Back to Journals » Journal of Healthcare Leadership » Volume 18
Chest Equivalent Dose as a Symbolic Radiation Communication Tool: Leadership Implications for Nurses’ Knowledge, Anxiety, and Risk Attribution
Authors Ayasrah M ![]() , Alrashdan YG
, Alrashdan YG ![]()
Received 4 February 2026
Accepted for publication 29 April 2026
Published 25 May 2026 Volume 2026:18 601232
DOI https://doi.org/10.2147/JHL.S601232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Mohammad Ayasrah, Youssef Ghaleb Alrashdan
Department of Allied Medical Sciences-Radiologic Technology, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, 22110, Jordan
Correspondence: Mohammad Ayasrah, Department of Allied Medical Sciences-Radiologic Technology, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, 22110, Jordan, Email [email protected]
Introduction: Communicating radiation dose to nurses using Sievert-based units may be difficult to interpret and may heighten anxiety. Chest Equivalent Dose (CED) is a symbolic approach that anchors dose information to a familiar chest imaging reference frame.
Objective: To compare the effects of Chest Equivalent Dose (CED) versus conventional Sievert-based dose communication on nurses’ radiation knowledge, radiation anxiety, and radiation-related feelings/experiences.
Methods: A quasi-experimental pretest–posttest comparative study was conducted among nurses in Jordan. Participants received Sievert-based education (n=40) or CED-based education (n=31). Radiation knowledge (RKQ), radiation anxiety (RAQ), and radiation-related feelings and experiences (RREF) were measured immediately before and after the session. Paired- and independent-samples tests were used, and time effects were explored using mixed-model analyses.
Results: Baseline scores did not differ between groups (all p> 0.05). In the CED group, RKQ increased from 59.76± 8.32 to 79.76± 10.16, while RAQ decreased from 57.97± 1.33 to 36.74± 1.83 and RREF decreased from 77.58± 2.87 to 47.12± 2.90 (all p< 0.001). In the Sievert group, RKQ was unchanged (56.08± 10.89 to 58.32± 9.04; p=0.329), with small decreases in RAQ (58.23± 1.19 to 56.45± 1.58; p< 0.001) and RREF (77.67± 3.02 to 75.67± 3.17; p=0.005). Posttest outcomes favoured CED for RKQ, RAQ, and RREF (all p< 0.001).
Conclusion: CED-based symbolic dose communication produced larger improvements in knowledge and larger reductions in anxiety and radiation-related experiences than Sievert-based education.
Plain Language Summary: Radiation dose is usually reported using scientific units such as millisieverts (mSv), which many nurses find difficult to interpret. When dose information is hard to interpret, it can increase worry, reduce confidence when answering patient questions, and weaken consistent risk communication across teams. Healthcare leaders and nurse educators are responsible for selecting training approaches and communication standards that support staff understanding and psychological safety.
In this study, nurses received a brief educational session using either conventional Sievert-based teaching or a symbolic approach called Chest Equivalent Dose (CED), which explains dose using a familiar reference (the dose from a standard chest X-ray). We measured nurses’ radiation knowledge, anxiety, and radiation-related feelings before and after training.
Compared with Sievert-based teaching, CED led to larger improvements in knowledge and larger reductions in anxiety and radiation-related concerns. These findings suggest that leaders can improve staff communication by standardizing an interpretable dose message that is accurate but easier to use in daily practice.
For leaders, CED can be implemented through onboarding, annual competency training, and short, standardized scripts for staff-to-staff and staff-to-patient communication, supported by local champions and periodic audits to ensure consistent use.
Keywords: radiation dose communication, chest equivalent dose, nurses, radiation anxiety, radiation knowledge, risk perception
Introduction
Radiation dose communication remains a persistent challenge in clinical imaging and radiotherapy environments.1 Although ionising radiation is integral to modern diagnostic and therapeutic procedures, its risks are often perceived as abstract and can be poorly understood by healthcare professionals—particularly nurses, who are frequently exposed indirectly through their clinical roles and contribute to patient care across departments where radiation is used, including radiology, emergency, and intensive care settings.2–5 Conventional radiation education commonly relies on physical dosimetric units such as the sievert, yet these measures may lack intuitive meaning for staff without a background in physics or radiography and may therefore fail to support effective risk understanding and emotional regulation.6 From a healthcare leadership perspective, improving dose communication is part of clinical governance because it requires consistent messaging, training fidelity, and mechanisms that support staff confidence in patient-facing discussions.
Nurses represent a large proportion of the healthcare workforce and are routinely involved in care pathways that include radiation-based investigations and interventions, positioning them at the interface between technical processes and patient experience.7 Despite this central role, many nurses receive limited formal education in radiation protection principles and dose interpretation, leaving knowledge gaps that may be filled by misconceptions and heightened concern.8 Inadequate understanding of radiation dose and risk has been associated with increased anxiety, misjudgement of exposure magnitude, and reduced confidence in clinical communication, particularly when responding to patient questions or supporting shared decision-making.9 These consequences are not limited to individual comfort; they may influence safety culture and the quality of risk communication delivered within clinical teams.
