Back to Journals » Clinical and Experimental Gastroenterology » Volume 18
Characterization of Bacterial Biofilm Composition in Occluded Plastic Biliary Stents
Authors Flumignan VK ![]() , Sircili MP, Germano LG, Souza AVDS, Silva NF
, Sircili MP, Germano LG, Souza AVDS, Silva NF ![]() , Fukumasu NK, Anjos RM
, Fukumasu NK, Anjos RM ![]() , Otoch JP, Artifon ELA
, Otoch JP, Artifon ELA
Received 3 October 2024
Accepted for publication 29 July 2025
Published 7 August 2025 Volume 2025:18 Pages 179—189
DOI https://doi.org/10.2147/CEG.S499088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Andreas M. Kaiser
Victor Kalil Flumignan,1 Marcelo Palma Sircili,2 Lígia Garcia Germano,2 Ana Vitoria dos Santos Souza,2 Nicole Fernandes Silva,2 Newton Kiyoshi Fukumasu,3 Raphaela Marques Anjos,4 Jose Pinhata Otoch,1 Everson Luiz de Almeida Artifon1
1Postgraduate Program in Anesthesiology and Surgical Sciences, Faculty of Medicine, University of São Paulo, São Paulo, Brazil; 2Laboratory of Genetics, Butantan Institute and Interunit Graduate Program in Biotechnology, University of São Paulo, São Paulo, Brazil; 3Institute for Technological Research (IPT), University of São Paulo, São Paulo, Brazil; 4Faculty of Medicine, University of São Paulo, São Paulo, Brazil
Correspondence: Victor Kalil Flumignan, Email [email protected]
Purpose: Plastic biliary stents are an effective treatment for biliary obstruction. Despite being resolutive and accessible, they are known to have a low patency rate, estimated at 3 to 6 months. This can be attributed to the formation of bacterial biofilm, which leads to the luminal obstruction of the stent. The aim of this study is to identify the bacterial composition of biofilms from obstructed plastic biliary stents removed through ERCP.
Methods: Obstructed plastic biliary stents were retrieved from patients undergoing ERCP. The stents were fragmented into three segments of 2.0 cm each: proximal, medial, and distal. Gram staining was performed on each fragment, followed by assessment using optical microscopy. Subsequently, 4 μm cross-sections were made of each fragment, with subsequent analysis by confocal microscopy. The material from the inside of the stents was also placed in culture medium and colony-forming units were counted.
Results: Optical microscopy and analysis by confocal microscopy showed a seemingly higher number of bacterial colonies in the distal portion of the stents compared to the proximal and medial regions. A greater presence of bacteria in the distal segments of the stents was confirmed, with growth reaching up to 1014, while growth in the proximal and medial segments was only observed up to 109 and 108, respectively. Biochemical identification using Gram staining identified both Gram-positive and Gram-negative species: Enterococcus faecium; Aeromonas hydrophila/caviae; Escherichia coli; Enterobacter cloacae; Citrobacter freundii; Klebsiella oxytoca; Proteus vulgaris; Proteus mirabilis; Pantoea sp; Morganella morganii.
Conclusion: The composition of the biofilm in biliary stents confirmed to be polymicrobial. The distal portion of the stents is likely the most frequent site of obstruction. New strategies, such as the development and improvement of plastic stents, should be considered to slow this growth and enhance permeability.
Keywords: biliary system, biofilm, ERCP
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is the gold standard treatment for obstructive jaundice. Both benign and malignant disease can be treated, with the biliary stent placement.1–4
Despite the high initial success rates in achieving endoscopic biliary drainage, the patency duration of this stent is limited by the progressive obstruction of its lumen, generally after 3 to 5 months of use for plastic stents and 9 to 12 months for metal stents.5,6 This is considered the most significant complication of biliary stents, occurring in a substantial number of cases (10% to 30%)7,8 and is associated with the recurrence of jaundice, with or without cholangitis, requiring the removal and replacement of a new stent, which leads to increased morbidity rates as well as additional costs for the healthcare system. Several factors are involved in the occlusion of biliary stents, with the formation of adherent bacterial biofilm in their lumen appearing to play a major role in these cases.9,10 For this reason, it is important to gain a better understanding of the biofilm formation mechanism on plastic biliary stents and develop strategies to mitigate its formation, ultimately improving stent patency.
This study aims to analyze the composition of biofilms present in plastic biliary stents.
Materials and Methods
Obtaining the Occluded Biliary Stents
The biliary stents were removed through Endoscopic Retrograde Cholangiopancreatography (ERCP) using a duodenoscope (Olympus, TJF 160) and a polypectomy snare (Captivator, Boston Scientific) – Figure 1. After removal, the stents were placed in sterile vials containing PBS (Phosphate-Buffered Saline) buffer solution and sent to the Genetics Laboratory at the Butantan Institute for analysis.
