Back to Journals » Clinical Optometry » Volume 18
Changes in Corneal Epithelial Thickness and Tear Film Stability After Carboxymethyl Cellulose Use in Young Adults with High Screen Time Exposure
Authors Belbase U ![]() , Khanal P
, Khanal P ![]() , Subedi A
, Subedi A ![]() , Chhetri S
, Chhetri S ![]() , Sah PP, Parajuli A
, Sah PP, Parajuli A ![]()
Received 29 November 2025
Accepted for publication 14 February 2026
Published 19 February 2026 Volume 2026:18 585390
DOI https://doi.org/10.2147/OPTO.S585390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Chris Lievens
Umesh Belbase,1,* Prastuti Khanal,1,* Anup Subedi,1 Santosh Chhetri,2 Punay Pratap Sah,1 Anil Parajuli3
1Department of Optometry, Himalaya Eye Hospital, Pokhara University, Pokhara, Nepal; 2Department of Optometry and Ophthalmology, Metro Eye Care Lumbini, Butwal, Nepal; 3Department of Ophthalmology, Himalaya Eye Hospital, Pokhara, Nepal
*These authors contributed equally to this work
Correspondence: Prastuti Khanal, Department of Optometry, Himalaya Eye Hospital, Pokhara University, Pokhara, Nepal, Email [email protected]
Background: Dry eye disease (DED) is increasingly prevalent among young adults, largely driven by prolonged digital screen exposure. This study evaluated changes in ocular surface–related parameters following carboxymethyl cellulose (CMC) use in a young population with high digital screen exposure and explored baseline factors associated with anatomical change.
Methods: This prospective, single-arm interventional study enrolled 76 patients (120 eyes) aged 20– 40 years with symptomatic DED and high screen time. Participants used preservative-free 0.5% CMC artificial tears four times daily for one month. Primary outcome was the change in central corneal epithelial thickness (CET) measured by Fourier-domain optical coherence tomography (OCT). Secondary outcomes included changes in non-invasive tear break-up time (NIBUT), central corneal thickness (CCT), and an analysis of predictors of anatomical improvement.
Results: One month of CMC treatment was associated with the statistically significant increase in central CET (from 52.79 ± 2.86 μm to 53.65 ± 2.92 μm; Δ = +0.86 μm, p < 0.001), with significant thickening observed across all corneal zones. Tear film stability also improved significantly, with NIBUT increasing from 6.52 ± 2.14 seconds to 7.89 ± 3.13 seconds (Δ = +1.37 seconds, p < 0.001). A strong negative correlation was found between daily screen time and baseline NIBUT (r = − 0.72, p < 0.001). Binary logistic regression identified that older age within the cohort was a significant predictor of a positive anatomical response to treatment (adjusted OR = 1.15, p = 0.013).
Conclusion: In young adults with screen-time-associated DED, one month of CMC may be associated with changes in corneal epithelial thickness and tear film stability. The strong correlation with screen time underscores its role as a key risk factor.
Keywords: dry eye disease, carboxymethyl cellulose, corneal epithelial thickness, digital screen time, optical coherence tomography
Introduction
Dry eye disease (DED) is a pervasive and multifactorial disorder of the ocular surface, representing one of the most common reasons patients seek ophthalmological care worldwide.1 Its pathology is characterized by a vicious cycle of tear film instability, hyperosmolarity, and ocular surface inflammation, leading to symptoms of discomfort, visual disturbance, and a significant reduction in quality of life.2 The global prevalence of DED is substantial, with recent meta-analyses estimating it affects over 11% of the global population, with rates soaring to over 20% in Asian cohorts.3 While historically associated with aging, a modern epidemic of DED is emerging among a younger demographic, driven largely by pervasive digital device use.4,5 This shift necessitates a renewed focus on understanding and managing the disease in this specific population, particularly in regions with high digital adoption and environmental risk factors.
Maintaining the corneal epithelium is crucial for ocular surface health, as it serves as the primary barrier protecting the eye from external environmental factors. In DED, the combination of an inflammatory environment and abnormal blinking patterns such as those induced by prolonged screen use leads to mechanical stress, disrupting the normal balance and function of the corneal epithelium.6 These alterations are not merely symptomatic; they manifest as measurable changes in the corneal epithelial structure. Fourier-domain optical coherence tomography (OCT) now allows for the precise, non-invasive, and high-resolution measurement of corneal epithelial thickness (CET), providing an objective biomarker for ocular surface health.7 Emerging evidence suggests that CET alterations are a sensitive indicator of early epithelial stress in DED, with thinning often observed in chronic, severe cases, while subclinical thickening may represent an adaptive response to hyperosmolar and inflammatory insult in earlier stages.8,9 CET serves not only as a diagnostic marker but also as a potential metric for monitoring therapeutic response, though its clinical interpretation in young, digitally exposed populations remains underexplored.
