Back to Journals » Clinical Ophthalmology » Volume 12
Characteristics of diabetic macular edema on optical coherence tomography may change over time or after treatment
Authors Sheu SJ ![]() , Lee YY, Horng YH, Lin HS, Lai WY, Tsen CL
, Lee YY, Horng YH, Lin HS, Lai WY, Tsen CL
Received 14 May 2018
Accepted for publication 11 July 2018
Published 26 September 2018 Volume 2018:12 Pages 1887—1893
DOI https://doi.org/10.2147/OPTH.S173956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Shwu-Jiuan Sheu,1,2 Ying-Yen Lee,1 Yu-Harn Horng,1 Huey-Shyan Lin,3 Wei-Yu Lai,1 Chui-Lien Tsen1
1Department of Ophthalmology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 2Department of Ophthalmology, School of Medicine, National Yang-Ming University, Taipei, Taiwan; 3Department of Health-Business Administration, Fooyin University, Kaohsiung, Taiwan
Purpose: To investigate optical coherence tomography (OCT) characteristics in diabetic macular edema (DME) over time and after treatment.
Patients and methods: OCT morphological features in DME eyes treated with ranibizumab with at least 1 year of follow-up were retrospectively analyzed.
Results: Thirty-five eyes were included. From baseline to Month 12, mean visual gain was 7.2±13.6 letters and mean central retinal thickness reduction was 61.9±121.8 µm. Fovea-involving ellipsoid zone (EZ) disruption was significantly associated with final vision of <70 letters. Subretinal fluid at baseline was present only in eyes naïve to previous intravitreal pharmacotherapy and was related to better visual gain and fewer injections. Treatment-naïve eyes had shorter DME duration and less EZ damage.
Conclusion: DME characteristics on OCT may change over time or after treatment. Subretinal fluid may be associated with earlier change and less EZ damage in DME.
Keywords: diabetic macular edema, optical coherence tomography, OCT, subretinal fluid, SRF, vascular endothelial growth factor, VEGF
Introduction
Since the introduction of optical coherence tomography (OCT), it has become the most frequently used tool in the diagnosis and monitoring of many retinal diseases, including diabetic macular edema (DME). Although central retinal thickness (CRT) has been used to guide DME treatment and has served as the secondary efficacy endpoint in the majority of clinical trials related to DME, increasing evidence suggests that the morphological features of OCT are related to treatment course and response.1–8 Furthermore, OCT biomarkers have been considered to be key identifiers in individualized pro re nata treatment regimens. However, patients recruited in clinical trials are typically treatment naïve; therefore, the findings are not fully applicable to real-world clinical practice. The purpose of this study was to investigate whether the characteristics of OCT change over time or with treatment in DME in real-world practice.
Patients and methods
A retrospective chart review of adult patients with type 2 diabetes mellitus and DME treated with ranibizumab according to the reimbursement policy of the Taiwan National Health Insurance in a single medical center from February 1, 2013 to December 31, 2014 was conducted. The reimbursement criteria were baseline best-corrected visual acuity of 3/60 to 6/12, presence of center-involved DME, CRT ≥300 μm on OCT and HbA1c ≦10%. The institutional review board and ethics committee of Kaohsiung Veterans General Hospital approved this study, which adhered to the tenets of the Declaration of Helsinki. Since this research was retrospective, using already existing information, patient’s informed consent was not needed. All the patients were recorded with a number code without leakage of any personal information. Eyes with previous vitrectomy were excluded due to possible different drug bioavailability. Patients with <1 year of follow-up data were excluded. Of note, due to the required three-step reimbursement application with limit of maximum eight injections per eye for ranibizumab, patients were treated mostly on a pro re nata basis, leading to loss of follow-up in many patients who did not obtain the second approval. Data related to demographic characteristics, medical history, date of DME diagnosis, comorbidities, initial and final visual acuity (VA), slit-lamp biomicroscopy, intraocular pressure, fundus photography, fundus fluorescein angiography, CRT and optical characteristics according to OCT, and treatment were analyzed. Morphological features of OCT were identified as cystoid macular edema (CME), diffuse retinal thickening (DRT), subretinal fluid (SRF) and presence of epiretinal membrane involving the fovea. Ellipsoid zone (EZ) integrity was scored in a 3 mm scan into four grades (0–3), with “0” representing intact EZ, “1” representing partial disruption with weak reflectivity band, “2” representing loss at fovea but present elsewhere in the scan and “3” representing severe disruption with loss of signal along the entire scan.