Dose information is typically communicated using standardised physical quantities, primarily the sievert (Sv) and its sub-units, which underpin regulatory frameworks and radiation protection standards.10 However, translating an exposure described in mSv into a meaningful sense of magnitude or practical implication can be difficult under routine clinical conditions, especially when rapid decisions and communication are required. When dose information is experienced as technical and inaccessible, it may be less likely to improve knowledge or reduce anxiety in non-physics-trained staff.6 For leaders, this gap can create variation in communication across shifts and units, undermining standardization and patient trust. A pragmatic solution is to adopt a dose language that is scientifically defensible and easier to apply in daily work.
Alternative approaches to dose representation—such as analogies and reference-based comparisons, including background equivalent radiation time (BERT)—have been proposed to anchor abstract quantities to familiar experiences and thereby improve comprehension.11 Despite growing interest in such strategies, empirical evidence evaluating their effectiveness in nursing populations remains limited. Given nurses’ central role in clinical coordination and patient-facing communication, evidence is needed on whether alternative dose communication formats can improve both cognitive outcomes (knowledge) and affective outcomes (anxiety and perceptions).
CED has been proposed as a symbolic radiation communication tool that expresses dose relative to the dose received from a standard chest radiograph.12 For example, an abdominal/pelvic CT examination may be described as equivalent to approximately 100–200 chest radiographs.13 By translating dose magnitude into a familiar and clinically meaningful reference, CED may reduce interpretive burden, enhance understanding, and support more adaptive appraisal of radiation-related risk.14 Importantly, symbolic dose representation is not intended to replace conventional dosimetry; rather, it functions as a complementary communication strategy aimed at improving comprehension and emotional response while maintaining scientific accuracy.15 However, the effects of CED-based education on nurses’ radiation knowledge, anxiety, and radiation-related perceptions have not been adequately investigated.
The present study addresses this gap by comparing the effects of CED-based education with conventional Sievert-based education among nurses working in imaging-related clinical settings. It evaluates pre–post changes in radiation knowledge, radiation-related anxiety, and radiation-related feelings and experiences following a structured educational intervention, providing evidence on whether symbolic dose communication can strengthen interdisciplinary radiation education and improve nurse-facing risk communication.12–15
Materials and Methods
Study Design
A quasi-experimental pretest–posttest comparative design was employed to evaluate the effects of two radiation dose communication approaches on nurses’ radiation knowledge and psychological responses. This design was selected because random allocation was not feasible within the operational constraints of clinical nursing services, including shift-based schedules and staffing demands, while still allowing systematic comparison of educational interventions over time. The design enabled within-group assessment of change following education and between-group comparison of outcomes associated with different dose communication formats.
Setting and Participants
The study was conducted in hospital-based clinical settings in Jordan where nurses routinely work in environments involving ionising radiation, including radiology departments, interventional units, operating theatres, emergency departments, and intensive care units. Nurses were selected as the target population because they frequently encounter radiation-related procedures, support patients undergoing imaging or interventional examinations, and may experience indirect occupational exposure despite not being primary operators.2
Eligible participants were registered nurses with active clinical duties in radiation-associated environments. Nurses with prior specialist training in medical physics or radiography were excluded to ensure that the sample reflected typical nursing educational backgrounds. Participation was voluntary, and recruitment was conducted using convenience sampling through departmental coordination.
A total of 71 nurses completed both pretest and posttest assessments and were included in the final analysis. Participants were allocated to either a Sievert-based education group (n = 40) or a CED -based education group (n = 31). The relatively small sample size reflects practical constraints inherent to face-to-face educational interventions in clinical settings, including rotating shift patterns, workload pressures, the requirement for participants to attend a full-day session under standardized conditions, and attrition due to clinical duties. These constraints are characteristic of applied educational research in healthcare environments and were considered acceptable given the study’s controlled pre–post design.
Group allocation followed operational scheduling rather than randomization. Two separate education sessions were delivered, and nurses attended the session assigned by their departmental roster/availability to avoid cross-group contamination during the same session. All eligible nurses received a study information sheet prior to participation and provided written informed consent before completing the pretest questionnaire. Participants were informed that both sessions covered the same radiation-protection content but used different dose communication formats (Sievert vs CED), and that participation was voluntary and would not affect their employment or training record.
Educational Intervention
Both groups received a structured, 45-minute face-to-face educational session delivered over a single day in a standardized learning environment. The educational content was identical for both groups and covered fundamental principles of ionising radiation, radiation protection, occupational exposure, and clinical risk awareness. The sole difference was the dose communication format: the control group received information in Sieverts, while the experimental group received it in CED.
