Back to Journals » Open Access Emergency Medicine » Volume 14
Characteristics of Patients Presented with Complicated Appendicitis in Adama, Ethiopia: A Cross-Sectional Study
Received 24 July 2022
Accepted for publication 19 October 2022
Published 21 October 2022 Volume 2022:14 Pages 573—580
DOI https://doi.org/10.2147/OAEM.S383550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Haset Dagne,1 Tsega-Ab Abebaw2
1Maternal, and Child Health Department, Wereda 6 Health Center, Nifas Silk Lafto Sub-City, Addis Ababa, Ethiopia; 2School of Public Health, GAMBY Medical and Business College, Addis Ababa, Ethiopia
Correspondence: Tsega-Ab Abebaw, Tel +251911792982, Email [email protected]
Background: Complicated appendicitis (CA) is defined as perforated appendicitis, peritonitis, peri-appendicular abscess, or appendicular mass. One-third of patients who develop appendicitis are diagnosed with CA at presentation. Studies regarding the prevalence of CA are lacking in low-income countries, and the characteristics of patients presented with CA are incoherently identified.
Objective: To assess the prevalence and the significant characteristics associated with CA among patients admitted with the diagnosis of acute appendicitis at Adama Hospital Medical College.
Methods: A cross-sectional study was conducted from January 1, 2018, up to December 31, 2019. From a total of 1043 patients during the study period, the charts of 431 patients were selected using a systematic random sampling technique. Data were collected by a structured checklist. Bivariate and multivariable binary logistic regression analyses were employed to assess the association of patients’ characteristics with CA.
Results: Out of 431 patients, 157 (36.4%) had CA. Characteristics of patients having a significant association with CA were found to be generalized abdominal tenderness (AOR: 27.48, 95% CI: 4.03, 187.24), diagnosis with peritonitis (AOR: 14.87, 95% CI: 4.05, 54.54), right lower quadrant (RLQ) abdominal mass (AOR: 7.79, 95% CI: 2.02, 29.99), shock (10.37, 95% CI: 3.18, 33.76), white blood cell (WBC) count > 11,000 (AOR: 2.16, 95% CI: 1.02, 4.61), onset to visit interval of 8– 14 days (AOR: 10.45, 95% CI: 2.4, 45.52) and ultrasound report of acute appendicitis (AOR: 0.33, 95% CI: 0.13, 0.85), appendiceal abscess (AOR: 5.05, 95% CI: 1.48, 17.31), and appendiceal mass (AOR: 6.04, 95% CI: 1.45, 25.14).
Conclusion: The prevalence of CA was very high. Generalized abdominal tenderness, RLQ abdominal mass, shock, WBC count, onset to visit interval, abdominopelvic ultrasound report, and clinical diagnosis of peritonitis were significantly associated with CA.