Statistical analysis was performed using SPSS Version 12.0 (SPSS Inc., Chicago, IL, USA). Snellen VA measurements were converted to approximate Early Treatment Diabetic Retinopathy Study letter scores for statistical manipulations according to the methods described previously.9 Descriptive statistics are expressed as mean with SD. Paired t-test was performed to evaluate the mean changes from baseline to endpoints. If a variable was not with a normal distribution, the Wilcoxon signed-rank test was adopted to compare the variable between two groups. A P-value of <0.05 was considered statistically significant. To understand the substantive clinical significance, effect size value (d) was calculated according to the methods described previously.10 The denominator standardized the difference by transforming the absolute difference into SD units. The effect size was classified as small (0.2≦d<0.5), medium (0.5≦d<0.8) and large (d≥0.8).
Results
A total of 35 eyes of 26 patients, including 6 women and 20 men, were included. Mean age was 60.62±7.28 years. Mean duration of DME was 22.11±23.71 months (range, 1–121). Nine eyes had history of DME-related anti-vascular endothelial growth factor (anti-VEGF) treatment. The interval from previous treatment was at least 3 months. Due to the reimbursement limitations, most patients were undertreated with a mean number of 4.43±2.05 injections over 12 months (range, 1–11). VA improved from 48.34±16.97 letters to 55.51±14.81 letters with a mean gain of 7.2±13.6 letters from baseline at Month 12. CRT was reduced from 399.83±97.35 to 337.89±130.5 μm with a mean reduction of 61.9±121.8 μm from baseline to Month 12.