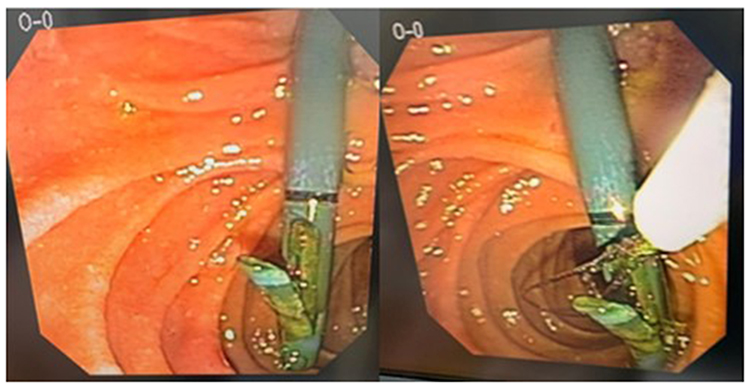 |
Figure 1 Left: Endoscopic view of an occluded biliary stent. Right: Endoscopic removal of a prosthesis occluded by ERCP, with the aid of a polypectomy snare. |
Processing of the Occluded Biliary Stents
The biliary stents were divided into three portions, approximately 2.0 cm long, according to their biliary and duodenal positioning, identified as proximal, medial, and distal. The proximal part was inserted into the bile duct, while the distal part was located near the major duodenal papilla/duodenal lumen (Figure 2). The material from each portion was collected using 500 µL of PBS.
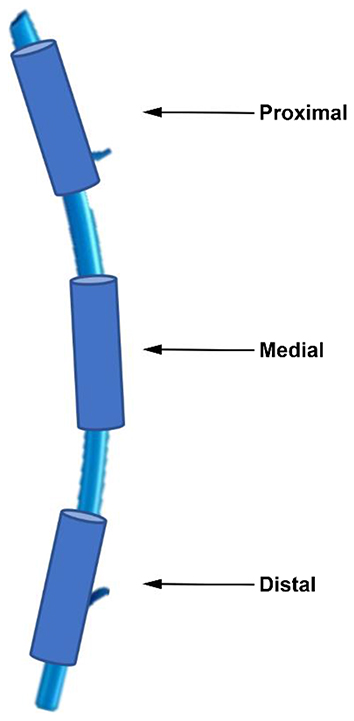 |
Figure 2 Schematic representation of the occluded, fragmented segments of the stents for analysis. |
Analysis and Identification of Occluded Biliary Stents
Each portion of the stent material, resuspended in PBS, was transferred to LB culture medium (Luria-Bertani) to promote bacterial growth. The samples were incubated at 37°C with constant agitation at 180 rpm. After incubation, the colonies were isolated and counted using colony-forming units (CFU). This method allowed the identification of viable bacteria in each sample portion, providing a quantitative assessment of the bacterial load and potential infectivity.
The isolated bacterial colonies were biochemically identified using the API20E kit (Biomérieux), where each division of the kit was inoculated with the bacterial suspension and incubated according to the instructions. After the 18-hour incubation period at 37°C, the results were read based on the bacterial reactions to form a biochemical profile, which was compared to the database for precise identification. This kit serves to differentiate and identify Gram-negative bacilli based on the bacteria’s metabolic profile, analyzing their ability to perform various biochemical reactions, such as sugar fermentation, production of specific enzymes, and substrate utilization.
For each portion of the stents, Gram staining was performed directly from the PBS resuspension using 10 µL of the sample. This technique provides an initial characterization of the bacteria regarding their morphology and classification as Gram-positive or Gram-negative.
For structural analysis, 4 µm transverse sections of the samples were prepared and subjected to laser scanning confocal microscopy (CLSM). The samples were stained with propidium iodide at a final concentration of 1:1000, a fluorescent dye and DNA marker that allows the identification of bacterial structuring and biofilm formation. The slides were incubated in the dark to protect the dye from light degradation and washed with PBS to remove excess dye.
Statistical Analysis
The number of bacteria adhered to the stents was transformed into base 10 logarithms for data normalization, and the results were expressed as log10 CFU/cm²/day ± standard deviation (CFU: colony-forming units). This approach allowed for better comparison between the different experimental conditions, minimizing extreme variations and facilitating subsequent statistical analysis. The data were analyzed using appropriate statistical methods to determine the significance of the observed differences between samples.
Results
Bacterial Quantification by CFU
The results showed different distributions of bacterial growth, with a significantly higher concentration in the distal portion. Specifically, CFU counts reached values of up to 10−14 in the distal segment, while the proximal and medial segments had lower counts, reaching 10−9 and 10−10 CFU, respectively. Results can be observed in Figures 3–5.
