Back to Journals » Infection and Drug Resistance » Volume 13
Characteristics, Outcomes and Indicators of Severity for COVID-19 Among Sample of ESNA Quarantine Hospital’s Patients, Egypt: A Retrospective Study
Authors Ghweil AA, Hassan MH ![]() , Khodeary A
, Khodeary A ![]() , Mohamed AO, Mohammed HM, Abdelazez AA, Osman HA
, Mohamed AO, Mohammed HM, Abdelazez AA, Osman HA ![]() , Bazeed SES
, Bazeed SES ![]()
Received 22 May 2020
Accepted for publication 24 June 2020
Published 17 July 2020 Volume 2020:13 Pages 2375—2383
DOI https://doi.org/10.2147/IDR.S263489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Ali A Ghweil,1 Mohammed H Hassan,2 Ashraf Khodeary,3 Ahmed Okasha Mohamed,4 Haggagy Mansour Mohammed,5 Ahmed Alyan Abdelazez,1 Heba Ahmed Osman,1 Shamardan Ezzeldin S Bazeed1
1Department of Tropical Medicine and Gastroenterology, Faculty of Medicine, South Valley University, Qena 83523, Egypt; 2Department of Medical Biochemistry, Faculty of Medicine, South Valley University, Qena 83523, Egypt; 3Clinical Pathology Department, Faculty of Medicine, Sohag University, Sohag 82519, Egypt; 4Department of Radiology, Faculty of Medicine, South Valley University, Qena 83523, Egypt; 5Department of Chest Diseases, Faculty of Medicine, South Valley University, Qena 83523, Egypt
Correspondence: Mohammed H Hassan
Medical Biochemistry Department, Faculty of Medicine, South Valley University, Qena, Egypt
Tel +201098473605
Email [email protected]
Background: The risk factors, disease characteristics, severity, and mortality of COVID-19 are unclear, particularly in Egypt.
Objective: The objective was to analyze the patients’ characteristics, hematological, biochemical, and chest imaging findings among the cohort of patients with COVID-19 in Egypt and also to shed light on the predictors of COVID-19 severity.
Patients and Methods: A retrospective study was conducted on 66 patients with COVID-19 in Egypt. Medical history, imaging data (CT chest findings), and measured hematological and biochemical parameters at diagnosis were recorded in the form of complete blood counts and differential counts; CRP, ESR, serum ferritin, creatinine, and liver function tests . Results of real-time reverse transcription-polymerase chain reaction (rRT-PCR) for detection of SARS-CoV-2 RNA at diagnosis and during follow up of these patients were also recorded.
Results: The study included 36 patients with mild to moderate COVID-19 and 30 patients with severe/critical infection. There was a significant older age among severe (62.6 years old ± 10.1SD) than mild to moderate infection (55.5 ± 10.1) (p˂0.05). Fever, dry cough, dyspnea, and sore throat malaise were highly frequent among COVID-19 patients, while headache and diarrhea were the least frequently occurring manifestations. All included cases (30 patients, 100%) with severe COVID-19 showed crazy-paving appearance (in the form of reticular and/or interlobular septal thickening) with or without GGO. There were significantly lower mean values of WBCs, lymphocytic count, total protein, and albumin among the severely infected than those who had mild to moderate COVID-19 infection, p˂0.05 for all. Additionally, there were significantly higher mean values of CRP, ESR, ferritin, ALT, and AST among patients with severe/critical COVID-19 when compared with those having mild to moderate COVID-19, p˂0.05 for all.
Conclusion: Among the studied demographic, clinical, hematological, biochemical, and imaging data, dyspnea, diabetes mellitus, lymphopenia, raised CRP, ESR, ferritin, ALT, AST, low albumin, and presence of CT chest findings could be considered as predictors for COVID-19 severity using binary logistic regression analysis.
Keywords: COVID-19, Egypt, clinical data, hematological parameters, SARS-CoV-2 RNA, biochemical markers, severity
Introduction
The outbreak of the 2019 novel coronavirus disease (COVID-19) in Wuhan, China, has spread rapidly worldwide.1 This coronavirus was named as severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) by the World Health Organization and International Committee on Taxonomy of Viruses.2 On the 11th of March 2020, the WHO announced COVID-19 as a pandemic infectious disease. Since then, all practice, knowledge, and attitudes have been continuously developed for the COVID-19 siege.3 The full clinical presentation of COVID-19 still not understood, but among the most common presentations were cough, fever, dyspnea, and pneumonia. To date, no effective vaccines or specific drugs have been reported that specifically act against COVID-19.4 So, early identification of severity and prognosis of COVID-19 is very important to enable intervention for the reduction of mortality risk. Egypt announced the detection of the first COVID-19 case on the 14th of February 2020.5 After this, Egypt aimed to prevent the spread of COVID-19 infection with a partial ban that began on the 25th of March. Nasopharyngeal swabs for real-time reverse transcription-PCR (rRT-PCR) were obtained from patients with symptoms and, for cases confirmed to have COVID-19, contacts from the previous 2 weeks were traced and swabs were also obtained from them. rRT-PCR was repeated 48 h later for highly suspicious patients. Additionally, screening at the Egyptian airports by measurement of body temperature, clinical evaluation, and the use of the rapid diagnostic specific IgM and IgG test was performed.6 Since no previous Egyptian studies could be traced in the literature regarding COVID-19, we performed a retrospective analysis of a cohort of patients proved to have COVID-19 who were managed in ESNA’s quarantine hospital, Upper Egypt. The analysis included their characteristics and outcomes. Additionally, we assessed some routinely done hematological and biochemical parameters as indicators for COVID-19 severity and their possible prognostic values in such infectious disease.
Patients and Methods
The current retrospective cohort study has been conducted on a series of COVID-19 patients who were admitted to ESNA’s quarantine hospital, Upper Egypt during the period from March 2020 to April 2020. Before starting the study, approval from the Ethics Committee, Faculty of Medicine, South Valley University, Qena, Egypt, was obtained (Ethical approval code: SVU2020/6/48). Additionally, informed written consent from the patients or relatives for use of their medical reports was obtained. The study was performed in line with the Declaration of Helsinki. Patients proved to have COVID-19 infection and who had inflammatory diseases such as chronic obstructive pulmonary disease or immunological diseases were excluded to avoid any confounding factors affecting the inflammatory markers that were assessed in the study. Also, those with missed data were excluded.