Keywords: complicated appendicitis, characteristics of patients, acute appendicitis, Adama, Ethiopia
Introduction
The appendix is an immunologic organ that participates in the secretion of immunoglobulin, such as immunoglobulin A.1 Acute appendicitis is an inflammation of the vermiform appendix. It is a common cause of acute abdomen, with an estimated lifetime risk of 7–8% worldwide. It is typically diagnosed according to a reliable set of signs and symptoms and can be effectively treated with surgery, with low morbidity and mortality rates.1,2 Acute appendicitis can be divided into two main categories: uncomplicated and complicated.3
Acute appendicitis is often overlooked and a significant number of patients are presented with complications. Of the 300,000 appendectomies performed each year, 25% are due to complicated appendicitis (CA).4 The proportion of CA varies, and it can reach up to 50% in some reports.5
The diagnosis of CA is made by the macroscopic appearance during the trans-operative period or by histopathological study.5 Complicated appendicitis is defined as perforated appendicitis, peritonitis, peri-appendicular abscess, or appendicular mass.6 If acute appendicitis is left untreated, necrosis, gangrene, and perforation occur.1,7,8 Treatment of uncomplicated acute appendicitis is surgery. But in cases with CA, additional treatments such as percutaneous drainage and antibiotics and afterward delayed appendectomy are needed.9 Compared to the uncomplicated one, the prognosis worsens significantly in CA, predisposing the patient to a prolonged hospital stay, broad-spectrum antibiotics use and increased morbidity.10
Several studies have tried to evaluate CA, its contributing factors, and patients at risk. According to these studies, diabetes, diarrhea, malaise, epigastric pain, duration of symptoms before surgery, extremes of age, various laboratory markers or other novel parameters, types of medical insurance, imaging findings, and also the underlying pathology of an inflamed appendix were the identified factors associated to CA.11–15
This study is one amongst the few from low-income countries regarding the prevalence, and characteristics of patients presented with CA. There is no available data regarding the extent of CA and the patients’ characteristics in Ethiopia. The provision of the information is especially important for low-income countries like Ethiopia, where access to surgical care is limited. Therefore, this study aimed to assess the prevalence, and the significant characteristics associated with CA among patients admitted with the diagnosis of acute appendicitis in Adama Hospital Medical College (AHMC), Adama, Ethiopia.
The study will help generate data as a basis for subsequent studies and interventions. The results will provide information that will help clinicians diagnose CA early and begin timely management.
Materials and Methods
Study Area and Period
The study was conducted at Adama Hospital Medical College, Adama, Ethiopia from January 1, 2018, to December 31, 2019.
Study Design
An institution-based cross-sectional study was conducted.
Source and Study Population
The source population was all patients admitted with the diagnosis of appendicitis to the AHMC surgical ward during the study period. The study population consisted of patients who were selected by employing a systematic random sampling technique. All the desired information was gathered from the charts of the patients.
Sample Size
Epi Info version 7.2.4.0 software was used to calculate the sample size for a single population proportion. Since no published data showing the magnitude of CA in Ethiopia was available, 50% of prevalence was used to get the maximum sample size. Considering a 97% confidence level, a 4% margin of error, and a total source population of 1043, the calculated sample size was 431.
Sampling Procedure
The total number of patients admitted with a diagnosis of appendicitis in the Department of Surgery of AHMC from January 1, 2018, to December 31, 2019, was 1043. Of the 1043 patients, 431 patients were selected by a systematic random sampling technique. The patient registration list served as a sample frame.
The formula “K = N/n” was used for sample selection. The total number of patients (N=1043) divided by the actual sample size (n=431) gave a constant (K) of 2.4. The first sample was determined using the lottery method. Then every other patient was selected from the sampling frame.
Inclusion and Exclusion Criteria
All patients admitted to the AHMC surgical ward with the diagnosis of appendicitis during the study period were eligible, and charts of patients with incomplete data were excluded.
Variables
Dependent Variable
- Complicated appendicitis.
Independent Variables
- Demographic variables (age, sex, and residency).
- Subjective variables (site of abdominal pain, nausea, vomiting, anorexia, constipation, diarrhea, onset to first visit interval, and presence of comorbid illness).
- Objective variables (fever, site of abdominal tenderness, right lower quadrant (RLQ) mass, peritonitis, and shock).
- Investigations (white blood cell (WBC) count, and abdominopelvic ultrasound).
Operational Definitions
- Complicated appendicitis: Appendicitis with abscess formation, gangrenous appendix, or a perforated appendix with, or without peritonitis noted after surgery.
Data Collection Procedures
The data was collected by employing a structured checklist. The source populations’ medical registration numbers were collected from the surgical ward register book. All the desired quantitative information was collected from the charts of the patients.
Quality Assurance
To assure the quality of the data, the checklist was pre-tested on 5% of the targeted sample size at AHMC before running the actual data. Necessary modifications to the checklist were carried out based on the pre-test feedback. The reliability of the checklist was checked.
