Back to Journals » Medical Devices: Evidence and Research » Volume 18
Characterization and Optimization of the Subsalve Helmet Ventilation Circuit in a High-Fidelity Acute Respiratory Distress Syndrome (ARDS) Lung Model
Authors Donahue J ![]() , Chichester III CO, Hornstein A, Lombardi M, Chichester AM
, Chichester III CO, Hornstein A, Lombardi M, Chichester AM ![]()
Received 3 September 2024
Accepted for publication 23 January 2025
Published 16 April 2025 Volume 2025:18 Pages 261—270
DOI https://doi.org/10.2147/MDER.S487868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
John Donahue,1 Clinton O Chichester III,1 Alex Hornstein,2 Michael Lombardi,3 Amanda M Chichester4
1Department of Biomedical and Pharmaceutical Sciences, University of Rhode Island, Kingston, RI, USA; 2Inventilator LLC, Pawtucket, RI, USA; 3Lombardi Undersea LLC, Middletown, RI, USA; 4Department of Pharmacy Practice and Clinical Research, University of Rhode Island, Kingston, RI, USA
Correspondence: Amanda M Chichester, Department of Pharmacy Practice and Clinical Research, University of Rhode Island, Avedisian Hall, 7 Greenhouse Road, Kingston, RI, USA, Tel +1-401-874-5037, Email [email protected]
Purpose: The Subsalve helmet continuous positive airway pressure (CPAP) circuit is a low-cost, easy to implement non-invasive ventilation option for treatment of acute respiratory failure. The circuit is simple to set up and operate, and is designed to be used with any commonly available continuous positive airway pressure device.
Model (Materials) and Methods: Simulation of an acute respiratory distress syndrome (ARDS) patient allows optimization of treatment parameters without risk. The boundaries of safe and effective helmet CPAP treatment were measured in the TestChest® lung simulator with AQAI SIS software. The capabilities of the TestChest allow for representation of complex breathing patterns, simulation of muscular fatigue, and the ability to model patients with worsening ARDS. Treatment settings were tested by varying CPAP pressure and oxygen flow rate in a simulated ARDS patient.
Results: Moderate CPAP pressure led to significant increases in SpO2 (oxygen saturation) (10% increase at 14 cmH2O pressure) and maintained improvements compared to the control even at the latest stage of the disease. When oxygen was introduced, patient SpO2 increased proportional to the oxygen flow rate. 5 liters per minute (LPM) oxygen increased patient SpO2 by 3% in the severe ARDS model and 30 LPM oxygen increased SpO2 by 7%. Moderate pressure led to significant increases in SpO2 comparable to high concentrations of oxygen. CO2 does not accumulate in the helmet as long as the minimal flow rate (60 LPM of air) is maintained during treatment.
Conclusion: Our data demonstrate that the Subsalve helmet CPAP circuit, with limited oxygen availability, is an effective treatment strategy for ARDS patients in low-resource settings. Moderate positive end expiratory pressure (PEEP) is recommended to improve blood oxygenation. Subsalve has the potential to conserve critical resources in future epidemics.
Keywords: acute respiratory distress syndrome, noninvasive ventilation, continuous positive airway pressure, helmet-CPAP, positive end expiratory pressure
Introduction
Noninvasive ventilation (NIV) broadly refers to respiratory support techniques that do not require endotracheal intubation. NIV is commonly employed to treat respiratory failure such as acute respiratory distress syndrome (ARDS), often in the form of a face mask or high flow nasal cannula (HFNC). Effective NIV treatment is ideal to obviate the need for invasive mechanical ventilation, which requires sedation, ICU capacity, and trained personnel, and carries a risk of trauma from intubation.1 Helmet ventilation is a form of NIV that utilizes a helmet interface connected to a continuous positive airway pressure (CPAP) device to provide positive pressure and oxygen support. Helmet ventilation saw a rise in use during the COVID-19 pandemic, as it is effective in treating moderate cases of COVID-19, and reduced exposure of healthcare workers to aerosolized viral particles.2
The use of helmet ventilation is well established and the efficacy of helmet ventilation was tested against face masks for ARDS patients in a clinical trial at the University of Chicago from 2012 to 2015 while utilizing a wall-gas titration technique.3 Helmet ventilation reduced the number of days on a ventilator compared to the face mask group, as well as the mortality rate after a 90-day period. In a meta-analysis of clinical trials, helmet ventilation had a lower mortality rate and a lower intubation rate than both face mask and high flow nasal oxygen treatments.4 A recent systematic review supports that helmet ventilation is comparable if not superior to high flow nasal cannula.5 A rise in use of helmet ventilation was observed and reported during the COVID-19 pandemic.6 The helmet was well tolerated, as there are no pressure points on the face causing ulceration, patients reported less claustrophobia than with a full face mask, and helmet ventilation limits droplet contamination when compared to other forms of NIV.1
The Subsalve (North Kingstown, RI, USA) Oxygen Treatment Hood was specifically designed to be paired with low-cost commonly available CPAP machines and was granted an Emergency Use Authorization (EUA) by the United States Food and Drug Administration (FDA).7 As a circuit, the helmet and CPAP were designed to be a low-cost, easy-to-use NIV option in response to the COVID-19 pandemic. Conventional, hospital-based NIV therapies have significant limitations including high cost of the device and a limited number of practitioners with knowledge of proper use. To ensure the consistency of the Subsalve Oxygen Treatment Hood with multiple CPAP devices, we tested its efficacy paired with three low-cost commercially available CPAP devices.