Instruments
Data were collected using three validated instruments administered immediately before and after the educational intervention. Radiation knowledge was assessed using the RKQ, which evaluates understanding of radiation principles, exposure, and protection. Radiation-related anxiety was measured using the RAQ, designed to capture emotional responses and concern related to radiation exposure. Radiation-related feelings and experiences were assessed using the RREF, which evaluates subjective perceptions and confidence related to radiation contexts.
All instruments had been previously validated and demonstrated acceptable psychometric properties in healthcare populations. In the present study, internal consistency reliability was high, with Cronbach’s alpha coefficients (Cronbach’s α >0.85) exceeding acceptable thresholds for all scales at both pretest and posttest assessments.
Data Collection Procedure
Participants completed the pretest questionnaires immediately prior to the educational session. Posttest questionnaires were administered at the conclusion of the intervention on the same day to ensure consistency of learning conditions and minimize external influences. Each participant completed two assessments (pretest and posttest). Some attrition occurred between recruitment and completion due to clinical workload and shift changes; only participants with complete paired data were included in the analysis.
Statistical Analysis
Data were analyzed using SPSS v26 statistical software. Descriptive statistics were used to summarize participant characteristics and outcome measures. Baseline equivalence between groups was assessed using independent-samples tests. Within-group pre–post changes were evaluated using paired-samples tests. Between-group differences at posttest and in change scores were assessed using independent-samples tests.
General linear models were used to examine time effects and interactions with selected demographic and professional variables. Assumptions of normality and homogeneity of variance were evaluated prior to inferential testing. Effect sizes were reported using partial eta-squared (η2) to quantify the magnitude of observed effects.7 Statistical significance was set at p <0.05.
Results
Participant Characteristics
The final analytical sample comprised 71 nurses, (Sievert group, n=40; CED group, n=31). Demographic and professional characteristics are presented in Table 1. Most participants were aged 20–29 years (57/71, 80.3%), and females constituted 57.7% (41/71) of the sample. The majority held a bachelor’s degree in nursing (90.1%) and had ≤5 years of clinical experience (62.0%). Only 19.7% (14/71) reported prior formal training in radiation protection. Participants were drawn from multiple clinical departments, including radiology, emergency, intensive care, operating rooms, and other units (Table 1).
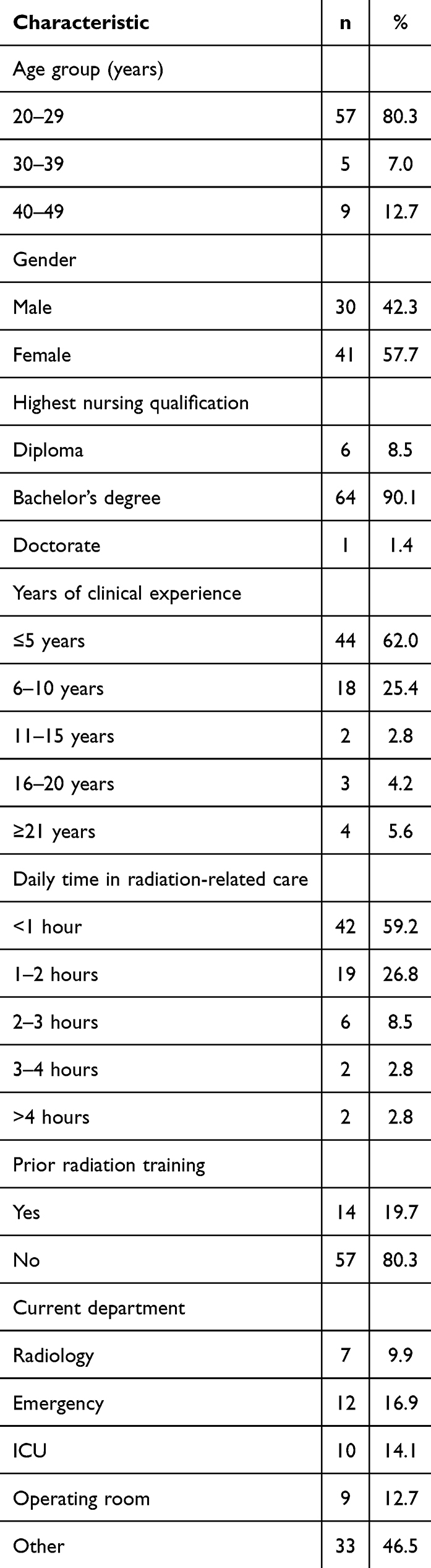 |
Table 1 Demographic and Professional Characteristics of Participants (N = 71) |
Baseline Equivalence Between Educational Groups
Baseline (pretest) comparisons between the Sievert-based group (n = 40) and the CED-based group (n = 31) are shown in Table 2. No statistically significant differences were observed between groups for any outcome measure at baseline. Mean radiation knowledge RKQ scores were 56.08 ± 10.89 in the Sievert group and 59.76 ± 8.32 in the CED group (t(69) = −1.544, p =0.127). Mean radiation anxiety RAQ scores were 58.23 ± 1.19 and 57.97 ± 1.33, respectively (t(69) = 0.860, p =0.393). Mean radiation-related feelings and experiences RREF scores were 77.67 ± 3.02 in the Sievert group and 77.58 ± 2.87 in the CED group (t(69) = 0.122, p =0.903).