Diagnosis of COVID-19 is based on the history of epidemiologic exposure. Clinical manifestations include: (1) fever and/or respiratory symptoms; (2) imaging features of COVID-19 infection; (3) total white blood cell counts showing normal, decreased, or reduced lymphocyte count in the early onset stage.7 In addition, diagnosis was based on a positive result for the COVID-19 nucleic acid via real-time reverse transcript-ion-polymerase chain reaction (rRT-PCR) in samples from blood or respiratory tract swabs which were performed at Central Laboratories, Ministry of Health and Population, Cairo, Egypt. The assays were performed using a nucleic acid diagnostic kit (PCR-Fluorescence probing) for the qualitative detection of the ORF1ab and a specific conserved sequence of coding nucleocapsid protein N genes of novel coronavirus (2019-nCOV). This kit was supplied by Sansure Biotech Inc., Hunan Province, China with catalog No. S3102E, using a 7500 real-time fluorescence quantitative RT-PCR system (Applied Biosystems, Foster City, CA, USA) to achieve detection of sample RNA through fluorescent signal changes.
Confirmed infected COVID-19 cases were categorized according to the latest guidelines to have severe/critical illness based on the presence of any of the following: dyspnea with a respiratory rate equal to or more than 30 cycle/min; oxygen saturation percent equal to or less than 93 at rest; PaO2/FiO2 equal to or less than 300 mmHg; respiratory failure with the requirement for mechanical ventilation; shock; other organ dysfunction syndrome and ICU admission needed.8 COVID-19 patients not having these criteria with a positive nucleic acid test for COVID-19 were considered to have mild to moderate disease severity.9
Detailed medical history for the included patients was recorded in the form of age, gender, nationality, BMI, co-morbidity (eg, diabetes mellitus, hypertension, ischemic heart disease), and smoking history. Clinical manifestations (fever, dry cough, dyspnea, sore throat, malaise, diarrhea, or headache) were analyzed. Findings of CT chest (presence or absence of ground glass or crazy paving appearance) were also recorded. Measured hematological and biochemical parameters at diagnosis were recorded in the form of complete blood counts and differential counts; CRP, ESR, serum ferritin, creatinine, and liver function tests were added.
Statistical Analysis
IBM SPSS Statistics v.22 was used for the analysis of the data. Mean ± SD was used for the expression of quantitative data, while, number and percentage were used for qualitative data. Kolmogorov–Smirnov and Shapiro–Wilk normality tests were used. For normally distributed data, the independent samples t-test was used for comparison between two quantitative data, and one way-ANOVA was for comparison between more than two quantitative data. For qualitative variables, Chi-square (χ2) and Fisher’s Exact tests were used. Binary logistic regression analysis was used to study the predictors of COVID-19 severity. The level of significance was considered at P˂0.05.
Results
Demographic and Clinical Characteristics of COVID-19 Patients