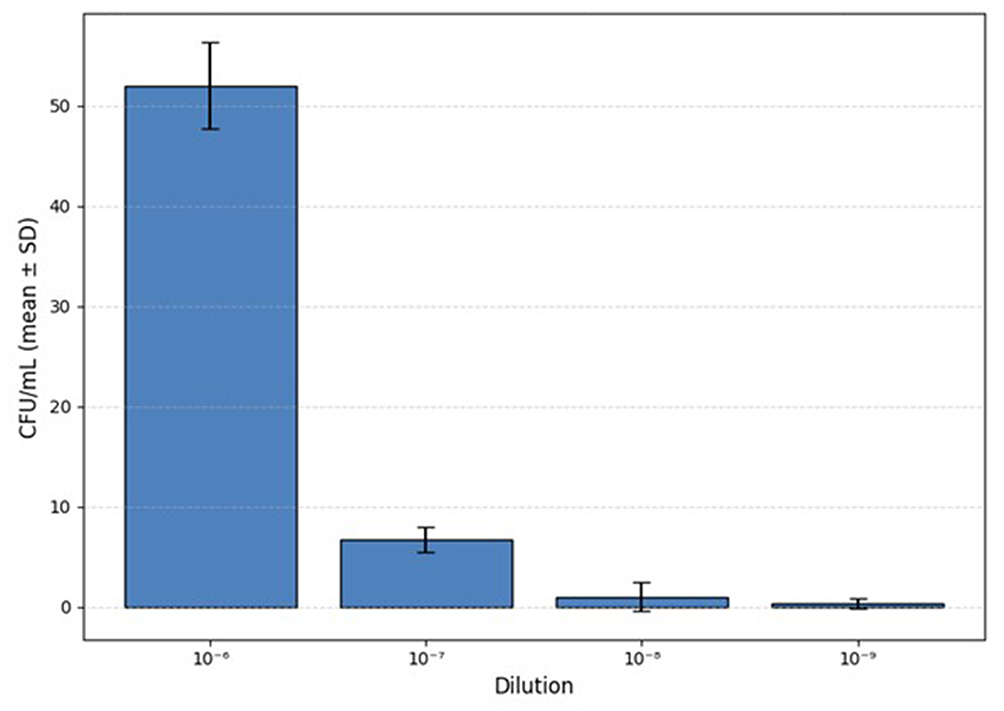 |
Figure 3 CFU/mL count of the stent in the proximal third. |
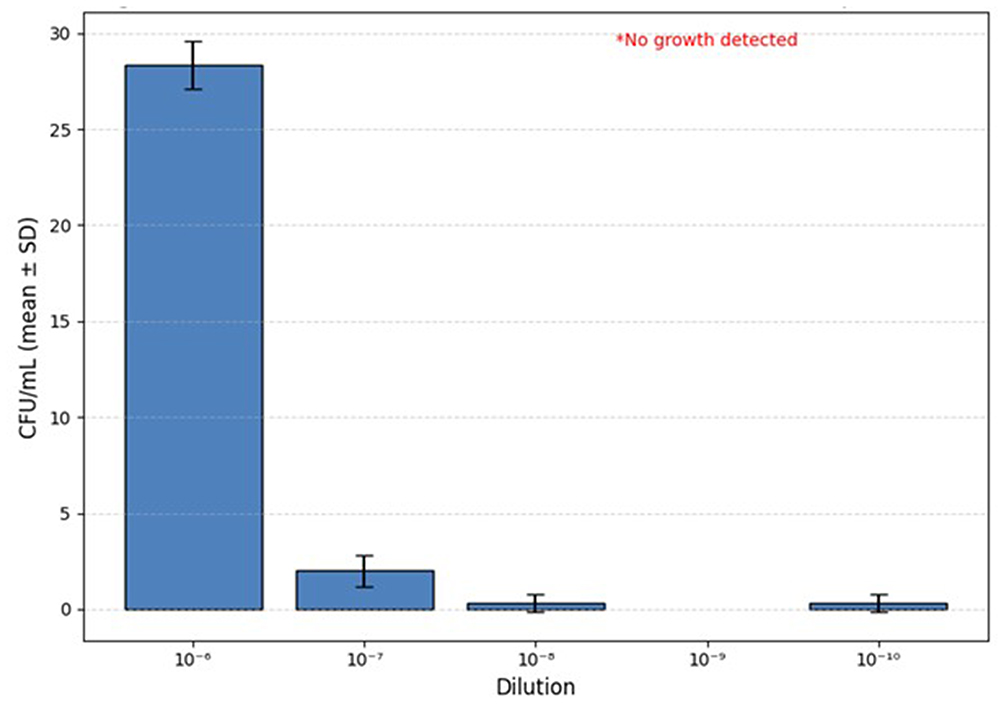 |
Figure 4 CFU/mL count of the stent in the medial third. |
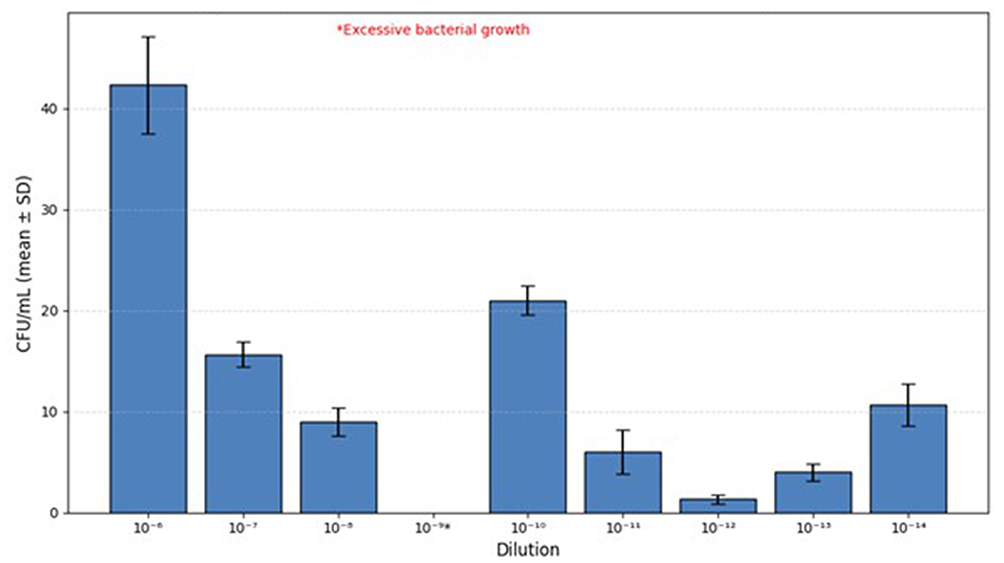 |
Figure 5 CFU/mL count of the stent in the distal third. |
Each bar represents the mean value obtained from three independent replicates (n = 3), and error bars indicate the standard deviation (SD). A one-way ANOVA followed by Tukey’s post hoc test was performed to assess statistical differences among the dilution (p<0.05).
