Back to Journals » Risk Management and Healthcare Policy » Volume 16
Characterization of Parental Knowledge on Early Child Sleep and Association with Child Sleep Quality: A Cross-Sectional Pilot Study in Chongqing, China
Authors Li D
Received 13 February 2023
Accepted for publication 29 April 2023
Published 10 May 2023 Volume 2023:16 Pages 851—864
DOI https://doi.org/10.2147/RMHP.S408428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Dan Li1,2
1College of Pre-School Education, Chongqing University of Education, Chongqing, People’s Republic of China; 2Children’s Research Institute, Chongqing University of Education, Chongqing, People’s Republic of China
Correspondence: Dan Li, Nanshan Campus, 1 Chongjiao Road, Nanshan Street, Nan’an District, Chongqing, 400065, People’s Republic of China, Tel +86 23 61638000, Email [email protected]
Purpose: Parental knowledge of child sleep is typically poor, and profiling of knowledge patterns has not been performed. In recent years, the Chinese government has issued a series of administrative and legal documents to promote guidance on family education and parenting knowledge. The purpose of this study was to characterize the pattern of parental sleep knowledge for 0~3-year-old children in Chongqing, China, and to examine the associations among the knowledge pattern, guidance channel, and sleep quality.
Participants and Methods: This was a cross-sectional pilot study of 264 primary caregivers of children aged 1~36 months who completed a brief survey using the 9-item Parents’ Knowledge of Child Sleep (PKCS) and a modified Chinese version of the Brief Infant Sleep Questionnaire (BISQ). Hierarchical clustering was performed to determine knowledge patterns. Logistic and multiple linear regressions were used to assess the associations.
Results: The average PKCS score was 50.2%. Parental knowledge showed a five-group pattern from I to V, with knowledge score increasing with the group number. Parents’ access to sources for guidance and information on children’s sleep was categorized into three categories from i to iii considering the authenticity of sources and richness of channels. Significant correlates of knowledge pattern were age (mo.) of the child (OR=0.97, p=0.019), low family income (vs high, OR=0.44, p=0.022; vs medium, OR=0.55, p=0.014), and information access patterns i and ii (vs iii with the lowest credibility and richness, OR=2.22/1.85, p=0.004/0.022). Knowledge pattern IV, with a few critical structural defects, showed a significant association with longer daytime napping (β=0.121, p< 0.001).
Conclusion: The child sleep knowledge of parents in Chongqing, China, was at a low level but showed characteristic patterns. Considering the social need and policy directions, it is necessary to improve public services to provide authentic and extensive guidance to strengthen parental knowledge on child sleep in Chongqing.
Keywords: parenting knowledge pattern, 0~3-year-old children, infant and toddler, sleep knowledge, information access, daytime napping
Graphical Abstract:

Plain Language Summary
Infants and toddlers aged 0~3 years are largely dependent on parental understanding of their developmental sleep needs. Caregivers should be well informed regarding children’s sleep to ensure good sleep hygiene. However, parental knowledge of child sleep is typically poor worldwide. Previous studies evaluated parental knowledge mainly by descriptive statistics; they did not analyze the internal structure of parental sleep knowledge and did not address if there were specific weaknesses. This might result in a lack of targeted sleep guidance for parents. To fill this gap, in the current pilot study, we characterized patterns of parental sleep knowledge for 0~3-year-old children in Chongqing, one of the representative emerging megacities of China and in the world. Parental knowledge showed a five-group pattern. We further found critical defects in the structure of specific knowledge patterns. For example, a group of parents having a high score of total sleep knowledge but with a few but critical points of defects reflected that their young children experienced poor sleep. Finally, we examined the associations of access channels to parenting guidance and children’s sleep quality. It is necessary to improve public services providing authentic and extensive guidance aiming to strengthen parental knowledge on early child sleep.
Introduction
A healthy sleep regimen is a critical part of normal child development; it is important for young children’s general health and learning ability1,2 and regulates their emotions and behavior.3–6 Infants and toddlers, aged 0~3 years, are largely dependent on parental understanding of their developmental sleep needs, so parents/caregivers must be well-educated in terms of children’s sleep knowledge to ensure that good sleep hygiene is maintained.7,8 However, as a universal issue, insufficient, irregular and poor-quality sleep is prevalent in children,9,10 and parental knowledge of child sleep is poor.11 To address this problem in China, Guidelines on Promoting the Development of Care Services for Infants and Young Children Under 3 Years of Age (2019) issued by the General Office of the State Council clearly indicated that “the focus of developing care services for infants and toddlers is to provide scientific parenting guidance for families”, in which the guidance of parents’ sleep knowledge for children and the improvement of children’s sleep quality have become the key content.12 With the promulgation of the Family Education Promotion Law in 2021, the provision of parenting guidance and sleep education to families rearing infants and toddlers has been elevated to a mandatory legal issue.13
Sleep hygiene, also called healthy sleep practices, has been empirically linked to better quality and more adequate sleep in children. Healthy sleep practices include regular sleep-wake schedules, appropriately early bedtimes, a bedtime routine, healthy settling methods, a restful sleeping environment, adequate daytime activities, and so on.14,15 Sleep practices are learned behaviors; therefore, by definition, they are amenable to education efforts targeting behavior change. Behavioral education interventions aiming to promote healthy sleep in infancy and early childhood have shown some success.16–19 Generally, more knowledgeable parents are more likely to report that their children exhibit healthy sleep practices; however, McDowall et al reported that an increase in parental knowledge was observed in the short term, but effects were not maintained at follow-up.11 As parents have uneven reserves of sleep knowledge and different experiences of child sleep practices, common nontargeted sleep guidance might not fill the specific gaps and improve the various weaknesses in their knowledge of child sleep. Therefore, to develop more effective guidance, a prerequisite is to identify the knowledge patterns of parents/caregivers regarding child sleep. Such work has not yet been done.
The purpose of this study was to create, for the first time, a preliminary profile of parental knowledge on child sleep in Chongqing, the largest municipality directly under the central government of China. This emerging megacity is among the typical representative municipalities of China, which has been urbanizing rapidly and which has a high proportion of immigrants and former agriculturalists in its resident population. Our specific goals were (i) to profile parents’ sleep knowledge for 0~3-year-old children; (ii) to identify information access associated with variation in the identified profiles and (iii) to understand how sleep knowledge and the resulting practices correlate with the sleep quality of 0~3-year-old children.
Materials and Methods
Participants and Procedure
Parents/primary caregivers of young children aged 0~3 years were recruited from 21 out of the 38 districts/counties/autonomous counties of Chongqing. A two-stage convenience sampling procedure was used. Basically, students from the 21 areas of Chongqing who were taking the course Family Education and Guidance for Infants and Toddlers Aged 0~3 Years were asked to find and investigate eligible parents in their hometowns during the first week of October 2021. In this stage, investigations were performed by household survey or over the phone, and they were part of the course assignment. All participating parents gave informed consent before the formal survey. At a second stage, the participants were encouraged to forward an online session request via the Sojump app (SurveyStar Corp., Changsha, China), which had identical questionnaires, to other parents. All online responses were collected by late October 2021; they were deidentified, and informed consent was double-checked at the beginning and completion of the questionnaire. Ethics approval (Ref. No. 2021092201H) was obtained from the Children’s Research Institute, Chongqing University of Education.