Data Management and Analysis
The data was collected under regular supervision after giving a one-day training course for two data collectors and a supervisor before the data collection process. The data collected from the charts were checked for completeness and consistencies, and then cleaned and entered using Epi Info version 7.2.4.0 statistical software and analyzed using the SPSS version 26 statistical package. Logical and consistency errors identified during data entry were corrected after revision of the original data. The descriptive analyses were presented by frequency tables and percentages. A multiple logistic regression model was fitted. All variables were screened by carrying out binary logistic regression analysis. Then, variables having a p-value less than 0.2 were taken to the multivariable binary logistic regression model to identify confounders. Statistical significance was declared when the p-value was less than 0.05 at 95% CI.
Results
Socio-Demographic Characteristics
The total number of patients’ charts reviewed was 431, with a 100% success rate. The mean age of respondents was 28.28 years, with a standard deviation of 13.79. The age range of respondents was 15–75 years. Most of the patients, 241 (55.9%), were in the age group of 15–25 years. Males accounted for 252 (58.5%) of the study participants, and the majority of the respondents, 296 (68.7%), were from urban areas (Table 1).
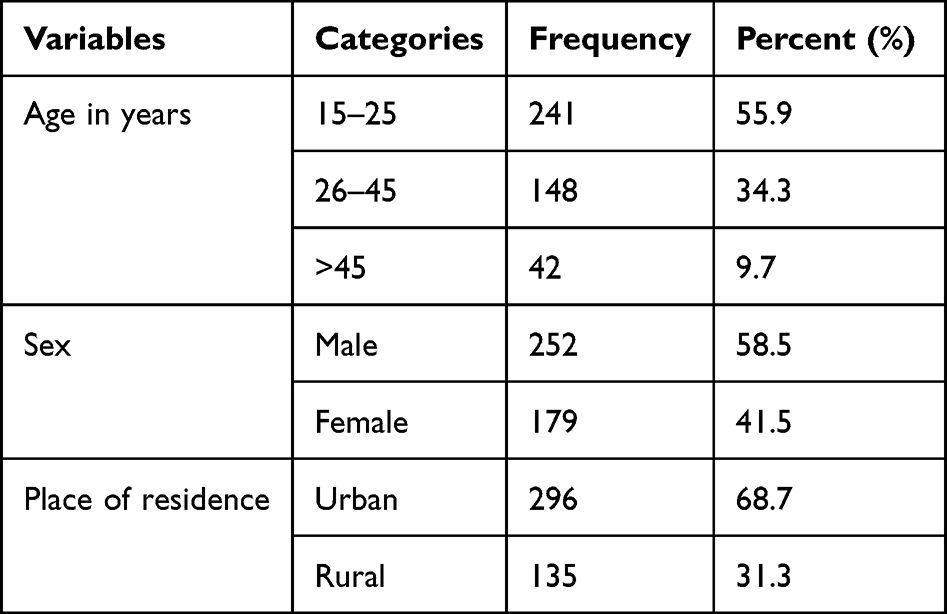 |
Table 1 Socio-Demographic Characteristics of Patients Diagnosed with Appendicitis in Adama, Ethiopia, 2021 |
Complicated Appendicitis
Out of 431 patients, 157 (36.4%) were diagnosed with CA.
Characteristics Associated with the Diagnosis of Complicated Appendicitis
After multivariable logistic regression analysis, seven variables were found to be significantly associated with the diagnosis of CA. The variables were: abdominal tenderness, RLQ abdominal mass, shock, onset to visit interval, clinical diagnosis of peritonitis, ultrasound report, and WBC count.
Respondents who had generalized abdominal tenderness and those who were clinically diagnosed with peritonitis were more than 27 times (AOR: 27.48, 95% CI: 4.03, 187.24) and about 15 times (AOR: 14.87, 95% CI: 4.05, 54.54) more likely to have CA than those who had not had abdominal tenderness and were not diagnosed with peritonitis, respectively.