A community initiative entitled CircumVent Project developed a breathing circuit and technique to use CPAP machines with the helmet interface.8 In this configuration, only low voltage electricity is required to run the system so this NIV strategy can be employed when power is limited. Helmet ventilation combined with CPAP is low-cost and may decrease ICU stay when compared to a face mask.9
The Subsalve Oxygen Treatment Hood itself is a clear plastic hood that fits over the patient’s head and seals at the neck to provide a tight, adjustable fit. Two ports are positioned to serve as an inlet and outlet for a flow of breathing gas. The expiratory limb typically includes a HEPA or viral filter to create resistance in the circuit, build pressure, and filter aerosolized particles,6 and may also incorporate a PEEP valve for additional pressure regulation. The Subsalve Oxygen Treatment Hood was designed to be paired with any available CPAP machine and requires no specialized training for use making it particularly suitable as a low-cost treatment in resource limited settings.
This study determined the boundaries of safe and effective usage of the Subsalve Oxygen Treatment Hood paired with simple CPAP machines utilizing a TestChest® lung simulator manufactured by Organis GmbH (Graubünden, Switzerland). The TestChest is designed to simulate the respiratory system with patient simulator integration and simulated CO2 production.10 The TestChest allows for real-time simulation of a human lung. Using integrated pressure and oxygen sensors in combination with the AQAI Simulation Interface Software (SIS) (AQAI GmbH, Mainz, Germany), the TestChest calculates oxygen uptake and models a patient’s physiology in healthy or diseased states.11 This physiologically accurate simulator also accounts for muscular activity during spontaneous breathing, allowing simulation of muscular fatigue.11 The accuracy and dynamic response of the TestChest simulator allowed us to precisely model an ARDS patient and accurately determines the effect of pressure support and supplemental oxygen introduced to the Subsalve Oxygen Treatment Hood paired with CPAP circuit.
Model (Materials) and Methods
Testing of the Subsalve Oxygen Treatment Hood paired with a CPAP machine was performed on the TestChest lung simulator paired with AQAI SIS software. The TestChest was connected with a 30 cm long tube to a Styrofoam head with a drilled airway. The Subsalve Oxygen Treatment Hood was fitted over the head with a tight seal to prevent air leaks. The CPAP machine was connected to the inspiratory limb of the helmet by 22 mm tubing, while the expiratory limb was fitted to a viral filter, followed by a PEEP valve in some trial sequences to determine its effect. A supplemental oxygen flow was connected to the inspiratory limb immediately after the machine outlet (Figure 1).
 |
Figure 1 Configuration of the Helmet CPAP circuit. Abbreviation: CPAP, continuous positive airway pressure. |
The ARDS scenario utilized in this study was developed by AQAI GmbH. Details of the scenario progression are included in Table 1. In each experiment, physiological data was recorded every three minutes as the scenario progressed over fifteen minutes with treatment initiated one minute after the initial recording of data. In addition to the parameters recorded by the simulation software, oxygen concentrations were continuously recorded throughout the trial by a PASCO (Auburn, CA) oxygen sensor.