 |
Table 2 Baseline (Pretest) Equivalence Between Educational Groups |
Within-Group Pre–Post Changes
Within-group pre–post comparisons are summarized in Table 3 using mean values with 95% confidence interval error bars. In the Sievert-based group, the change in RKQ scores from pretest (56.08 ± 10.89) to posttest (58.32 ± 9.04) was not statistically significant (t(78) = −0.983, p =0.329). Statistically significant reductions were observed for RAQ (58.23 ± 1.19 to 56.45 ± 1.58, t(78) = 5.670, p <0.001) and for RREF (77.67 ± 3.02 to 75.67 ± 3.17, t(78) = 2.896, p =0.005).
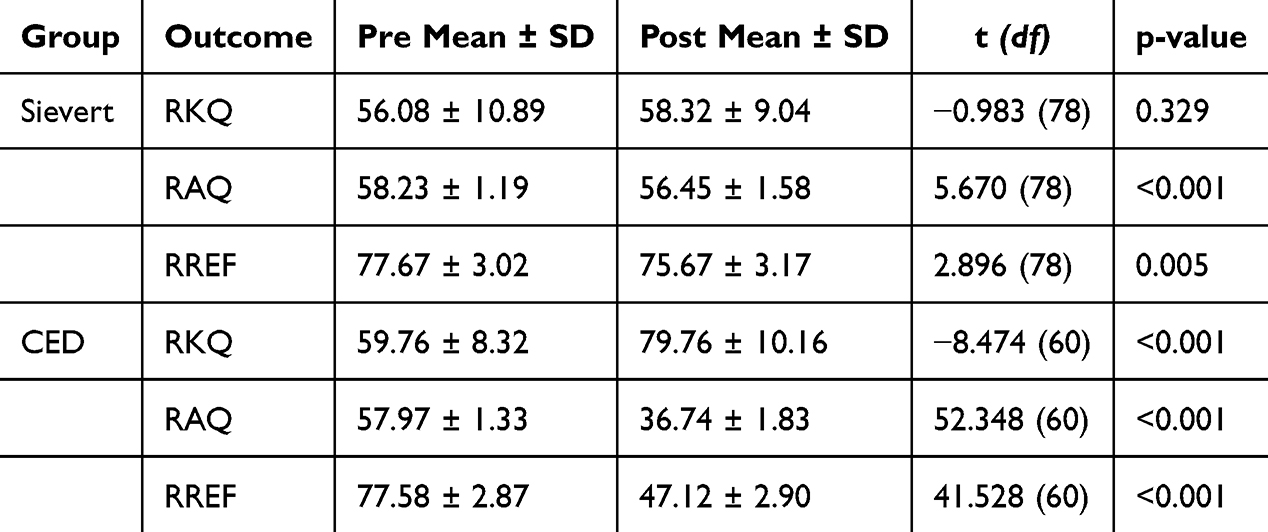 |
Table 3 Within-Group Pre–Post Comparisons |
In the CED-based group, statistically significant changes were observed across all outcomes. RKQ scores increased from 59.76 ± 8.32 at pretest to 79.76 ± 10.16 at posttest (t(60) = −8.474, p <0.001) Figure 1.
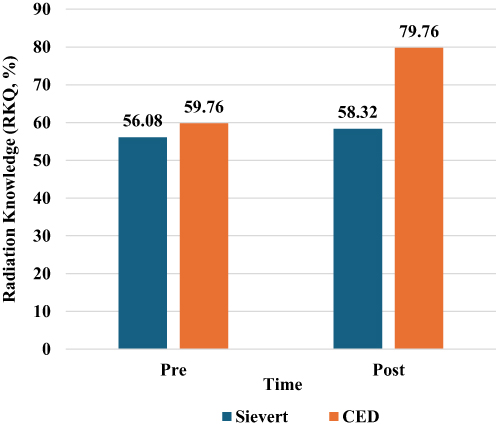 |
Figure 1 Radiation Knowledge (RKQ) Scores Before and After Education Using Sievert-Based and CED Communication. |
RAQ scores decreased from 57.97 ± 1.33 to 36.74 ± 1.83 (t(60) = 52.348, p <0.001). RREF scores decreased from 77.58 ± 2.87 to 47.12 ± 2.90 (t(60) = 41.528, p <0.001). These pre–post patterns are illustrated in Figure 2, which depict group-wise mean changes with confidence intervals.