Study participants who presented with RLQ abdominal mass, shock, and WBC count > 11,000 were about 8 times (AOR: 7.79, 95% CI: 2.02, 29.99), more than 10 times (AOR: 10.37, 95% CI: 3.18, 33.76), and more than 2 times (AOR: 2.16, 95% CI: 1.02, 4.61) more likely to have CA than those who presented without RLQ abdominal mass, shock, and WBC count ≤ 11,000, respectively.
Among the respondents, those who had an onset to visit interval of 8–14 days were more than 10 times (AOR: 10.45, 95% CI: 2.4, 45.52) more likely to have CA than those who had <2 days. Regarding the ultrasound reports, those with a report of acute appendicitis were 67% less likely (AOR: 0.33, 95% CI: 0.13, 0.85) and those with a report of appendiceal abscess and appendiceal masses were 5 (AOR: 5.05, 95% CI: 1.48, 17.31), and 6 (AOR: 6.04, 95% CI: 1.45, 25.14) times more likely to have CA than those without ultrasound imaging, respectively (Table 2).
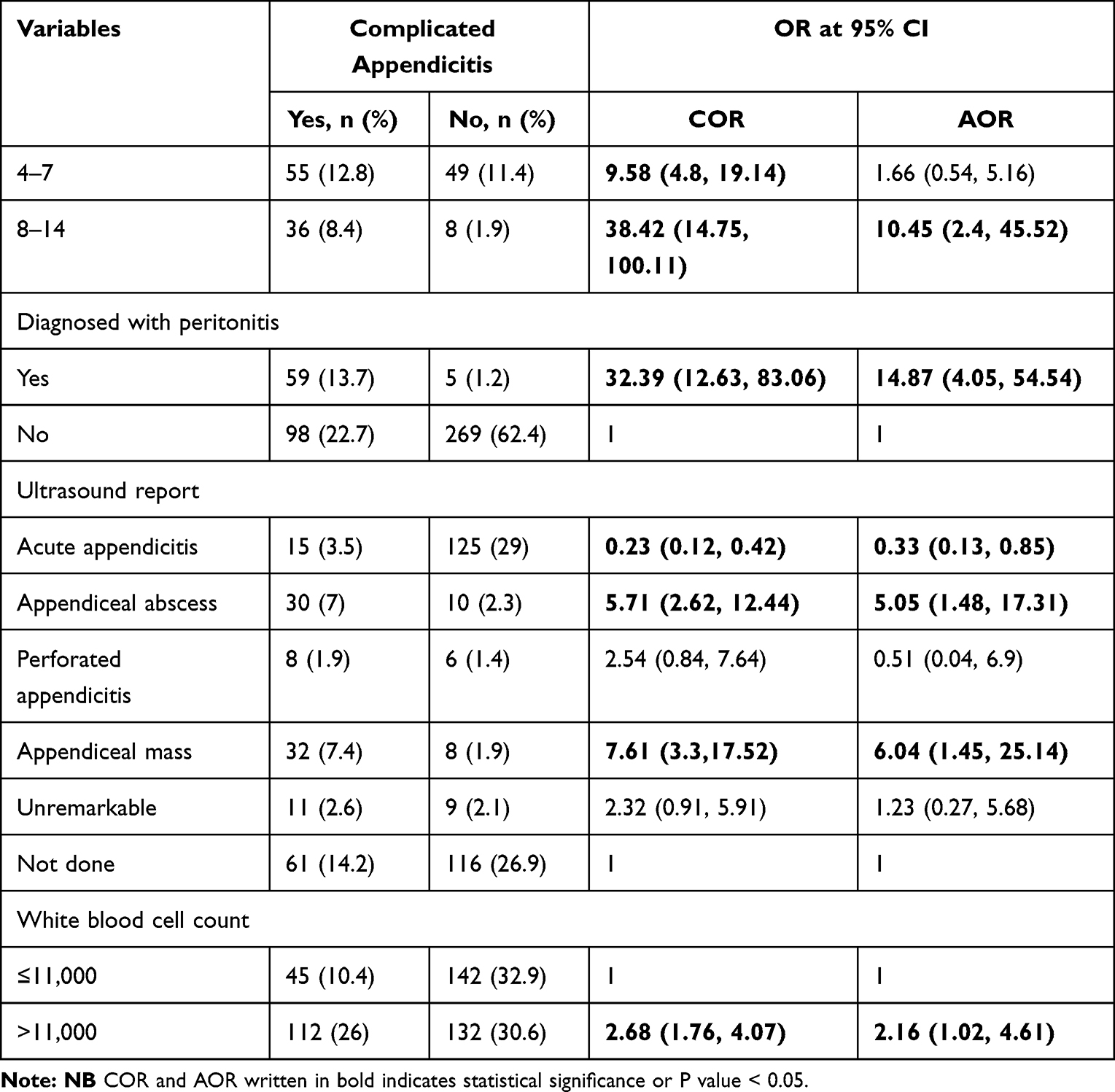 |
Table 2 Factors Associated with Complicated Appendicitis in Adama, Ethiopia, 2021 |
Discussion
Out of the respondents, 36.4% were reported to have CA. The prevalence of CA in this study was found to be higher when compared to other studies conducted in Pakistan, Japan, and India, which reported the prevalence as 20%, 16.1%, and 31.8%, respectively.16–18 Another multicenter observational study performed in 18 surgical centers also stated the prevalence of CA was 27.48%.19 The higher prevalence in our study may be attributed to the low-income status of the country. Associated with this, a delay in presentation or referral from primary health care facilities is expected to be high.
Factors associated with the presentation of CA have been inconsistently identified. The pain usually localizes to the RLQ if the perforation has been walled off by regional intra-abdominal structures, but can be diffuse if generalized peritonitis occurs.20 According to our study, respondents who had generalized abdominal tenderness and who were clinically diagnosed to have peritonitis were more likely to have CA than their counterparts. Generalized abdominal tenderness may have occurred as a result of peritonitis, which is one of the complications of perforated appendicitis.