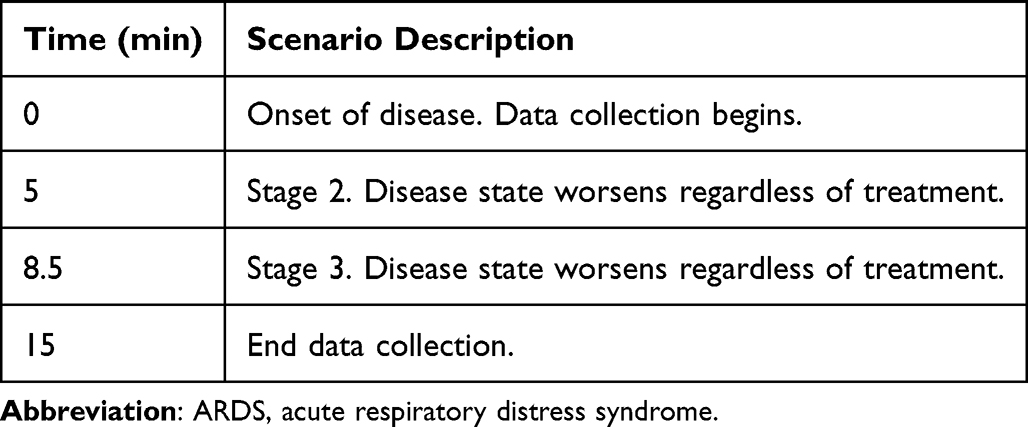 |
Table 1 ARDS Progression |
In this study, three commonly used CPAP machines were paired with the Subsalve Oxygen Treatment Hood and tested for efficacy: the Nanotronics (Brooklyn, NY) nHale, the Resmed S9 (San Diego, CA), and the Resmed Airsense 10. In each trial, the variables altered were CPAP pressure and supplemental oxygen flow rate. Pressures tested range from 4 to 14 cmH2O, while oxygen flow rates are varied from 0 to 30 liters per minute (LPM). Each trial was repeated in triplicate, and values are expressed as mean ± SEM.
To measure carbon dioxide concentrations in the helmet at specific flow rates, an Amico (Richmond Hill, ON, Canada) Medical Air Flowmeter was used to set the flow of compressed air entering the helmet in place of a CPAP. The carbon dioxide concentration in the helmet under each flow rate was continuously recorded using a PASCO wireless CO2 sensor.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism version 10.0.3 for Windows (GraphPad Software, Boston, Massachusetts, USA, www.graphpad.com). One-way ANOVA followed by Bonferroni’s multiple comparisons test was performed to analyze differences between treatment settings at each time point. A p value < 0.05 was considered to be statistically significant.
Results
SpO2 (oxygen saturation) and PaO2 (partial pressure of oxygen) were used as the primary measure of simulated patient outcome. End-tidal carbon dioxide (EtCO2), tidal volume, and respiratory rate were also recorded during the fifteen-minute scenario (Table 2). In the absence of treatment, SpO2 and PaO2 dramatically decrease as the disease worsens, while EtCO2 increases. In the final stage of the disease, there is a decrease in tidal volume with a concurrent increase in respiratory rate.
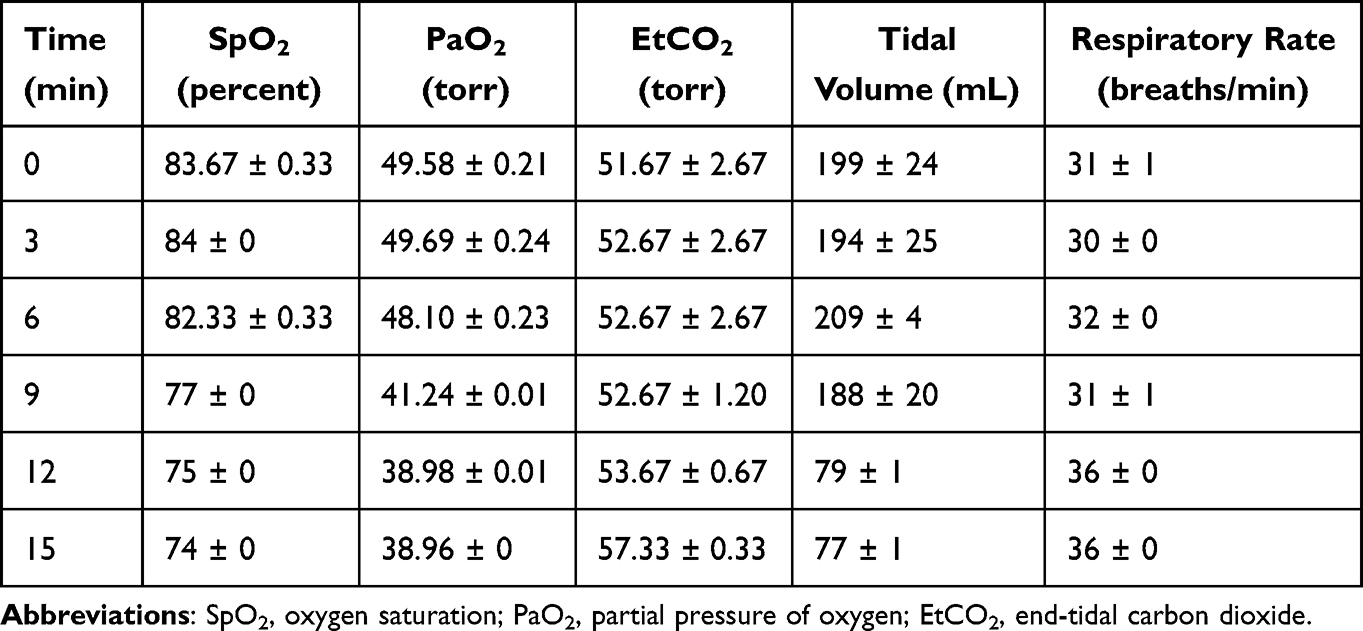 |
Table 2 Pulmonary Parameters During Each Stage of Simulated Patient Scenario |
