Back to Journals » Drug Design, Development and Therapy » Volume 19
Chemoradiotherapy with or Without Anlotinib for Postoperative Lymph Node Recurrence of Esophageal Squamous Cell Carcinoma: A Real-World Observational Study
Authors Zhu J, Tong YS ![]() , Zhu WG, Wang WW, Ji FZ, Zhou XL
, Zhu WG, Wang WW, Ji FZ, Zhou XL
Received 2 June 2025
Accepted for publication 13 September 2025
Published 15 October 2025 Volume 2025:19 Pages 9331—9342
DOI https://doi.org/10.2147/DDDT.S544203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jing Zhu,1,* Yu-Suo Tong,2,* Wei-Guo Zhu,2 Wan-Wei Wang,2 Fu-Zhi Ji,2 Xi-Lei Zhou2
1Department of Oncology, The Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University, Huai’an, People’s Republic of China; 2Department of Radiation Oncology, The Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University, Huai’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xi-Lei Zhou, Department of Radiation Oncology, The Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University, Huai’an, People’s Republic of China, Email [email protected]
Purpose: Anlotinib, a tyrosine kinase inhibitor, has shown encouraging anti-tumor activity in esophageal squamous cell carcinoma (ESCC). This study present real-world data on the efficacy and safety of chemoradiotherapy (CRT) plus anlotinib versus CRT alone in patients with lymph node recurrence of ESCC after radical resection.
Patients and Methods: Patients with lymph node recurrence of ESCC who received CRT with or without anlotinib between January 2017 and December 2019 were retrospectively analyzed. Treatment response, overall survival (OS), progression free survival (PFS) and treatment-related toxicities were compared between groups. Propensity score matching (PSM) analysis was used to balance baseline covariates.
Results: A total of 291 ESCC patients with lymph node recurrence received CRT plus anlotinib (n = 76) or CRT alone (n = 215). After PSM, 68 well-balanced patients in each group were included. The partial response rate (58.8% vs 41.2%, p = 0.04) and objective response rate (86.7% vs 61.8%, p = 0.001) were significantly higher in the CRT plus anlotinib group than in the CRT group. Patients in the CRT plus anlotinib group had significantly longer OS (3-year OS, 42.7% vs 23.5%, p = 0.008) and PFS (12-month PFS, 47.1% vs 32.4%, p = 0.026) than those in the CRT group. Multivariate survival analysis revealed that the treatment group (p = 0.007) was an independent predictor of OS. No significant differences were observed in grade 3– 4 treatment-related adverse events between the two groups (39.5% vs 30.7%, p = 0.162).
Conclusion: Compared with CRT alone, the addition of anlotinib to CRT was safe and provided survival benefits in ESCC patients with lymph node recurrence after radical resection.
Keywords: esophageal squamous cell carcinoma, lymph node recurrence, chemoradiotherapy, anlotinib, survival
Introduction
Esophageal squamous cell carcinoma (ESCC) is highly prevalent in south-east Asia and Africa.1 In 2017, approximate 235000 new cases of ESCC occurred in China, which accounts for 49.6% of the global cases.2 ESCC is an aggressive malignancy, frequently showing regional lymph node metastasis and invasion of adjacent organs. Despite therapeutic advances in surgical technique and neoadjuvant therapy in recent years, the clinical outcomes are poor due to local recurrence and distant metastasis after surgery. About 43–53% of patients will eventually develop regional or supraclavicular lymph node metastasis, and the median time to recurrence ranges from 10–12 months.3–6 Currently, treatments for recurrent or metastatic ESCC are chemotherapy, chemoradiotherapy (CRT), and immunotherapy. However, the outcome for patients receiving cisplatin-based CRT remains unsatisfactory, with a median overall survival (OS) of 17 months and a 3-year OS rate less than 11%.7 Therefore, more effective treatment regimens are urgently needed to improve clinical outcomes.
Angiogenesis is involved in the proliferation, progression and metastasis of tumor cells. Inhibitions of angiogenesis have been effective in treating multiple tumor types, including hepatocellular carcinoma, non-small cell lung cancer (NSCLC), and ESCC.8–10 Anlotinib is an oral multi-targeted tyrosine kinase inhibitor that blocks angiogenesis-related kinases such as vascular endothelial growth factor receptor 1–3, fibroblast growth factor receptor 1–4, platelet-derived growth factor receptor α/β, c-Kit and Ret.11,12 In vitro, anlotinib could suppress tumor cell proliferation, induce G2/M phase arrest and increase apoptosis in intrahepatic cholangiocarcinoma cell lines.13 In a phase II clinical trial, the use of anlotinib monotherapy (12 mg once per day) significantly improved progression free survival (PFS) compared with placebo (3.02 vs 1.41 months) in patients with advanced or metastatic ESCC.14 Recently, several studies have suggested that the combination of anlotinib with concurrent chemotherapy improves the prognosis of patients with NSCLC, recurrent glioblastoma and metastatic osteosarcoma.15–17 In a prior multi-center phase II study, anlotinib in combination with chemotherapy as the first line therapy achieved a satisfactory survival (median OS, 18.53 months) and manageable toxicities for patients with recurrent/advanced ESCC.18 Based on these results, anlotinib plus chemotherapy has been recommended in the 2022 version of the Chinese Society of Clinical Oncology for first-line or later treatment of metastatic ESCC. Although, a series of studies have demonstrated that anlotinib has promising antitumor activities and tolerable toxic effects in a variety of tumors, the use of anlotinib in combination with CRT for postoperative lymph node recurrence of ESCC has not been reported.
Therefore, the present study aimed to compare the differences in survival outcomes and safety of CRT plus anlotinib versus CRT alone in patients with lymph node recurrence of ESCC after radical surgery.