More eyes with lower baseline VA had significant visual gain at Week 12 (Table 1). More eyes with higher baseline VA had final vision of ≥70 letters, though it was not significant (Table 2). None of the previously treated eyes had final vision of ≥70 letters. Patients with better response seemed to have fewer injections over 1 year, though the difference was not significant (Table 2).
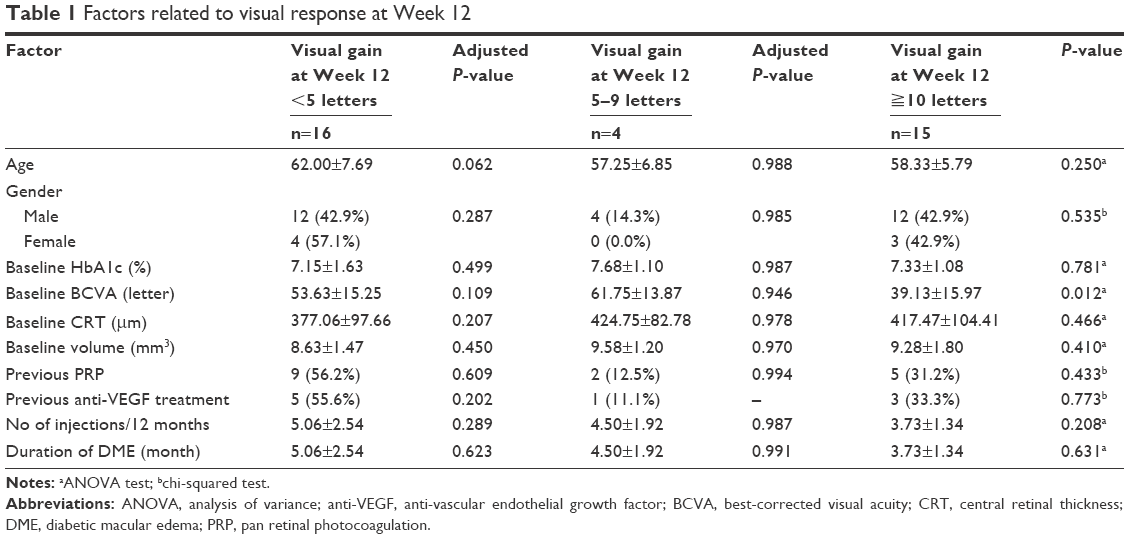 | Table 1 Factors related to visual response at Week 12 |
 | Table 2 Factors related to visual response at Month 12 |
Of the different morphological features of OCT at baseline, none were significantly associated with visual gain of <10 letters or final vision of <70 letters at Month 12, with the exception of EZ disruption score >1 (fovea involved). Fovea-involving EZ disruption was significantly associated with final visual outcome of <70 letters at Month 12 (Table 3). Compared to previously treated eyes, treatment-naïve eyes had shorter duration of DME and fewer had fovea-involving EZ disruption (Table 4). At baseline, SRF was present only in treatment-naïve eyes (Table 4). In eyes previously treated with panretinal photocoagulation, the proportion of eyes with SRF was similar to that of eyes with no previous treatment. In eyes with SRF at baseline, SRF disappeared rapidly after intravitreal ranibizumab treatment and recurred after a period of treatment discontinuation. The recurrence of SRF occurred mostly in treatment-naïve eyes. In one eye that was previously treated with intravitreal injection and macular and panretinal photocoagulation, SRF was not