To assess the efficacy of each treatment setting, we measured the interior helmet fraction of inspired oxygen (FiO2) generated at each oxygen and pressure setting (Figure 2). At a constant oxygen flow rate and CPAP pressure, the oxygen concentration in the helmet remains constant. The FiO2 decreases when CPAP pressure is increased, due to oxygen being diluted by the higher air flow needed to generate increased pressure. FiO2 does not increase linearly with the supplemental oxygen flow rate and higher oxygen flow rates produce a small increase in FiO2 (Figure 2). Therefore, lower flow rates represent a more efficient use of oxygen.
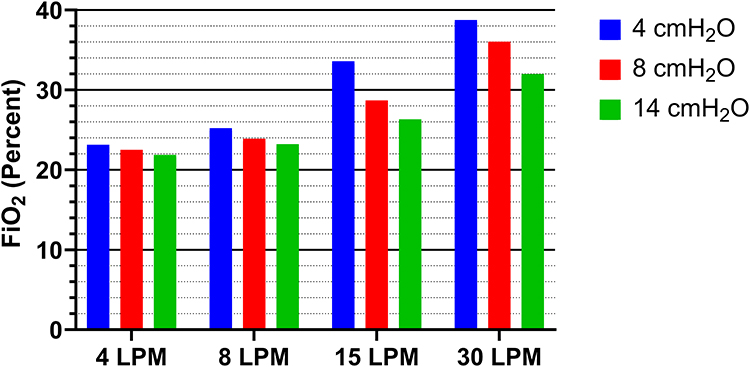 |
Figure 2 FiO2 at increasing oxygen concentrations and increasing pressure settings in the nHale circuit. Values are averaged over a twelve-minute period where FiO2 remains constant. Abbreviations: FiO2, fraction of inspired oxygen; LPM, liters per minute. |
Oxygen supplementation was varied at a set pressure of 4 cmH2O to determine the combination that would produce optimal support to the patient. SpO2 calculated by the AQAI software was recorded for each treatment setting. As shown in Figure 3, blood oxygenation increases proportional to the oxygen flow rate, then gradually decreases as the disease worsens over fifteen minutes. Higher oxygen flow rates produced a small increase in SpO2.
 |
Figure 3 Calculated SpO2 in ARDS scenario with effect of increasing oxygen flow. CPAP was set at 4 cmH2O pressure. Treatment (CPAP with oxygen) began one minute after initiation of scenario. Abbreviations: SpO2, oxygen saturation; LPM, liters per minute; ARDS, acute respiratory distress syndrome; CPAP, continuous positive airway pressure. |
To identify optimal pressure to support the patient, pressure was varied without the administration of oxygen. In the absence of supplemental oxygen, the Subsalve paired with CPAP significantly increased SpO2 at every pressure setting (Figure 4A). A CPAP pressure of 14 cmH2O resulted in 94% SpO2 during the initial stage of disease (t = 3 min) compared to 84% at the same time point without treatment. As expected, improvement diminishes as the disease state worsens but the effect of pressure support is maintained throughout the scenario.