Materials and Methods
Patients
The medical records of recurrent ESCC patients who received CRT with or without anlotinib at Huai’an First People’s Hospital between January 2017 and December 2019 were screened. For inclusion in the study, patients met all the following criteria: R0 resection for primary ESCC (if radiotherapy was performed in the previous treatment, at least 12 months had passed since the end of the previous radiotherapy), Eastern Cooperative Oncology Group performance status (ECOG PS) of 0–2, aged 20–75 years, lymph node recurrence (including supraclavicular, mediastinal and abdominal lymph nodes), and no history of targeted therapy. Patients were excluded if they had the following conditions: esophageal fistulas, fresh gastrointestinal bleeding, active infection, anastomotic recurrence or distant metastasis, incomplete medical data, or loss to follow up. Patients with other malignancy histories and/or serious cardiac, liver, pulmonary, renal, or blood system diseases were also excluded. The 7th edition of the International Union Against Cancer (UICC) TNM classification was used to stage the primary disease after surgery. Patients were divided into two groups according to whether they received anlotinib (CRT plus anlotinib group) or not (CRT group). This study adhered to the principles outlined in the Declaration of Helsinki, and was approved by the institutional review board of Huai’an First Hospital. All patients signed written informed consent forms for treatment and agreed to cooperate with the follow-up visits.
Treatments
Radiotherapy
Radiotherapy (intensity-modulated radiation therapy), with a median radiation dose of 50.4 Gy (range, 50–60 Gy) was administered in daily fractions of 1.8–2.0 Gy. Involved-field irradiation was adopted for all patients. Enhanced CT was used to define the gross tumor volume (GTV). Lymph nodes with short axis size ≥ 1 cm on CT or positive PET images were included in the GTV. The boundaries of lymph node regions were determined according to the 2014 International Association for the Study of Lung Cancer lymph node map.19 The clinical target volume (CTV) was defined as a 0.8 cm radial margin and a 1.5–2.0 cm craniocaudal margin from the GTV. The planning target volume (PTV) was defined as the CTV plus a 0.5 cm margin in all directions.
Chemotherapy
All patients received chemotherapy concurrently with radiotherapy. Most patients (74.2%, 216/291) were treated with cisplatin and docetaxel-based regimens. Among them, 87 patients received docetaxel 25 mg/m2 and cisplatin 25 mg/m2 weekly for 5–6 weeks. Another 119 patients received docetaxel 75 mg/m2 on day 1 and cisplatin 25 mg/m2 on days 1–3 every 3 weeks for 2 cycles. Patients aged 70 years or older were treated with S-1 (70 mg/m2, twice per day, on days 1–14 and days 22–36) based regimen. Approximately 4–5 weeks after the completion of CRT, four additional cycles of consolation chemotherapy with the same regimens were added for patients who still had sufficient performance status.
Anlotinib Treatment
At our institution, patients with bulky lymph node metastases and/or adverse histology were referred for CRT plus anlotinib. Patients received anlotinib (Chia Tai Tianqing Pharmaceutical Group Co., Ltd., Nanjing, China) once daily (2 weeks on/1 week off) on the first day of radiotherapy. The initial dose of anlotinib (8 mg, 10 mg or 12 mg) was determined by clinicians according to patient age, general condition, and weight. After CRT, patients received the same dose of anlotinib as maintenance therapy until disease progression or for 12 months. If patients developed grade 3 or higher drug-related toxicities, treatment interruption was performed to manage toxic events. Treatment was permanently discontinued when there was disease progression or unacceptable toxicity. The reported toxicities were hypertension, hand-foot syndrome, proteinuria, hepatic insufficiency, diarrhea, hemoptysis, and hematemesis.
Assessment of Toxicity and Response
Acute treatment-related toxicity was monitored throughout the treatment and 3 months after CRT. The hematology and biochemistry assessments were done every week during treatment. During CRT, barium swallow and CT scans were performed every 2 weeks to monitor adverse events. During anlotinib maintenance therapy, toxicities were assessed every 3 weeks and graded in accordance with the National Cancer Institute Common Toxicity Criteria for Adverse Events (NCI-CTCAE) version 4.0.
Tumor responses were evaluated by contrast-enhanced CT using the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1) 4–6 weeks after CRT. A complete response (CR) of the lymph node metastasis was defined as the complete disappearance of all visible lymph node metastases on a CT scan. A partial response (PR) was defined as more than 30% reduction in lymph node metastasis. Objective response rate (ORR) was the sum of the CR and PR rates.
Follow-up
In the CRT plus anlotinib group, tumor responses were evaluated every 3 cycles during maintenance therapy. After the completion of treatment, all patients were followed up every 3–6 months for the first 2 years and then once per year. Follow-up tests included physical examination, CT scans, complete blood count, and hepatic, renal, thyroid and coagulation function. Follow-up data were obtained from patients’ medical records and/or telephone interviews. This study was censored on 31 May 2025.
Statistical Analysis
Demographic, clinicopathologic and treatment characteristics were summarized using descriptive statistics and compared between groups using χ2 test or Fisher’s exact test. To reduce selection bias and balance patient characteristics, propensity score matching (PSM) analysis was performed for each patient using the variables including age, gender, ECOG PS, tumor location, differentiation, stage of primary tumor, previous treatment, lymph node recurrence site, maximum lymph node diameter, chemotherapy regimen and radiation dose. Patients in the study and control groups were matched (1:1) using nearest-neighbor matching without replacement. OS and PFS were calculated from the starting date of CRT to the date of death from any cause and the date of the first radiographic progression or recurrence, respectively, or to the last follow-up (censored). OS and PFS were estimated using the Kaplan‒Meier method. Univariate analysis was performed to evaluate the associations between potential prognostic factors and OS. Factors included in the final multivariate survival analysis were those with p < 0.05 in the univariate analysis. All statistical tests were two sided, and p values less than 0.05 were considered as significant. All statistical calculations and PSM analyses were performed using SPSS version 22.0.