The inclusion criteria of this study were as follows: (1) the child’s age was 0~36 months at the time of investigation; (2) the child was born a singleton without severe physical disability and was not subject to critical environmental risk factors that may affect growth and development; (3) the child did not use drugs that could affect sleep within the last three months; and (4) the primary caregiver had a clear understanding of the child and his or her sleep (assessed based on parent self-reports that they accompanied their children for more than 6 hours per day and put them to sleep at least two days per week).
Parents/primary caregivers of 177 families completed the household/telephone survey, for a response rate of 83.5%. Two parents with medical training were eliminated from further analysis because their children had suffered from severe sleep disorders. One questionnaire was eliminated due to incomplete responses to the Parents’ Knowledge of Child Sleep (PKCS) scale, leaving 174 valid samples. In addition, 90 valid responses were received out of the 95 completed online questionnaires. However, it was impossible to calculate the total number of E-surveys that may have been disseminated by participants. For example, a parent could have forwarded a link to the questionnaire to other parents without the knowledge of the authors. Thus, a return rate could not be calculated in this respect. The final sample included 264 participants.
Measures
Sleep Assessment
Brief Infant Sleep Questionnaire (BISQ). The BISQ is a sleep questionnaire aimed at assessing the infant’s average sleep patterns. The parents are instructed to refer to their infant’s regular sleep. The questionnaire was validated in a previous study, and its measures were found to be highly correlated with sleep diary and actigraphic measures.20 In this study, the Chinese version of the BISQ enclosed in the Guideline for Sleep Hygiene Among Children Aged 0~5 Years, a standard of the Health Industry of the P.R. China,21 was adopted with a few modifications. The derived measures were (a) night-sleep duration, 7 p.m.~7 a.m.; (b) accumulated daytime naps duration, 7 a.m.~7 p.m; (c) number of nighttime awakenings; (d) accumulated time of nighttime awakenings, 10 p.m.~6 a.m.; (e) sleep latency, based on the reported length of time it took the child to fall asleep; and (f) bedtime. The categorical items included (1) sleep site, such as in a crib in a separate room, in a crib in the same room with the caregivers, or in the same bed with the caregivers; (2) sleep initiating manner, such as independent (falling asleep by oneself), accompanied (lying in bed but with parents alongside), cuddled or patted/rocked (being held in the caregivers’ arms until falling asleep), or breast/bottle fed; and (3) degree of difficulty sleeping, such as none, somewhat and very. The reliability and validity of this slightly modified BISQ (Chinese version) were acceptable as the Cronbach’s alpha coefficient was 0.682 and the Kaiser‒Meyer‒Olkin’s (KMO) value was 0.674 which was strongly significant (p<0.005) according to the Bartlett’s sphericity test.
Sleep Knowledge
Parents’ Knowledge of Child Sleep (PKCS) Questionnaire. To assess sleep knowledge, parents were required to respond to 9 true-or-false questions on child sleep. We referred to the Parents’ Sleep Knowledge Inventory (PSKI), composed of 62 items,22 and the 10-item measure developed by Owens et al,23 with slight modifications to adhere to the local context and timeliness. A few questions were created as an adaptation of the items from the Guideline for Sleep Hygiene Among Children Aged 0~5 Years21 and added to the PKCS to provide more comprehensive coverage of child sleep knowledge. The questions and correct answers are shown below:
(Q1) Breastfeeding has been found to decrease an infant’s ability to sleep soundly throughout the night; T
(Q2) From the age of 3 months, a consistent and pleasant bedtime routine can be established; T
(Q3) Toddlers, aged 2~3 years, typically have trouble sleeping when they use a security object (eg, a blanket, teddy bear) to go to sleep; F
(Q4) It is normal for an infant (up to 24 months) to have difficulty sleeping alone versus sleeping with a parent; F
(Q5) Infants, up to 24 months old, should sleep at a temperature no less than 26°C; F
(Q6) Parent viewing a screen when accompanying a child at bedtime does not affect the child falling sleep; F
(Q7) One-year-olds typically go to bed before 9 pm, sleep soundly throughout the night and take one nap during the day; T
(Q8) It is considered unnecessary for toddlers (aged 1~3 years) to get enough exercise in the daytime; F
(Q9) For infants who have high fever, sweating to cool is more conducive to sleep than the use of a cooling patch; F
A panel from the Children’s Research Institute comprised of professionals in pediatrics, early education, and family education reviewed the questionnaires on the basis of their expertise. The reliability as represented by Cronbach’s alpha coefficient was 0.738, and the validity using Kaiser‒Meyer‒Olkin’s test showed KMO=0.706, which was extremely significant (p<0.001) according to Bartlett’s sphericity test.
Additionally, parents were asked to give a self-evaluation of their mastery level of children’s sleep knowledge. The options were abundant, average and deficient.
Access to Sleep Guidance
At the end of the survey, the participants were asked to answer a multiple-choice question: “What channels do you use often to acquire information about improving children’s sleep?” The response options included child health clinics, specialized books/periodicals, on-site public lectures by experts, paid consultation by experts, TV programs, early education and instruction (on parent‒child activities for children aged 0~3 years specifically carried out by early education institutions and corporations), community education, public networks, and shared experiences from people around. An additional blank option was provided for free-text responses if more approaches had been accessed. However, only 6 responses were received, such as own experience or self-enlightened, and they provided no more useful information, so this item was excluded from further analysis.
Statistical Analysis
Descriptive statistics and frequencies were used to show the basic information of 0~3-year-old children and their families with different sociodemographic statuses. The descriptive measures of sleep and other continuous variables were slightly skewed; nevertheless, one-way analysis of variance (ANOVA) was conducted due to its robustness to nonnormality.24 Duncan’s multiple test and least-significant difference (LSD)-t-test or Games-Howell post hoc test were used for pairwise comparisons between groups dependent on the homogeneity of variance. The chi-square test was used for categorical variables, and Kendall’s tau-b correlation was used for ordinal variables. Associations between continuous and categorical variables were measured through Spearman rank-ordered correlations. Logistic regressions were performed to explore the potential factors associated with the profiling of parental knowledge of child sleep. Multiple linear regression analysis was used to evaluate the influencing factors of sleep quality. All these analyses were performed using the SPSS Statistics 22 program (IBM, USA). Statistical significance was set at p<0.05. Profiling of parental knowledge based on the PKCS questionnaire and the identification of channels by which parents acquired education information on child sleep were performed by clustering analysis using Unscrambler 10.4 (Camo, Norway). A heatmap was drawn using Excel 365 (Microsoft, USA).
Results
Sample Characteristics
Table 1 shows the descriptive demographic variables for the study sample. Nearly half of the infants and toddlers were boys (51.1%). The average age of the young children was 19.12±9.89 months old, and the number of their primary caregivers ranged between 1~4 and averaged approximately 2. The educational level of mothers was considerably higher than that of fathers, with 91.7% of mothers vs 86.4% of fathers reporting high (obtained graduate and bachelor’s degree) or medium (finished a high school or higher vocational education) education levels. More than 60% of the surveyed families lived in central urban areas, while less than 10% of them lived in the countryside. The proportions of the three levels of household income, low (<30,000 CNY), medium (≥30,000 CNY and <300,000 CNY), and high (≥300,000 CNY), were 46.6%, 41.3% and 12.1%, respectively.