This retrospective study included 66 confirmed COVID-19 patients who were categorized according to disease severity into 36 patients (28 males and 8 females) with mild to moderate infection and 30 patients (20 males and 10 females) with severe infection. The patients were BMI-matched as indicated by the non-significant difference between them with a non-significant difference as regard gender (p˃0.05 for both). There was a significant older age among severe (62.6 years old ±10.1SD) than mild to moderate infection (55.5 ± 10.1) (p˂0.05). The co-morbidities (diabetes mellitus, hypertension, and ischemic heart disease) and smoking history presented among the included patients were with their frequency percentages as presented in (Table 1), with non-significant differences between the two groups (p˂0.05).
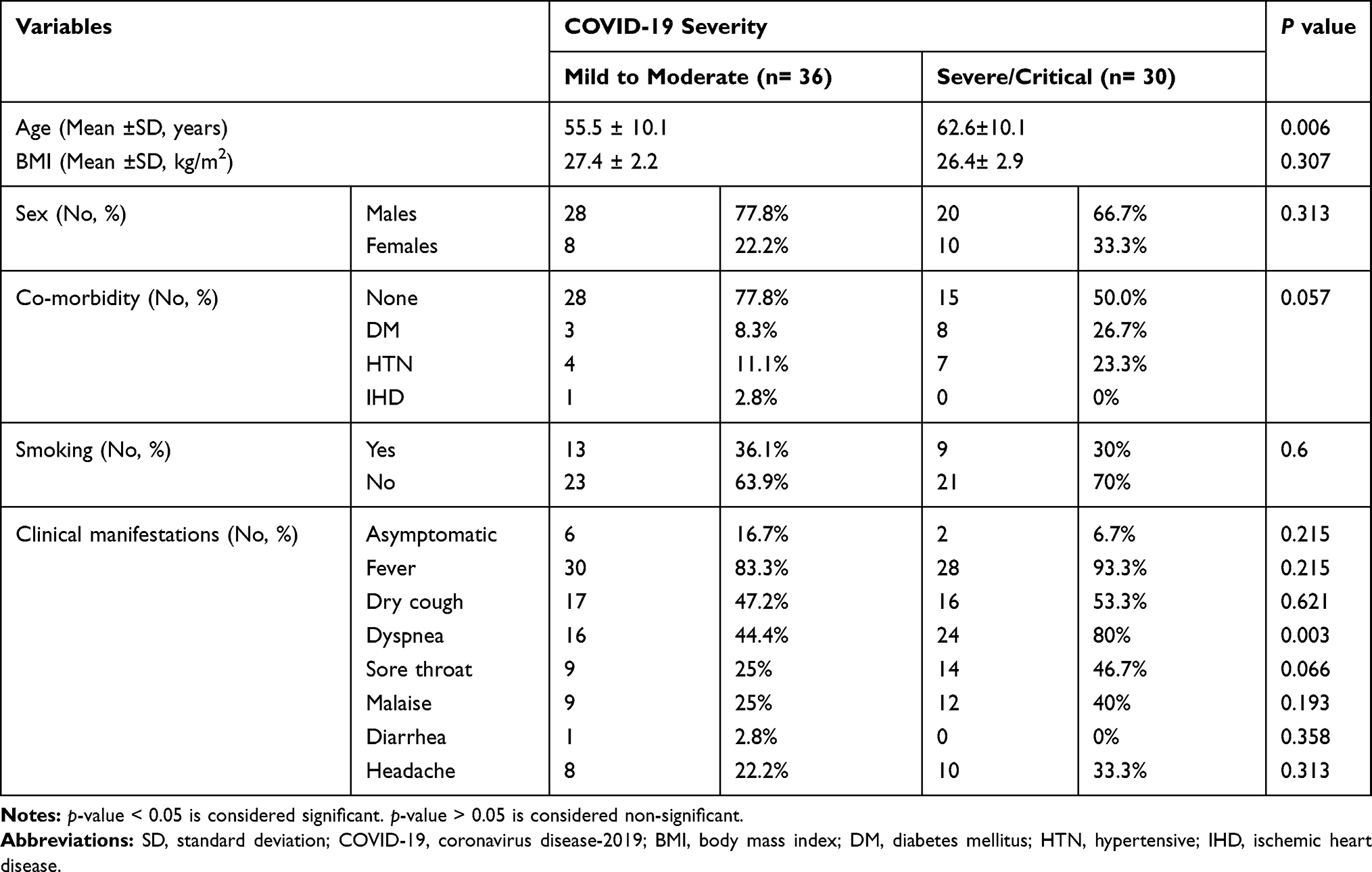 |
Table 1 Demographic and Clinical Data of the Included COVID-19 Patients |
Regarding the frequency percentages of the presenting manifestations in the form of fever, dry cough, dyspnea, sore throat malaise, headache, and diarrhea, all are described in Table 1, with significantly higher values for dyspnea among severely infected patients vs those with mild to moderate infection (p˂0.05). Fever, dry cough, dyspnea, and sore throat malaise were highly frequent among COVID-19patients, while headache and diarrhea were the least frequently occurring manifestation (Table 1).
CT Chest Findings of the Included COVID-19 Patients
Normal CT chest was recorded in 12 cases (33.3%) with mild to moderate infection and the remaining 24 patients (66.6%) exhibited focal or multifocal ground glass opacities (GGO) with patchy consolidations and distributed peripherally (subpleural), involving mostly the posterior part or lower lung lobes, while all include cases (30 patients, 100%) with severe COVID-19 showed crazy-paving appearance (in the form of reticular and/or interlobular septal thickening) with or without GGO (Table 2).
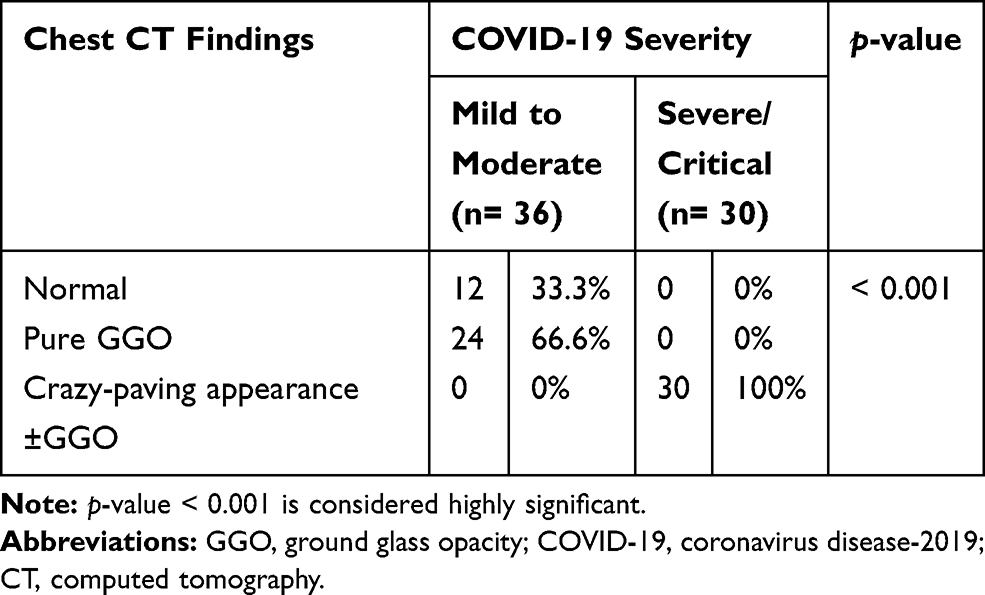 |
Table 2 Chest CT Findings of the Included COVID-19 Patients |
Hematological and Biochemical Indicators for COVID-19 Severity
There were significantly lower mean values of WBC (x103 mm−3), lymphocytic count (x103 mm−3), total protein (g/dL) and albumin (g/dL) (3.9 ± 1.5, 0.85 ± 0.3, 6.06 ± 0.4 and 2.5 ± 0.2, respectively) among severely infected than those had mild to moderate COVID-19 (5.6 ± 1.7, 1.12 ± 0.4, 6.9 ± 0.3, and 2.9 ± 0.1), p˂0.05 for all (Table 3). Additionally, there were significantly higher mean values of CRP (mg/dL), ESR, ferritin (ng/mL), ALT (IU/L) and AST (IU/L) among patients with severe/critical COVID-19 (119.8 ± 39, 78.7 ± 20.4, 440.3 ± 87.3, 41.5 ± 6.7, and 44.5 ± 4.5, respectively) when compared with those having mild to moderate COVID-19 (51.1 ± 9.5, 50.8 ± 21.3, 268.6 ± 57.5, 33.3 ± 8.03, and 32.8 ± 7.2, respectively), p˂0.05 for all (Table 3). As regards the analysis of the abnormalities of the measured hematological and biochemical parameters as categorical data, there were no significant differences (p>0.05) between COVID-19 severity categories as regards the frequency percentage of anemia, leucopenia, raised ESR or serum creatinine, low serum total protein, or albumin (Table 4). There were significantly higher frequencies of lymphopenia, raised CRP, ALT, and AST among severe COVID-19 in comparison to mild to moderate COVID-19, p˂0.05 for all (Table 4).