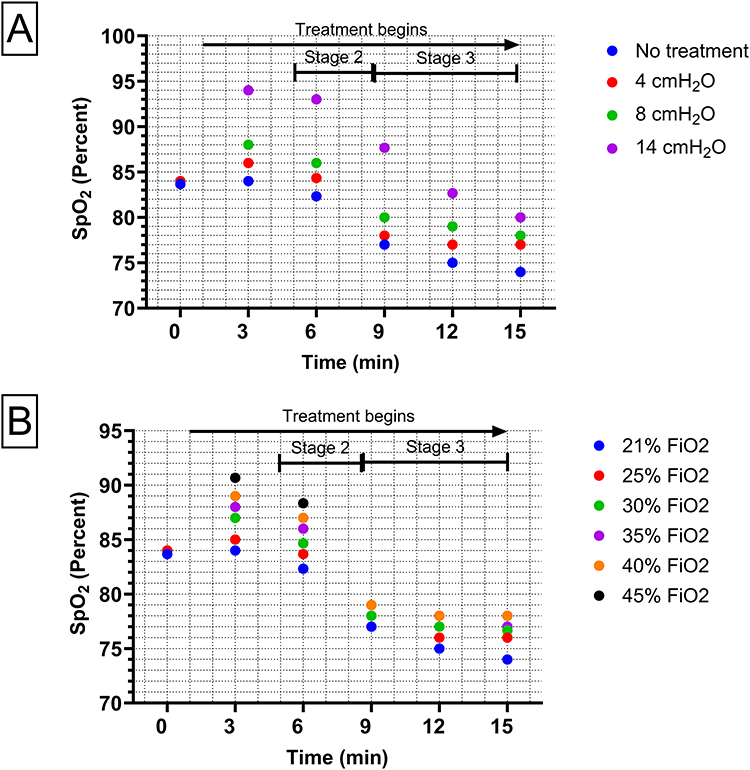 |
Figure 4 Comparison of the separate effects of pressure and oxygen on calculated SpO2 over the course of the ARDS scenario. (A) SpO2 at three pressures without oxygen. (B) SpO2 at six oxygen concentrations modeled by the TestChest simulator without CPAP pressure. Abbreviations: SpO2, oxygen saturation; FiO2, fraction of inspired oxygen; ARDS, acute respiratory distress syndrome; CPAP, continuous positive airway pressure. |
The effect of oxygen without added pressure was tested by increasing the FiO2 within the AQAI software (Figure 4B). Increasing the FiO2 in the absence of pressure led to modest increases in SpO2, but these were not as significant as the improvements observed from high pressures.
A PEEP valve is often included on the expiratory limb of respiratory circuits to add resistance to the circuit, therefore increasing positive end expiratory pressure, or PEEP, delivered to the patient. The addition of a PEEP valve to the helmet CPAP configuration set to 5 cmH2O did not have a measurable effect on PEEP and did not cause a significant increase in PaO2 (Figure 5). Because this circuit produces adequate pressure without a PEEP valve, the use of one is not required.
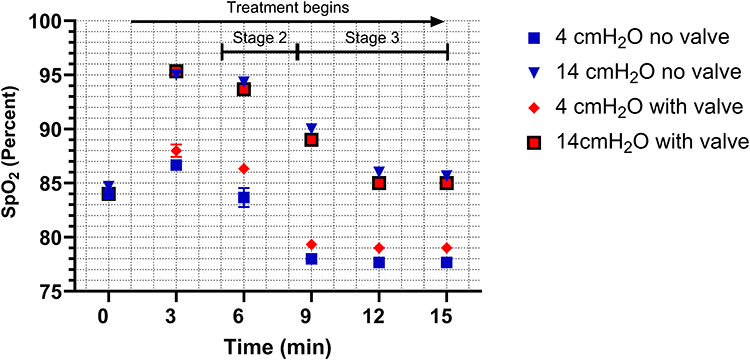 |
Figure 5 Effect of a PEEP valve on calculated PaO2 in ARDS scenario. Recorded in the Resmed S9 circuit with oxygen flow rate set to 4 LPM and CPAP pressure set to 4 cmH2O. PEEP valve was set to 5 cmH2O. Abbreviations: SpO2, oxygen saturation; PEEP, positive end expiratory pressure; PaO2, partial pressure of oxygen; ARDS, acute respiratory distress syndrome; LPM, liters per minute; CPAP, continuous positive airway pressure. |
Carbon dioxide may quickly accumulate if a tube is disconnected leading to a zero-flow situation. Therefore, we sought to determine how quickly CO2 accumulates to an unacceptable concentration under zero flow. In this experiment, a helmet concentration of 45 mmHg or 6% FiCO2 was taken to be an unacceptable level for acute CO2 rebreathing. CO2 accumulation was measured using the TestChest with three different simulated patients, on the basis that CO2 accumulation will be more rapid in patients with increased CO2 production dependent on the severity of the disease state. The three simulations tested were a healthy patient, an ARDS patient in the initial stage of the disease, and a patient in the most severe form of the disease. In the two ARDS patients, the stage of the disease was kept constant and did not worsen over the fifteen-minute period. In the healthy patient, 45 mmHg of carbon dioxide was reached after 8 minutes, while the same concentration was reached after five minutes in the ARDS patients (Figure 6). In each trial, after fifteen minutes, the high flow of air was re-applied to demonstrate how quickly carbon dioxide is washed out of the helmet under high flow.