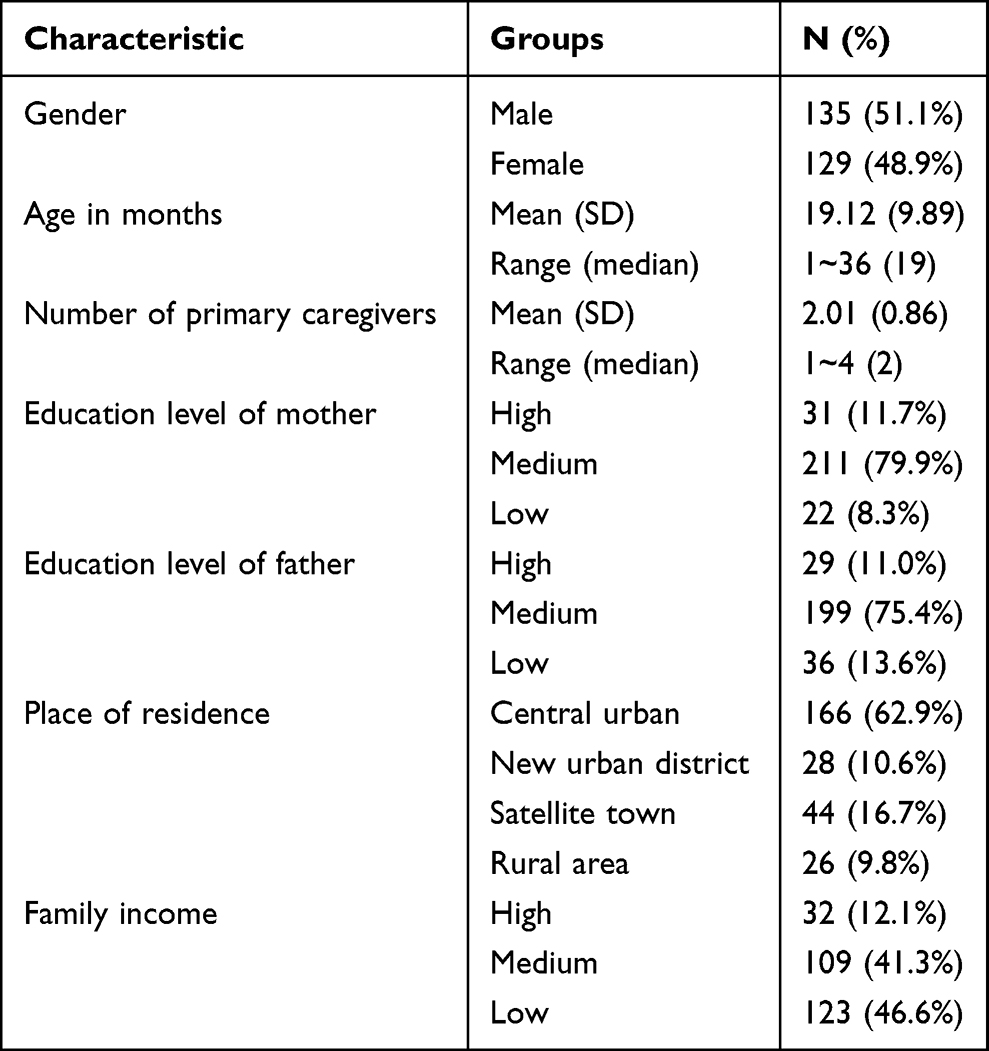 |
Table 1 Demographic Characteristics of Infants/Toddlers and Their Families (N=264) |
Profiling and Clustering of Parental Knowledge on Early Childhood Sleep
Across all participants, the total correct PKCS score (maximum possible score = 9) for each participant was calculated, with missing items counted as incorrect. Parents scored between 0 (no question correct, 0.8%) and 9 (all questions correct, 8.0%), with 47.3% of parents receiving scores ≥5. The average correct rate was 50.2%.
The nine questions of the PKCS, which correspond to nine essential factors that affect children’s sleep practices, cover the three fundamental aspects of sleep knowledge, viz. sleep onset routine, sleep environment, and everyday hygiene. These questions were randomized in the questionnaire to avoid mutual interference within the knowledge category. The profile of the parent/caregiver’s cognition about child sleep-related knowledge is shown in Figure 1. The scoring matrix, 9 questions × 264 participants, was visually presented as a heatmap, where each correct response was labeled with a red bar. Specifically, Q1 (settling methods), Q2 (sleep ritual) and Q3 (comforter), which assessed caregivers’ cognition of the bedtime routine, had scoring rates of 56.1%, 37.0% and 21.4%, respectively. Parents were less informed about the latter two factors, showing the lowest correct score rate among all nine questions. Q4 (sleep site), Q5 (temperature) and Q6 (light), assessing knowledge of environmental conditions, had an average score of 41.2%, which was slightly higher than that of the routine part, which had an average score of 38.2%. Parents better understood the importance of everyday hygiene to children’s sleep, with correct score rates of 66.8%, 68.3% and 82.1% for Q7 (regular daily schedule), Q8 (daytime activity) and Q9 (disease and discomfort), respectively.