According to our study, those who presented with shock were more likely to have CA than their counterparts. CA may be accompanied by septic shock as a result of abscess formation within the mesoappendix, which could explain the finding of this study.
In our study, participants who presented with RLQ abdominal mass were more likely to have CA than their counterparts. The possible explanation for this phenomenon could be the formation of an appendicular mass. The inflammation in acute appendicitis may sometimes be enclosed by the patient’s defense mechanisms, by the formation of an inflammatory phlegmon or a circumscribed abscess.21
Many studies have reported that an increase in WBC count has been the earliest sign of appendiceal inflammation, while increased C-reactive protein has been noted in more advanced stages of appendicitis.20 Despite this, and the same as our study, the elevation of WBC was found to be significantly associated with CA in many other studies.22–24
The results of the importance of the preoperative interval as a predictor of CA are inconsistent. Some studies show that longer durations before operation or admission are risk factors for perforation.25,26 Similarly, other studies found that the chances of CA increased 1.5 times with each additional day from the onset of symptoms,17 and also the odds of appendiceal perforation on the 8th day after admission increased to 4.7 times.27 However, another high-quality study using logistic regression showed that the preoperative interval was insignificant.28 Our data demonstrated that timing matters. An extended duration from symptom to onset was indeed found to be a risk factor for CA. Patients who had an onset to visit interval of 8–14 days were more likely to possess CA than patients who had <2 days. Duration of symptoms, a modifiable risk factor, can determine access to surgical care.