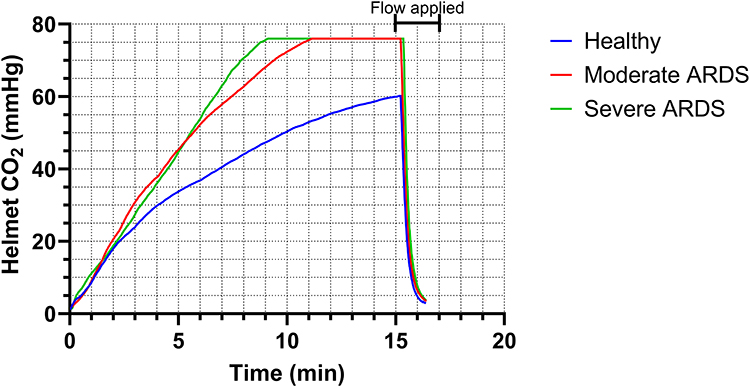 |
Figure 6 CO2 accumulation under periods of zero flow. A high flow after fifteen minutes quickly returns CO2 to negligible concentrations. Abbreviation: ARDS, acute respiratory distress syndrome. |
To confirm that this treatment produces a sufficient flow rate to preclude dangerous CO2 rebreathing, we determined the minimum fresh gas flow rate through the helmet that prevents CO2 from accumulating (Figure 7). By testing a variety of flow rates, we found that fresh gas flow rates lower than 10 LPM did not prevent the accumulation of CO2, while flow rates greater than 10 LPM maintained CO2 concentrations at a constant value. We further tested eight air flow rates ranging from 10 to 60 LPM. The carbon dioxide concentration quickly increased in each trial before reaching a plateau. Increasing the flow rate decreased the CO2 concentration in a linear fashion. These findings support previous data on helmet CO2 concentrations at a constant flow rate.12 The highest flow rate tested, 60 LPM, maintained helmet CO2 concentration below 2 mmHg, which is not a concerning concentration for rebreathing.13 All treatment settings tested for this helmet CPAP circuit produce a flow rate greater than 60 LPM.14
 |
Figure 7 CO2 concentrations at varying flow rates. At each flow rate, helmet CO2 was recorded continuously for 11 minutes. Abbreviation: LPM, liters per minute. |
Discussion
We used the TestChest simulator to determine the optimal parameters for Subsalve Oxygen Treatment Hood CPAP treatment in a simulated ARDS patient. The capabilities of the TestChest with AQAI SIS software allowed us to model worsening stages of the disease and observe changes in physiological parameters in response to treatment.
The Subsalve Oxygen Treatment Hood is low-cost and can be used with any CPAP machine and has limited oxygen consumption under the parameters described in the study. Helmet ventilation is an effective form of NIV at preventing the need for mechanical ventilation while protecting healthcare workers from viral exposure.4,6 This is especially critical in low-resource settings where treatment of severe respiratory disease is complicated by a lack of trained personnel to intubate and the need to conserve a limited oxygen supply.
We found that this treatment is effective using most commonly available CPAP devices, enabling practitioners to use simple and readily available equipment. Helmet CPAP treatment led to improvements in SpO2 comparable to high flow nasal cannula, with significantly lower oxygen use.15 Significant improvements were achieved even without the use of oxygen, indicating that helmet ventilation administered via CPAP can be an effective treatment even when oxygen is unavailable or in limited supply. These data also support prior findings that high PEEP (10 to 15 cmH2O) is critical when using the helmet interface.16 The parameters described can serve as the basis for treatment of respiratory failure.