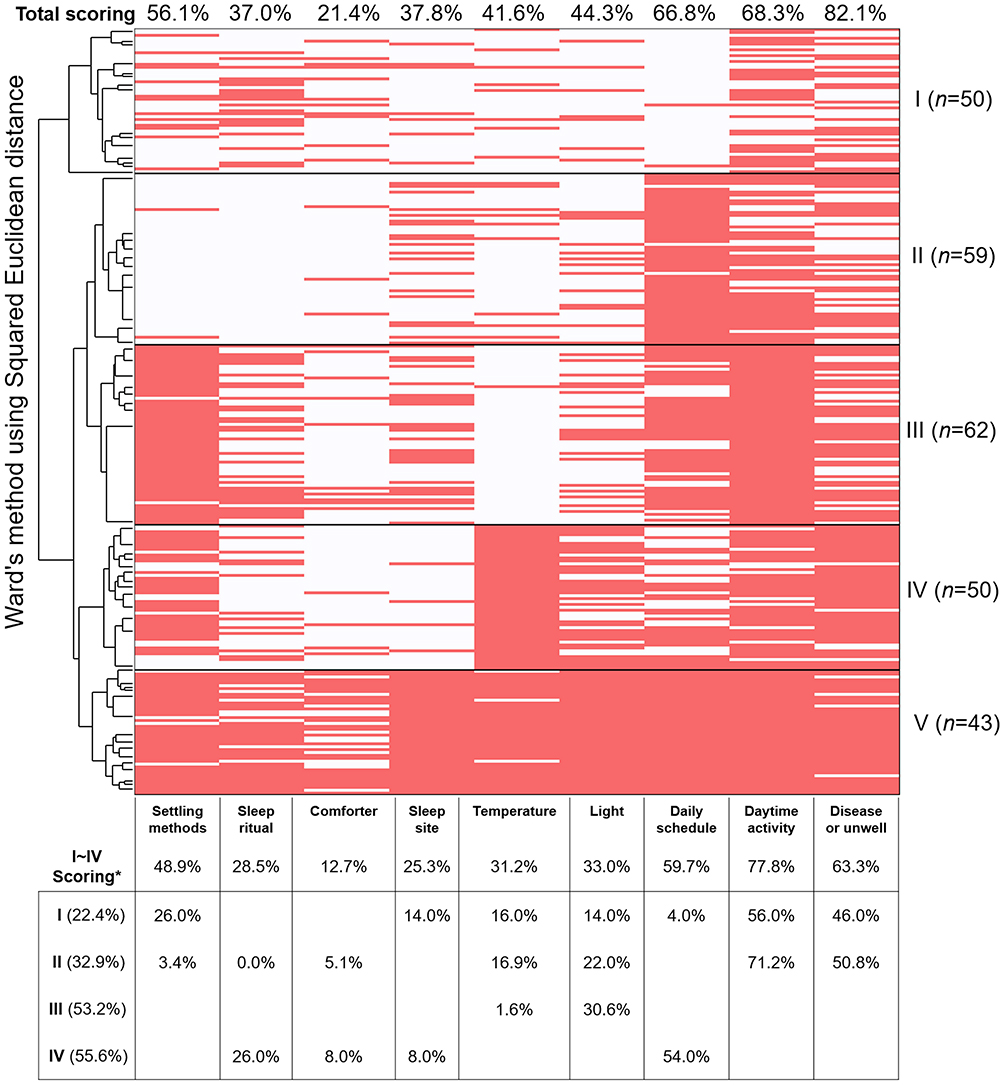 |
Figure 1 Profile and Groupings of the caregivers’ cognition about child sleep related knowledge. The table underneath showed the deficient aspects of each group of which scoring rate lower than the average. *Cluster V showed a very high score in all the 9 aspects of sleep related questions (average 91.0%); it was set as a reference group and not included to calculate the scoring average. |
The knowledge pattern of parents was further revealed using hierarchical clustering analysis with Ward’s method and the binary squared Euclidean distance. The results showed that the best grouping number was five to meet the criteria for even classification and practical meanings. Figure 1 exhibits the classification tree and the consequent knowledge patterns from I~V. Generally, the total scoring average increased in the numerical order of groups, and the scoring distributions were found to be highly characteristic among the five groups. The 43 parents in Group V received a 91.0% accurate score rate and even had full marks for four questions, showing sound knowledge of all nine factors. The only comparative deficiency in their knowledge structure for the comforter question (~65% correct rate). Groups II, III and IV, comprising 59, 62 and 50 individuals, respectively, showed at least one factor relating to sleep that they understood very well, eg, regular daily schedule for Group II, settling methods and daytime activities for Group III, and temperature for Group IV. However, Group I (n=50) showed a poor knowledge profile in almost all aspects.
Furthermore, the sleep knowledge deficit of each group excluding group V was analyzed. Individual correct answer rates lower than the total average of groups I to IV are simply listed beneath the heatmap. The results showed that for Group I, the participants’ cognition of all aspects of sleep knowledge except for the sleep ritual and comforter was well behind the average. For Group II, the correct score rate for the three questions on bedtime routine was extremely low (0.0%~5.1%), and the participants’ cognition of environmental conditions such as temperature and light was also significantly lower than the average. Group III had the lowest cognition of temperature, and Group IV had the lowest correct score rate on the sleep site question and the second lowest on the comforter question.
Relationship of Information Access and Demographic Variables of Sleep Knowledge
Empirically, the shaping of knowledge is directly related to the acquisition of information and guidance and implicitly involves demographic relations. All these potential factors were considered and analyzed using chi-square tests. The results showed that there were statistically significant differences in the parents’ sleep knowledge pattern among choices/categories of the following three variables: access channels of information (χ2=76.4, p<0.001), age in months (χ2=28.9, p=0.004), and family income (χ2=17.9, p=0.022). In addition, correlations with the knowledge pattern were found for the latter two factors using a chi-square test for trend, with χ2=5.1 and 5.5, respectively, and p<0.05. Kendall’s tau-b coefficient showed a weak correlation between knowledge groups and month groups/income groups (R=−0.125/0.127, p=0.010/0.015), indicating that the older the children and the lower the family income were, the smaller the knowledge pattern group number was.
Patterning of Information
The internal structure of the multiple-choice data of access to information was studied using the classification procedure as described in Section 3.2. The parents were classified into three groups, and the results are shown in Table 2. Overall, child health clinics and social media were most common channels and were evenly adopted across all the groups; they represented public services affordable for most families, and approximately half (45.7%~57.4%) of the parents chose each of them. On average, paid consultations, on-site lectures by experts, and community outreach were the least commonly used channels, with only 2.3%~6.8% of the parents using them. The access rate of early education and instruction was less than 20% on average, and each group was not far from others.
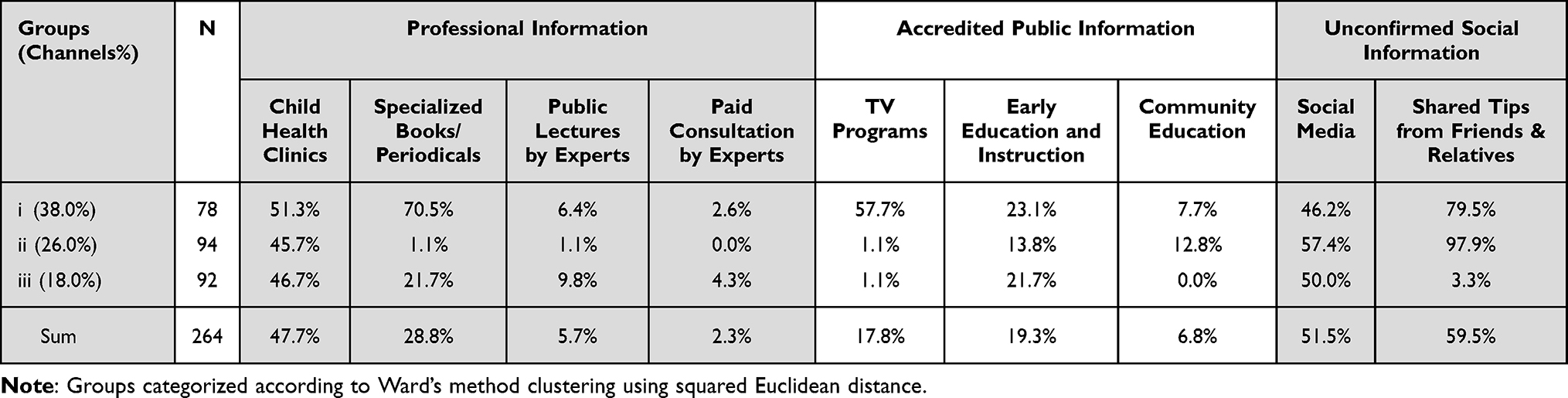 |
Table 2 Frequency Distribution of the Three Parent/Caregiver Groups to Obtain Information/Guidance on Improving Children’s Sleep |
In addition, the nine channels led parents to three different sources of information, ie, professional (by the first four channels), accredited public (by the next three), and unconfirmed social (by the last two). Interestingly, specialized books/periodicals, TV programs, and shared tips from friends and relatives, which constituted the major differences in access to sleep information that determined the clustering of the parent groups, fell into the three information sources. Specifically, Group i parents adopted specialized materials (70.5%) and TV programs (57.7%) much more often than the other two groups did. Group i parents were also good at learning from the experiences of people around them (79.5%). In this way, Group i showed a pattern of obtaining sleep information that valued both the credibility and richness of sources. A second pattern, as shown by Group ii parents, was characterized largely by shared tips (97.9%), the correctness of which was unconfirmed and questionable in terms of practicability. Group iii represented another pattern. Although they considerably preferred professional information, their total channel usage (18.0% iii vs 26.0% ii and 38.0% i) for sleep information and guidance was the narrowest.