The mainstay of DED management, artificial tears, aims to break the pathological cycle by supplementing the tear film and stabilizing the ocular surface. Among various formulations, carboxymethyl cellulose (CMC) is widely prescribed for its mucoadhesive properties and prolonged retention time.10 Beyond its lubricating function, emerging evidence from in vitro and animal models suggests CMC may play an active role in promoting wound healing by facilitating corneal epithelial cell adhesion and migration.11 This implies a potential restorative mechanism beyond mere palliation, though clinical translation in young symptomatic populations with screen-associated dry eye remains limited.
Significantly, the advent of anterior segment OCT has revealed that DED is associated with measurable alterations in CET, though reported findings have been paradoxical, showing both thinning and thickening in different studies.8,12 This discrepancy highlights the complexity of the disease and the influence of factors like disease subtype, severity, and duration. While several studies have utilized OCT to document changes in corneal parameters following artificial tear instillation,13 the literature remains largely descriptive, confirming change without identifying which patients are most likely to benefit.
Crucially, there remains a paucity of evidence investigating whether pre-treatment characteristics—such as baseline epithelial morphology, demographic factors, or lifestyle habits like digital screen time—can predict a patient’s response to therapy. This represents a significant gap in the journey towards personalized medicine in ophthalmology. Furthermore, no such study has been conducted within the specific context of a young, digitally intensive Nepalese population, a cohort particularly vulnerable to modern DED risk factors yet underrepresented in clinical studies.
Therefore, this study was designed to observe anatomical and functional changes following CMC use. We aimed to examine OCT parameters that may be associated with treatment-related changes. Our primary objective was to determine the effect of CMC artificial tears on corneal epithelial thickness in patients with digital device-associated dry eye. Our secondary objectives were to identify baseline factors that predict treatment response and to evaluate the association between anatomical change and functional improvement. By doing so, we seek to contribute to a more personalized and effective treatment paradigm for dry eye disease in the digital age.
Methods
This prospective, interventional, single-arm study was conducted at the Himalaya Eye Hospital, Pokhara, Nepal. The study protocol received approval from the Institutional Review Board of Pokhara University (Approval No: 106-2079/80) and was performed in accordance with the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment.
Consecutive patients aged 20–40 years presenting with symptoms of ocular irritation, dryness, or visual fatigue were screened for eligibility. Inclusion criteria required an Ocular Surface Disease Index (OSDI) score >20 (indicating moderate-to-severe symptoms),14 a non-invasive tear break-up time (NIBUT) <10 seconds,14 and no use of artificial tears in the preceding three months.8 Exclusion criteria included active ocular disease (including any corneal or ocular surface pathology affecting topography), history of ocular surgery or trauma, regular contact lens wear, systemic diseases associated with dry eye (eg, Sjögren’s syndrome, rheumatoid arthritis), and use of medications that affect tear production (eg, antihistamines, antidepressants).
The sample size was estimated to detect a 3 µm change in corneal epithelial thickness (CET), a threshold previously reported as meaningful in OCT-based dry eye studies.13 Assuming a standard deviation of 5 µm, 80% power, and a two-sided alpha of 0.05, a minimum of 65 eyes was required. Because both eyes were included, linear mixed-effects models were used to account for inter-eye correlation. As the observed CET change was smaller than initially assumed, findings should be interpreted as exploratory rather than confirmatory.
All assessments were performed by a single optometrist between 9:00 AM and 12:00 PM to minimize diurnal variation. Tear film stability was measured with the CA-800 Corneal Analyzer (Topcon Corporation, Tokyo, Japan; software version 1.04.02), averaging three consecutive NIBUT readings.15 High-resolution imaging was obtained using Fourier-Domain Optical Coherence Tomography (RTvue XR Avanti, Optovue, Fremont, CA, USA; software version 2018.1.0.43) with an anterior segment module (CAM, CAM-L adapter). A superluminescent diode laser (840 nm, 5 μm axial resolution) acquired 8 radial B-scans (6.0 mm, 1024 A-scans each) centered on the corneal vertex.16 Participants were advised to avoid artificial tear instillation immediately before the visit; however, variability in timing may still have contributed to transient hydration effects. Participants blinked completely before acquisition to ensure tear film uniformity. The software generated epithelial and total corneal thickness maps, and mean central 2-mm zone values were recorded.
Eligible participants were prescribed preservative-free carboxymethyl cellulose 0.5% ophthalmic solution (Refresh Tears PF®, AbbVie Inc.), instilled as one drop in each eye four times daily for one month. All participants received standardized training on drop instillation technique. Compliance was monitored using patient-maintained diaries and gravimetric analysis of returned bottles, with adherence defined as ≥80% of prescribed doses. After one month, baseline assessments were repeated using identical protocols and equipment settings. The examiner was masked to baseline data at follow-up to minimize bias. The primary outcome was change in CET within the central 2-mm zone. Secondary outcomes included changes in central corneal thickness (CCT) and NIBUT and an analysis of predictors of anatomical improvement.
The primary analysis was conducted using linear mixed-effects models with a random intercept for each participant to account for inter-eye correlation. This approach was selected because it appropriately handles clustered data when both eyes contribute observations. Time (pre- vs post-intervention) was included as a fixed effect, and baseline covariates were added where relevant.
Paired t-tests were performed only as secondary sensitivity analyses to confirm the direction and magnitude of changes identified by the mixed-effects models and were not used for inferential interpretation.