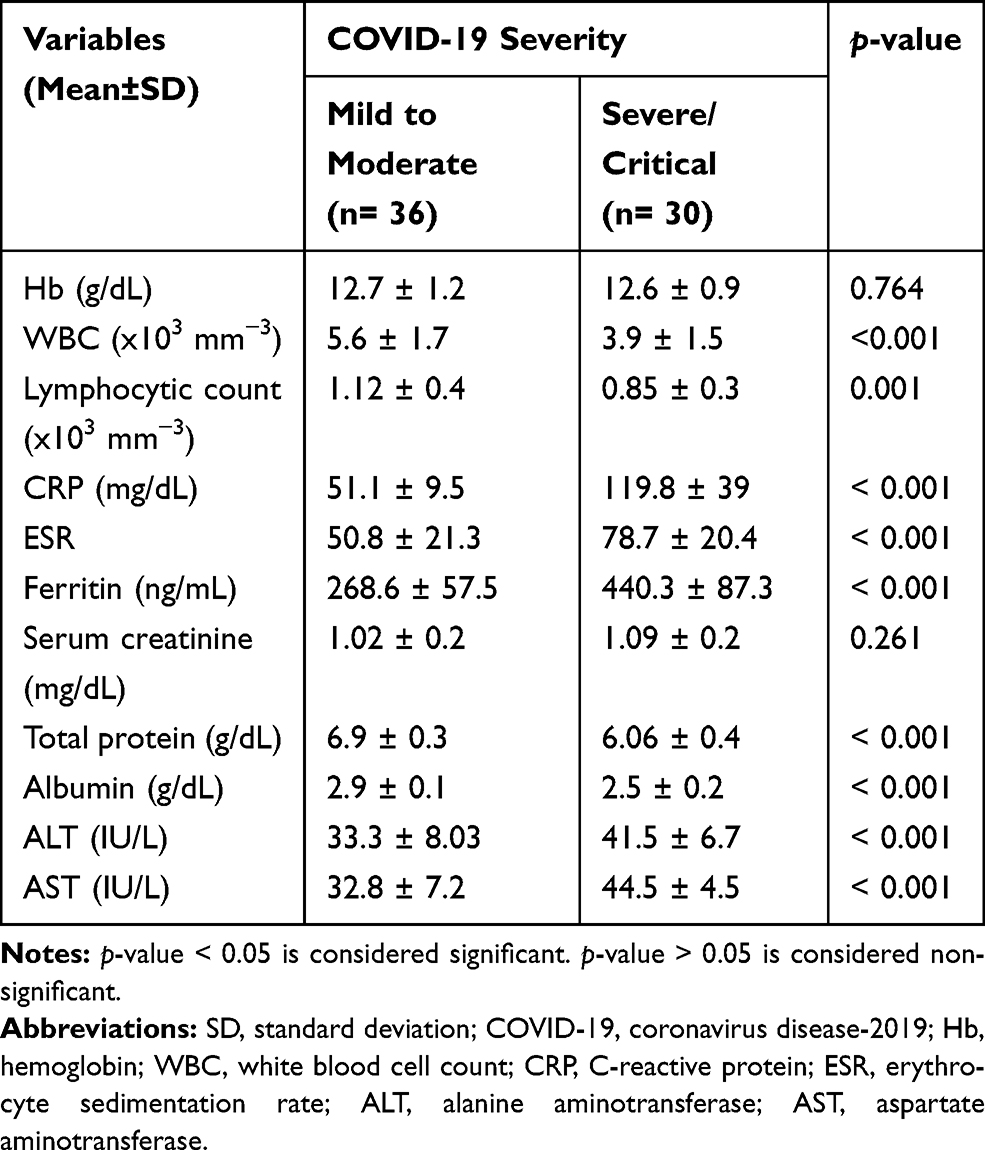 |
Table 3 Mean±SD of Some Measured Hematological and Biochemical Markers of the Included COVID-19 Patients at Admission |
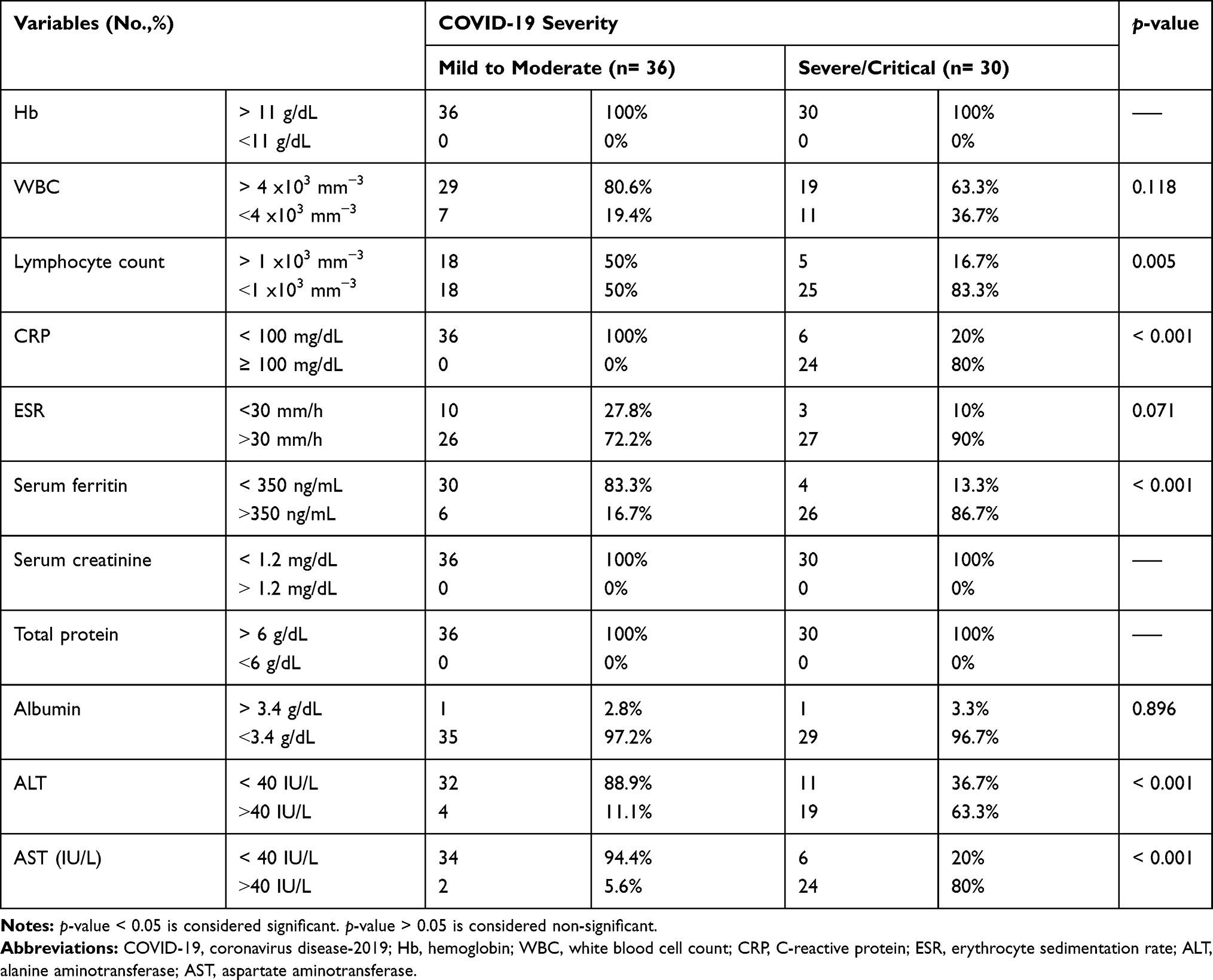 |
Table 4 Comparison of the Frequency Percent of Some Hematological and Biochemical Abnormalities of the Included COVID-19 Patients Measured at Admission, in Terms of COVID-19 Severity |
Outcome and Recovery Period of the Included COVID-19 Patients
The current report revealed that all patients who had mild to moderate COVID-19 were improved (36 cases, 100%) and the majority of those who had severe/critical COVID-19 infection were also cured (28 cases, 93.3%) with no significant differences between the two groups, p˃0.05 (Table 5). Meanwhile, the proportion of patients whom nucleic acid test turned negative within ≤8 days was higher among cases with mild to moderate infection (23 patients, 63.9%) than those with severe/critical COVID-19 (2 cases, 6.7%), p˂0.05 for all (Table 5). Additionally, the frequency percentages of patients whom nucleic acid test turned negative within >8–14 days or who were still positive after 14 days were significantly higher among