Results
Patient and Treatment Characteristics
From January 2017 to December 2019, a total of 291 patients met the inclusion criteria and were included in this retrospective analysis. Of all patients, 217 (74.6%) received surgery alone, and 74 (25.4%) received postoperative adjuvant therapy (including 28 with postoperative radiotherapy, 26 with postoperative chemotherapy, and 20 with postoperative CRT). The diagnosis of lymph node recurrence was mainly based on follow-up CT (245, 84.2%), PET-CT (28, 9.6%), or biopsy (18, 6.2%). The most common site of recurrence was station 2R (95, 32.6%), followed by 7 (77, 26.5%) and supraclavicular (71, 24.4%) lymph nodes. The number of lymph node recurrences was one in 79 patients (27.1%), two in 116 patients (39.9%), three in 81 patients (27.8%) and ≥ four in 15 patients (5.2%). The median time from surgery to the diagnosis of lymph node recurrence was 11 months (range, 2–68 months).
Of the 291 patients, 76 received CRT plus anlotinib (CRT plus anlotinib group), and 215 received CRT (CRT group). The clinical and treatment characteristics of each group are listed in Table 1. Patients in the CRT plus anlotinib group were younger (p = 0.026), had larger tumor (p = 0.007) and had poorer differentiation (p = 0.044) than those in the CRT group. The rate of consolidation chemotherapy was also higher in the CRT plus anlotinib group (p = 0.004, Table 1). No other significant differences were found between the two groups with respect of gender, ECOG PS, tumor location, primary tumor stage, previous treatment, chemotherapy regimen or radiation dose.
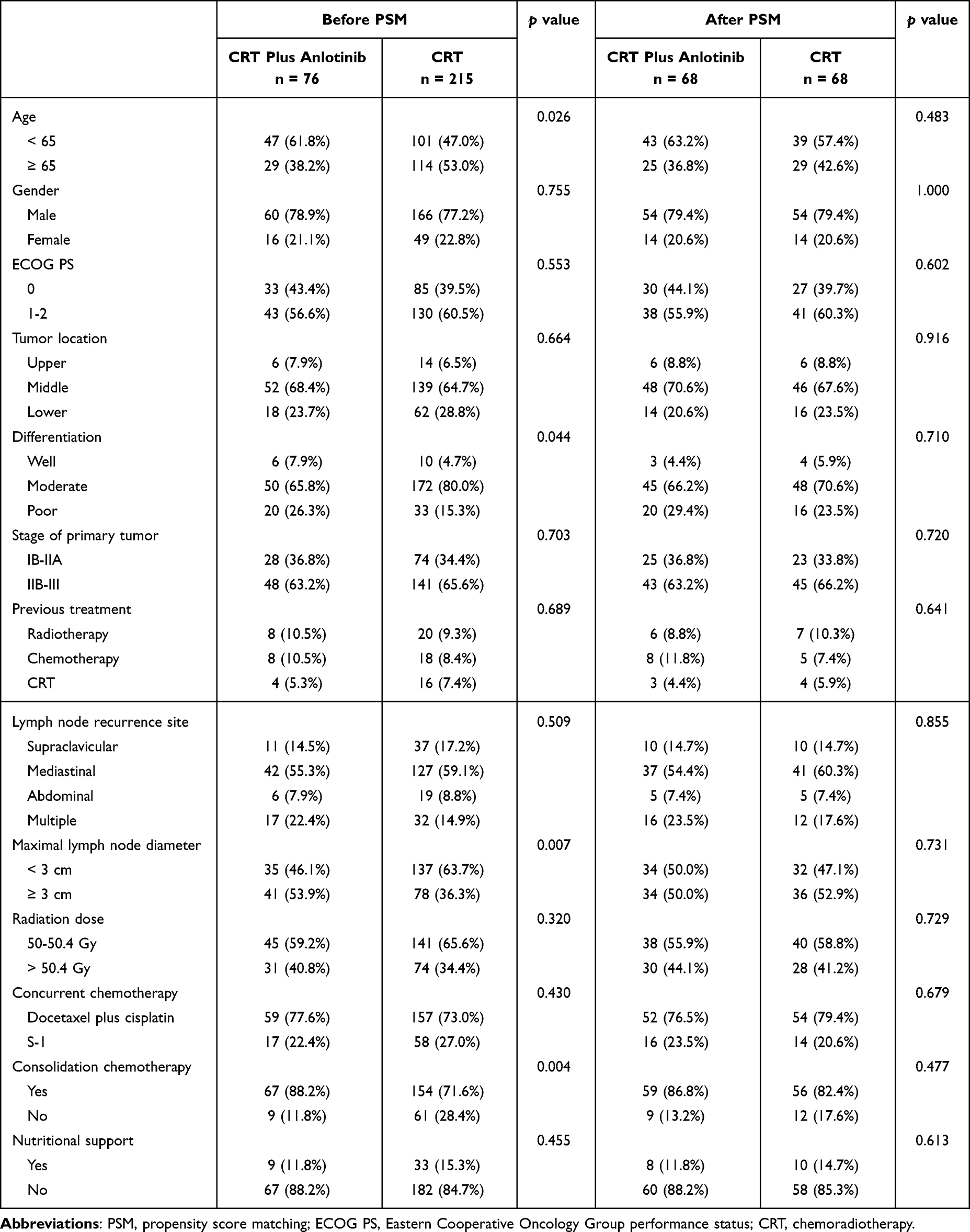 |
Table 1 Baseline Patient, Tumor, and Treatment Characteristics Before and After PSM |
After 1:1 PSM, 68 patients in the CRT plus anlotinib group and 68 matched patients in the CRT group were finally selected. The baseline demographics and tumor characteristics were well matched between the two groups (all p > 0.4, Table 1). In the CRT plus anlotinib group, 63 patients (92.6%) received anlotinib at an initial dose of 12 mg. During CRT, 66 (97.1%) of the 68 patients completed 2 cycles of the planned anlotinib regimen. The median treatment duration for anlotinib was 34 weeks (range, 2–52 weeks). Fifty-six patients (82.4%) received anlotinib for more than 6 cycles.