Model assumptions, including normality of residuals and homoscedasticity, were verified and met. Statistical significance was defined as a two-tailed p-value < 0.05.
Results
A total of 76 patients (120 eyes) completed the one-month study protocol. The cohort had a mean age of 28.80 ± 6.30 years with a female predominance (71.1%). Students (47.4%) and housewives (42.1%) constituted the majority of participants, reflecting a population with substantial digital device exposure. This was corroborated by a self-reported mean daily screen time of 6.30 ± 3.30 hours. Baseline clinical assessment confirmed a dry eye phenotype, characterized by a mean non-invasive tear break-up time (NIBUT) of 6.52 ± 2.14 seconds. The mean central corneal thickness (CCT) was 512.95 ± 29.41 µm, and the mean central CET was 52.79 ± 2.84 µm (Table 1).
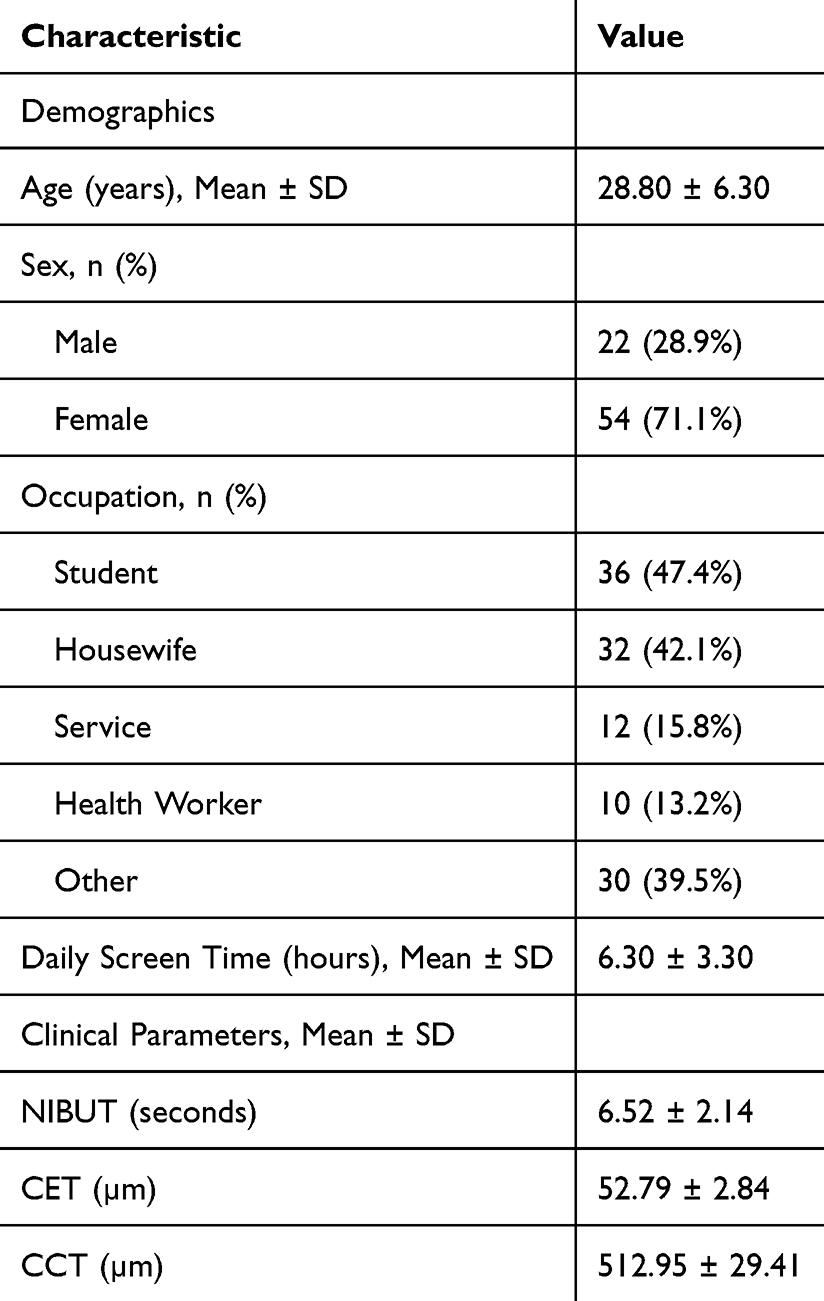 |
Table 1 Baseline Demographics and Clinical Characteristics of the Study Cohort (N=76 Patients, 120 Eyes) |
Effect of Intervention on Ocular Surface Parameters
One month of preservative-free carboxymethyl cellulose use was associated with significant changes in objective ocular surface parameters.
Tear film stability, as measured by NIBUT, improved significantly from 6.52 ± 2.14 seconds to 7.89 ± 3.13 seconds (mean difference Δ = +1.37 seconds; 95% CI [0.69, 2.04]; p < 0.001).