severe/critical COVID-19 (22 cases (73%) and 6 cases (20%) respectively) than those had mild to moderate infection (12 cases (33.3%)) and 1 case (2.8%), p˂0.05 for all (Table 5).
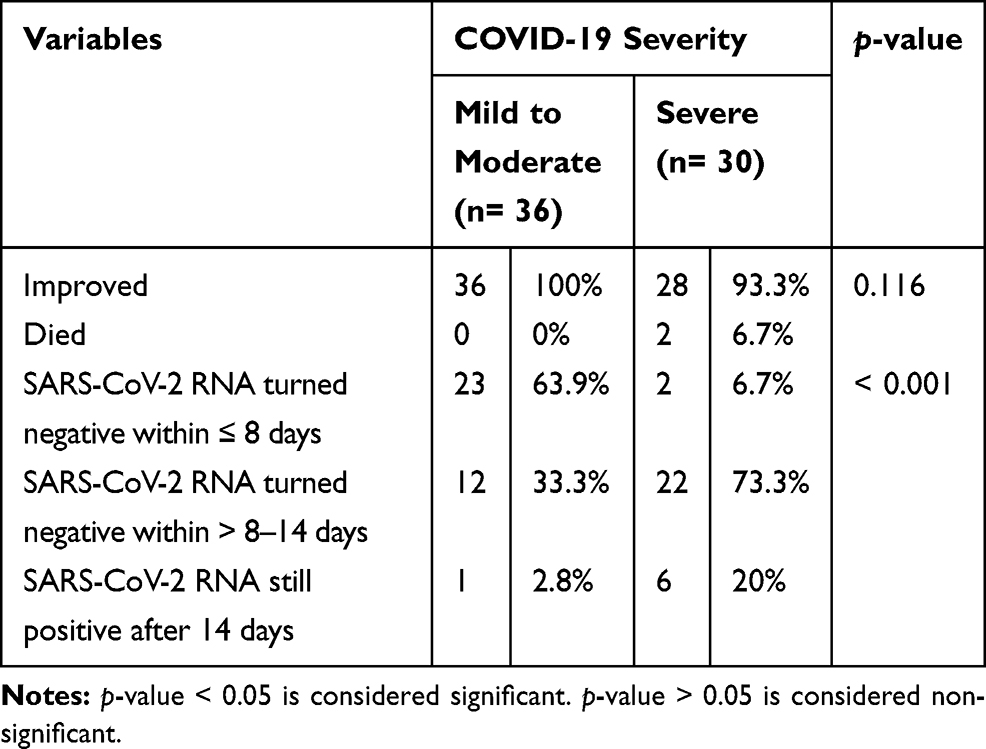 |
Table 5 Outcome and Recovery Duration of the Studied COVID-19 Patients |
Indicators of COVID-19 Severity Among the Included Patients Using Binary Logistic Regression Analysis
Predictors of severity for COVID-19 in the studied patients were presence of diabetes mellitus as a co-morbidity (95% CI: 1.14–21.5, p=0.032), dyspnea (95% CI: 1.64–15.2, p=0.004), lymphopenia (95% CI: 0.99–1.0, p=0.014), raised inflammatory markers in the form of CRP (95% CI: 1.04–1.13), ESR (95% CI: 1.03–1.08), and ferritin (95% CI: 1.01–1.03) with p<0.001 for all, abnormal liver function in the form of low serum albumin (95% CI: 0.0–0.002) and raised liver enzymes in the form of ALT (95% CI: 1.07–1.28) and AST (95% CI: 1.42–31.9) with p<0.001 for all. Additionally, the presence of CT chest findings was a predictor (95% CI: 0.001–0.04, p<0.001), whereas there were no associations among COVID-19 severity and other studied parameters in the studied patients (Table 6).