Colony-forming unit (CFU) counts in the proximal portion of the stents revealed a mean of 52.00 CFU/mL (± 5.29) at the 10−6 dilution, with individual values of 58, 48, and 50 CFU/mL. In subsequent dilutions, a progressive reduction was observed, with means of 6.67 CFU/mL (± 1.52) at 10−7 (values of 8, 7, and 5 CFU/mL), 1.00 CFU/mL (± 1.73) at 10−8 (values of 0, 0, and 3 CFU/mL), and 0.33 CFU/mL (± 0.58) at 10−9 (values of 0, 1, and 0 CFU/mL).Statistical analysis yielded an F-value of 219.75 and a p-value of 5.06 × 10−8, indicating a statistically significant difference among the tested dilutions (p < 0.05). Colony-forming unit (CFU) counts in the medial portion of the stents revealed a mean of 28.33 CFU/mL (± 1.53) at the 10−6 dilution, with individual values of 27, 28, and 30 CFU/mL. In subsequent dilutions, a marked decrease was observed, with means of 2.00 CFU/mL (± 1.00) at 10−7 (values of 1, 2, and 3 CFU/mL), 0.33 CFU/mL (± 0.58) at 10−8 (values of 1, 0, and 0 CFU/mL), and 0.33 CFU/mL (± 0.58) at 10−10 (values of 0, 0, and 1 CFU/mL). The 10−9 dilution was not analyzed due to the absence of bacterial growth.One-way ANOVA yielded an F-value of 566.75 and a p-value of 1.18 × 10−9, indicating statistically significant differences among the tested dilutions (p < 0.05). Colony-forming unit (CFU) counts in the distal portion of the stents revealed a mean of 42.33 CFU/mL (± 5.78) at the 10−6 dilution, with individual values of 49, 38, and 40 CFU/mL. At the 10−7 dilution, the mean was 15.67 CFU/mL (± 1.53) (values of 14, 17, and 16 CFU/mL), and at 10−8, the mean was 9.00 CFU/mL (± 1.41) (values of 8, 8, and 11 CFU/mL).
The 10−9 dilution showed excessive bacterial growth, preventing reliable quantification and was therefore excluded from the statistical analysis.The remaining dilutions showed the following means: 21.00 CFU/mL (± 1.41) at 10−10 (values of 23, 20, and 20 CFU/mL), 6.00 CFU/mL (± 2.65) at 10−11 (values of 4, 5, and 9 CFU/mL), 1.33 CFU/mL (± 0.58) at 10−¹² (values of 2, 1, and 1 CFU/mL), 4.00 CFU/mL (± 1.00) at 10−13 (values of 5, 4, and 3 CFU/mL), and 10.67 CFU/mL (± 2.52) at 10−14 (values of 13, 11, and 8 CFU/mL).Statistical analysis yielded an F-value of 72.63 and a p-value of 6.22 × 10−11, indicating statistically significant differences among the tested dilutions (p < 0.05).
Thus, it can be observed that the distal portion of the catheter represented a favorable environment for bacterial growth. This can be explained by factors such as fluid flow, proximity to the infection source, or catheter geometry, which influence biofilm formation and stability. Additionally, the high density of microorganisms in the distal portion of the catheters suggests a high risk of clinical infections associated with medical devices, emphasizing the need for specific intervention strategies in this region. In all catheters, a greater presence of bacterial colonies was observed in the distal portion than in the medial and proximal portions.
Regarding Figure 6, each bar represents the mean value obtained from three independent replicates (n = 3), and error bars indicate the standard deviation (SD). A two-way ANOVA followed by Tukey’s post hoc test was performed to evaluate statistical differences among regions (proximal, medial, distal) and dilutions, as well as the interaction between these factors (p < 0.05). Statistically significant differences were observed for the factors Dilution (p < 0.0001), Region (p < 0.0001), and the Dilution × Region interaction (p < 0.0001).