The primary outcome, central corneal epithelial thickness (CET), demonstrated a statistically significant increase from 52.79 ± 2.86 µm to 53.65 ± 2.92 µm (Δ = +0.86 µm; 95% CI [0.61, 1.12]; p < 0.001). This pattern of significant epithelial thickening was consistent across all measured corneal zones, including the minimum (Δ = +0.93 µm, p < 0.001), maximum (Δ = +0.81 µm, p < 0.001), superior (Δ = +0.97 µm, p < 0.001), and inferior regions (Δ = +0.61 µm, p < 0.001) (Table 2). Although these changes reached statistical significance, the absolute magnitude of thickening (<1 µm) is small and should be interpreted cautiously in the context of known epithelial mapping measurement variability.
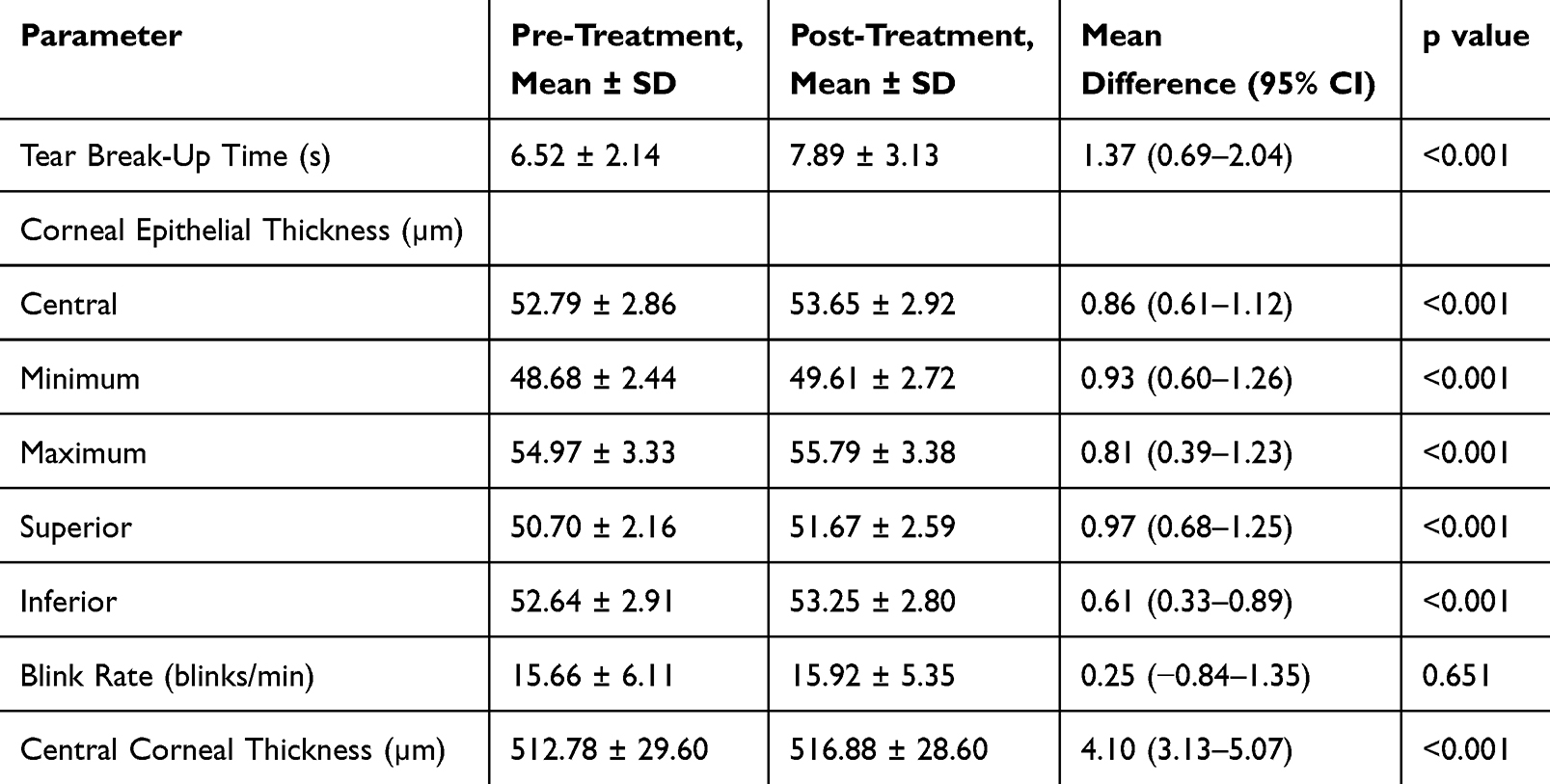 |
Table 2 Changes in Ocular Surface Parameters Following One Month of Carboxymethyl Cellulose Treatment |
A statistically significant change was also observed in central corneal thickness (CCT), which increased from 512.78 ± 29.60 µm to 516.88 ± 28.60 µm (Δ = +4.10 µm; 95% CI [3.13, 5.07]; p < 0.001). In contrast, no significant change was observed in blink rate (15.66 ± 6.11 blinks/min to 15.92 ± 5.35 blinks/min; Δ = +0.25 blinks/min; 95% CI [−0.84, 1.35]; p = 0.651). The pre- versus post-intervention comparison for CET, NIBUT, and CCT is illustrated in Figure 1.