Tumor Response
Seven patients (2 in the CRT plus anlotinib group and 5 in the CRT group) were not evaluable by RECIST 1.1 criteria because they died before the first evaluation of treatment effect. Before PSM, a total of 74 patients (97.4%) in the CRT plus anlotinib group and 201 patients (93.5%) in the CRT group completed at least 50 Gy of radiation. The PR rate (58.1% vs 40.5%, p = 0.009) and ORR (86.5% vs 69.5%, p = 0.004) were significantly higher in the CRT plus anlotinib group than in the CRT group (Table 2).
 |
Table 2 Tumor Response to Treatment Before and After PSM |
After PSM, all patients completed full dose radiotherapy. The PR rate (58.8% vs 41.2%, p = 0.04) and ORR (86.7% vs 61.8%, p = 0.001) were still significantly higher in the CRT plus anlotinib group than in the CRT group (Table 2). In addition, a higher number of patients in the CRT plus anlotinib group achieved CR than did those in the CRT group, but the difference was not significant (27.9% vs 20.6%, p = 0.317, Table 2).
Overall Survival Rate and Progression Free Survival Rate Before and After PSM
Before PSM, 60 of 76 patients (78.9%) in the CRT plus anlotinib group and 191 of 215 patients (88.8%) in the CRT group experienced disease progression. The incidence of tumor recurrence was significantly lower in the CRT plus anlotinib group than in the CRT group (p = 0.016). The 6- and 12-month PFS rates were 82.9% and 44.7%, respectively, in the CRT plus anlotinib group, and 67.4% and 32.1%, respectively, in the CRT group (Figure 1A). At the time of the analysis, 58 patients (76.3%) in the CRT plus anlotinib group and 188 patients (87.4%) in the CRT group had died. OS was significantly improved in the CRT plus anlotinib group compared with the CRT group (p = 0.006). The 1-year and 3-year OS rates were 76.3% and 39.5%, respectively, in the CRT plus anlotinib group, and 62.3% and 25.5%, respectively, in the CRT group (Figure 1B).
 |
Figure 1 Progression free survival rate (PFS) and overall survival rate (OS) before (A and B) and after PSM (C and D). The CRT plus anlotinib group had significantly longer PFS and better OS than the CRT group (all p < 0.05). |
After PSM, PFS and OS were still significantly higher in the CRT plus anlotinib group than in the CRT group (6-month PFS, 88.2% vs 63.2%; 12-month PFS, 47.1% vs 32.4%, p = 0.026, and 1-year OS, 79.4% vs 61.8%; 3-year OS, 42.7% vs 23.5%, p = 0.008, Figure 1C and D).
Univariate and Multivariate Analysis of Prognostic Factors for Overall Survival
Table 3 shows the univariate and multivariate analysis of potential prognostic factors for OS in matched patients. Patient age (p = 0.047), primary tumor stage (p = 0.043), number of recurrent lymph nodes (p = 0.016), tumor response after CRT (p = 0.039) and treatment group (p = 0.009) were significantly associated with OS. In the multivariate analysis, the number of recurrent lymph nodes (HR = 2.023, 95% CI 1.258–3.253, p = 0.004), tumor response after CRT (HR = 1.771, 95% CI 1.115–2.814, p = 0.015) and treatment group (HR = 0.596, 95% CI 0.408–0.871, p = 0.007) were identified as significant prognostic factors of OS (Table 3).
 |
Table 3 Univariate and Multivariate Cox Analysis of Overall Survival After PSM |
Treatment Toxicities
Table 4 lists the grade 3–4 treatment-related adverse events (TRAEs) that occurred in more than 5% of patients. The most frequent grade 3–4 TRAEs in the CRT plus anlotinib group were leukopenia (23.7% vs 21.9% in the CRT group, p = 0.743), neutropenia (22.4% vs 20.5%, p = 0.726), anemia (10.5% vs 8.8%, p = 0.663), nausea/vomiting (7.9% vs 9.8%, p = 0.629), esophagitis (7.9% vs 8.4%, p = 0.897) and pneumonitis (3.9% vs 5.1%, p = 0.922). During CRT, two treatment-related deaths occurred in the CRT plus anlotinib group (1 was attributed to pulmonary embolism and 1 to gastrointestinal bleeding) and 5 occurred in the CRT group (3 to complications of febrile neutropenia, 1 to stroke, and 1 to a probable pulmonary embolism).