present at baseline but appeared during follow-up (Table 5). Compared to eyes without SRF, eyes with SRF at baseline were significantly more likely to be treatment naïve and have a shorter duration of DME. Although there was no statistically significant difference in visual gain at Week 12 or Month 12 or in the number of injections over 1 year between eyes with or without SRF at baseline, the effect size value revealed that eyes with SRF at baseline had higher probability of more visual gain at Week 12 (d=0.69) and Month 12 (d=0.66). Moreover, fewer injections were administered over 12 months in eyes with SRF at baseline compared to those without (d=0.34), as shown in Table 6. Besides, the effect size analysis showed EZ integrity had more impact on the baseline and final vision, but less impact on visual gain (Table 7).
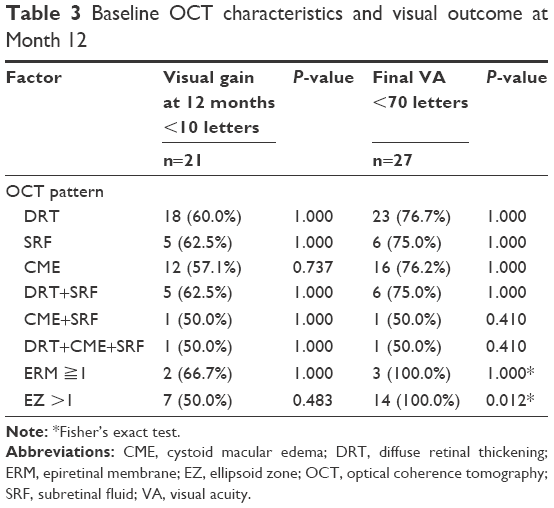 | Table 3 Baseline OCT characteristics and visual outcome at Month 12 |
 | Table 4 Baseline OCT characteristics and duration of DME in naïve vs non-naïve eyes |
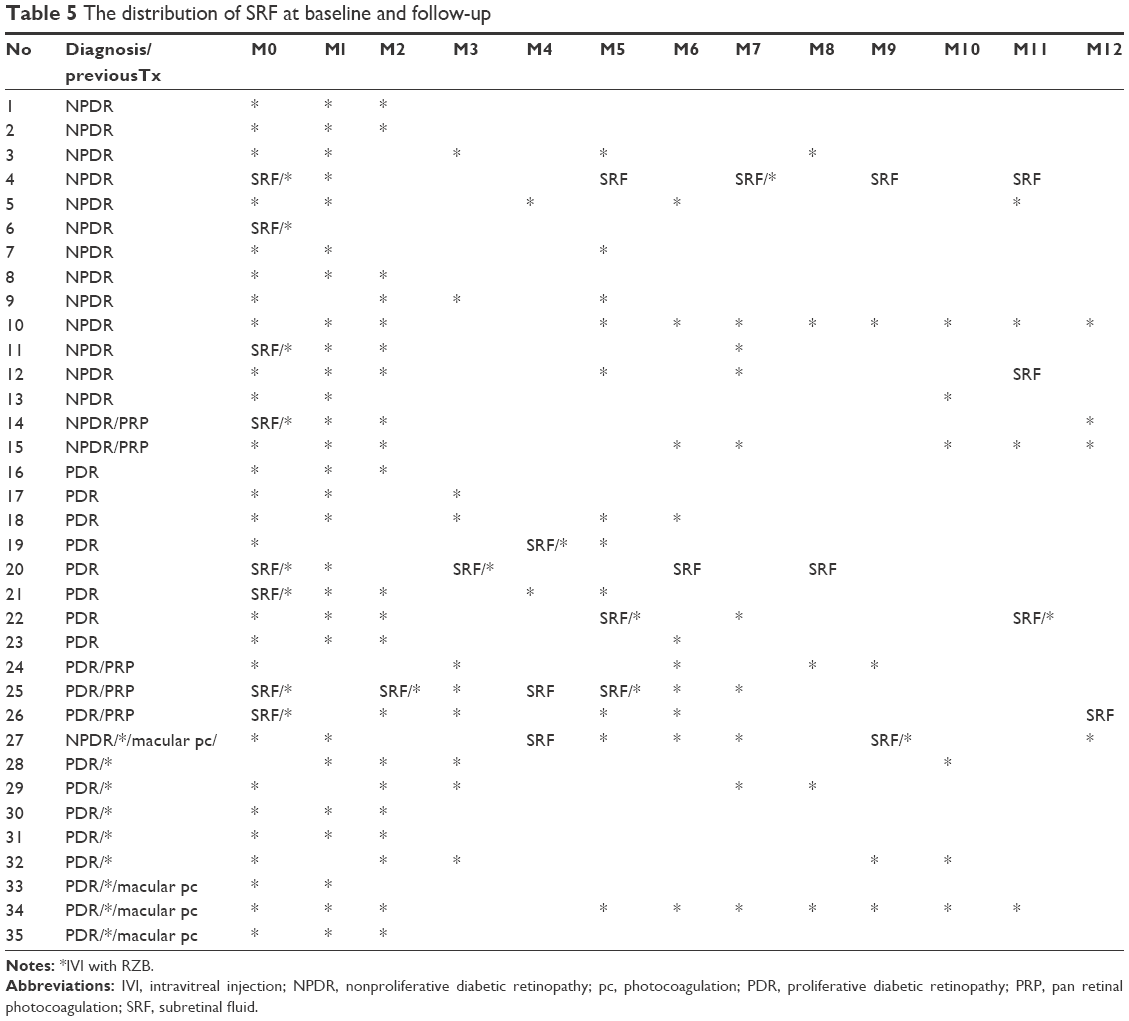 | Table 5 The distribution of SRF at baseline and follow-up |
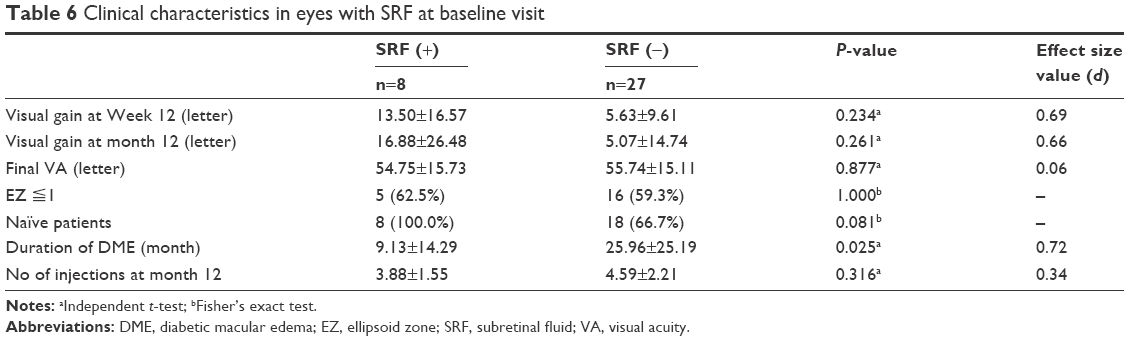 | Table 6 Clinical characteristics in eyes with SRF at baseline visit |
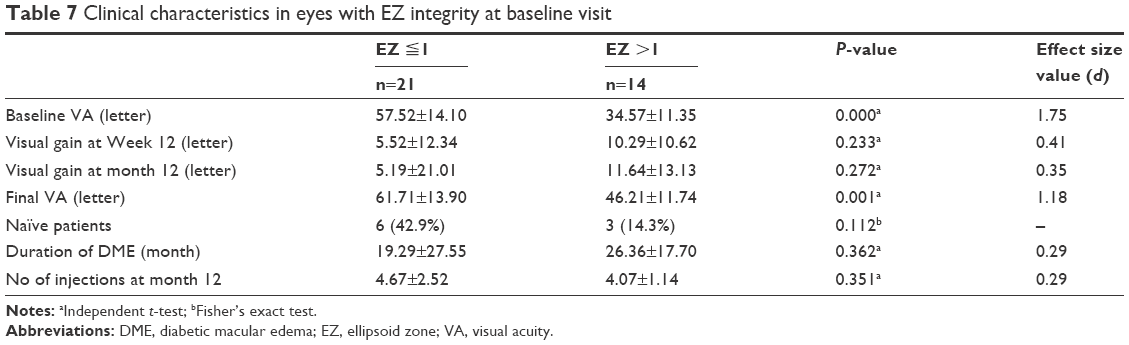 | Table 7 Clinical characteristics in eyes with EZ integrity at baseline visit |
Discussion
Study results showed a beneficial effect from ranibizumab in DME eyes with or without previous treatment, as well as in eyes with longer DME duration. Overall, mean VA gain was 7.2±13.6 letters and mean CRT reduction was 61.9±121.8 μm after a mean of 4.43±2.05 