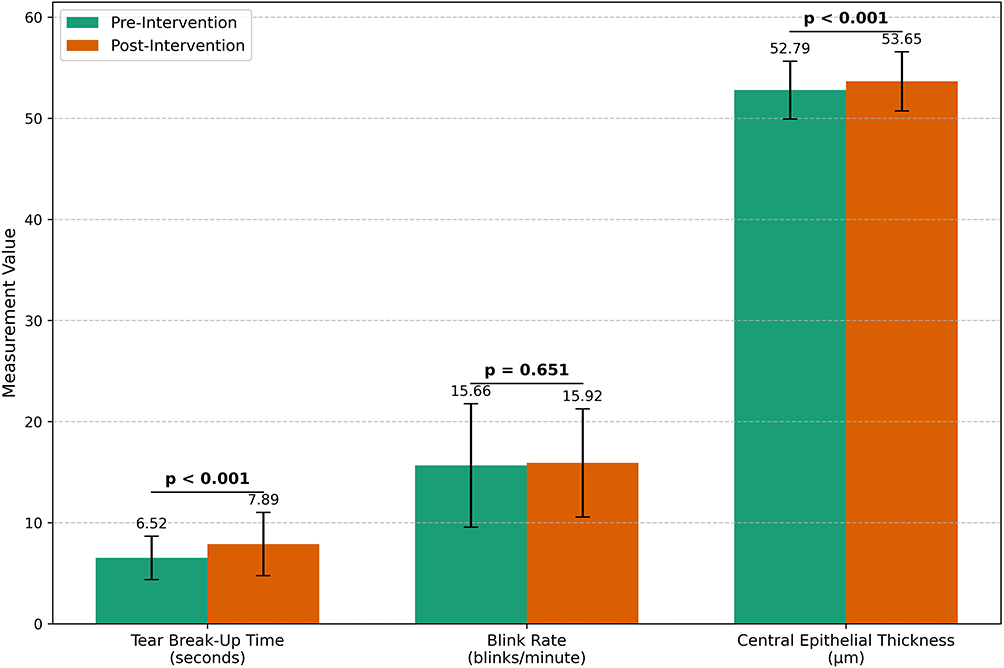 |
Figure 1 Comparison of ocular surface parameters before and after one month of carboxymethyl cellulose treatment. Bar chart showing mean values with standard deviation error bars for central corneal epithelial thickness (CET), non-invasive tear break-up time (NIBUT), and central corneal thickness (CCT). Bar chart showing mean values with standard deviation error bars for central corneal epithelial thickness (CET), non-invasive tear break-up time (NIBUT), and central corneal thickness (CCT). Bold text indicates a statistically significant change from baseline (p < 0.001). |
Correlation Between Screen Time and Baseline Tear Film Stability
Analysis of baseline characteristics revealed a significant negative correlation between daily digital screen time and baseline tear film stability (Pearson’s r = −0.72, p < 0.001), indicating that higher screen time was strongly associated with a lower NIBUT (Figure 2).
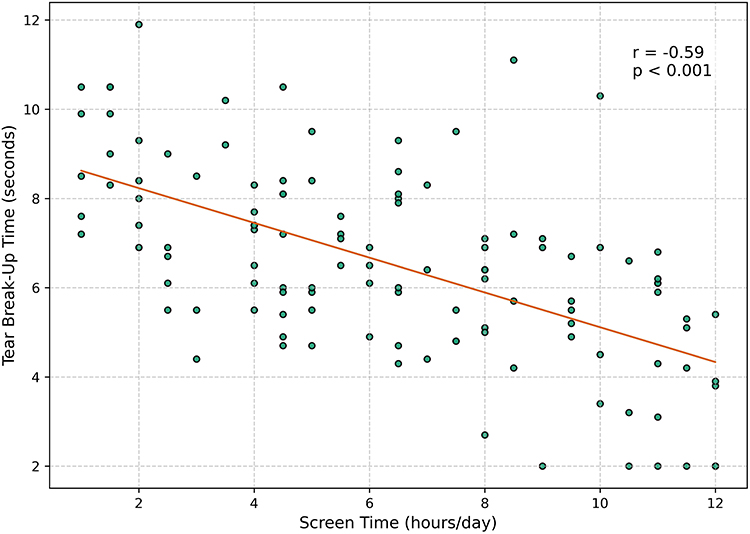 |
Figure 2 Correlation between daily digital screen time and baseline tear film stability. Scatterplot demonstrating a strong negative correlation (Pearson’s r = −0.72, p < 0.001) between self-reported daily screen time (hours) and baseline non-invasive tear break-up time (NIBUT in seconds). |
Predictors of Anatomical Response
A binary logistic regression was performed to explore baseline factors associated with anatomical change, defined as a post-treatment increase in central epithelial thickness. The analysis identified that older age within the cohort was a significant predictor of treatment response (adjusted OR = 1.15, 95% CI: 1.03–1.29, p = 0.013). Other baseline factors, including daily screen time, baseline tear break-up time, blink rate, central epithelial thickness, and gender, were not statistically significant predictors (Table 3). The forest plot in Figure 3 visually represents the adjusted odds ratios for each predictor.