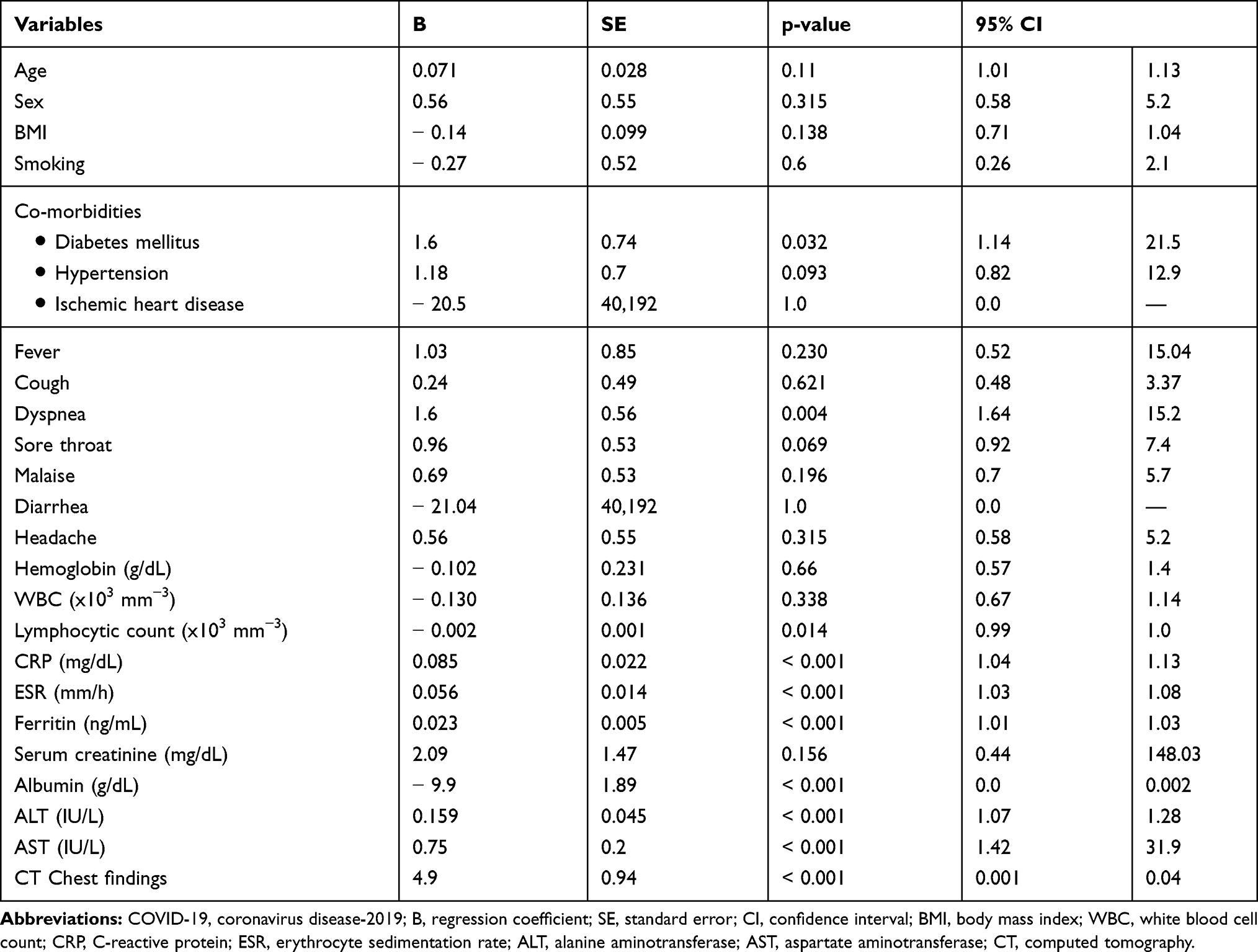 |
Table 6 Binary Logistic Regression Analysis for Factors Predictive of COVID-19 Severity |
Discussion
Coronavirus disease (COVID-19) emerged in December 2019 in Wuhan. However, the risk factors, disease characteristics, severity, and mortality of COVID-19 are unclear,9 particularly in Egypt, so our study aim was to shed light on these points.
The current study revealed that severe COVID-19 was more frequent in older age, while mild to moderate infection was more frequent in younger patients. In agreement with our findings, Liu et al10 reported that elderly patients with COVID-19 are more likely to progress to severe COVID-19 disease in comparison with young and middle-aged COVID-19 patients. Also, Mahase11 and Yang et al12 reported similar findings. This could be explained by the age-dependent decline in cell-mediated immune function and reduced humoral immune function.13
Among the co-morbidities associated with COVID-19 in our study, diabetes mellitus, hypertension, and ischemic heart disease were the most prevalent chronic diseases. These findings were in accordance with a meta-analysis study which reported that hypertension, cardiovascular diseases, and diabetes mellitus were among the most prevalent underlying diseases among hospitalized COVID-19 patients.14 Using logistic regression analysis, the present study revealed that the presence of diabetes mellitus could be a significant predictor for the severity of COVID-19. In line with our findings, Marhl et al15 reported a higher risk for COVID-19 among diabetic patients because of the associated dysregulation of angiotensin-converting enzyme 2 (ACE2), liver dysfunction, and chronic inflammation. Also, Singh et al16 provided evidence of increased incidence and severity of COVID-19 in diabetic patients.
Limited data are available regarding the contribution of tobacco smoking to the spread, severity, and poor outcome in COVID-19.17 Smoking has been related to higher ACE2 expression, which has been stated to be a receptor for SARS-CoV-2 (pre-print).18 Our findings revealed the lack of significant difference regarding COVID-19 severity in terms of smoking. A systematic review included five studies and reported that smoking may be associated with a negative outcome.19 This heterogeneity could be attributed to differences in the study designs, outcomes, or regions.