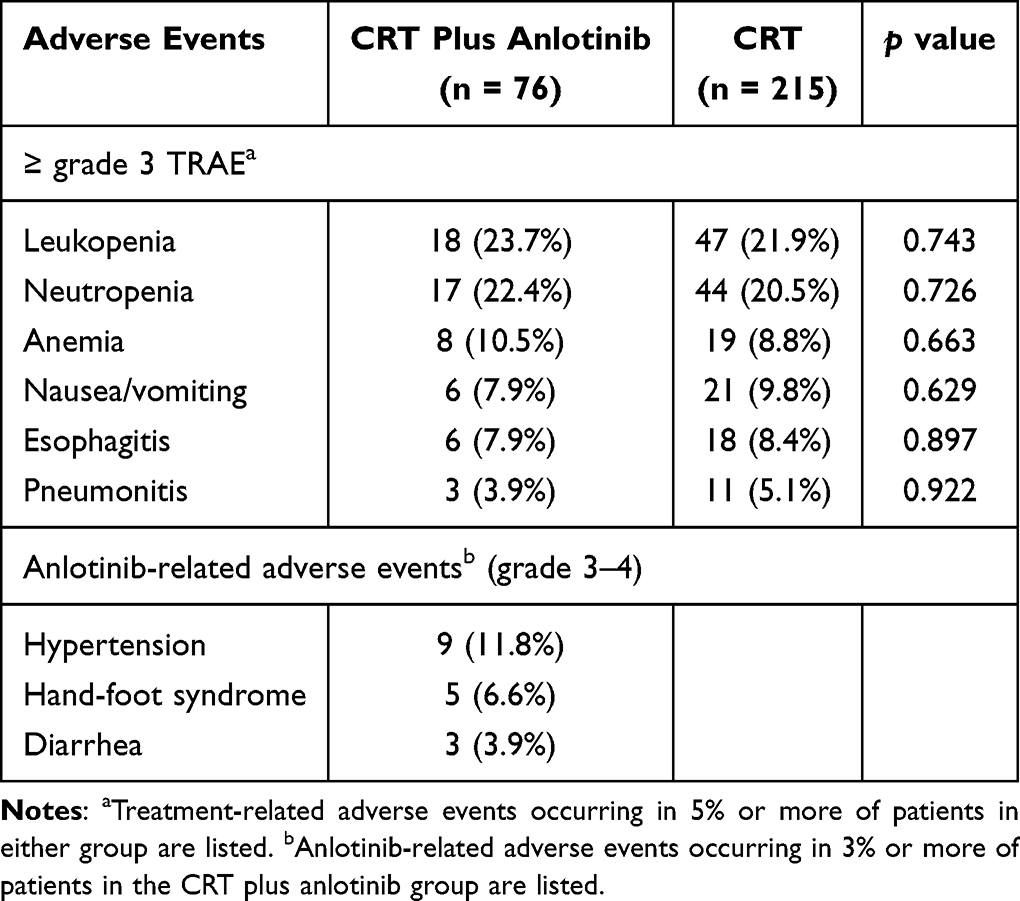 |
Table 4 Treatment-Related Adverse Events Stratified by Treatment Group |
During the entire treatment period, 93.4% of patients in the CRT plus anlotinib group experienced at least one anlotinib related adverse event, but most were grade 1–2. The most common adverse events associated with anlotinib were hypertension (39, 51.3%), hand and foot syndrome (27, 35.5%), proteinuria (23, 30.3%), hypothyroidism (12, 15.8%) and diarrhea (8, 10.5%). The incidences of grade 3–4 hypertension, hand and foot syndrome and diarrhea were 11.8%, 6.6% and 3.9%, respectively. A total of 6 patients had dose reduction to 10 mg (3 for hand and foot syndrome, 2 for diarrhea and 1 for proteinuria). There were no grade 5 TRAEs during anlotinib maintenance therapy. Finally, the occurrence of grade 3–4 TRAEs was slightly higher in the CRT plus anlotinib group than in the CRT group (39.5% vs 30.7%, p = 0.162).
Discussion
To our knowledge, this is the first study to evaluate CRT plus anlotinib in patients with postoperative lymph node recurrence of ESCC. The present study demonstrated that, compared with CRT alone, CRT plus anlotinib significantly increased PFS and OS in patients with postoperative lymph node recurrence of ESCC. In addition, this combination therapy was found to have manageable toxicity, and no treatment-related deaths were observed during anlotinib maintenance therapy. After PSM, the number of recurrent lymph node, tumor response after CRT and treatment group were identified as significant prognostic factors for OS.
Over the past decade, cisplatin in combination with 5-fluorouracil or paclitaxel has been frequently used as the first line treatment for patients with advanced or metastatic ESCC.20,21 However, the outcomes of patients treated with chemotherapy alone were poor, with an ORR ranging between 9.7% and 48.6%, and a median OS ranging from 7 to 13 months.22–24 For patients with regional lymph node recurrence without distant metastasis, treatments included lymphadenectomy, radiotherapy and CRT. Lymphadenectomy has been proven to increase locoregional disease control and prolong survival in patients with solitary lymph node recurrence,25 however, only a small portion of patients are eligible for salvage resection. Makino et al studied patients with solitary lymph node recurrence of ESCC, reporting that only 16.7% of patients had a chance to undergo surgery.26 According to previous studies of radiotherapy or CRT for treating postoperative lymph node recurrence in patients with ESCC, the median ORR of the 10 studies was 75.9% (range, 68.8–85.0%), and the median 3-year OS was 37.0% (range, 10.5% to 56.3%).7,27–35 Among them, Kawamoto et al reported the survival rates of 57 patients with lymph node recurrence treated with CRT. With a median follow-up of 24 months, the ORR was 82.5%, and the 3-year OS was 36.9%.28 Yamashita et al reported similar results in a study involving 237 recurrent ESCC patients who were treated with salvage radiotherapy or CRT. In that study, patients who received CRT had better OS than those who received radiotherapy alone (3-year OS, 39.7% vs 20.8%).30 In our study, compared with CRT alone, CRT plus anlotinib significantly prolonged PFS and OS in patients with postoperative lymph node recurrence. In addition, the ORR was also higher in the CRT plus anlotinib group than in the CRT group (86.7% vs 61.8%, p = 0.001). In recent years, there have been several studies on monotherapy or combination therapy with antiangiogenic agents for recurrent or advanced ESCC.36–39 Anlotinib monotherapy achieved an ORR of 8.4% and a median PFS of 3.3 months in previously treated advanced or metastatic ESCC patients.40 In the ESO-Shanghai 11 study, patients with chemotherapy refractory ESCC who received apatinib treatment had an ORR of 7.5% and a median PFS of 3.8 months.37 In a phase II study involving patients with recurrent or advanced ESCC, treatment with anlotinib plus paclitaxel and cisplatin as the first-line therapy yielded an ORR of 76.1%, a median PFS of 8.38 months with 12-month PFS of 25.17%, and a median OS of 18.53 months with 2-year OS of 37.21%.18 Our ORR, 12-month PFS and 3-year OS of patients in the CRT plus anlotinib group were 86.7%, 47.1% and 42.7%, respectively, which were greater than those reported in the phase II study. The higher ORR in this study may be attributed to the synergistic effect of CRT and anlotinib. A recent study has demonstrated that anlotinib can hinder radiotherapy-induced DNA double-strand breaks repair, increase the accumulation of cytosolic dsDNA and activate cGAS/STING signaling pathway, thus enhancing the response of tumor to radiotherapy.41
Although chemotherapy has been a widely used first-line therapy for advanced or metastatic ESCC, survival benefits were recently reported with anti-PD-1 immunotherapy plus chemotherapy over chemotherapy alone.42–44 In the multicenter Phase III ORIENT-15 and JUPITER-06 studies,45,46 anti-PD-1 immunotherapy (sintilimab, toripalimab) combined cisplatin plus paclitaxel significantly improved PFS and OS compared with cisplatin plus paclitaxel chemotherapy alone in the treatment of advanced or metastatic ESCC, with 1-year PFS ranging from 27.8% to 38%, and 1-year OS ranging from 52% to 66%. Treatment efficacy in our study was higher than reported for sintilimab or toripalimab in patients with advanced or metastatic ESCC.