injections over 12 months. Presence of fovea-involving EZ disruption was significantly associated with final visual outcome of <70 letters at Month 12. At baseline, SRF was present only in treatment-naïve eyes, which had shorter duration of DME and less fovea-involving EZ damage compared to previously treated eyes. Eyes with SRF at baseline tended to be more likely treatment naïve and have shorter DME duration, more visual gain at Week 12 and Month 12 from baseline, as well as fewer injections over 1 year.
Compared to our previous prospective interventional study conducted at the same hospital, in this study, more patients were undertreated due to resource limitations in real-world practice, resulting in poorer visual outcome.11 Studies conducted in different regions of the world have similarly reported that DME treatment in real-world settings are less intensive than treatment administered in trial settings.12,13
The pathogenesis of DME is complicated and involves not only vascular endothelial growth factor (VEGF) but also inflammatory cytokines and vitreoretinal interface abnormality.14 Anti-VEGF agents are currently considered as appropriate first-line treatment for center-involved DME; however, certain degrees of macular edema persist even under the treatment protocol of controlled trials.15 These findings support the hypothesis that in eyes with poor response, underlying mechanisms of pathogenesis other than VEGF may be involved. It is also possible that patients who are anti-VEGF non-responders were included in this study, which may account for the trend of poorer response to treatment in this series.