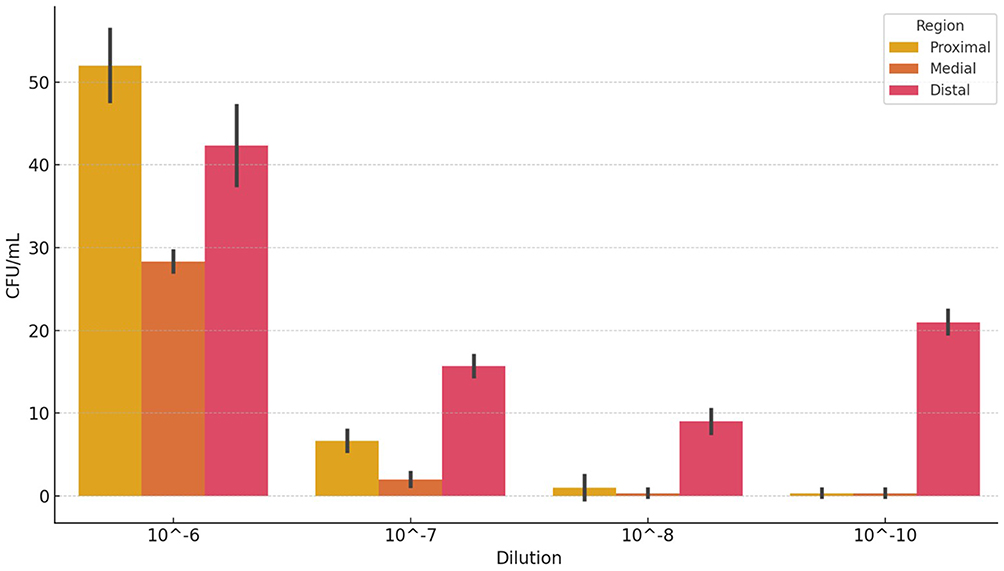 |
Figure 6 Quantification of CFU/mL in the proximal, medial, and distal portions of the stents at different dilutions. |
Colony-forming unit (CFU/mL) quantification revealed significant differences between the proximal, medial, and distal portions of the stents across the tested dilutions. The mean values obtained for each group showed a progressive decrease in bacterial concentration with increasing dilution across all regions.
At the 10−6 dilution, the proximal region exhibited the highest CFU/mL counts (58, 48, and 50 CFU/mL), followed by the distal region (49, 38, and 40 CFU/mL), and then the medial region (27, 28, and 30 CFU/mL). This trend was maintained across subsequent dilutions, with consistently higher values in the proximal portion and lower values in the medial portion.The two-way ANOVA revealed that both the Dilution factor (F = 408.56, p < 0.0001) and the Region factor (F = 91.01, p < 0.0001) had statistically significant effects on CFU/mL values. Additionally, a significant interaction between these factors was detected (F = 22.76, p < 0.0001), indicating that the effect of dilution on bacterial growth varied according to the stent region analyzed.
Biochemical Identification and Microbial Diversity
The identification of bacterial species in the biofilms was performed using the API20E kit, a standard method in microbiology for the biochemical identification of Gram-negative bacteria. The analyses revealed significant bacterial diversity in the analyzed catheters, indicating that the biofilms were not composed of a single species but a complex microbial community.
Among the identified species were Enterococcus faecium, Aeromonas hydrophila/caviae, Escherichia coli, Enterobacter cloacae, Citrobacter freundii, Klebsiella oxytoca, Proteus mirabilis, Morganella morganii, and Proteus vulgaris (Table 1).
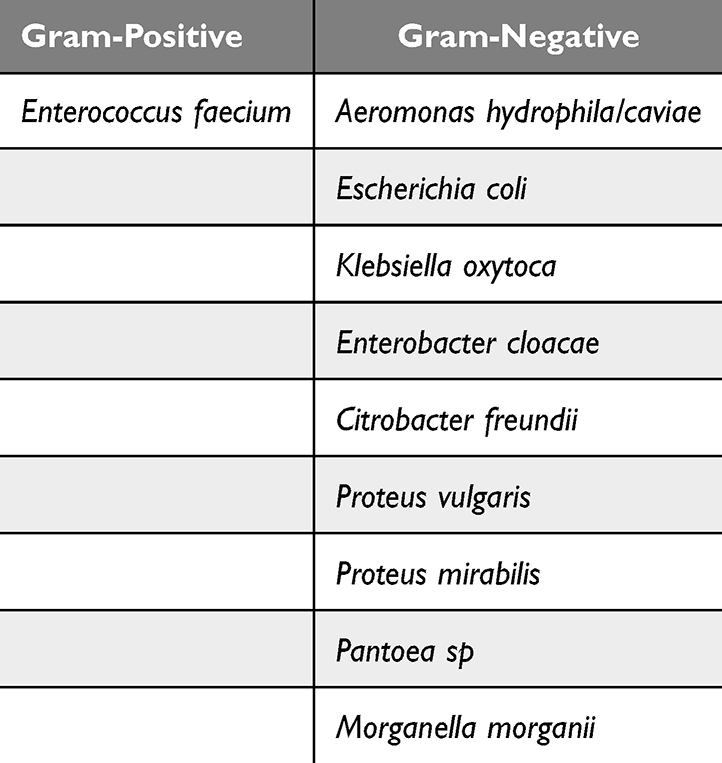 |
Table 1 Bacterial Identification of Occluded Stents |
The presence of these species, many of which are known for their ability to form biofilms and their resistance to multiple antibiotics, suggests that the biofilms on the catheters represent a significant clinical challenge. The microbial diversity also implies that antimicrobial treatments need to be multifaceted, addressing the specific characteristics of each species to be effective.
Moreover, the identification of these species in different parts of the catheters indicates that biofilm composition may vary along the device, possibly influenced by local factors such as nutrient availability, pH, and the presence of host immune components. This variability highlights the need for prevention and treatment strategies that consider the dynamic and heterogeneous nature of biofilms on medical devices.
Microscopic Observations and Bacterial Distribution
Microscopy revealed that the biofilms formed on the catheters displayed mixed and polymicrobial morphologies after Gram staining. Both Gram-positive and Gram-negative bacteria were identified, along with various cell forms, including cocci, bacilli, and streptobacilli (Figure 7).