In the present study, multivariate analysis revealed that the number of recurrent lymph node, tumor response after CRT and treatment group were independent prognostic factors for OS. Recently, researchers have made efforts to identify prognostic factors for patients with postoperative lymph node recurrence of ESCC. Age, radiation dose, ECOG PS, number of recurrent lymph nodes, tumor size, and chemotherapy regimen have been demonstrated to be significant prognostic factors.27,32,47–49 Yamashita et al reported that patients with a maximum lymph node diameter ≤ 22 mm had a significantly better prognosis than those with a diameter > 22 mm.30 Nemoto et al demonstrated that patients with a short time interval between surgery and recurrence and younger patients had shorter survival times.50 Our results were different from previous findings. The radiation dose, ECOG PS, and chemotherapy regimen did not significantly affected OS. In addition, contrary to previous studies, our results showed that older patients had a worse prognosis. The differences in treatments and stage of primary tumor or the heterogeneity of the patient populations may be possible explanations for the difference in survival.
In our study, the incidence of grade 3–4 TRAEs in the CRT plus anlotinib group was 39.5%, which was consistent with that of previous CRT for patients with lymph node recurrence of ESCC.29,51 The most common grade 3–4 TRAEs observed in the CRT plus anlotinib group were leukopenia, neutropenia, anemia, nausea/vomiting, and esophagitis, indicating that the majority of these TRAEs were associated with CRT. There was no increase in toxicity with the addition of anlotinib other than some non-hematological adverse events. Hypertension, hand-foot syndrome, proteinuria and diarrhea observed in the present study are adverse events that had previously been associated with anlotinib treatment.52,53 These adverse events occurred at a similar incidence to those observed in other anti-vascular targeted therapies.37,54 Hemorrhage, previously reported as the most serious complication of anlotinib, was reduced in the present study. All TRAEs during the CRT period were manageable, demonstrating that anlotinib can be safely added to CRT.
This study had several limitations. First, this was a single-center retrospective analysis, resulting in inherent selection bias, despite we used PSM analysis to mitigate these biases. Second, the number of patients included in this study was small. In addition, some patients received subsequent therapies after disease progression, which might affect the survival analysis.
Conclusion
In conclusion, compared with CRT alone, the addition of anlotinib to CRT significantly improved the response rate and survival outcomes in patients with postoperative lymph node recurrence of ESCC. Prospective randomized clinical trials are needed to confirm the clinical benefits of this combination.
Acknowledgments
We would like to express gratitude to all those colleagues who contributed to this study. Jing Zhu and Yu-Suo Tong contributed equally to this work and should be considered as joint first authors.
Funding
No funding was received to assist with the preparation of this paper.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Arnold M, Soerjomataram I, Ferlay J, Forman D. Global incidence of oesophageal cancer by histological subtype in 2012. Gut. 2015;64(3):381–387. doi:10.1136/gutjnl-2014-308124
2. Kamangar F, Nasrollahzadeh D, Safiri S. The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol. 2020;5(6):582–597. doi:10.1016/S2468-1253(20)30007-8
3. Mariette C, Balon JM, Piessen G, Fabre S, Van Seuningen I, Triboulet JP. Pattern of recurrence following complete resection of esophageal carcinoma and factors predictive of recurrent disease. Cancer. 2003;97(7):1616–1623. doi:10.1002/cncr.11228
4. Hsu PK, Wang BY, Huang CS, Wu YC, Hsu WH. Prognostic factors for post-recurrence survival in esophageal squamous cell carcinoma patients with recurrence after resection. J Gastrointest Surg. 2011;15(4):558–565. doi:10.1007/s11605-011-1458-1
5. Dresner SM, Wayman J, Shenfine J, Harris A, Hayes N, Griffin SM. Pattern of recurrence following subtotal oesophagectomy with two field lymphadenectomy. Br J Surg. 2000;87(3):362–373.