The clinical diagnosis of CA is sometimes challenging and involves a mix of clinical, laboratory, and radiological findings. Although ultrasound has a lower rate of accuracy than a contrast-enhanced CT, the findings are often appreciated in experienced hands. Diagnosis of a perforated appendix is based on the presence of a right iliac fossa abscess or phlegmon in conjunction with signs of appendiceal inflammation and appendicolith.29 According to our study, those with an ultrasound report of acute appendicitis were significantly associated with acute appendicitis, while those with appendiceal abscess and appendiceal mass reports were significantly associated with CA.
Limitations
Since the study was retrospective cross-sectional, we could not collect some previously reported important information from the patient charts.
Conclusions
Around one-third of the study, participants had CA. Patients presenting with 8–14 days of onset to visit interval, generalized abdominal tenderness, RLQ abdominal mass, raised WBC, and shock had greater odds of CA. Abdominopelvic ultrasound reports of an appendiceal abscess and an appendiceal mass are among the predicting factors for CA.
Abbreviations
AHMC, Adama Hospital Medical College; CA, Complicated Appendicitis; CT, Computed Tomography; RLQ, Right Lower Quadrant; WBC, White Blood Cell.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was conducted and designed in accordance with the Declaration of Helsinki. To conduct the study, Adama General Hospital Medical College Ethical Review Committee gave ethical clearance and waived consent to all study participants. After that, AHMC permitted the study. The study participants’ confidentiality was maintained by omitting names and personal identifications. Information obtained from their charts was not disclosed to third parties. All methods were performed per the relevant guidelines and regulations of the ethical review committee.
Acknowledgments
We would like to express our deepest gratitude to Adama Hospital Medical College for facilitating the data collection activities for this research. We would also like to extend our appreciation to the data collectors who participated in the study.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Williams NOP. Bailey & Love’s Short Practice of Surgery 26E. Crc Press; 2013.
2. Stewart B, Khanduri P, McCord C, et al. Global disease burden of conditions requiring emergency surgery. Br J Surg. 2014;101:e9–e22. doi:10.1002/bjs.9329
3. Atema JJ, van Rossem CC, Leeuwenburgh MM, et al. Scoring system to distinguish uncomplicated from complicated acute appendicitis. Br J Surg. 2015;102(8):979–990. doi:10.1002/bjs.9835
4. Perez KS, Allen SR. Complicated appendicitis and considerations for interval appendectomy. JAAPA. 2018;31(9):35–41. doi:10.1097/01.JAA.0000544304.30954.40
5. Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15:27. doi:10.1186/s13017-020-00306-3
6. Mariage M, Sabbagh C, Grelpois G, et al. Surgeon’s Definition of Complicated Appendicitis: a Prospective Video Survey Study. Eur J Hepatogastroenterol. 2019;9(1):1–4. doi:10.5005/jp-journals-10018-1286
7. Froggatt P, Harmston C. Acute appendicitis. Surgery. 2011;29(8):372–376. doi:10.1016/j.mpsur.2011.05.016
8. Poon S, Lee J. The current management of acute uncomplicated appendicitis: should there be a change in paradigm? A systematic review of the literatures and analysis of treatment performance. World J Emerg Surg. 2017;12(46). doi:10.1186/s13017-017-0157-y