Considering the orderly pattern of access to information, the chi-square test for trend analysis was conducted among the three groups and the five categories of parents’ sleep knowledge profile. The results showed a linear correlation χ2=7.7, p=0.005 and a Kendall’s tau-b correlation coefficient R=0.144, p=0.006, which was a very significant correlation.
Multivariate Analysis of Sleep Knowledge
An ordinal logistic regression analysis for sleep knowledge was performed using information pattern and household income as independent variables and children’s months of age as the covariate. The fitted model was valid, and the estimated parameters, when only considering the main effects of the multiple factors, are shown in Table 3. The parameters predicted the following: (1) Months of age. The knowledge pattern of parents who had older children tended to be significantly less comprehensive and abundant (small group number) than those who had younger children, with an odds ratio, OR (exponential of B) =0.97 and p=0.019. (2) Family income. Compared with high-income families, parents in low-income families were more likely to have less comprehensive sleep knowledge (OR=0.44), and the difference was significant (p=0.022). Parents in middle-income families showed a similar trend of less comprehensive sleep knowledge (OR=0.79); however, the difference was not significant. Additionally, compared with medium-income families, which were recoded as the reference group, low-income families showed a likelihood of significantly lower scores for parental knowledge (OR=0.55, p=0.014). (3) Information pattern. The more diverse and reliable the information accessed was (following the order iii, ii and i), the more comprehensive the knowledge pattern would be. The OR values of Group i and ii to Group iii were 2.22 (p=0.004) and 1.85 (p=0.022), respectively, whereas the OR of Group i to ii was 1.20, showing no significant difference.
 |
Table 3 Ordered Multivariate Logistic Regression Analysis Showing Factors That Influence Parental Knowledge of Child Sleep |
Parental Knowledge and Sleep Quality of Children
Factors Relating to Sleep Quality
Children’s sleep quality, indicated by the 6 measures reported and the degree of child difficulty sleeping self-rated by parents in the BISQ, was studied to identify the differences among categories of related variables, namely, parental knowledge pattern, self-evaluated level of sleep knowledge, sleep initiating manner, and sleep site. The first three variables could be treated as ordinals, and therefore, they were further analyzed for Spearman rank-ordered partial correlations, controlling for child age, with sleep quality. Bedtime (21:18±1:00~21:36±1:12) and night-sleep duration (9.2±1.3~10.0±1.0 h) showed no significant difference among or correlation with any factor. The other results are shown in Table 4.
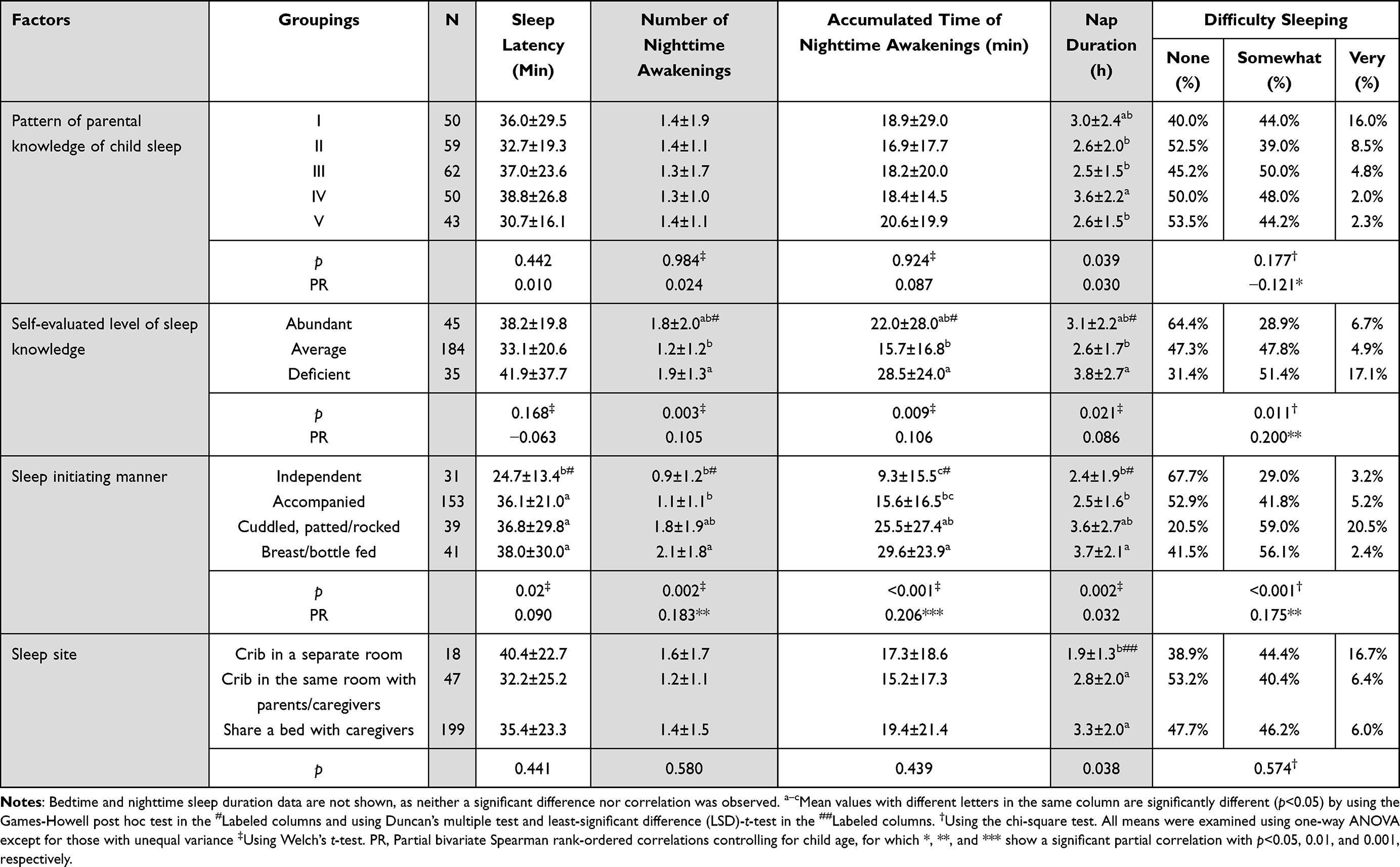 |
Table 4 Univariate Analysis and Partial Correlations with Children’s Sleep |
A significant difference in daytime nap duration was observed among categories of all four factors (p<0.04). All the listed sleep quality items showed significant differences among the sleep initiating manner groups (p<0.02). The degree of difficulty sleeping was significantly correlated with the three ordinal variables; coefficients were negative for parents’ knowledge pattern and positive for levels of sleep knowledge and sleep initiating manner. Sleep initiating manner was also positively correlated with the night-waking numbers and accumulated awake time, with partial coefficients statistically significant but weak.