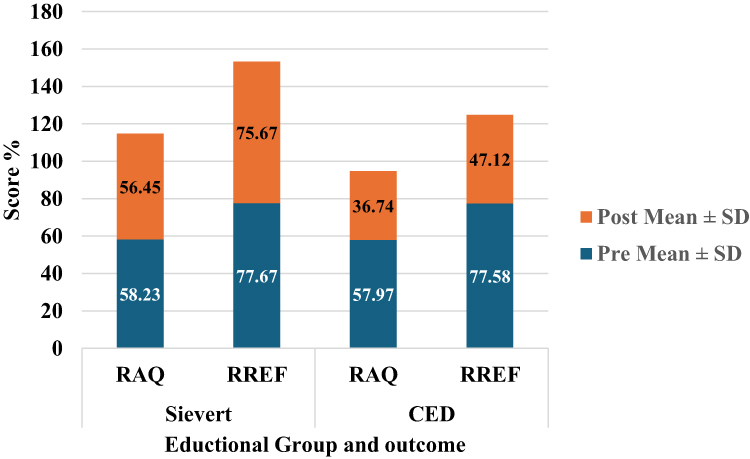 |
Figure 2 Radiation Anxiety (RAQ) and Radiation-Related Feelings and Experiences (RREF): Pre- and Post-Intervention Mean Scores (± SD) by Educational Group. |
Posttest Comparisons Between Educational Groups
Post-intervention comparisons between groups are presented in Table 4. At posttest, statistically significant differences were observed for all outcome measures. Mean RKQ scores were 58.32 ± 9.04 in the Sievert group compared with 79.76 ± 10.16 in the CED group (t(69) = −9.379, p <0.001). Mean RAQ scores were 56.45 ± 1.58 and 36.74 ± 1.83, respectively (t(69) = 48.641, p <0.001). Mean RREF scores were 75.67 ± 3.17 in the Sievert group and 47.12 ± 2.90 in the CED group (t(69) = 38.980, p <0.001).
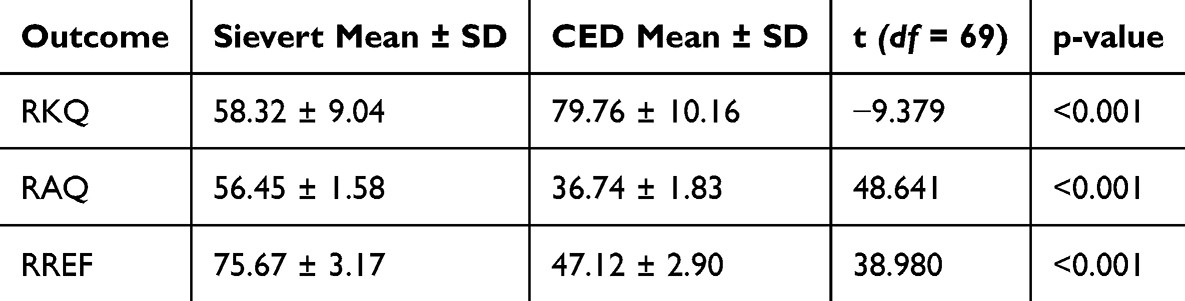 |
Table 4 Posttest Comparisons Between Educational Groups |
Change-Score Comparisons
Between-group comparisons of mean change scores (posttest minus pretest) are visualized in Figure 3, which displays mean change values for RKQ, RAQ, and RREF in both groups. The CED-based group demonstrated larger mean changes across all outcomes compared with the Sievert-based group.
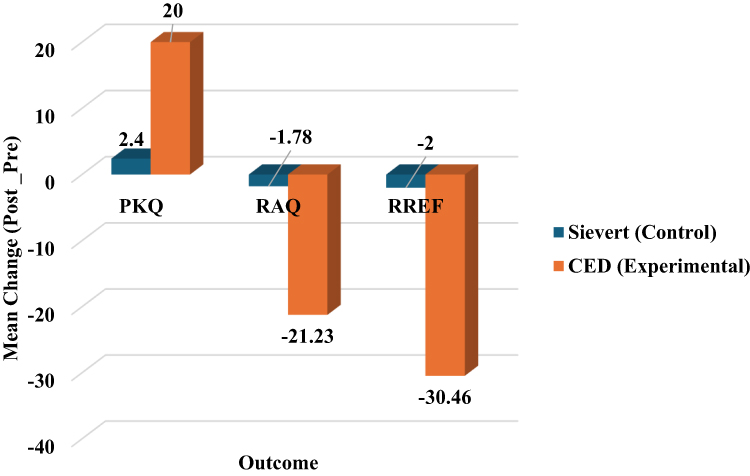 |
Figure 3 Mean change scores (post − pre) for RKQ, RAQ, and RREF by educational group. |
Interaction Effects and Covariate Analysis
Model-based analyses examining time effects and interactions with demographic and professional variables are summarized in Table 5. For radiation knowledge RKQ, a significant main effect of time was observed (F(1,69) = 24.862, p <0.001, partial η2 =0.265), along with a significant interaction between time and prior radiation training (F(1,69) = 10.034, p =0.002, partial η2 =0.127). Interactions between time and gender (p =0.872) and time and age (p =0.558) were not statistically significant (Table 5).