6. Miyata H, Yamasaki M, Kurokawa Y, et al. Survival factors in patients with recurrence after curative resection of esophageal squamous cell carcinomas. Ann Surg Oncol. 2011;18(12):3353–3361. doi:10.1245/s10434-011-1747-7
7. Lu JC, Kong C, Tao H. Radiotherapy with or without concurrent chemotherapy for lymph node recurrence after radical surgery of thoracic esophageal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2010;78(3):710–714. doi:10.1016/j.ijrobp.2009.08.065
8. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
9. Xu Y, Huang Z, Lu H, et al. Apatinib in patients with extensive-stage small-cell lung cancer after second-line or third-line chemotherapy: a phase II, single-arm, multicentre, prospective study. Br J Cancer. 2019;121(8):640–646. doi:10.1038/s41416-019-0583-6
10. Yanwei L, Feng H, Ren P, et al. Safety and efficacy of apatinib monotherapy for unresectable, metastatic esophageal cancer: a single-arm, open-label, phase II study. Oncologist. 2020;25(10):e1464–e1472. doi:10.1634/theoncologist.2020-0310
11. Wang G, Sun M, Jiang Y, Zhang T, Sun W, Wang H. Anlotinib, a novel small molecular tyrosine kinase inhibitor, suppresses growth and metastasis via dual blockade of VEGFR2 and MET in osteosarcoma. Int J Cancer. 2019;145(4):979–993. doi:10.1002/ijc.32180
12. Shen G, Zheng F, Ren D, et al. Anlotinib: a novel multi-targeting tyrosine kinase inhibitor in clinical development. J Hematol Oncol. 2018;11(1). doi:10.1186/s13045-018-0664-7
13. Song F, Hu B, Cheng J-W. Anlotinib suppresses tumor progression via blocking the VEGFR2/PI3K/AKT cascade in intrahepatic cholangiocarcinoma. Cell Death Differ. 2020;11(7):573. doi:10.1038/s41419-020-02749-7
14. Huang J, Xiao J, Fang W, Lu P, Fan Q, Shu Y. Anlotinib for previously treated advanced or metastatic esophageal squamous cell carcinoma: a double-blind randomized Phase 2 trial. Cancer Med. 2021;10(5):1681–1689. doi:10.1002/cam4.3771
15. Xu Q, Huang K, Meng X. Safety and efficacy of anlotinib hydrochloride plus temozolomide in patients with recurrent glioblastoma. Clin Cancer Res. 2023;29(19):3859–3866. doi:10.1158/1078-0432.CCR-23-0388
16. Xiang M, Yang X, Ren S, et al. Anlotinib combined with S-1 in third- or later-line stage IV non-small cell lung cancer treatment: a phase II clinical trial. Oncologist. 2021;26(12):e2130–e2135. doi:10.1002/onco.13950
17. Wang T, Lin F, Huang Y, et al. The combination of anlotinib and gemcitabine/docetaxel in patients with metastatic osteosarcoma who have failed standard chemotherapy. Cancer Manag Res. 2022;14:2945–2952. doi:10.2147/CMAR.S378264
18. Li N, Wu T, Hong YG, et al. A multi-center, single-arm, phase II study of anlotinib plus paclitaxel and cisplatin as the first-line therapy of recurrent/advanced esophageal squamous cell carcinoma. BMC Med. 2022;20(1):472. doi:10.1186/s12916-022-02649-x
19. El-Sherief AH, Lau CT, Wu CC, Drake RL, Abbott GF, Rice TW. International association for the study of lung cancer (IASLC) lymph node map: radiologic review with CT illustration. Radiographics. 2014;34(6):1680–1691. doi:10.1148/rg.346130097
20. Hiramoto S, Kato K, Shoji H, et al. A retrospective analysis of 5-fluorouracil plus cisplatin as first-line chemotherapy in the recent treatment strategy for patients with metastatic or recurrent esophageal squamous cell carcinoma. Int J Clin Oncol. 2018;23(3):466–472. doi:10.1007/s10147-018-1239-x
21. Huang J, Xu J, Chen Y, et al. Camrelizumab versus investigator’s choice of chemotherapy as second-line therapy for advanced or metastatic oesophageal squamous cell carcinoma (ESCORT): a multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2020;21(6):832–842. doi:10.1016/S1470-2045(20)30110-8
22. Petrasch S, Welt A, Reinacher A, Graeven U, König M, Schmiegel W. Chemotherapy with cisplatin and paclitaxel in patients with locally advanced, recurrent or metastatic oesophageal cancer. Br J Cancer. 1998;78(4):511–514. doi:10.1038/bjc.1998.524
23. Zhang X, Shen L, Li J, Li Y, Li J, Jin M. A phase II trial of paclitaxel and cisplatin in patients with advanced squamous-cell carcinoma of the esophagus. Am J Clin Oncol. 2008;31(1):29–33. doi:10.1097/COC.0b013e3181131ca9
24. Sun S, Yu H, Wang H, et al. Phase II study of S-1 plus cisplatin as first-line therapy in patients with metastatic esophageal carcinoma. Oncol Res Treat. 2019;42(3):115–122. doi:10.1159/000495700
25. Wang Z, Lin S, Wang F, Liu S. Salvage lymphadenectomy for isolated cervical lymph node recurrence after curative resection of thoracic esophageal squamous cell carcinoma. Ann Transl Med. 2019;7(11):238. doi:10.21037/atm.2019.04.64
26. Makino T, Yamasaki M, Miyata H, et al. Solitary lymph node recurrence of esophageal squamous cell carcinoma: surgical failure or systemic disease? Ann Surg Oncol. 2016;23(6):2087–2093. doi:10.1245/s10434-015-5086-y
27. Shioyama Y, Nakamura K, Ohga S, et al. Radiation therapy for recurrent esophageal cancer after surgery: clinical results and prognostic factors. Jpn J Clin Oncol. 2007;37(12):918–923. doi:10.1093/jjco/hym138
28. Kawamoto T, Nihei K, Sasai K, Karasawa K. Clinical outcomes and prognostic factors of chemoradiotherapy for postoperative lymph node recurrence of esophageal cancer. Jpn J Clin Oncol. 2018;48(3):259–264. doi:10.1093/jjco/hyx171
29. Jeene PM, Versteijne E, van Berge Henegouwen MI, et al. Definitive chemoradiation for locoregional recurrences of esophageal cancer after primary curative treatment. Dis Esophagus. 2017;30(2):1–5. doi:10.1111/dote.12539
30. Yamashita H, Jingu K, Niibe Y, et al. Definitive salvage radiation therapy and chemoradiation therapy for lymph node oligo-recurrence of esophageal cancer: a Japanese multi-institutional study of 237 patients. Radiat Oncol. 2017;12(1):38. doi:10.1186/s13014-017-0780-5