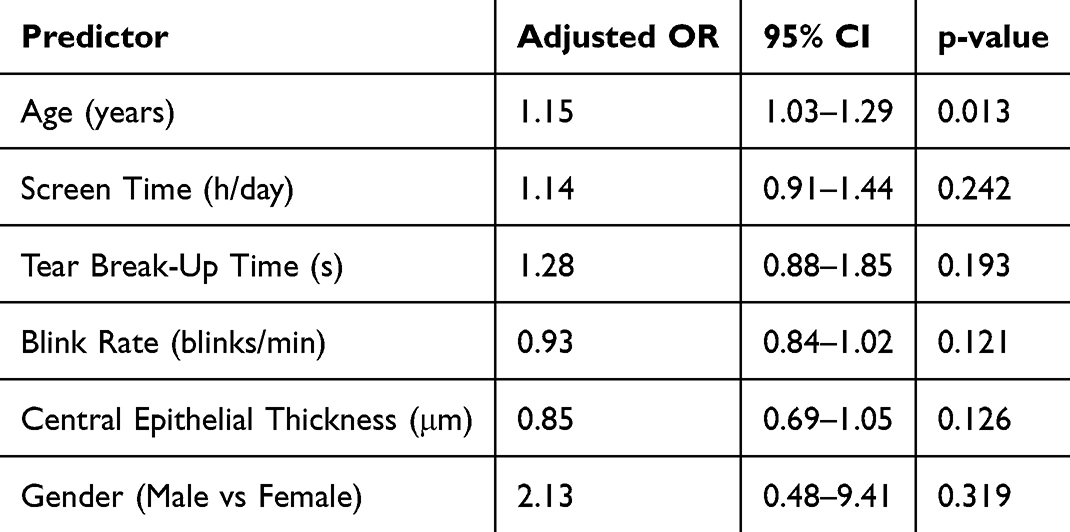 |
Table 3 Exploratory Analysis of Baseline Factors Associated with Central Corneal Epithelial Thickening Following Carboxymethyl Cellulose Treatment |
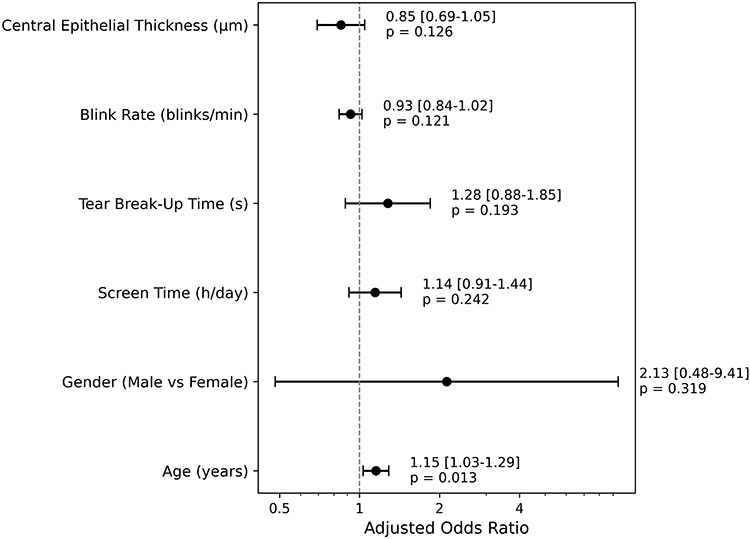 |
Figure 3 Forest plot of baseline factors associated with corneal epithelial thickening after carboxymethyl cellulose treatment. Adjusted odds ratios (OR) and 95% confidence intervals from a binary logistic regression analysis identifying factors associated with an increase in central epithelial thickness after treatment. An OR > 1 indicates higher odds of thickening. Older age was identified as a significant predictor (p = 0.013). |
Discussion
This prospective interventional study shows that after one month of preservative-free carboxymethyl cellulose (CMC) use, objective improvements in tear film stability and corneal epithelial thickness were observed in a young, digitally intensive population with DED. However, causality cannot be confirmed due to the single-arm design. Our key findings are threefold: First, we observed a clinically meaningful improvement in tear film stability, as evidenced by a significant increase in NIBUT, reinforcing the role of tear film supplementation as a cornerstone of DED management.1 Second, we documented a consistent, statistically significant increase in corneal epithelial thickness (CET) across all measured zones, although the absolute change was small (< 1 µm) and its clinical relevance remains uncertain.9,14 Third, we identified a strong negative correlation between daily digital screen time and baseline tear film stability, underscoring the role of modern lifestyle factors in DED pathogenesis, a growing concern in the era of digital device ubiquity.17,18
The observed increase in central CET (from 52.79 ± 2.86 µm to 53.65 ± 2.92 µm; Δ = +0.86 µm, p < 0.001) constitutes a key finding. Although statistically significant, the magnitude of change was below the reported repeatability limit of Fourier-domain OCT epithelial mapping (~1–2 µm), hence, these results should be interpreted cautiously. Nonetheless, the consistency of thickening across all corneal zones suggests that the effect may represent more than random measurement variability. While some studies have reported epithelial thinning in chronic, severe DED,19 our results in a younger cohort with screen-time-associated DED align with emerging evidence that subclinical edema or thickening may be an early adaptive response to chronic hyperosmolar and inflammatory stress.20 The high-resolution capability of Fourier-domain OCT allows detection of such subtle morphological changes before overt clinical signs appear.21,22
The mucoadhesive properties of carboxymethyl cellulose (CMC) may promote a more favorable tear film environment; however, this study cannot distinguish whether the observed epithelial thickening represents structural change or transient corneal hydration. Artificial tear instillation may induce short-term hydration detectable by OCT, and without a washout period or no-treatment control group, this effect cannot be excluded. Evidence from other external ocular surface exposures, such as regular periocular cosmetic use, indicates that tear film instability may occur without significant changes in tear secretion, underscoring the sensitivity of tear film dynamics to surface-level influences rather than structural alteration alone.23 Although measurements were standardized and obtained after complete blinking, transient fluid shifts may still influence epithelial thickness values. While the patterned thickening across corneal zones suggests a possible structural component, definitive differentiation requires controlled designs with untreated controls and multiple post-instillation time-point measurements.