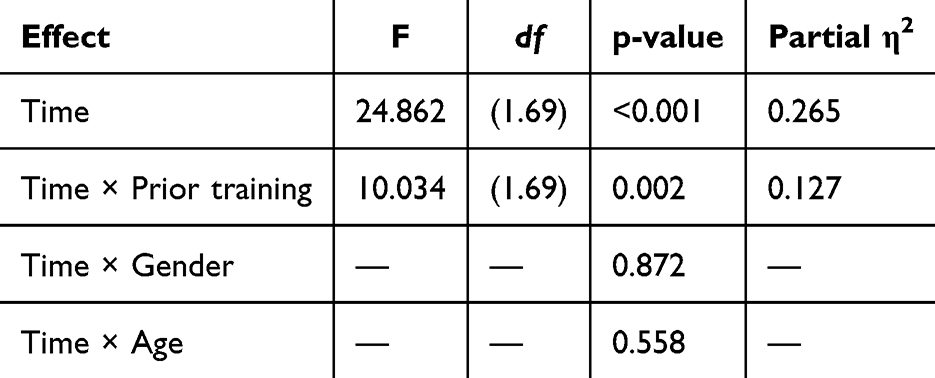 |
Table 5 Mixed ANOVA / GLM results for Time and Interaction Effects for RKQ (Knowledge) |
For radiation anxiety RAQ significant main effects of time were observed across demographic strata (eg, gender F(1,69) = 71.26, p <0.001, partial η2 =0.508), while interactions between time and gender (p =0.337), time and age (p =0.968), and time and prior training (p =0.092) were not statistically significant. (Table 6).
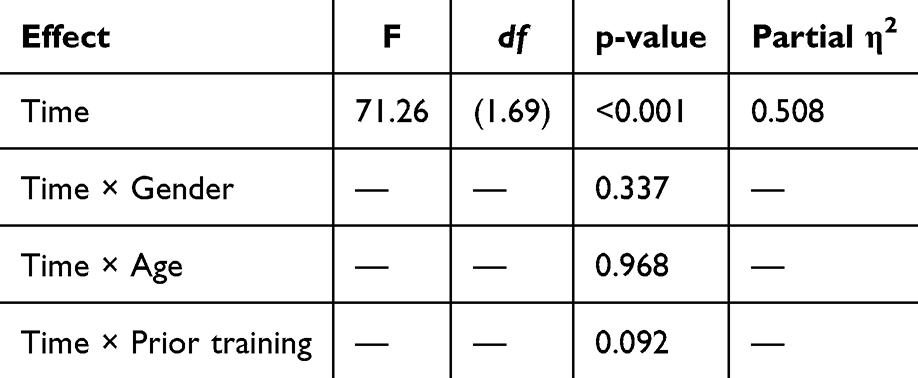 |
Table 6 Mixed ANOVA / GLM results for Time and Interaction Effects for RAQ (Anxiety) |
For radiation-related feelings and experiences RREF, significant main effects of time were also observed (gender F(1,69) = 64.36, p <0.001, partial η2 =0.482), with no statistically significant interactions involving gender, age, or prior radiation training (Table 7).
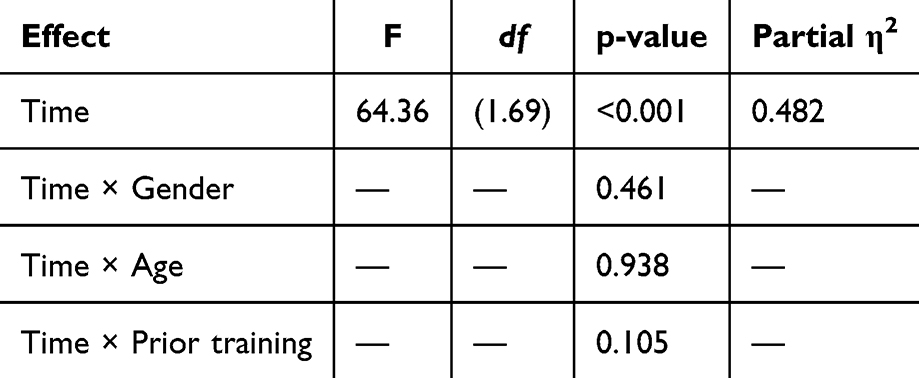 |
Table 7 Mixed ANOVA / GLM Results for Time and Interaction Effects for RREF (Feelings/Experiences) |
Discussion
This study indicates that symbolic dose communication, operationalised through CED, can serve as a practical leadership intervention for improving staff understanding and emotional responses to radiation exposure. Compared with conventional Sievert-based instruction, CED-based education produced larger improvements in radiation knowledge and larger reductions in anxiety and radiation-related experiences. For nurse leaders, educators, and safety managers, these outcomes matter because they support more consistent staff-to-staff and staff-to-patient communication, which is a core element of clinical governance and safety culture.
