Back to Journals » Patient Preference and Adherence » Volume 15
Changes in Beliefs About Post-Transplant Immunosuppressants Over Time and Its Relation to Medication Adherence and Kidney Graft Dysfunction: A Follow-Up Study
Authors Kostalova B ![]() , Mala-Ladova K
, Mala-Ladova K ![]() , Kubena AA, Horne R, Dusilova Sulkova S, Maly J
, Kubena AA, Horne R, Dusilova Sulkova S, Maly J ![]()
Received 17 October 2021
Accepted for publication 7 December 2021
Published 31 December 2021 Volume 2021:15 Pages 2877—2887
DOI https://doi.org/10.2147/PPA.S344878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Barbora Kostalova,1 Katerina Mala-Ladova,1 Ales Antonin Kubena,1 Rob Horne,2 Sylvie Dusilova Sulkova,3 Josef Maly1
1Department of Social and Clinical Pharmacy, Faculty of Pharmacy in Hradec Kralove, Charles University, Hradec Kralove, Czech Republic; 2Centre for Behavioural Medicine, UCL School of Pharmacy, University College London, London, UK; 3Hemodialysis Centre, University Hospital Hradec Kralove, Hradec Kralove, Czech Republic
Correspondence: Katerina Mala-Ladova
Department of Social and Clinical Pharmacy, Faculty of Pharmacy in Hradec Kralove, Charles University, Ak. Heyrovskeho 1203/8, Hradec Kralove, 500 05, Czech Republic
Tel +420 495 067 486
Email [email protected]
Purpose: The main aim was to evaluate the changes in beliefs about immunosuppressants over a 3-year period in patients after kidney transplantation. The second aim was to investigate the relationship between beliefs, medication adherence, and selected clinical outcomes such as graft functioning.
Patients and Methods: This observational follow-up study was conducted in the outpatient post-transplant clinic at the University Hospital Hradec Kralove in the Czech Republic. Adult patients, at least 4 weeks after kidney transplantation, were invited for the structured interview, which was followed by a self-administered questionnaire survey during their regularly scheduled visits at the clinic. Appropriate paired tests were used to compare two measurements of beliefs about immunosuppressants by BMQ-CZ© in 2016 (baseline) and in 2019 (follow-up). Self-reported adherence was measured by two validated tools (MARS-CZ© and BAASIS©) capturing implementation and discontinuation phases. A generalized linear model was used to investigate the relation between beliefs and the consecutive estimated glomerular filtration rate.
Results: The study involved 134 patients. Over time, their perceived treatment necessity beliefs of immunosuppressants decreased, while their treatment-related concerns increased. Overall self-reported non-adherence (ie, taking, dosing and discontinuation of immunosuppressants) was reported by 12% of the patients in both observation periods. In the follow-up period, timing non-adherence was reported by 52 (38.8%) patients. Higher baseline treatment concerns were associated with poor adherence whereas higher baseline treatment necessity beliefs corresponded with better kidney functioning, even after adjusting for age.
Conclusion: Higher treatment necessity beliefs corresponded with better kidney functioning, whereas higher treatment concerns were related to non-adherence to immunosuppressants at the beginning of the observed period. Still, most patients accepted their medicines that do not come without risk. Nevertheless, decreasing treatment necessity beliefs on one hand, and increasing treatment concerns on the other, should be considered in clinical practice.
