.
32. Zieff H. My Girl. United States: Sony Pictures; 1991.
33. Columbus C. Stepmom. United States: Sony Pictures; 1998.
34. Weir P. Dead Poets Society. United States: Buena Vista/Touchstone; 1989.
35. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–1070.
36. Bernstein DP, Fink L. Childhood Trauma Questionnaire: A Retrospective Self-Report: Manual. The Psychological Corporation; 1998.
37. Paivio SC, Cramer KM. Factor structure and reliability of the childhood trauma questionnaire in a Canadian undergraduate student sample. Child Abuse Negl. 2004;28:889–904.
38. Beck AT, Steer RA, Brown GK. Beck Depression Inventory-II. San Antonio: Psychological Corporation; 1996.
39. Beck AT, Steer RA, Ball R, Ranieri WF. Comparison of Beck depression inventories -IA and -II in psychiatric outpatients. J Pers Assess. 1996;67:588–597.
40. Dozois DJA, Dobson KS, Ahnberg JL. A psychometric evaluation of the Beck depression inventory-II. Psychol Assess. 1998;10:83.
41. Yaroslavsky I, Allard ES, Sanchez-Lopez A. Can’t look away: attention control deficits predict rumination, depression symptoms and depressive affect in daily life. J Affect Disord. 2019;245:1061–1069.
42. Hata M. Milo and Otis. United States: Sony Pictures; 1989.
43. Gotlib IH, Kasch KL, Traill S, Joormann J, Arnow BA, Johnson SL. Coherence and specificity of information-processing biases in depression and social phobia. J Abnorm Psychol. 2004;113(3):386.
44. Preacher KJ, Kelley K. Effect size measures for mediation models: quantitative strategies for communicating indirect effects. Psychol Methods. 2011;16(2):93–115.
45. Shrout P, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods. 2002;7(4):422–445.
46. Crawford E, Wright MO. The impact of childhood psychological maltreatment on interpersonal schemas and subsequent experiences of relationship aggression. J Emot Abuse. 2007;7(2):93–116.
47. Lumley MN, Harkness KL. Specificity in the relations among childhood adversity, early maladaptive schemas, and symptom profiles in adolescent depression. Cognit Ther Res. 2007;31(5):639–657.
48. Loader P. Such a shame—a consideration of shame and shaming mechanisms in families. Child Abuse Rev. 1998;7:44–57.
49. Lewis M. Self-conscious emotions: embarrassment, pride, shame, and guilt. In: Lewis M, Haviland-Jones JM, editors. Handbook of Emotions.
50. Stuewig J, McCloskey LA. The relation of child maltreatment to shame and guilt among adolescents: psychological routes to depression and delinquency. Child Maltreat. 2005;10(4):324–336.
51. Feiring C. Emotional development, shame, and adaptation to child maltreatment. Child Maltreat. 2005;10:307–310.
52. LeMoult J, Humphreys KL, Tracy A, Hoffmeister JA, Ip E, Gotlib IH. Meta-analysis: exposure to early life stress and risk for depression in childhood and adolescence. J Am Acad Child Adolesc Psychiatry. 2020.
53. Christ C, De Waal MM, Dekker JJM, et al. Linking childhood emotional abuse and depressive symptoms: the role of emotion dysregulation and interpersonal problems. PLoS One. 2019;14:e0211882.
54. Cohen JR, McNeil SL, Shorey RC, Temple JR. Maltreatment subtypes, depressed mood, and anhedonia: a longitudinal study with adolescents. Psychol Trauma. 2018.
55. Kendall-Tackett KA, Williams LM, Finkelhor D. Impact of sexual abuse on children: a review and synthesis of recent empirical studies. Psychol Bull. 1993;113:164–180.
56. Brewin CR, Andrews B, Gotlib IH. Psychopathology and early experience: a reappraisal of retrospective reports. Psychol Bull. 1993;113(1):82–98.
57. Merrick MT, Ford DC, Ports KA, Guinn AS. Prevalence of adverse childhood experiences from the 2011–2014 behavioral risk factor surveillance system in 23 states. JAMA Pediatr. 2018;172:1038.
58. American College Health Association. American College Health Association-National College Health Assessment II: Canadian Reference Group Executive Summary Spring 2016. Hanover, MD; American College Health Association; 2016.
59. Rytwinski NK, Scur MD, Feeny NC, Youngstrom EA. The co-occurrence of major depressive disorder among individuals with posttraumatic stress disorder: a meta-analysis. J Trauma Stress. 2013;26:299–309.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.