The knowledge gains in the CED group, contrasted with minimal change after Sievert-based education (Figures 1 and 3), suggest that standard physical quantities may not translate well into rapid conceptual learning for non-specialists.16 Interpreting dose expressed in mSv can require multiple mental conversions and may add extraneous cognitive effort in demanding clinical environments, limiting learning among shift-based nursing staff.17,18 CED anchors dose to a familiar clinical reference (a chest radiograph), thereby linking abstract quantities to an existing clinical schema and reducing extraneous processing demands, consistent with cognitive load theory.18 In short interventions, such anchoring may be critical for converting information into usable knowledge.
The interaction between time and prior radiation training for knowledge indicates that nurses without formal radiation education benefitted most from CED-based communication (Table 5). Reference-based learning strategies are often most effective when baseline domain knowledge is limited because they provide a scaffold for interpreting unfamiliar quantities.19 Nurses with previous training may already possess internal frameworks for interpreting physical dose units, reducing the incremental value of symbolic representations. This supports a leadership approach in which CED-based messages are prioritized for general nursing cohorts and units that do not routinely receive radiation-focused training.
The affective findings reinforce that dose communication is not purely informational. The larger reductions in anxiety and radiation-related experiences observed in the CED group (Figures 2 and 3) are operationally important because radiation-related anxiety among nurses has been linked to uncertainty, misunderstanding, and a perceived lack of control.4,20,21 A clinically meaningful reference frame may strengthen perceived comprehension and mastery, enabling nurses to distinguish routine low-risk occupational exposures from higher-dose procedures and thereby appraise workplace radiation risk more adaptively. Importantly, the observed reductions are compatible with informed reassurance rather than risk minimisation, because improved interpretability can reduce fear without obscuring the need for protection practices.
Reductions in anxiety and radiation-related concerns were broadly consistent across age and gender groups, suggesting usability across diverse nursing subgroups. This matters because nurses’ emotional responses can influence occupational wellbeing and engagement with radiation protection practices, and may shape the clarity and confidence of patient-facing explanations.15 Improved staff understanding may also strengthen interprofessional consistency when radiation benefit–risk is discussed in time-pressured settings such as emergency and critical care.
From a radiography practice perspective, these findings support integrating symbolic dose communication into interdisciplinary education. Radiographers remain responsible for dose optimization and technical accuracy, but nurses often lead peri-procedural care and patient explanations. Providing an interpretable reference such as CED can extend radiation-safety culture beyond imaging departments and strengthen shared understanding across teams.22,23 Implementation can be led through standardized CED-based scripts for staff and patient discussions, especially in high-throughput units where time pressure increases variability. Leaders should align the script with existing radiation-protection policies, embed CED in onboarding and annual refreshers co-delivered by nurse educators with radiology/radiation-safety staff, and appoint unit leader to reinforce consistent language across shifts. Brief audits (eg, a knowledge check and a single anxiety item) can feed continuous quality-improvement cycles This shared approach improves teamwork and patient reassurance.
Limitations
The quasi-experimental design and non-random group allocation limit causal inference. The modest sample reflects practical constraints of face-to-face education for nurses working rotating shifts, with some attrition between pre- and post-testing. Outcomes were assessed immediately post-intervention, preventing evaluation of longer-term retention or behavioural change. Reliance on self-reported measures may introduce response bias, and the single-centre setting may limit generalisability.
Conclusion
Symbolic dose communication using CED produced superior educational outcomes among nurses compared with Sievert-based education. CED was associated with greater improvements in radiation knowledge and larger decreases in radiation anxiety and radiation-related feelings and experiences, particularly among nurses without prior radiation training. Presenting dose using a clinically familiar reference frame appears to enhance interpretability and support calmer appraisal. Future research should test longer-term retention, behavioural outcomes, and effects on patient-facing discussions in larger samples.