Keywords: kidney transplantation, immunosuppressants, treatment necessity beliefs, treatment concerns, medication adherence
Introduction
Kidney transplant (KTx) is the most cost-effective treatment option for patients with end-stage renal failure. KTx significantly improves life expectancy, quality of life and reduces financial burdens on the health care system, leading to an increasing number of procedures worldwide.1–4 However, it is essential that patients manage a complex life-long therapeutic plan and attend medical follow-ups after KTx with emphasis on strict medication adherence. Medication adherence is defined as “the process by which patients take their medications as prescribed, composed of initiation, implementation and discontinuation”.5 Focusing on implementation patterns regarded as vital for immunosuppressive regimens, non-adherence may reach up to 17.4% and increases over time post-transplant.6–9
It is well known that many factors may influence implementation non-adherence. Factors at higher levels (ie, structural characteristics and practice patterns), however, do not differ within the same KTx follow-up care. Considering all the patient-related factors in general, beliefs about the medicines seem to play a decisive role.10–12 Usually, regardless of the level of adherence, patients themselves develop their own beliefs and attitudes towards the medication over time. This is supported by a recent meta-analysis involving 94 studies across 18 countries, showing that adherence to long-term medications was often related to patients’ beliefs about treatment where low adherence is linked to doubts about the personal feeling of need for the medication (treatment necessity beliefs) and the concerns about the potential adverse consequences (treatment concerns).13
Treatment necessity beliefs and treatment concerns can be reliably assessed by the Beliefs about Medicines Questionnaire (BMQ©).10 Compared with other chronic conditions, KTx recipients reported high treatment necessity beliefs and relatively high treatment concerns.11,12,14 The research suggests that adherence can be perceived as a ”double-edged sword”, in which the potential benefit is compromised by the tendency to cause harm.15
Even small deviations in adherence to immunosuppressants (>5%) are associated with a higher risk of graft rejection.16 Therefore, it is also important to evaluate the relationship between the patients’ behavior on one hand, and their perceived and easily monitored therapeutic goals on the other. In KTx patients, declining kidney function is one of the most clinically relevant markers of chronic graft rejection as a result of a possible under-immunosuppression, while the estimated glomerular filtration rate (GFR) is routinely assessed in the KTx follow-up care.17
The gap in our understanding exists because medication adherence is a dynamic process.18 Although there is evidence that non-adherence increases over time post-transplant,6,9 key information about the relationship between the change in adherence and the change in beliefs about immunosuppressants over time is still lacking. Nevertheless, it is observed that repeated assessment enables researchers to prove the consistency of beliefs during the treatment period. Therefore, we also need to know whether changes in the beliefs about immunosuppressants have any impact on key transplant outcomes.
The main aim of this study was to evaluate the changes in beliefs about immunosuppressants over a 3-year period in patients after kidney transplantation. The second aim was to investigate the relationship between beliefs, medication adherence, and selected clinical outcomes such as graft functioning.
Materials and Methods
Study Setting and Ethics
Waiting lists, organ allocation and management of transplant registries are managed by the Coordination Center for Transplantation, which is under direct supervision of the Ministry of Health in the Czech Republic.3 For the approximately 10 million Czech inhabitants, there are seven transplant centers providing over 500 KTx annually. Our study was performed in the University Hospital Hradec Kralove, providing approximately 30–50 KTx every year, and equipped with a separate inpatient and outpatient post-transplant clinic. In the context of the Czech health-care system, where each center is free to provide their own education regarding immunosuppressants and self-management, our hospital issues an educational booklet and an emergency phone number. Patients regularly visit the outpatient clinic in the prescribed follow-up periods (at first weekly, then once a month, followed by regular visits about every 3 months, a year after transplant), depending on the patients’ current health status. The follow-up care, just like the majority of medications, is covered by the public health insurance.
The Ethics Committee of the University Hospital Hradec Kralove approved the study protocol. The study was conducted in accordance with the Helsinki and Istanbul Declaration.
Study Population and Data Collection
This was an observational follow-up study, consisting of two data collection opportunities, conducted in an outpatient post-transplant clinic. The first baseline data collection (Phase I) was carried out from March 2016 to March 2017 using the convenience patient sample.14 The follow-up data collection (Phase II) was performed from April 2019 to December 2019 and all patients meeting the inclusion criteria were invited to participate. Subjects were considered eligible for inclusion in the study if they were aged ≥18 years and ≥4 weeks after KTx, and if they were on a maintenance immunosuppressive regimen in the given data collection period. Patients with severe cognitive or health impairment, or on acute anti-rejective therapy or hospitalized were all excluded.