Accumulation of SRF typically arises from disruption of retinal pigment epithelium tight junctions or its protective function, whereas CME arises from compromised tight junctions in the retinal vasculature and Muller cell disturbances which affect water and potassium channels.16,17 Although there is currently no consensus, several morphological features of OCT have been identified as possible biomarkers in DME, including SRF, CME, DRT, disorganization of retinal inner layer, status of vitreomacular interface, hyperreflective foci and changes in the integrity of the inner and outer photoreceptor segment border.18–22 In the RESTORE study, eyes with SRF at baseline had greater visual gain at the end of the first study year than those without SRF at baseline, though there was no significant difference in VA at baseline between groups.7 The protective role of SRF was further confirmed by a post hoc analysis of the RIDE/RISE studies.23 Results of a post hoc analysis of the RESTORE/RESTORE-extension studies also showed a trend of positive impact from SRF on response to ranibizumab therapy and a negative impact on response to laser therapy.24 Furthermore, eyes with SRF were reported to have better visual outcome in a study evaluating the effectiveness of vitrectomy for diffuse DME.25 In a recent observational cohort study on the functional outcome of DME treated by dexamethasone implant, submacular fluid was predictive of better visual outcome.26 However, a prospective study including 55 eyes with DME found that disruption of photoreceptor integrity at baseline correlated with poorer visual outcome and occurred more frequently in eyes with serous retinal detachment (SRD). The discrepancy may be due to the definition of SRD used in the study, which included eyes with DRT, CME and SRD together.27 Our results showed that the absence of fovea-involving EZ disruption predicts better final vision, and that the presence of SRF at baseline predicts more VA gain and fewer injections over 1 year. Moreover, changes in OCT parameters were observed in chronic and previously treated cases. As expected, previously treated eyes tended to have longer duration of DME and more fovea-involving EZ disruption. Baseline SRF presented only in treatment-naïve eyes in our series. SRF resolved rapidly after anti-VEGF treatment, but reappeared if treatment was discontinued for a period of time. According to these findings, SRF may be an indicator of earlier stage DME that would respond well to intravitreal anti-VEGF therapy. Improved visual gain may also be related to earlier intervention and possibly attributable to some eyes being good responders to anti-VEGF treatment.
This study was limited by the small sample size and lack of adequate treatment in the majority of the cases. Partial treatment as compared with treatment administered in trial settings, however, better reflects real-world conditions of DME treatment.
Conclusion
Our study showed that the characteristics of DME on OCT may change over time or after treatment. Presence of SRF in eyes with DME may indicate earlier change and lesser degree of EZ damage, and thus, may predict better outcome.
Disclosure
The authors report no conflicts of interest in this work.
References
Massin P, Bandello F, Garweg JG, et al. Safety and efficacy of ranibizumab in diabetic macular edema (RESOLVE Study): a 12-month, randomized, controlled, double-masked, multicenter Phase II study. Diabetes Care. 2010;33(11):2399–2405. | ||
Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011;118(4):615–625. | ||
Elman MJ, Bressler NM, Qin H, et al. Diabetic Retinopathy Clinical Research Network: expanded 2-year follow-up of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2011;118:609–614. | ||
Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema: results from 2 Phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119(4):789–801. | ||
Brown DM, Schmidt-Erfurth U, Do DV, et al. Intravitreal aflibercept for diabetic macular edema: 100-week results from the VISTA and VIVID studies. Ophthalmology. 2015;122(10):2044–2052. | ||