Multivariate Analysis for Nap Duration and Difficulty Sleeping
A multiple linear regression method was used to analyze the potential influencing factors of daytime nap duration. Although there were significant differences among all four factors, correlations were not found, as shown in Table 4. Therefore, the factors were included in the linear regression as unordered categorical variables and were further converted into dummy variables. A stepwise regression was performed using the backward method. The results showed that the regression model was valid, with F=7.100 and p<0.001. Independence and normality tests were passed, and homogeneity of variance existed. There was no multicollinearity between each independent variable.
As shown in Table 5, the optimized model included five independent variables from three factors: knowledge pattern, sleep initiating manner, and sleep site. The estimated parameters showed that (1) of the knowledge patterns, category IV significantly predicted longer daytime naps, with a standardized coefficient β=0.121 and p<0.05; (2) of the sleep initiating manners, compared with cuddled/patted/rocked and fed to sleep, independent (β=−0.117 and p<0.01) and parent-accompanied (β=−0.298 and p<0.001) sleeping significantly predicted shorter nap duration; and (3) among the sleep sites, crib in a separate room and crib in the same room with parents both predicted shorter (β=−0.124 and −0.102) nap duration than a shared bed with parents, and the former had a significant effect (p<0.05). These variables explained 12.1% of the total variance in daytime napping.
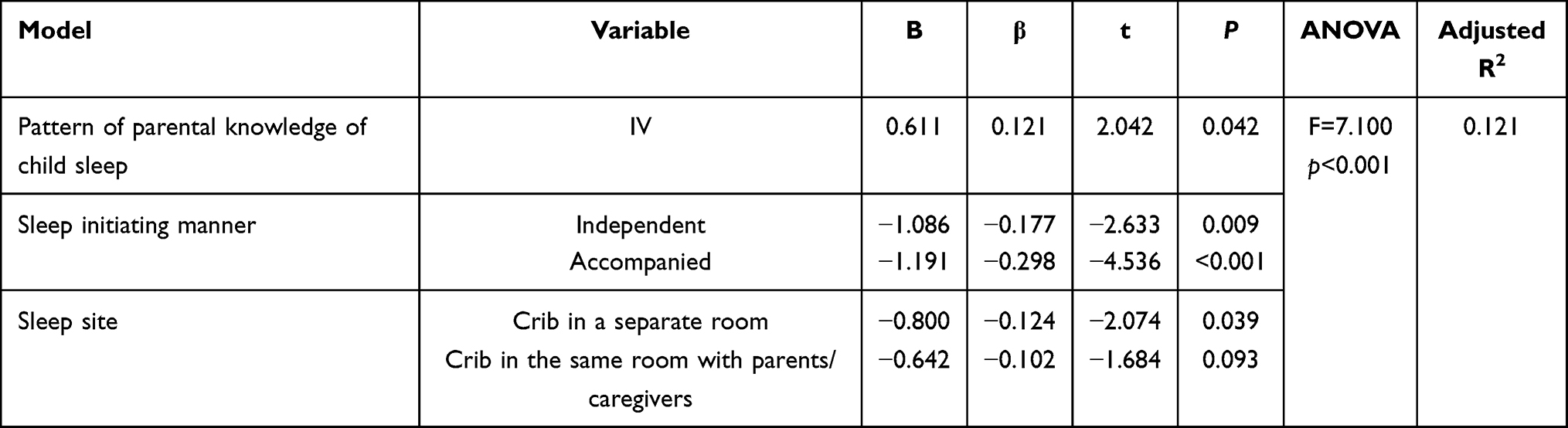 |
Table 5 Multiple Linear Regression Analysis of the Factors Influencing Nap Duration |
Similarly, a multinomial logistic regression analysis of children’s difficulty sleeping was performed in a backward stepwise manner. The fitted model, for which a difficulty level of “none” was set as the reference group, was highly significant (χ2=45.3, p<0.001), and the results showed that (1) compared with knowledge pattern I, all the other patterns predicted less difficulty sleeping, which was significant for the very difficult group (p=0.017) and nonsignificant for somewhat difficult; (2) compared with a deficient level of sleep knowledge, abundant and average levels predicted significantly less difficulty sleeping; (3) cuddled/patted/rocked to sleep exerted a significantly greater effect on difficulty sleeping than all the other sleep initiating manners; and (4) younger children were more likely, yet not significantly more likely, to have difficulty sleeping as expected given developmental trends.
Discussion
Parental knowledge of child sleep needs and healthy sleep practices is typically poor but variable.11 In the current study, the correct score rates of the 264 participating Chongqing parents for the 9 questions averaged 50.2%. A cross-sectional investigation of parents of preschool children (3~6 years) who completed a 17-item questionnaire in Jiangsu Province of China showed a 48.0% correct rate.25 Two studies by Owens, Jones et al used a 10-item questionnaire measuring knowledge about healthy sleep practices among parents in the USA whose children were aged between 3 months and 12 years; the results showed that their mean numbers of items answered correctly were 4.33 and 4.39, respectively.17,23 Parents of children aged 2~12 years in New Zealand, n=115, correctly answered half of the items (5.14±2.37) using a modified 10-item scale.26 The average correct answer rate of the PSKI items pertaining to infants was approximately 44% in a study of 170 Australian and American parents.22
In addition to the generally poor knowledge level, with correct score rates of approximately 43%~51%, some structural weaknesses in parental knowledge of child sleep were consistent between the current findings and those reported by Schreck and Richdale and Chen et al22,25 For example, the effects of a comforter/security object, the sleep site, and the physical environment were correctly understood by only 21.4%~38.0%, 19.2%~37.8% and 16.1%~41.2% of parents, respectively, from Chongqing and Jiangsu, China, the United States and Australia, which were even lower than their respective general means.
We examined the relations of parental knowledge and sample demographics, for example, parent education, income, family location, and age. Ordinal logistic regression showed that household income and children’s age significantly predicted differences in parental knowledge. Compared with age in months, OR=0.97, which predicted a mild decrease in knowledge scores, low income (OR=0.44) was associated with a drastic decline in sleep knowledge. No study has reported similar results before. This might reflect the characteristics of Chongqing, which has been urbanizing extremely quickly. The largest megacity of China and probably one of the largest in the world, Chongqing covers an area equal to the Republic of Serbia in Europe or South Carolina in the States. In just 25 years, less than a generation, over 3 million people have become citizens, with former agriculturalists and immigrants accounting for a large proportion of this population. A reasonable inference is that before the city fully implemented its public services, such as parenting education and childcare information, parents had already constructed parental knowledge based on their experiences and cognitive competence from their social class, which would be simply and roughly reflected by family income.
Due to the sharp decline in the birth rate in China, the demand for quality infant and early childhood care has increased. Providing essential guidance services to families nurturing young children has become a prominent issue that the government and society pay attention to. The National Guidelines for Family Education (Revised), 2019, jointly issued by the All-China Women’s Federation, Ministry of Education, and seven other ministries and commissions, specifically pointed out that the first important task for family guidance is to maintain infants’ and young children’s good sleep, mood and health.27 The guidance on parental sleep knowledge and the improvement of sleep quality of infants and toddlers has become the key content of family education guidance for children aged 0–3 years. These experiences and efforts may provide useful references for the developing countries and regions which are facing a rapid urbanization and adjustment of population pyramid and where parent education is much-needed to improve children’s sleep hygiene.