During their scheduled visit at the clinic, patients were asked by a nurse to participate in the study. After providing a written informed consent, patients were invited to a pharmacist-led (BK) structured interview using the questionaries explained below (Phase I) and afterwards, to complete the questionnaires by themselves in written form (Phase II). Data on biomedical pre-transplant and transplant characteristics were collected from the patients’ electronic medical records. All the patients who participated in both phases and had no more than one missing answer in either of the questionnaires that focused on their beliefs or adherence to immunosuppressants were included in the current analysis. A detailed description of the study population recruitment is presented in Figure 1. Patient (age, gender, family history), transplant (time post-transplant, type of KTx), medication (current immunosuppressive regimen, number of medication intakes), and graft function (estimated GFR, re-transplantation) characteristics were collected from the medical documentation.
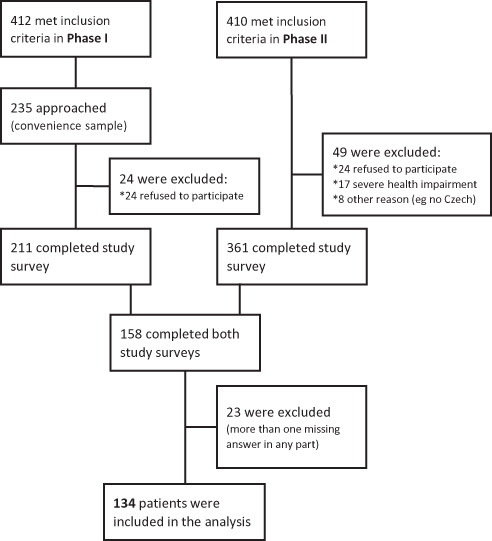 |
Figure 1 Study population. |
Survey
Data on socio-demographic characteristics (education, occupation), knowledge of the immunosuppressive regimen and perceived health status were reported by the patients in both study phases. During Phase I, self-reported adherence and beliefs about immunosuppressants were assessed using international tools previously validated in the Czech Republic, ie, BMQ-CZ and Medication Adherence Report Scale (MARS-CZ).10,19–21 During Phase II, the BMQ-CZ was repeated and the Czech written version of the Basel Assessment of Adherence to immunoSuppressive medIcations Scale (BAASIS©) was used to assess self-reported adherence to immunosuppressants.22
The BMQ© questionnaire has two versions: the BMQ Specific, assessing beliefs about medicines prescribed for a particular condition, and the BMQ General, assessing more general beliefs about medicines as a class of treatment. In our study, we employed the BMQ Specific, which comprises two scales: a 5-item Necessity scale assessing beliefs about the personal need for the medication and a 6-item Concerns scale assessing concerns about the potential adverse consequences of taking the medication. Each of the scale items are scored 1 (strongly disagree) to 5 (strongly agree). Individual item scores for the Necessity and Concerns scales are added up and divided by the number of items in the scale to give a scale score (range 1–5), with higher scores indicating stronger beliefs in treatment necessity beliefs and stronger treatment concerns, respectively. Additionally, the Necessity–Concerns Differential (NCD) was calculated by subtracting Concerns scores from Necessity scores to provide a numerical indicator (range −4 to +4) of how individual respondents judge their personal treatment necessity beliefs relative to their treatment concerns. According to the Necessity–Concerns Framework (NCF), patients can be divided into four subgroups based on whether they were above or below the scale midpoint for each of the scale scores, namely: accepting (high treatment necessity beliefs, low treatment concerns), ambivalent (high treatment necessity beliefs, high treatment concerns), indifferent (low treatment necessity beliefs, low treatment concerns) and skeptical (low treatment necessity beliefs, high treatment concerns).23 Cronbach’s alphas indicate good internal reliability for both the Necessity scale (α=0.75 in Phase I and α=0.67 in Phase II, respectively) and the Concerns scale (α=0.73 and α=0.80 (Phase II)).14
The MARS-5© consists of five statements about implementation (taking, dosing) and discontinuation. Each item is scored on a 5-point Likert scale, with 1 indicating ‘always‘ and 5 indicating ‘never‘. The sum score of 25 points represents full adherence; the non-adherence cut off varies among studies. The internal reliability was α=0.67.14
The BAASIS© was translated from English to Czech for the purposes of Phase II using forward and backward translation and following ISPOR guidelines.24 The recent version consists of six questions and assesses all phases of adherence: initiation of co-medications, implementation (taking, timing, dosing) and discontinuation of immunosuppressants. Any positive answer means non-adherence.22
Data Analysis
Data were analyzed using the software Wolfram Mathematica 12.0. The descriptive outputs were presented as the relative frequency (%) for binomial or multinomial variables, and as median (lower and upper quartile) for the numerical variables. In case of ceiling effect, the form of mean ± standard deviation was preferred. For numerical variables, the changes between two observations on the same subject were tested using the Wilcoxon paired test, the difference between two groups by the Mann Whitney U-test, and consistency in responses across two variables by the McNemar test or Fisher’s test, where appropriate. The difference in repeated measurements was demonstrated by the Box-Whisker chart.