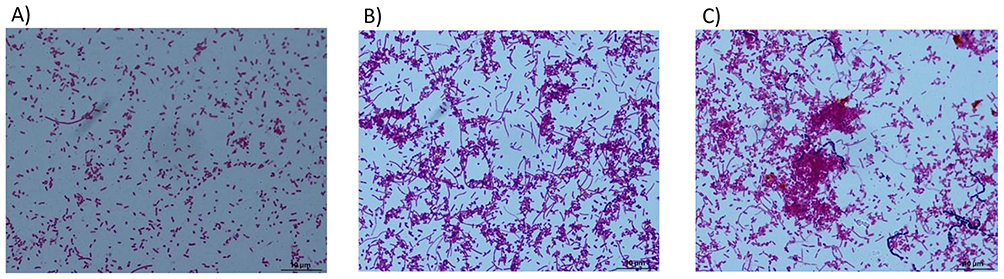 |
Figure 7 Gram staining images of samples containing biofilm from different regions of the biliary catheter: (A) proximal region, (B) medial region, and (C) distal region. Optical microscopy, 1000x magnification. |
These characteristics suggest the complexity of the bacterial community, where different bacterial species interact, making the biofilm more stable and persistent. The morphological heterogeneity may indicate bacterial adaptation to the catheter environment and reflect a functional distribution within the biofilm, with different bacterial groups playing complementary roles in defense against the host immune system and resistance to antimicrobial treatments.
Structural Analysis of Biofilms by Confocal Microscopy
For a deeper understanding of biofilm structural organization, transverse sections of the catheters were prepared and analyzed by laser scanning confocal microscopy (CLSM). This technique allowed high-resolution visualization of the bacterial layers composing the biofilms, revealing a heterogeneous formation along the different sections of the catheters (Figures 8–10).
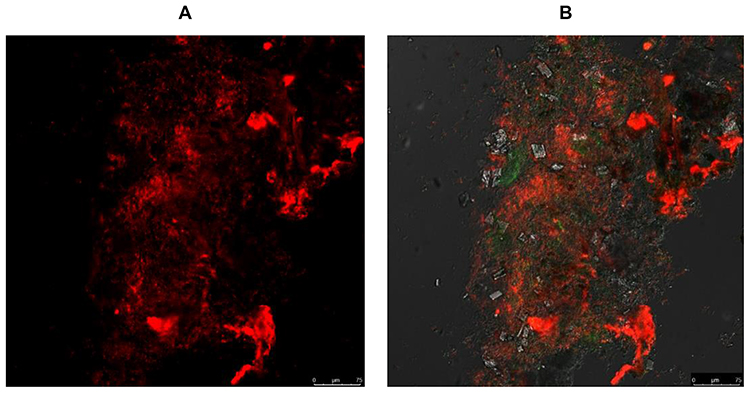 |
Figure 8 Images of cross-sections from the medial region of a biliary catheter containing bacterial biofilm stained with propidium iodide. Confocal laser microscopy. Magnification 620x (A and B). |
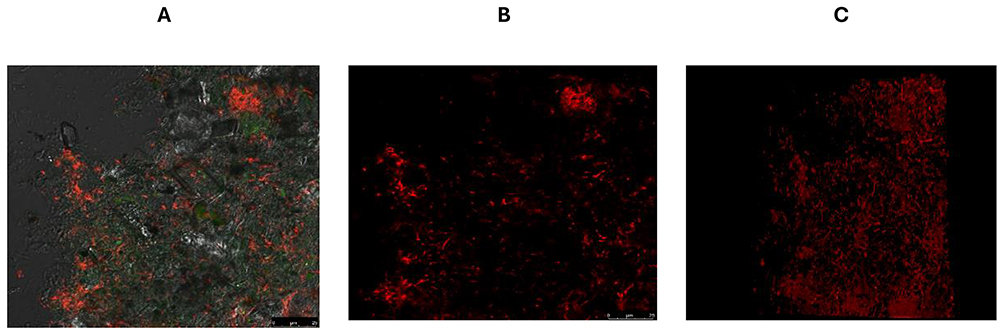 |
Figure 9 Images of cross-sections from the distal region of a biliary catheter containing bacterial biofilm stained with propidium iodide. Confocal laser microscopy. Magnification 620x (A–C). |
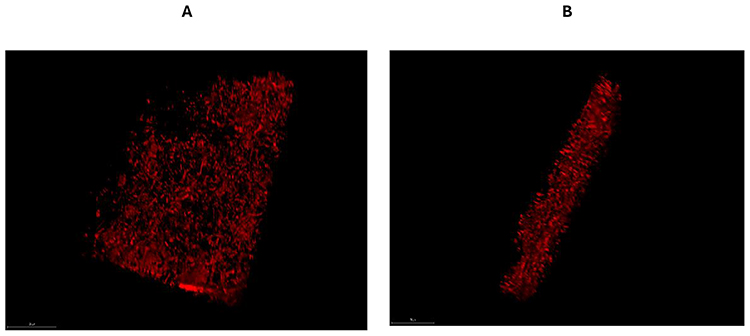 |
Figure 10 Three-dimensional images of cross-sections from the distal region of a biliary catheter containing bacterial biofilm stained with propidium iodide. Confocal laser microscopy. Magnification 620x (A and B). |
CLSM analysis showed that biofilms in the distal portion of the catheters were thicker and denser compared to the proximal and medial portions. This structural heterogeneity may indicate different stages of biofilm maturation, with the distal portion presenting a more advanced developmental stage, possibly due to greater exposure to nutrients or reduced shear flow. The presence of more compact bacterial layers in the distal portion may also hinder the penetration of antimicrobial agents, explaining the greater persistence and resistance of biofilms in this area.