There has been concern of carbon dioxide rebreathing when using helmet ventilation.17 The helmet interface exposes the patient to higher risk of rebreathing compared to other forms of NIV as the increased volume of the helmet allows CO2 to accumulate. However, our data show that carbon dioxide did not accumulate to unacceptable levels at any treatment setting tested. All settings in this helmet CPAP circuit produce a flow rate greater than 60 LPM, the minimum flow rate to preclude rebreathing, therefore the carbon dioxide concentration in the helmet is negligible during treatment.13 Routine monitoring of helmet CPAP equipment as well as intermittent pCO2 measurements may be taken to minimize this risk. If flow is interrupted due to loss of power to the CPAP, CO2 accumulates to 45 mmHg after five minutes. The helmet should be removed, ports opened, and hose connections detached to reduce the accumulation of carbon dioxide.
High pressure produced the best outcome compared to lower pressure at the same flow rate. We suggest using a CPAP setting of 14 cmH2O, generating a helmet pressure of 12 cmH2O, as this supports patient breathing without excessive pressure. Diminishing returns are observed at high oxygen flow rates. Since CPAP machines self-regulate flow rates to achieve the desired circuit pressure, there is no requirement to additionally regulate PEEP with a secondary PEEP valve. A PEEP valve may introduce error as a partially closed PEEP valve could result in the CPAP machine shunting its flow to maintain the set pressure. Therefore, a PEEP valve is not needed for this configuration as it did not significantly increase helmet pressure.
Strengths and Limitations
The TestChest lung simulator with AQAI SIS software is particularly suited to optimize ventilation treatments without risk to actual patients. Unlike simpler lung simulators, the 8 liter volume of the TestChest bellows allows accurate simulation of the vital capacity of a human lung.11 The simulator integrates oxygen and PEEP input in real time, and in tandem with AQAI SIS, displays the immediate physiological effects of the treatment. The SIS software allows high-fidelity modeling of an ARDS patient and demonstrates changes in the treatment’s effectiveness as the disease progresses.
While this study supports the safety and efficacy of Subsalve Oxygen Treatment Hood CPAP, it is limited in its scope compared to a clinical study. Our scenario simulates a single ARDS patient over the course of disease and cannot reflect the complete variability observed in clinical practice as actual patients vary in both the severity of their disease and their response to treatment.
Conclusion
We demonstrate that a CPAP machine paired with the Subsalve Oxygen Treatment Hood provides sufficient support to a simulated patient breathing and increase blood oxygenation in moderate and severe forms of ARDS, providing an alternative to mechanical ventilation.
Our results define treatment parameters which physicians may use to guide the use of helmet CPAP in clinical practice. Our findings also suggest that use of helmet ventilation may provide another viable therapeutic option when treating other respiratory conditions where increased PEEP is desired. Further investigation to determine the applicability of helmet ventilation to treat respiratory failure from other causes is particularly important in low-resource settings where helmet ventilation has the potential to greatly reduce patient mortality where respiratory support options remain limited. Our study supports the use of the TestChest as a preliminary test for optimizing emerging ventilation techniques.
Abbreviations
ARDS, acute respiratory distress syndrome; CPAP, continuous positive airway pressure; EtCO2, end-tidal carbon dioxide; FiO2, fraction of inspired oxygen; HFNC, high flow nasal cannula; LPM, liters per minute; NIV, noninvasive ventilation; PaO2, partial pressure of oxygen; PEEP, positive end expiratory pressure; SIS, simulation interface software; SpO2, oxygen saturation.
Data Sharing Statement
The datasets supporting these conclusions are available from the authors by reasonable request.
Acknowledgments
Inventilator LLC contracted with NYU on a project studying a similar ventilation system. NYU was largely funded by the CDC Foundation, and Inventilator’s role was in collecting and shipping supplies, creating and providing training modules for health care workers, and analyzing data collected through the study. During COVID, Inventilator ran a program with the state of Rhode Island to collect and refurbish CPAP machines, for use in simple, positive-pressure ventilation as performed in the paper. Subsalve is a local manufacturer in Rhode Island who makes the Oxygen helmets used in the study. Inventilator maintained relationships with health care organizations around the country during COVID surges, and on eight occasions, health care systems purchases sample units of systems similar to the ones used in the paper for evaluation. Each purchase was for $300, and a total of eight units were sold.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Financial support was provided by the RI Commerce Corporation.