31. Zhang C, Ge XL, Huang CJ, Zhang S, Sun XC. Outcomes and prognostic factors of salvage radiation for postoperative lymph node recurrence of esophageal squamous cell carcinoma. Front Oncol. 2021;11:638521. doi:10.3389/fonc.2021.638521
32. Jingu K, Nemoto K, Matsushita H, et al. Results of radiation therapy combined with nedaplatin (cis-diammine-glycoplatinum) and 5-fluorouracil for postoperative locoregional recurrent esophageal cancer. BMC Cancer. 2006;6(1):50. doi:10.1186/1471-2407-6-50
33. Chen J, Yin W, Yao H, Gu W. Salvage treatment for lymph node recurrence after radical resection of esophageal squamous cell carcinoma. Radiat Oncol. 2019;14(1):169. doi:10.1186/s13014-019-1377-y
34. Chen B, Li Q, Li Q, et al. Weekly chemotherapy of 5-Fluorouracil plus cisplatin concurrent with radiotherapy for esophageal squamous cell carcinoma patients with postoperative locoregional recurrence: results from a phase II study. Oncologist. 2020;25(4):308–e625. doi:10.1634/theoncologist.2019-0931
35. Bao Y, Liu S, Zhou Q, et al. Three-dimensional conformal radiotherapy with concurrent chemotherapy for postoperative recurrence of esophageal squamous cell carcinoma: clinical efficacy and failure pattern. Radiat Oncol. 2013;8(1):241. doi:10.1186/1748-717X-8-241
36. Liu Y, Ge Q, Xu S, Li K, Liu Y. Efficacy and safety of anlotinib plus programmed death-1 blockade versus anlotinib monotherapy as second or further-line treatment in advanced esophageal squamous cell carcinoma: a retrospective study. Front Oncol. 2022;12:942678. doi:10.3389/fonc.2022.942678
37. Chu L, Chen Y, Liu Q, et al. A phase II study of apatinib in patients with chemotherapy-refractory esophageal squamous cell carcinoma (ESO-Shanghai 11). Oncologist. 2021;26(6):e925–e935. doi:10.1002/onco.13668
38. Zhao J, Lei J, Yu J, et al. Clinical efficacy and safety of apatinib combined with S-1 in advanced esophageal squamous cell carcinoma. Invest New Drugs. 2020;38(2):500–506. doi:10.1007/s10637-019-00866-5
39. Qu Y, Munire A, Zhou N, et al. Camrelizumab combined with apatinib for unresectable, metastatic esophageal squamous cell carcinoma: a single-center, single-arm, prospective study. J Gastrointestinal Oncol. 2024;15(1):1–11. doi:10.21037/jgo-23-610
40. Zhang S, Wang X, Gu H, Liu JQ. Feasibility and safety of anlotinib monotherapy for patients with previously treated advanced esophageal squamous cell carcinoma: a real-world exploratory study. Cancer Manag Res. 2022;14:1715–1727. doi:10.2147/CMAR.S359482
41. Han D, Zhang J, Bao Y, Liu L, Wang P, Qian D. Anlotinib enhances the antitumor immunity of radiotherapy by activating cGAS/STING in non-small cell lung cancer. Cell Death Discov. 2022;8(1):468. doi:10.1038/s41420-022-01256-2
42. Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27–40. doi:10.1016/S0140-6736(21)00797-2
43. Luo H, Lu J, Bai Y, et al. Effect of camrelizumab vs placebo added to chemotherapy on survival and progression-free survival in patients with advanced or metastatic esophageal squamous cell carcinoma: the ESCORT-1st randomized clinical trial. JAMA. 2021;326(10):916–925. doi:10.1001/jama.2021.12836
44. Sun J-M, Shen L, Shah MA, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759–771. doi:10.1016/S0140-6736(21)01234-4
45. Lu Z, Wang J, Shu Y, et al. Sintilimab versus placebo in combination with chemotherapy as first line treatment for locally advanced or metastatic oesophageal squamous cell carcinoma (ORIENT-15): multicentre, randomised, double blind, phase 3 trial. BMJ;2022. e068714. doi:10.1136/bmj-2021-068714
46. Wang ZX, Cui C, Yao J, et al. Toripalimab plus chemotherapy in treatment-naïve, advanced esophageal squamous cell carcinoma (Jupiter-06): a multi-center phase 3 trial. Cancer Cell. 2022;40(3):277–288.e273. doi:10.1016/j.ccell.2022.02.007
47. Fakhrian K, Gamisch N, Schuster T, Thamm R, Molls M, Geinitz H. Salvage radiotherapy in patients with recurrent esophageal carcinoma. Strahlenther Onkol. 2012;188(2):136–142. doi:10.1007/s00066-011-0023-x
48. Nakamura T, Ota M, Narumiya K, et al. Multimodal treatment for lymph node recurrence of esophageal carcinoma after curative resection. Ann Surg Oncol. 2008;15(9):2451–2457. doi:10.1245/s10434-008-0016-x
49. Zhang J, Peng F, Li N, et al. Salvage concurrent radio-chemotherapy for post-operative local recurrence of squamous-cell esophageal cancer. Radiat Oncol. 2012;7(1):93. doi:10.1186/1748-717X-7-93
50. Nemoto K, Ariga H, Kakuto Y, et al. Radiation therapy for loco-regionally recurrent esophageal cancer after surgery. Radiother Oncol. 2001;61(2):165–168. doi:10.1016/S0167-8140(01)00392-9
51. Xu YY, Zhou XL, Yu CH, et al. Association of sarcopenia with toxicity and survival in postoperative recurrent esophageal squamous cell carcinoma patients receiving chemoradiotherapy. Front Oncol. 2021;11:655071. doi:10.3389/fonc.2021.655071
52. Sun Y, Niu W, Du F, et al. Safety, pharmacokinetics, and antitumor properties of anlotinib, an oral multi-target tyrosine kinase inhibitor, in patients with advanced refractory solid tumors. J Hematol Oncol. 2016;9(1):105. doi:10.1186/s13045-016-0332-8
53. Zhou AP, Bai Y, Song Y, et al. Anlotinib versus sunitinib as first-line treatment for metastatic renal cell carcinoma: a randomized phase II clinical trial. Oncologist. 2019;24(8):e702–e708. doi:10.1634/theoncologist.2018-0839
54. Chi Y, Shu Y, Ba Y, et al. Anlotinib monotherapy for refractory metastatic colorectal cancer: a double-blinded, placebo-controlled, randomized phase iii trial (ALTER0703). Oncologist. 2021;26(10):e1693–e1703. doi:10.1002/onco.13857
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.