Wells JA, Glassman AR, Ayala AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology. 2016;123(6):1351–1359. | ||
Gerendas B, Simader C, Deak GG, et al. Morphological parameters relevant for visual and anatomic outcomes during anti-VEGF therapy of diabetic macular edema in the RESTORE trial. Invest Ophthalmol Vis Sci. 2014;55(13):1791–1791. | ||
Gerendas BS, Prager SG, Deak GG, et al. Morphological parameters relevant for long-term outcomes during therapy of diabetic macular edema in the RESTORE Extension trial. Invest Ophthalmol Vis Sci. 2015;56(7):4686–4686. | ||
Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30(7):1046–1050. | ||
Cohen. Statistical Power Analysis for the Behavioral Science. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. | ||
Sheu SJ, Lee YY. Early response to ranibizumab is associated with 12-month outcome in diabetic macular edema after prior macular laser therapy. Ophthalmologica. 2017;238(3):139–146. | ||
Wecker T, Ehlken C, Bühler A, et al. Five-year visual acuity outcomes and injection patterns in patients with pro-re-nata treatments for AMD, DME, RVO and myopic CNV. Br J Ophthalmol. 2017;101(3):353–359. | ||
Egan C, Zhu H, Lee A, et al. The United Kingdom Diabetic Retinopathy Electronic Medical Record Users Group, Report 1: baseline characteristics and visual acuity outcomes in eyes treated with intravitreal injections of ranibizumab for diabetic macular oedema. Br J Ophthalmol. 2017;101(1):75–80. | ||
Romero-Aroca P, Baget-Bernaldiz M, Pareja-Rios A, Lopez-Galvez M, Navarro-Gil R, Verges R. Diabetic macular edema pathophysiology: vasogenic versus inflammatory. J Diabetes Res. 2016;2016:2156273. | ||
Bressler SB, Ayala AR, Bressler NM, et al. Diabetic Retinopathy Clinical Research Network: persistent macular thickening after ranibizumab treatment for diabetic macular edema with vision impairment. JAMA Ophthalmol. 2016;134:278–285. | ||
Johnson MW. Etiology and treatment of macular edema. Am J Ophthalmol. 2009;147(1):11–21. | ||
Spaide RF. Retinal vascular cystoid macular edema: review and new theory. Retina. 2016;36(10):1823–1842. | ||
Pelosini L, Hull CC, Boyce JF, Mchugh D, Stanford MR, Marshall J. Optical coherence tomography may be used to predict visual acuity in patients with macular edema. Invest Ophthalmol Vis Sci. 2011;52(5):2741–2748. | ||
Shin HJ, Lee SH, Chung H, Kim HC. Association between photoreceptor integrity and visual outcome in diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2012;250(1):61–70. | ||
Shen Y, Liu K, Xu X. Correlation between visual function and photoreceptor integrity in diabetic macular edema: spectral-domain optical coherence tomography. Curr Eye Res. 2016;41(3):391–399. | ||
Sun JK, Radwan SH, Soliman AZ, et al. Neural retinal disorganization as a robust marker of visual acuity in current and resolved diabetic macular edema. Diabetes. 2015;64(7):2560–2570. | ||
Itoh Y, Petkovsek D, Kaiser PK, Singh RP, Ehlers JP. Optical coherence tomography features in diabetic macular edema and the impact on anti-VEGF response. Ophthalmic Surg Lasers Imaging Retina. 2016;47(10):908–913. | ||
Sophie R, Lu N, Campochiaro PA. Predictors of functional and anatomic outcomes in patients with diabetic macular edema treated with ranibizumab. Ophthalmology. 2015;122(7):1395–1401. | ||
Gerendas BS, Prager S, Deak G, et al. Predictive imaging biomarkers relevant for functional and anatomical outcomes during ranibizumab therapy of diabetic macular oedema. Br J Ophthalmol. 2018;102(2):195–203. | ||
Ichiyama Y, Sawada O, Mori T, et al. The effectiveness of vitrectomy for diffuse diabetic macular edema may depend on its preoperative optical coherence tomography pattern. Graefes Arch Clin Exp Ophthalmol. 2016;254(8):1545–1551. | ||
Zur D, Iglicki M, Busch C, et al. OCT biomarkers as functional outcome predictors in diabetic macular edema treated with dexamethasone implant. Ophthalmology. 2018;125(2):267–275. | ||
Seo KH, Yu SY, Kim M, Kwak HW. Visual and morphologic outcomes of intravitreal ranibizumab for diabetic macular edema based on optical coherence tomography patterns. Retina. 2016;36(3):588–595. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.