Disclosure
Mr Michael Lombardi authored the Instructions for Use (IFU) document for the Subsalve helmet device which supplemented its FDA authorization. The authors report no other conflicts of interest in this work.
References
1. Amirfarzan H, Cereda M, Gaulton TG, et al. Use of helmet CPAP in COVID-19 – a practical review. Pulmonology. 2021;27(5):413–422. doi:10.1016/j.pulmoe.2021.01.008
2. Chao K-Y, Wang J-S, Liu W-L. Role of helmet ventilation during the 2019 coronavirus disease pandemic. Sci Prog. 2022;105(2):003685042210928. doi:10.1177/00368504221092891
3. Patel BK, Wolfe KS, Pohlman AS, Hall JB, Kress JP. Effect of noninvasive ventilation delivered by helmet vs face mask on the rate of endotracheal intubation in patients with acute respiratory distress syndrome. JAMA. 2016;315(22):2435. doi:10.1001/jama.2016.6338
4. Ferreyro BL, Angriman F, Munshi L, et al. Association of noninvasive oxygenation strategies with all-cause mortality in adults with acute hypoxemic respiratory failure. JAMA. 2020;324(1):57. doi:10.1001/jama.2020.9524
5. Chaudhuri D, Trivedi V, Lewis K, Rochwerg B. High-flow nasal cannula compared with noninvasive positive pressure ventilation in acute hypoxic respiratory failure: a systematic review and meta-analysis. Critic Care Explorat. 2023;5(4):e0892. doi:10.1097/cce.0000000000000892
6. Lucchini A, Giani M, Isgrò S, Rona R, Foti G. The “helmet bundle” in COVID-19 patients undergoing non invasive ventilation. Intensive Crit Care Nurs. 2020;58:102859. doi:10.1016/j.iccn.2020.102859
7. Ventilators and Ventilator Accessories EUAs. U.S. Food & Drug Administration. Available from: https://www.fda.gov/medical-devices/covid-19-emergency-use-authorizations-medical-devices/ventilators-and-ventilator-accessories-euas.
8. Ahonkhai AA, Musa AZ, Fenton AA, et al. The CircumVent Project: a CPAP/O2 helmet solution for non-invasive ventilation using an implementation research framework. Implement Sci Commun. 2021;2(1). doi:10.1186/s43058-021-00193-y
9. Kyeremanteng K, Gagnon L-P, Robidoux R, et al. Cost analysis of noninvasive helmet ventilation compared with use of noninvasive face mask in ARDS. Can Respir J. 2018;2018:1–5. doi:10.1155/2018/6518572
10. Operator Manual TestChest V2. Available from: http://www.organis-gmbh.ch/wp-content/uploads/2015/05/Operator_Manual_TestChest.pdf.
11. Heinrichs W. Chapter 5 - Physiologic modeling for simulators. In: Clinical Simulation.
12. Patroniti N, Foti G, Manfio A, Coppo A, Bellani G, Pesenti A. Head helmet versus face mask for non-invasive continuous positive airway pressure: a physiological study. Intensive Care Med. 2003;29(10):1680–1687. doi:10.1007/s00134-003-1931-8
13. Carbon dioxide. The National Institute for Occupational Safety and Health. Available from: https://www.cdc.gov/niosh/idlh/124389.html.
14. Lombardi MR. Instructions for Use | Subsalve Oxygen Treatment Hood. Cleared by the US Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) during the Covid-19 pandemic. 2020.
15. Geng S, Mei Q, Zhu C, et al. High flow nasal cannula is a good treatment option for COVID-19. Heart Lung. 2020;49(5):444–445. doi:10.1016/j.hrtlng.2020.03.018
16. Cesarano M, Grieco DL, Michi T, et al. Helmet noninvasive support for acute hypoxemic respiratory failure: rationale, mechanism of action and bedside application. Ann Intens Care. 2022;12(1). doi:10.1186/s13613-022-01069-7
17. Taccone P, Hess D, Caironi P, Bigatello LM. Continuous positive airway pressure delivered with a “helmet”: effects on carbon dioxide rebreathing. Crit Care Med. 2004;32(10):2090–2096. doi:10.1097/01.CCM.0000142577.63316.C0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.