Therefore, we are concerned about the channels through which parents acquire information and receive guidance from parental knowledge, as these channels can directly influence the shaping of specific knowledge patterns. By evaluating two dimensions of the source property, ie, reliability and richness, the information pattern of the investigated parents in Chongqing was characterized into three groups: credible and well-rounded, less credible and poorly informed, and less credible and the narrowest. Conventionally, primary care physicians were often looked to for guidance relating to common sleep issues of children;28 information and training for parents were mostly provided by child health clinics and professionals.29 However, this conventional pattern overlooked the parent motivation and multiple channels to access information, especially in an era prevailing of social media and online resources. As might be expected, we found that more than half of parents use social media to seek information on children’s sleep, ranking as the second most frequently used channel. We further confirmed the hypothesized association of parents’ knowledge pattern and sleep information pattern: the sounder and richer the information is, the more abundant the knowledge on children’s sleep.
Noticeably, the access rates of child health clinics (47.7%), early education and instruction (19.3%), community education (6.8%), and public lectures by experts (5.7%) were still very low in Chongqing. These are public services that are affordable or free for most families and that provide highly accredited information; thus, there is a good reason to expend every effort to improve their coverage rate.
Daytime napping has been recognized as an important indicator of sleep quality and regulation for young children, contributing to children’s social-emotional functioning.30 Napping is also considered compensation for inadequate or poor-quality night sleeping. One finding showed that more night waking was related to more frequent and longer naps.31 In our study, a significant correlation of the accumulated awake time and nap duration was also found, R=0.327 and p<0.001. Long naps leading to insufficient sleep need at bedtime were introduced to understand the homeostatic regulation of sleep in an intervention training program.7
The parental knowledge profile found in this study showed a five-group pattern in which the acquisition of children’s sleep knowledge increased as the group number increased. However, we found that parents possessing knowledge pattern IV, characterized by the second most abundant knowledge (scoring=55.6%), tended to report significantly longer daytime naps for their children, which was interpreted as indicating a poor quality of night sleep. This result is at odds with the common sense that greater knowledge in a domain leads to better outcomes in guiding practice. It is worth scrutinizing the knowledge structure.
As shown in Figure 1, pattern IV parents’ performance on questions regarding the sleep site and comforting objects was the lowest and second lowest (ea. 8.0%). No other patterns showed this combination of deficiency. Corresponding to the lack of knowledge on the sleep site, putting a child in a crib in a separate room or a crib in the same room with the parents together came in at 18.1% for the parents in pattern IV, which was the lowest proportion compared with the other four patterns (22.1%~30.2%). As sleep comforters/security objects are helpful for children to develop self-soothing ability, they have been recommended for use and are especially useful in the practice of independent and accompanied sleeping.21 However, consistent with the lack of knowledge on comforters, the lowest ratio of independent and caregiver accompanied sleep was observed in pattern IV, at 58.0% vs the others at 64.0%~83.0%. All these inferiorities predicted longer daytime napping, as derived by the linear regression model shown in Table 5.
This finding suggests that even for parents with relatively rich general knowledge on child sleep, due to the lack of a few critical points (in this case, a combination of extremely low cognition of sleep location and comfort), poor sleep practices might be externalized, resulting in a decline in children’s sleep quality.
This study has a few limitations. First, the interviewees in this study were mostly parents (93.5%), but 21.6% of families had more than two primary caregivers. Considering the internal exchange of sleep knowledge and information, there may be inconsistency and bias. Second, to guarantee an acceptable completion rate and recovery of the PKCS, one basic question was used for each of the 9 factors to keep the questionnaire concise and short. This all-or-none approach might have resulted in either over- or underestimation of a specific point of the knowledge. Third, this was a cross-sectional study, which rarely present sound causality between identified correlates. Longitudinal data are warranted to further confirm the causal relationships among access to information, knowledge patterns and sleep practice and quality. Last, we did not consider the effects of COVID-19 on the data collection and children’s sleep quality. Although Chongqing had been largely unaffected by China’s “dynamic zero-COVID” strategy, lockdowns of other regions might have influenced the local lifestyle unavoidably. Cerasuolo et al reported that sleep schedules were delayed in toddlers during the Covid-19-related lockdown in Italy.32 A delayed schedule could increase the number of naps during the day and the waking time during the night. To sum up, this is a pilot study with inspiration but limitations; a further research requires more careful design of the method, better arrangement of the sampling procedure, and inclusion of more representative population to strengthen the statistical steadiness and practical significance of the findings.
Conclusion
The profile of knowledge of sleep among 0~3-year-old children that parents in Chongqing acquired was outlined. The knowledge pattern, which was composed of responses regarding the bedtime routine, environmental conditions, and related daily hygiene questions, was further clustered into 5 categories, basically reflecting different levels and degrees of sleep knowledge. The channel through which children’s sleep information was accessed and family income showed significant correlations with the knowledge profile. Accessing information sources with high reliability and richness as well as earning higher family incomes were associated with more comprehensive sleep knowledge. The reported child sleep quality elements, such as daytime napping and difficulty sleeping, were significantly correlated with parental knowledge patterns and sleep practices. Knowledge pattern IV, with a few but critical structural defects, predicted increases in nap duration, which is linked with poor-quality night sleep. We suggest that public services should improve the provision of authentic and rich guidance aiming to strengthen parenting knowledge on child sleep.
Ethics Approval and Informed Consent
This study scheme was reviewed and approved by the Ethics Committee of Children’s Research Institute, Chongqing University of Education (Ref. No. 2021092201H). We conducted this study under the Declaration of Helsinki. Participants were informed that filling in and submitting the questionnaire would be considered as informed consent.
Acknowledgments
The author thanks all the participating students for their team collaboration work and all the parents involved in this study for their cooperation. Many thanks to my son, little Pomelo, and all my family members for their support. Special thanks to dear reverent Mr. Da Xiong @ Xingerswz Community for his heartwarming, wise and professional guidance.