The significant improvement in NIBUT (from 6.52 ± 2.14 seconds to 7.89 ± 3.13 seconds; Δ = +1.37 seconds, p < 0.001) confirms the efficacy of CMC in stabilizing the tear film, a finding consistent with previous studies on electrolyte-balanced formulations.24 This functional improvement is clinically relevant, as tear film stabilization is a primary goal in DED management. The strong inverse correlation we found between daily screen time and baseline NIBUT (r = −0.72, p < 0.001) powerfully reinforces the well-established causative link between prolonged digital device use, reduced blink rate, and ocular surface dysfunction.17,25 This finding is particularly relevant for our cohort of students and young professionals, highlighting a critical public health concern in the digital age.
In an exploratory predictive analysis, older age within our young cohort was associated with greater odds of CET improvement after treatment (adjusted OR = 1.15, p = 0.013). However, the effect size was modest, confidence intervals were wide, and the model may be underpowered given the number of covariates relative to outcome events. Therefore, this finding should be considered preliminary and requires validation in larger studies.2 Interestingly, baseline CET, screen time, blink rate, and other factors were not predictive, suggesting that CMC response may occur across different phenotypic presentations of screen-time-associated DED. This observation, though tentative, hints at the potential for personalized treatment approaches once better validated.26
Our study possesses several notable strengths. First, to our knowledge, it is the first to prospectively evaluate the structural and functional effects of artificial tears using advanced OCT epithelial mapping in a young, digitally intensive Nepalese population, a cohort underrepresented in the ophthalmic literature yet highly vulnerable to modern DED risk factors.17,18 Second, the use of objective, high-resolution Fourier-domain OCT provides precise, quantitative data on corneal epithelial changes, moving beyond subjective symptom scores alone and offering a robust biomarker for treatment efficacy.9,21 Third, our study design incorporated a comprehensive analysis that included not only efficacy outcomes but also an exploration of predictive baseline factors, adding a layer of depth that moves toward personalized medicine.26 Finally, rigorous methodology—including standardized measurement times, a single masked examiner, and objective compliance monitoring—enhances the internal validity of our findings.
However, these findings must be interpreted in light of several limitations. The primary limitation is the single-arm, non-randomized design, which precludes definitive causal attribution of the observed improvements solely to the CMC intervention and limits our ability to compare its efficacy against other formulations or a control arm.10 Second, the one-month follow-up is sufficient to detect initial changes but does not capture long-term sustainability or natural history. Third, the predictive analysis may be underpowered; larger samples are needed for validation. Furthermore, the predominantly female cohort, while typical for DED clinics, may limit generalizability to males.1 Lastly, the absence of molecular analyses (eg, tear cytokine profiling) means the biological mechanisms underlying the observed changes remain unclear.
In conclusion, our study provides evidence that carboxymethyl cellulose artificial tear use was associated with increased corneal epithelial thickness and improved tear film stability in young patients with digital device-associated dry eye. These findings suggest that CMC may contribute to a more stable ocular surface environment; however, controlled studies are required to confirm causality and restorative potential.
Future research should prioritize randomized controlled trials comparing different artificial tear formulations over longer follow-up periods to establish comparative efficacy and durability.10 Investigating the cellular and molecular mechanisms—through in vivo confocal microscopy or tear cytokine analysis—could clarify CMC’s mode of action and the pathophysiology of early-stage DED. Finally, validating our predictive model in larger, more diverse cohorts would help advance personalized dry eye therapy.
Ultimately, by demonstrating objective structural and functional changes, this study reinforces the importance of early intervention with appropriate lubricants in managing the modern epidemic of digital eye strain and dry eye disease.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, PK, upon reasonable request.