Ethical Approval
The Research Ethics Committee of the Faculty of Medicine of the University of São Paulo approved the study protocol No. 427/11, entitled “Comparison between biliary plastic stents with and without application of silver nanoparticles: an in vitro study of intraluminal biofilm formation”, during a session held on October 3, 2012. The study was submitted by the Department of Surgery.
According to Resolution No. 196/96 of the Brazilian National Health Council, the principal investigator is responsible for submitting interim and final reports to the Ethics Committee.
Discussion
Early occlusion of plastic biliary stents is a concern as it can precipitate the evolution to cholangitis, in addition to the need for multiple hospitalizations and interventions, resulting in high costs for the healthcare system and increased morbidity and mortality for patients.10 Biofilm formation is an important step in the occlusion of biliary stents and depends on several factors, such as bacterial colonization.3,11 Initially, interaction occurs between the surface, the bacteria, and the liquids in the medium, leading to the formation of an EPS, creating the biofilm.12 However, it has been demonstrated that human bile is sterile and, therefore, there is no biofilm formation in the gallbladder or the walls of the biliary ducts.13 One possible explanation is that due to biliary stasis resulting from strictures and stones that do not allow adequate bile drainage, opportunistic microorganisms adhere to the lumen of the stents, leading to biofilm formation. The biofilm is a micro-ecosystem composed of bacterial cells encased in an EPS. Another factor explaining this phenomenon is that the Sphincter of Oddi is a natural barrier to microbial colonization, and the passage of stents breaks this barrier, allowing colonization by microorganisms present in the intestine.14 This explains the fact that a large part of the bacteria isolated from bile samples (in situations of stasis or infection) are intestinal.13 Despite this, microorganisms isolated from biliary stents still include anaerobic, aerobic species, and fungi.2 Even though the patency of plastic biliary stents is low and their associated complications are well known, they continue to be widely used—and rightly so, given their cost-effectiveness. The main issue is that they work well, but only for a short period. Therefore, more research is needed to better understand the mechanisms of occlusion, which begin with biofilm formation, in order to develop strategies to prevent these events. Due to the scarcity of studies demonstrating the factors causing obstruction of biliary stents, as well as the composition of the biofilms that lead to stent obstruction, this study was initiated to better understand the obstruction process of plastic biliary stents. Initially, the study focused on these stents, which were evaluated immediately after removal. To understand the biofilm composition, various electron microscopy techniques with different magnifications were performed on the three segments of the stents (proximal, medial, and distal). Until now, there was no clear information or specific study in the literature comparing segments of occluded biliary stents.In all stents, a higher concentration of bacteria was observed in the distal portion compared to the proximal and medial portions. It is worth noting that the distal portion of the biliary stent is the only part that is exposed in the duodenal lumen, while the rest of the catheter remains inside the biliary tract. As previously reported, bile is sterile, and there is no biofilm formation within the biliary ducts or gallbladder. These facts lead us to believe that the intimate contact of the distal portion of the biliary stent with the duodenal lumen plays a fundamental role in the biofilm formation process, which ultimately leads to its obstruction. Due to the intense flow of food, saliva, and secretions that constantly pass through the duodenum, along with the presence of bacteria that constitute the duodenal microbiota, biofilm formation likely occurs in the distal portion of the catheter (which is in the duodenal lumen), which explains the higher concentration of bacteria and biofilm in this portion compared to the others located within the biliary tract.To better understand the composition of the biofilms, the identification of the bacteria that are part of their composition was carried out, a crucial step for the next phase of the study: the attempt to develop a coating on the surface of the stents capable of reducing or even inhibiting bacterial growth and biofilm formation. To test the material being developed, it is fundamental to understand which microorganisms are present in these biofilms, thus testing the coating in contact with the same microorganisms present in the occluded stents. After completing the bacterial identification of the occluded biliary catheters, data compatible with the literature were observed. Despite the scarcity of studies related to the composition of biofilms in plastic biliary stents, the existing literature shows that biofilms are mostly polymicrobial, containing anaerobes 6% to 40% of the time, predominantly Enterococcus sp and Bacteroides sp.1,2 Among aerobic bacteria, the gram-positive Enterococcus sp and the gram-negative Escherichia coli and Klebsiella were the most commonly found. The data are consistent with what was observed in this study, showing an interesting diversity of gram-negative and