Funding
This work was supported by the Humanities and Social Science Research Project of Chongqing Municipal Education Commission (Grant No. 23SKGH357), the Family Education Research Center for children aged 0–6 years of Chongqing University of Education (Grant No. 16XJP03), and Young Scholar Funding of Chongqing Bayu Scholars Program (PI: DL, 2021~2024). The funding sources listed had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Galland B, Spruyt K, Dawes P, McDowall PS, Elder D, Schaughency E. Sleep disordered breathing and academic performance: a meta-analysis. Pediatrics. 2015;136(4):E934–E946. doi:10.1542/peds.2015-1677
2. Curcio G, Ferrara M, De Gennaro L. Sleep loss, learning capacity and academic performance. Sleep Med Rev. 2006;10(5):323–337. doi:10.1016/j.smrv.2005.11.001
3. Jiang L, Shi X, Wang Z, Wang S, Li Z, Wang A. Sleep problems and emotional dysregulation mediate the relationship between childhood emotional abuse and suicidal behaviors: a three-wave longitudinal study. J Affect Disord. 2021;295:981–988. doi:10.1016/j.jad.2021.09.003
4. Prehn-Kristensen A, Molzow I, Foerster A, et al. Memory consolidation of socially relevant stimuli during sleep in healthy children and children with attention-deficit/hyperactivity disorder and oppositional defiant disorder: what you can see in their eyes. Biol Psychol. 2017;123:196–204. doi:10.1016/j.biopsycho.2016.12.017
5. Berger RH, Miller AL, Seifer R, Cares SR, Lebourgeois MK. Acute sleep restriction effects on emotion responses in 30-to 36-month-old children. J Sleep Res. 2012;21(3):235–246. doi:10.1111/j.1365-2869.2011.00962.x
6. Nolte N, Pott W, Pauli-Pott U. Sleeping problems and attachment quality in toddlers. Psychother Psychosom Med Psychol. 2006;56(3–4):154–161. doi:10.1055/s-2005-915342
7. Whittingham K, Palmer C, Douglas P, Creedy DK, Sheffield J. Evaluating the “possums” health professional training in parent-infant sleep. Infant Ment Health J. 2020;41(5):603–613. doi:10.1002/imhj.21885
8. Vilvens HL, Vaughn LM, Southworth H, Denny SA, Gittelman MA. Personalising safe sleep messaging for infant caregivers in the United States. Health Soc Care Community. 2020;28(3):891–902. doi:10.1111/hsc.12920
9. El-Sheikh M, Buckhalt JA. Moving sleep and child development research forward: priorities and recommendations from the srcd-sponsored forum on sleep and child development. Monogr Soc Res Child Dev. 2015;80(1):15–32. doi:10.1111/mono.12142
10. Hash JB, Oxford ML, Fleming CB, Ward TM, Spieker SJ. Sleep problems, daily napping behavior, and social-emotional functioning among young children from families referred to child protective services. Behav Sleep Med. 2020;18(4):447–459. doi:10.1080/15402002.2019.1611579
11. McDowall PS, Galland BC, Campbell AJ, Elder DE. Parent knowledge of children’s sleep: a systematic review. Sleep Med Rev. 2017;31:39–47. doi:10.1016/j.smrv.2016.01.002
12. Xia R. Infant Care: china issues guidelines to improve services for children under 3. China Global Television Network; 2019. Available from: https://news.cgtn.com/news/35516a4d35494464776c6d636a4e6e62684a4856/index.html.
13. Agency XN. China adopts new law on family education promotion; 2021. Ministry of Education, PRC. Available from: http://en.moe.gov.cn/news/media_highlights/202110/t20211025_574765.html.
14. van Bindsbergen KLA, van der Hoek H, van Gorp M, et al. Interactive education on sleep hygiene with a social robot at a pediatric oncology outpatient clinic: feasibility, experiences, and preliminary effectiveness. Cancers. 2022;14(15). doi:10.3390/cancers14153792
15. Jarrin DC, Abu Awad Y, Rowe H, Noel NAO, Ramil J, McGrath JJ. Parental expectations are associated with children’s sleep duration and sleep hygiene habits. J Dev Behav Pediatr. 2020;41(7):550–558. doi:10.1097/DBP.0000000000000818
16. Stremler R, Hodnett E, Lee K, et al. A behavioral-educational intervention to promote maternal and infant sleep: a pilot randomized, controlled trial. Sleep. 2006;29(12):1609–1615. doi:10.1093/sleep/29.12.1609
17. Jones CHD, Owens JA, Pham B. Can a brief educational intervention improve parents’ knowledge of healthy children’s sleep? A pilot-test. Health Educ J. 2013;72(5):601–610. doi:10.1177/0017896912464606
18. MacDonald LL, Gray L, Loring W, et al. A community-based sleep educational intervention for children with autism spectrum disorder. Res Autism Spectr Disord. 2021;81:101719. doi:10.1016/j.rasd.2020.101719
19. Sheares BJ, Lamm CI, Leu CS, et al. Efficacy of an educational and behavioral intervention to increase nightly sleep duration in urban latino and African American early school-aged children: a randomized controlled trial. Am J Respir Crit Care Med. 2016;2016:193.
20. Sadeh A. A brief screening questionnaire for infant sleep problems: validation and findings for an Internet sample. Pediatrics. 2004;113(6):E570–E577. doi:10.1542/peds.113.6.e570
21. 0岁~5岁儿童睡眠卫生指南 [Guideline for sleep hygiene among children aged 0~5 years]. Vol WS/T 579-2017. National Health and Family Planning Commission of the People’s Republic of China (中华人民共和国国家卫生和计划生育委员会); 2018. Chinese. Available from: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/10/20171026154305316.pdf.
22. Schreck KA, Richdale AL. Knowledge of childhood sleep: a possible variable in under or misdiagnosis of childhood sleep problems. J Sleep Res. 2011;20(4):589–597. doi:10.1111/j.1365-2869.2011.00922.x
23. Owens JA, Jones C. Parental knowledge of healthy sleep in young children: results of a primary care clinic survey. J Dev Behav Pediatr. 2011;32(6):447–453. doi:10.1097/DBP.0b013e31821bd20b
24. McDonald JH. Kruskal–Wallis test. In: Handbook of Biological Statistics.
25. Chen H, Yu F, Han S. 学龄前儿童家长的睡眠知识现状调查与分析 [Investigation and analysis of status of sleep knowledge of parents of preschool children]. Med J Chin People Health. 2015;27(8):101–103. Chinese.
26. McDowall PS, Elder DE, Campbell AJ. Relationship between parent knowledge of child sleep, and child sleep practices and problems: a pilot study in a children’s hospital cohort. J Paediatr Child Health. 2017;53(8):788–793. doi:10.1111/jpc.13542
27. All-China Women’s Federation. The national guidelines for family education. Beijing, China: All-China Women’s Federation, Ministry of Education, Central Civilization Office, Ministry of Civil Affairs, Ministry of Culture and Tourism, National Health Commission, National Radio and Television Administration, China Association for Science and Technology, China Working Committee for the Care of the Next Generation; 2019.
28. Brayden RM, Poole SR. Common behavioral-problems in infants and children. Prim Care. 1995;22(1):81–97. doi:10.1016/S0095-4543(21)00502-9
29. Cook G, Appleton JV, Wiggs L. Parentally reported barriers to seeking help and advice for child sleep from healthcare professionals. Child Care Health Dev. 2020;46(4):513–521. doi:10.1111/cch.12739
30. Kang Y-Q, Song X-R, Wang G-F, Su -Y-Y, Li P-Y, Zhang X. Sleep problems influence emotional/behavioral symptoms and repetitive behavior in preschool-aged children with autism spectrum disorder in the unique social context of China. Front Psychiatry. 2020;11. doi:10.3389/fpsyt.2020.00273
31. DeLeon CW, Karraker KH. Intrinsic and extrinsic factors associated with night waking in 9-month-old infants. Infant Behav Dev. 2007;30(4):596–605. doi:10.1016/j.infbeh.2007.03.009
32. Cerasuolo M, Malloggi S, Conte F, et al. The effects of the COVID19-related lockdown are modulated by age: an Italian study in toddlers and pre-schoolers. Brain Sci. 2021;11(8):1051. doi:10.3390/brainsci11081051
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.