Our study revealed that dyspnea, fever, dry cough, sore throat, and malaise were the most frequent clinical presentations among COVID-19 patients, while headache and diarrhea were the least frequent ones, and some patients were asymptomatic. In line with our findings, Guan et al20 reported that the most common COVID-19 presentations were fever and cough (88.7% and 67.8%, respectively). Although nausea and/or vomiting (5%) and diarrhea (3.8%) were reported, they were uncommon. A possible explanation for the mild gastrointestinal manifestation is the attenuation of SARS-CoV-2 virulence after swallowing by the effect of digestive enzymes which cause its degradation.9 Also, Chan et al21 and Wang et al22 were in agreement with our findings. Additionally, our data revealed that only dyspnea rather than other presenting manifestations was significantly associated with COVID-19 severity. In accordance, Zheng et al23 reported a significant positive association of shortness of breath/dyspnea with COVID-19 progression to severe illness and death. Additionally, a meta-analysis study reported similar findings and recommended dyspnea rather than fever as an indicator of poor outcome in COVID-19 patients.24
The use of CT for the diagnosis of viral pneumonia allows patients with suspected SARS-CoV-2 infection to be isolated and treated in time for recovery, thus optimizing patient management.25 The results of the current study showed a significantly high frequency of bilateral peripheral GGO among patients with mild to moderate COVID-19, while in those with severe/critical infection, their CT chest revealed a crazy-paving appearance. Additionally, CT chest findings were a significant predictor for the severity of COVID-19 infection. Pan et al26 reviewed 21 confirmed COVID-19 patients. They noticed the rapid growth of GGOs into crazy-paving appearance as the disease progresses, with its disappearance in the absorption stage, concluding that crazy-paving pattern could be considered as one of the indices that could be used to evaluate the course of the disease. Similar findings were reported by Song et al.27 Also, in line with our findings are Wang et al22 and Majidi and Niksolat.28
In the present study, we analyzed the hematological indices of the included COVID-19-patients and revealed significantly lower mean values of WBCs and lymphocytic count among severely infected patients than those had mild to moderate COVID-19. Additionally, lymphopenia was significantly associated with the severity of COVID-19. In accordance, both Fan et al29 and Li and Fan30 reported lymphocytopenia among most COVID-19 patients on admission and leucopenia. Lymphopenia has been well described in a retrospective analysis of patients in Hong Kong and Singapore afflicted with SARS-CoV in 2003 and was associated with adverse outcome and ICU stay.31 Although the cytokine profile and the dynamic lymphocytic changes and their relation to COVID-19 severity are still not understood, some of the severely infected patients exhibited significant lymphocytopenia and neutrophilia with decreased T cells particularly CD8+ type and raised cytokines (IL-2, -6 and -10, and interferon-γ) than those had mild infection, with the subsequent gradual normalization of such parameters among severely infected survivors. This indicates that the neutrophil/CD8+ T cell ratio is a powerful prognostic factor in COVID-19. Additionally, lymphopenia was noticed more in severe than mild infection and was associated with disease severity.32
It has been reported that viral infection could induce a severe immunological reaction in the host, known as a cytokine storm, which is an acute systemic inflammatory syndrome characterized by fever and multiple organ dysfunction. Additionally, viral infection induces acute phase reactant production.33 Our findings revealed significantly higher acute phase reactants (CRP, ESR, and ferritin) among severely COVID-19 patients when compared with those who have mild to moderate infection and were significantly associated with COVID-19 severity. These findings were in agreement with many studies.10,30,34 Binding and storage of iron are functions of ferritin which are also associated with immune and inflammatory responses.35 The increase in the serum ferritin levels following bacterial or viral infection could be attributed to iron release into the reticuloendothelial system, and increased intracellular ferritin synthesis and release, with the decreased ability of ferritin transport into spleen and liver.36 Human angiotensin-converting enzyme 2 (ACE-2) receptor binding is one of the mechanisms by which COVID-19 can invade the human body with subsequent increased expression of ACE-2 in hepatocytes.37 In the present study, there were significantly higher mean serum values of both ALT and AST with significantly lower serum levels of total proteins and albumin among severely infected COVID-19 patients vs those who had mild to moderate infection. Additionally, we reported that raised ALT and AST serum levels and low serum albumin levels were significantly associated with COVID-19 severity. Hepatic dysfunction in SARS-CoV-2 infection was reported for the first time by Chen et al,38 who noticed increased serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) serum levels in 43.4% of COVID-19 cases from Wuhan, with mild elevation in most of them. Recently, a strong reasonable relation between abnormal liver biochemistries and SARS-CoV-2 infection severity has been highlighted.30 In a study in Shanghai, severe to critical cases exhibited significantly higher serum ALT and AST levels than those who had mild to moderate COVID-19.39 Similar findings were reported by other studies.17,40
Conclusion
This is the first retrospective Egyptian study describing patients' characteristics and predictors of severity in SARS-CoV-2 infection. It revealed that older age and non-Egyptian persons are more vulnerable to severe COVID-19. Additionally, CT chest findings, leucopenia, lymphocytopenia, raised CRP, ESR, ferritin, and liver enzymes significantly occurred more with severe than mild to moderate COVID-19. Finally, among the studied demographic, clinical, hematological, biochemical, and imaging data, leucopenia, raised ALT and CT chest findings could be considered as predictors for COVID-19 severity using multivariate regression analysis.
Study Limitations
Retrospective design and relatively small sample size were the main limitations to the current study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lei S, Jiang F, Su W, et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClin Med. 2020;21:100331. doi:10.1016/j.eclinm.2020.100331
2. WHO. WHO director-general’s remarks at the media briefing on SARS-CoV2 on 16 March 2020; 2020. Available from: http://www.nhc.gov.cn/xcs/yqfkdt/202003/114113d25c1d47aabe68381e836f06a8.shtml
3. Alzoubi H, Alnawaiseh N, Al-Mnayyis A, Abu- Lubada M, Aqel A, Al-Shagahin H. COVID-19 - knowledge, attitude and practice among medical and non-medical university students in jordan. J Pure Appl Microbiol. 2020;14(1):17–24. doi:10.22207/JPAM.14.1.04
4. Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
5. WHO. COVID-2019 situation report—26. 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200215-sitrep-26-covid-19.pdf?sfvrsn=a4cc6787_2. (
6. Hassany M, Abdel-Razek W, Asem N, AbdAllah M, Zaid H. Estimation of COVID-19 burden in Egypt. Lancet Infect Dis. 2020. doi:10.1016/S1473-3099(20)30319-4
7. Wang YY, Jin YH, Ren XQ, et al. Updating the diagnostic criteria of COVID-19 “suspected case” and “confirmed case” is necessary. Mil Med Res. 2020;7(1):17. doi:10.1186/s40779-020-00245-9
8. Li L, Li R, Wu Z, et al. Therapeutic strategies for critically ill patients with COVID-19. Ann Intensive Care. 2020;10(1):45. doi:10.1186/s13613-020-00661-z
9. Zhang J, Wang X, Jia X, et al. Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clin Microbiol Infect. 2020;26(6):767–772. doi:10.1016/j.cmi.2020.04.012
10. Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J Infect. 2020. doi:10.1016/j.jinf.2020.03.005
11. Mahase E. Covid-19: death rate is 0.66% and increases with age, study estimates. BMJ. 2020;369:m1327. doi:10.1136/bmj.m1327
12. Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. 2020;94:91–95. doi:10.1016/j.ijid.2020.03.017
13. Zhou F, Yu T, Du R, Fan G, Liu Y. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054e62. doi:10.1016/S0140-6736(20)30566-3
14. Emami A, Javanmardi F, Pirbonyeh N, Akbari A. Prevalence of underlying diseases in hospitalized patients with COVID-19: a systematic review and meta-analysis. Arch Acad Emerg Med. 2020;8(1):e35.