gram-positive microorganisms.Another important factor that may lead to catheter obstruction is the production of biliary sludge - its formation begins after bacterial colonization of the stent.9,15 Other factors described in the literature, such as the friction coefficient, can contribute to biofilm formation. Polyethylene and polyurethane stents are the most common and have a high friction coefficient, which can be detrimental in this regard. Other theories initially involved the detrimental presence of side holes in plastic biliary stents, as they favored future colonization leading to obstruction. However, future studies did not confirm this hypothesis.16,17 Biofilm infections on implant surfaces can lead to implant failure, chronic infections, and high mortality rates.18 That´s why new strategies should be considered to mitigate biofilm formation, such as coating techniques using electrospinning, adsorption, chemical conjugation, and binding, which have shown good results in previous studies.19
Conclusion
The composition of biofilms in occluded plastic biliary stents is predominantly polymicrobial, primarily concentrating in the distal portion of the stents.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Grant No.: 88887.688425/2022-00.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schneider J, Hapfelmeier A, Fremd J, et al. Biliary endoprosthesis: a prospective analysis of bacterial colonization and risk factors for sludge formation. PLoS One. 2014;9(10):e110112.PMID: 25314593; PMCID: PMC4197023. doi:10.1371/journal.pone.0110112
2. Kwon CI, Lehman GA. Mechanisms of biliary plastic stent occlusion and efforts at prevention. Clin Endosc. 2016;49(2):139–146.Epub 2016 Mar 22. PMID: 27000422; PMCID: PMC4821514. doi:10.5946/ce.2016.024
3. Vaishnavi C, Samanta J, Kochhar R. Characterization of biofilms in biliary stents and potential factors involved in occlusion. World J Gastroenterol. 2018;24(1):112–123.PMID: 29358888; PMCID: PMC5757116. doi:10.3748/wjg.v24.i1.112
4. Wen W, Ma LM, He W, et al. Silver-nanoparticle-coated biliary stent inhibits bacterial adhesion in bacterial cholangitis in swine. Hepatobiliary Pancreat Dis Int. 2016;15(1):87–92.PMID: 26818548. doi:10.1016/s1499-3872(15)60410-6
5. Pfau PR, Pleskow DK, Banerjee S; ASGE Technology Assessment Committee, et al. Pancreatic and biliary stents. Gastrointest Endosc. 2013;77(3):319–327. Erratum in: Gastrointest Endosc. 2013;78(1):193-5. PMID: 23410693. doi:10.1016/j.gie.2012.09.026
6. Kaassis M, Boyer J, Dumas R, et al. Plastic or metal stents for malignant stricture of the common bile duct? Results of a randomized prospective study. Gastrointest Endosc. 2003;57(2):178–182.PMID: 12556780. doi:10.1067/mge.2003.66
7. Huibregtse K, Tytgat GN. Palliative treatment of obstructive jaundice by transpapillary introduction of large bore bile duct endoprosthesis. Gut. 1982;23(5):371–375. doi:10.1136/gut.23.5.371
8. Sung JY, Lai CW, Chung SCS. Omitting side holes in biliary stents does not improve patency of stents in malignant biliary obstructive disease: univariate and multivariate analysis. Am J Gastroenterol. 1991;86(7):843–849.
9. Dowidar N, Kolmos HJ, Matzen P. Experimental clogging of biliary endoprostheses. Role of bacteria, endoprosthesis material, and design. Scand J Gastroenterol. 1992;27(1):77–80. doi:10.3109/00365529209011171
10. Weickert U, Venzke T, König J, Janssen J, Remberger K, Greiner L. Why do bilioduodenal plastic stents become occluded? A clinical and pathological investigation on 100 consecutive patients. Endoscopy. 2001;33(9):786–790. doi:10.1055/s-2001-16519
11. Faigel DO. Preventing biliary stent occlusion. Gastrointest Endosc. 2000;51(1):104–107. doi:10.1016/S0016-5107(00)70403-2
12. Cheng Y, Feng G, Moraru CI. Micro- and nanotopography sensitive bacterial attachment mechanisms: a review. Front Microbiol. 2019;10:191. doi:10.3389/fmicb.2019.00191
13. Tajeddin E, Sherafat SJ, Majidi MR, Alebouyeh M, Alizadeh AH, Zali MR. Association of diverse bacterial communities in human bile samples with biliary tract disorders: a survey using culture and polymerase chain reaction-denaturing gradient gel electrophoresis methods. Eur J Clin Microbiol Infect Dis. 2016;35(8):1331–1339. doi:10.1007/s10096-016-2669-x
14. Vaishnavi C, Gupta PK, Sharma M, Kochhar R. Quantification of major constituents of biofilms in occluded pancreatic stents. J Med Microbiol. 2018;67(9):1225–1231. doi:10.1099/jmm.0.000805
15. Leung JW, Ling TK, Kung JL, Vallance-Owen J. The role of bacteria in the blockage of biliary stents. Gastrointest Endosc. 1988;34(1):19–22. doi:10.1016/S0016-5107(88)71223-7
16. Seitz U, Vadeyar H, Soehendra N. Prolonged patency with a new-design Teflon biliary prosthesis. Endoscopy. 1994;26(5):478–482. doi:10.1055/s-2007-1009008
17. van Berkel AM, Boland C, Redekop WK, et al. A prospective randomized trial of Teflon versus polyethylene stents for distal malignant biliary obstruction. Endoscopy. 1998;30(8):681–686. doi:10.1055/s-2007-1001388
18. Kadirvelu L, Sivaramalingam SS, Jothivel D, Chithiraiselvan DD, Govindarajan DK, Kandaswamy K. A review on antimicrobial strategies in mitigating biofilm-associated infections on medical implants. Curr Res Microb Sci. 2024;6:100231. doi:10.1016/j.crmicr.2024.100231
19. Govindarajan DK, Kandaswamy K. Kumaravel Kandaswamy,Antimicrobial peptides: a small molecule for sustainable healthcare applications. Med Microecolog. 2023;18:100090. doi:10.1016/j.medmic.2023.100090
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.