9. Perez KS, Allen SR. Complicated appendicitis and considerations for interval appendectomy. JAAPA. 2018;31:35–41.
10. Lastunen K, Leppäniemi A, Mentula P. Perforation rate after a diagnosis of uncomplicated appendicitis on CT. BJS Open. 2021;5(1):zraa034. doi:10.1093/bjsopen/zraa034
11. Naderan M, Babaki A, Shoar S, et al. Risk factors for the development of complicated appendicitis in adults. Ulus Cerrahi Derg. 2016;32(1):37–42. doi:10.5152/UCD.2015.3031
12. Bratton SL, Haberkern CM, Waldhausen JH. Acute appendicitis risks of complications: age and Medicaid insurance. Pediatrics. 2000;106:75–78. doi:10.1542/peds.106.1.75
13. Moon HM, Park BS, Moon DJ. Diagnostic value of C-reactive protein in complicated appendicitis. J Korean Soc Coloproctol. 2011;27:122–126. doi:10.3393/jksc.2011.27.3.122
14. Tsukada K, Miyazaki T, Katoh H, et al. CT is useful for identifying patients with complicated appendicitis. Dig Liver Dis. 2004;36:195–198. doi:10.1016/j.dld.2003.11.026
15. Reid RI, Dobbs BR, Frizelle FA. Risk factors for post-appendectomy intra-abdominal abscess. Aust N Z J Surg. 1999;69:373–374. doi:10.1046/j.1440-1622.1999.01576.x
16. Sasaki Y, Komatsu F, Kashima N, et al. Clinical prediction of complicated appendicitis: a case-control study utilizing logistic regression. World J Clin Cases. 2020;8(11):2127–2136. doi:10.12998/wjcc.v8.i11.2127
17. Khan M, Siddiqui M, Shahzad N, et al. Factors Associated with Complicated Appendicitis: view from a Low-middle Income Country. Cureus. 2019;11(5):e4765. doi:10.7759/cureus.4765
18. Bakshi S, Mandal N. Evaluation of role of hyperbilirubinemia as a new diagnostic marker of complicated appendicitis. BMC Gastroenterol. 2021;21(1):42. doi:10.1186/s12876-021-01614-x
19. Pedziwiatr M, Lasek A, Wysocki M, et al. Complicated appendicitis: risk factors and outcomes of laparoscopic appendectomy – polish laparoscopic appendectomy results from a multicenter, large-cohort study. Ulus Travma Acil Cerrahi Derg. 2019;25(2):129–136. doi:10.5505/tjtes.2018.80103
20. Mekakas A, Nagorni E, Tablaridis T. Complicated Appendicitis: a Surgical Controversy Concerning Risk Factors, Diagnostic Algorithm and Therapeutic Management. In Doubts, Problems and Certainties about Acute Appendicitis. IntechOpen. 2021.
21. Tannoury J, Abboud B. Treatment options of inflammatory appendiceal masses in adults. World J Gastroenterol. 2013;19(25):3942–3950. doi:10.3748/wjg.v19.i25.3942
22. Horattas M, Guyton D, Diane W. A reappraisal of appendicitis in the elderly. Am J Surg. 1990;160:291–293. doi:10.1016/S0002-9610(06)80026-7
23. Storm-Dickerson T, Horattas M. What we have learned over the past 20 years about appendicitis in the elderly? Am J Surg. 2003;185(3):198–201. doi:10.1016/S0002-9610(02)01390-9
24. Sheu B, Chiu T, Chen J, et al. Risk factors associated with perforated appendicitis in elderly patients presenting with signs and symptoms of acute appendicitis. ANZ J Surg. 2007;77(8):662–666. doi:10.1111/j.1445-2197.2007.04182.x
25. Sirikurnpiboon S, Amornpornchareon S. Factors Associated with Perforated Appendicitis in Elderly Patients in a Tertiary Care Hospital. Surg Res Pract. 2015;2015:847681. doi:10.1155/2015/847681
26. Omari A, Khammash M, Qasaimeh G, et al. Acute appendicitis in the elderly: risk factors for perforation. World J Eme Surg. 2014;9(6). doi:10.1186/1749-7922-9-6
27. Papandria D, Goldstein S, Rhee D, et al. Risk of perforation increases with delay in recognition and surgery for acute appendicitis. J Surg Res. 2013;184(2):723–729. doi:10.1016/j.jss.2012.12.008
28. Drake F, Mottey N, Farrokhi E, et al. Time to Appendectomy and Risk of Perforation in Acute Appendicitis. JAMA Surg. 2014;149(8):837–844. doi:10.1001/jamasurg.2014.77
29. Jones J, Hartung M Radiopaedia.org; 2009. Available from: https://radiopaedia.org/articles/6233.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.