Acknowledgment
We would like to express our sincere gratitude to the Himalaya Eye Hospital for their support. We are especially thankful to those who participated in our research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
All expenses related to this project were covered personally, and no financial assistance was received from any specific organization.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocular Surf. 2017;15:276–10. doi:10.1016/j.jtos.2017.05.008
2. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
3. Cai Y, Wei J, Zhou J, Zou W. Prevalence and incidence of dry eye disease in Asia: a systematic review and meta-analysis. Ophthalmic Res. 2022;65(6):647–658. doi:10.1159/000525696
4. Al-Mohtaseb Z, Schachter S, Lee BS, Garlich J, Trattler W. The relationship between dry eye disease and digital screen use. Clin Ophthalmol. 2021;15:3811–3820. doi:10.2147/OPTH.S321591
5. Smith JA, Albenz J, Begley C, et al. The epidemiology of dry eye disease: report of the epidemiology subcommittee of the international Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):93–107.
6. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438–510. doi:10.1016/j.jtos.2017.05.011
7. Cui X, Hong J, Wang F, et al. Assessment of corneal epithelial thickness. Optom Vis Sci. 2014;91(12):1446–1454. doi:10.1097/OPX.0000000000000417
8. Çakır B, Doğan E, Çelik E, Babashli T, Uçak T, Alagöz G. Effects of artificial tear treatment on corneal epithelial thickness and corneal topography findings in dry eye patients. J Fr Ophtalmol. 2018;41(5):407–411. doi:10.1016/j.jfo.2017.06.032
9. Ribeiro BB, Marques JH, Baptista PM, et al. Corneal epithelial thickness correlation with dry eye symptom severity: a cross-sectional study. Clin Ophthalmol. 2024;18:3691–3692. doi:10.2147/OPTH.S509241
10. Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
11. Garrett Q, Simmons PA, Xu S, et al. Carboxymethylcellulose binds to human corneal epithelial cells and is a modulator of corneal epithelial wound healing. Investig Ophthalmol Vis Sci. 2007;48(4):1559–1567. doi:10.1167/iovs.06-0848
12. Liang Q, Liang H, Liu H, Pan Z, Baudouin C, Labbé A. Ocular surface epithelial thickness evaluation in dry eye patients: clinical correlations. J Ophthalmol. 2016;2016:1–8. doi:10.1155/2016/1628469
13. Yang Y, Hong J, Deng SX, Xu J. Age-related changes in human corneal epithelial thickness measured with anterior segment optical coherence tomography. Investig Ophthalmol Vis Sci. 2014;55(8):5032–5038. doi:10.1167/iovs.13-13831
14. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
15. Muhafiz E, Demir MS. Ability of non-invasive tear break-up time to determine tear instability in contact lens wearers. Int Ophthalmol. 2022;42(3):959–968. doi:10.1007/s10792-021-02079-3
16. Huang D, Li Y, Radhakrishnan S. Optical coherence tomography of the anterior segment of the eye. Ophthalmol Clin North Am. 2004;17(1):1–6. doi:10.1016/S0896-1549(03)00103-2
17. Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3(1):e000146. doi:10.1136/bmjophth-2018-000146
18. Coles-Brennan C, Sulley A, Young G. Management of digital eye strain. Clin Exp Optom. 2019;102(1):18–29. doi:10.1111/cxo.12798
19. Yu K, Asbell PA, Shtein RM, Ying GS. Dry Eye Subtypes in the Dry Eye Assessment and Management (DREAM) Study: a latent profile analysis. Transl Vis Sci Technol. 2022;11(11):1–9. doi:10.1167/tvst.11.11.13
20. Yokoi N, Georgiev GA. Tear film–oriented diagnosis and tear film–oriented therapy for dry eye based on tear film dynamics. Investig Ophthalmol Vis Sci. 2018;59(14 Special Issue):DES13–22. doi:10.1167/iovs.17-23700
21. Abtahi MA, Beheshtnejad AH, Latifi G, et al. Corneal epithelial thickness mapping: a major review. J Ophthalmol. 2024;2024(1):1–28. doi:10.1155/2024/6674747
22. Ang M, Baskaran M, Werkmeister RM, et al. Anterior segment optical coherence tomography. Prog Retin Eye Res. 2018;66:132–156. doi:10.1016/j.preteyeres.2018.04.002
23. Belbase U, Subedi A, Chhetri S. Impact of eye cosmetic use on tear break ‑ up time in females: a comparative study. Delhi J Ophthalmol. 2025;35(4):256–259. doi:10.4103/DLJO.DLJO_51_25
24. Asharlous A, Mirzajani A, Jafarzadehpur E, KhabazKhoob M, Ostadimoghaddam H. Objective and subjective assessing efficacy of a lubricating drop in eyes wearing silicone hydrogel contact lenses. J Curr Ophthalmol. 2016;28(2):69–74. doi:10.1016/j.joco.2016.03.007
25. Chu CA, Rosenfield M, Portello JK. Blink patterns: reading from a computer screen versus hard copy. Optom Vis Sci. 2014;91(3):297–302. doi:10.1097/OPX.0000000000000157
26. Baudouin C, Aragona P, Van Setten G, et al. Diagnosing the severity of dry eye: a clear and practical algorithm. Br J Ophthalmol. 2014;98(9):1168–1176. doi:10.1136/bjophthalmol-2013-304619
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.