Data Sharing Statement
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study received ethical approval from the Institutional Review Board of Jordan University of Science and Technology (approval reference June 2025/183-19). All procedures were conducted in compliance with relevant ethical standards. Data were collected and handled confidentially, no identifying personal information was obtained, and all responses were anonymized prior to analysis. Data management adhered to stringent confidentiality protocols, ensuring patient privacy and upholding the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants prior to participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Deanship of Research at Jordan University of Science and Technology (JUST) No. 20230660.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Salerno S, Nardi C, Pace M, et al. Communicating radiation dose in medical imaging: how to best inform our patients? Acta Radiol Open. 2023;12(4):20584601231168967. doi:10.1177/20584601231168967
2. Rincón G, González Y, Sánchez C. Risk perception among workers exposed to ionizing radiation: a qualitative view. Radioprotection. 2024;59(3):173–11. doi:10.1051/radiopro/2024004
3. Najjar R. Radiology’s ionising radiation paradox: weighing the indispensable against the detrimental in medical imaging. Cureus. 2023;15(7):e41623. doi:10.7759/cureus.41623
4. Rehman A, Mudassar DU, Jawed O, et al. Radiation safety awareness among nurses: understanding ionizing and non-ionizing hazards in clinical practice. Int J Environ Sci. 2024:683–689. doi:10.64252/50xchx68
5. Baudin C, Vacquier B, Thin G, et al. Occupational exposure to ionizing radiation in medical staff: trends during the 2009–2019 period in a multicentric study. Eur Radiol. 2023;33(8):5675–5684. doi:10.1007/s00330-023-09541-z
6. Allam SME, Algany MMA, Khider YIA. Radiation safety compliance awareness among healthcare workers exposed to ionizing radiation. BMC Nurs. 2024;23(1):208. doi:10.1186/s12912-024-01858-4
7. Farea A, A S, Alsaeed A, et al. Nursing and radiology teams collaboration to enhance patient safety during imaging procedures. Int J Comput Exp Sci Eng. 2024;10(4):2840–2852. doi:10.22399/ijcesen.4285
8. Shbeer A. Radiation in the intensive care units: a review of staff knowledge, practices, and radiation exposure. J Radiat Res Appl Sci. 2024;17(2):100849. doi:10.1016/j.jrras.2024.100849
9. Alotaibi M, Al-Abdulsalam A, Bakir Y, Mohammed A. Radiation awareness among nurses in nuclear medicine departments. Aust J Adv Nurs. 2015;32(3):25–33. doi:10.37464/2015.323.1577
10. Harrison JD, Balonov M, Bochud F, et al. The use of dose quantities in radiological protection: ICRP publication 147 Ann ICRP 50(1) 2021. J Radiol Prot Off J Soc Radiol Prot. 2021;41(2):410–422. doi:10.1088/1361-6498/abe548
11. Nickoloff EL, Lu ZF, Dutta AK, So JC. Radiation dose descriptors: BERT, COD, DAP, and other strange creatures. Radiogr Rev Publ Radiol Soc N Am Inc. 2008;28(5):1439–1450. doi:10.1148/rg.285075748
12. Diederich S, Lenzen H. Radiation exposure associated with imaging of the chest. Cancer. 2000;89(S11):2457–2460.
13. McNierney-Moore A, Smith C, Guardiola J, Xu KT, Richman PB. Patient understanding of radiation risk from medical computed tomography—A comparison of Hispanic vs. non-Hispanic emergency department populations. PeerJ. 2015;3:e937.
14. World Health Organization. Communicating radiation risks in paediatric imaging: information to support healthcare discussions about benefit and risk [Internet]; [cited January 6, 2026]. Available from: https://www.who.int/publications/i/item/978924151034.
15. Kim Y. The radiation problem and its solution from a health communication perspective. J Korean Med Sci. 2016;31(Suppl 1):S88–S98. doi:10.3346/jkms.2016.31.S1.S88
16. Slovic P, Finucane M, Peters E, MacGregor D. Risk as analysis and risk as feelings: some thoughts about affect, reason, risk, and rationality. Risk Anal off Publ Soc Risk Anal. 2004;24(2):311–322. doi:10.1111/j.0272-4332.2004.00433.x
17. Govasli L, Solvoll BA. Nurses’ experiences of busyness in their daily work. Nurs Inq. 2020;27(3):e12350. doi:10.1111/nin.12350
18. Paas F, Renkl A, Sweller J. Cognitive load theory and instructional design: recent developments. Educ Psychol. 2003;38(1):1–4. doi:10.1207/S15326985EP3801_1
19. Rix J. Active learning strategies, such as analogical models, aid in student learning of spinal anatomy and biomechanics. J Chiropr Educ. 2021;35(1):65–71. doi:10.7899/JCE-18-25
20. Iyama K, Sato Y, Ohba T, Hasegawa A. Objective stress values during radiation emergency medicine for future human resources: findings from a survey of nurses. PLoS One. 2022;17(9):e0274482. doi:10.1371/journal.pone.0274482
21. Fukuoka M, Yamaguchi T, Shinkawa T, Urata H, Orita M, Takamura N. Risk perception and anxiety regarding radiation among nurses working at Nuclear Emergency Core Hospitals in an Urgent Protective Action Planning Zone. 日本放射線看護学会誌. 2022;9:75–87. doi:10.24680/rnsj.10002
22. Hankin RA, Jones SP. The impact of educational interventions on clinicians’ knowledge of radiation protection: an integrative review. Radiogr Lond Engl. 2020;26(3):e179–e185. doi:10.1016/j.radi.2020.01.008
23. Kelly T, Surjan Y, Rinks M, Warren-Forward H. Effect of communication skills training on radiation therapy student’s confidence and interactions during their first clinical placement. Radiogr Lond Engl. 2021;27(1):59–66. doi:10.1016/j.radi.2020.05.015
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.