15. Marhl M, Grubelnik V, Magdič M, Markovič R. Diabetes and metabolic syndrome as risk factors for COVID-19. Diabetes Metab Syndr. 2020;14(4):671–677. doi:10.1016/j.dsx.2020.05.013
16. Singh AK, Gupta R, Ghosh A, Misra A. Diabetes in COVID-19: prevalence, pathophysiology, prognosis and practical considerations. Diabetes Metab Syndr. 2020;14(4):303–310. doi:10.1016/j.dsx.2020.04.004
17. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Prevalence, severity and mortality associated with COPD and Smoking in patients with COVID-19: A rapid systematic review and meta-analysis. PLoS One. 2020;15(5):e0233147. doi:10.1371/journal.pone.0233147
18. Cai G, Cui X, Zhu X, Zhou J. A Hint on the COVID-19 Risk: population disparities in gene expression of three receptors of SARS-CoV. 2020.
19. Vardavas CI, Nikitara K. COVID-19 and smoking: A systematic review of the evidence. Tob Induc Dis. 2020;18(March):20. doi:10.18332/tid/119324
20. Guan GW, Gao L, Wang JW, et al. Exploring the mechanism of liver enzyme abnormalities in patients with novel coronavirus-infected pneumonia. Zhonghua Gan Zang Bing Za Zhi. 2020;28(2):100–106. doi:10.3760/cma.j.issn.1007-3418.2020.02.002
21. Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514–523. doi:10.1016/S0140-6736(20)30154-9
22. Wang D, Hu B, Hu C, et al. Clinical Characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China.. JAMA. 2020;323(11):1061. doi:10.1001/jama.2020.1585
23. Zheng Z, Peng F, Xu B, Zhao J, Liu H, Peng J. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. J Infect. 2020. doi:10.1016/j.jinf.2020.04.021
24. Shi L, Wang Y, Wang Y, Duan G, Yang H. Dyspnea rather than fever is a risk factor for predicting mortality in patients with COVID-19. J Infect. 2020. doi:10.1016/j.jinf.2020.05.013
25. Li Y, Coronavirus Disease XL. 2019 (COVID-19): role of Chest CT in diagnosis and management. AJR Am J Roentgenol. 2020;4:1–7. doi:10.2214/AJR.20.22954
26. Pan F, Ye T, Sun P, et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology. 2020;295(3):715–721. doi:10.1148/radiol.2020200370
27. Song F, Shi N, Shan F, et al. Emerging coronavirus 2019-nCoV pneumonia. Radiology. 2020:200274. doi:10.1148/radiol.2020200274
28. Majidi H, Niksolat F. Chest CT in patients suspected of COVID-19 infection: A reliable alternative for RT-PCR. Am J Emerg Med. 2020. doi:10.1016/j.ajem.2020.04.016
29. Fan BE, Chong VCL, Chan SSW, et al. Hematologic parameters in patients with COVID-19 infection. Am J Hematol. 2020;95(6):E131–E134. doi:10.1002/ajh.25774
30. Li J, Fan JG. Characteristics and mechanism of liver injury in 2019 coronavirus disease. J Clin Transl Hepatol. 2020;8(1):
31. Chng WJ, Lai HC, Earnest A, Kuperan P. Haematological parameters in severe acute respiratory syndrome. Clin Lab Haematol. 2005;27(1):15–20. doi:10.1111/j.1365-2257.2004.00652.x
32. Liu J, Li S, Liu J, et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020;18:102763. doi:10.1016/j.ebiom.2020.102763
33. Cascella M, Rajnik M, Cuomo A, Dulebohn S, Napoli RD. Features, Evaluation and Treatment Coronavirus (COVID-19). StatPearls: Treasure Island, StatPearls Publishing; 2020.
34. Rodriguez-Morales AJC-O JA, Gutiérrez-Ocampo E, Villamizar-Peña R, et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Preprints. 2020:2020020378. doi:10.20944/preprints202002.0378.v3
35. Lalueza A, Ayuso B, Arrieta E, et al. Elevation of serum ferritin levels for predicting a poor outcome in hospitalized patients with influenza infection. Clin Microbiol Infect. 2020. doi:10.1016/j.cmi.2020.02.018
36. Senjo H, Higuchi T, Okada S, Takahashi O. Hyperferritinemia: causes and significance in a general hospital. Hematology. 2018;23(10):817–822. doi:10.1080/10245332.2018.1488569
37. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
38. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
39. Lu H, Ai J, Shen Y, et al. A descriptive study of the impact of diseases control and prevention on the epidemics dynamics and clinical features of SARS-CoV-2 outbreak in Shanghai, lessons learned for metropolis epidemics prevention. medRxiv. 2020. doi:10.1101/2020.02.19.20025031
40. Aly MH, Rahman SS, Ahmed WA, et al. Indicators of critical illness and predictors of mortality in COVID-19 patients. Infect Drug Resist. 2020;Volume 13:1995–2000. doi:10.2147/IDR.S261159
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.