Kidney function was determined by the estimated GFR, which was routinely assessed during medical follow-ups and calculated using the CKD-EPI equation. The time series of six GFR values obtained retrospectively from 2019 were transformed to one index for each patient by estimating the mean value (time-weighted average, TWA). For the estimation, the values between adjacent measurements were approximated by the uniform distribution parameterized by these adjacent values. The predictors of decreasing kidney function in association with treatment beliefs were evaluated by the General linear model, repeated measures.
A p-value of <0.05 was considered as statistically significant. As additional information to the p-value of the predictor, its effect size indicator η2 was calculated. Based on that, the predictors were categorized as small-medium-large effect size according to the Cohen convention.
Results
Population Characteristics
There were 134 KTx outpatients who participated in both Phase I and Phase II in the study. Comparing participants and non-participants, we found no difference regarding gender, age, and time after transplantation. Table 1 shows the socio-demographic and clinical information for each phase. There were 117 patients after their first KTx, 17 after a second KTx and only one patient who received a re-transplant between Phases I and II. The number of medication intakes increased as 78 patients were taking more drugs in Phase II than in Phase I (p<0.001). Table 1 also demonstrates that the respondents perceived their health condition similarly in both phases with no significant change, marking their health most frequently as ‘good‘.
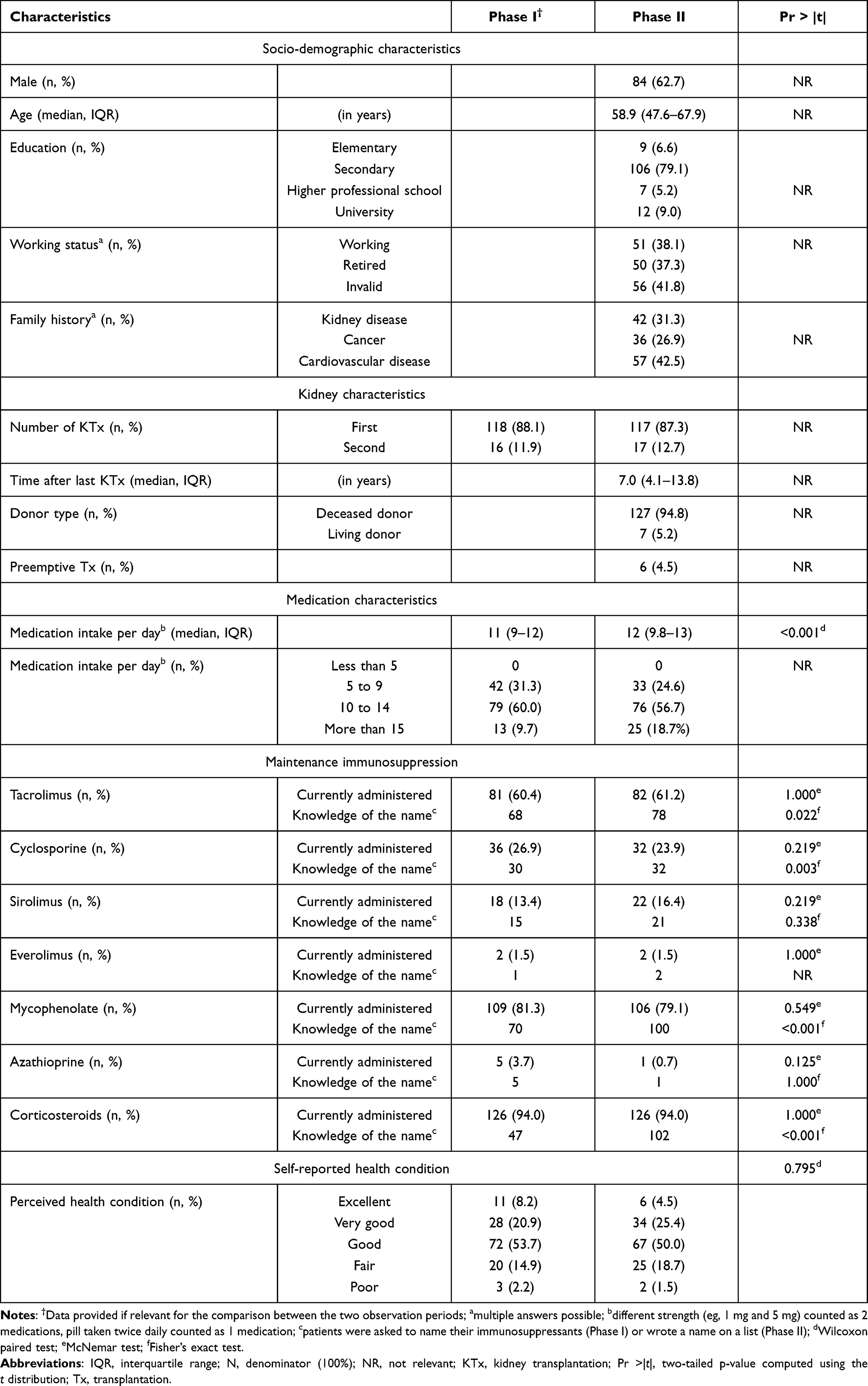 |
Table 1 Patient Characteristics by Observation Period (N=134) |
The most commonly prescribed IS regimen was a combination of tacrolimus, mycophenolate, and corticosteroid. A significant difference was observed between the abilities of patients to remember the name of the immunosuppressant, an ability which increased over time (p<0.001) as shown in Table 1.
BMQ-CZ Results
The mean Necessity scale score was 4.74 ± 0.47 and 4.33 ± 0.53 for Phase I and Phase II, respectively. Compared to the baseline, 84 patients had a lower perception of treatment necessity beliefs for immunosuppressants in the follow-up and only 13 patients showed higher perception in this regard. The mean Concerns scale score was 2.17 ± 0.96 and 2.54 ± 0.74, with 80 patients having a higher perception of treatment concerns in the follow-up, while 43 patients had lower treatment concerns. The analysis revealed that the Necessity scale score significantly decreased over time (p<0.001, large effect size η2=0.320), whereas the Concerns scale score increased (p<0.001, medium effect size η2=0.097). Changes in beliefs did not differ between gender, age, and time posttransplant. The NCD was positive (2.57 ± 1.06 vs 1.79 ± 0.97) but declined over time (p<0.001) as shown in Figure 2. One patient had a higher Concerns than Necessity score during both phases. The evolution of Necessity and Concerns scale scores is demonstrated in Figure 3.
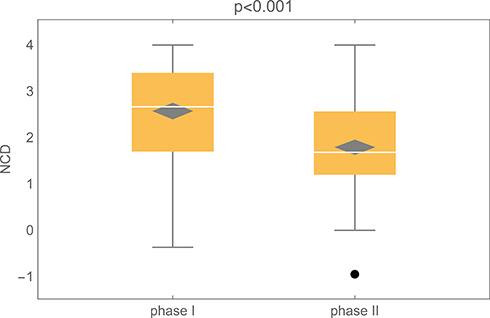 |
Figure 2 Boxplots showing the Necessity–Concerns Differential (NCD) scores during Phase I and II (n=134). |
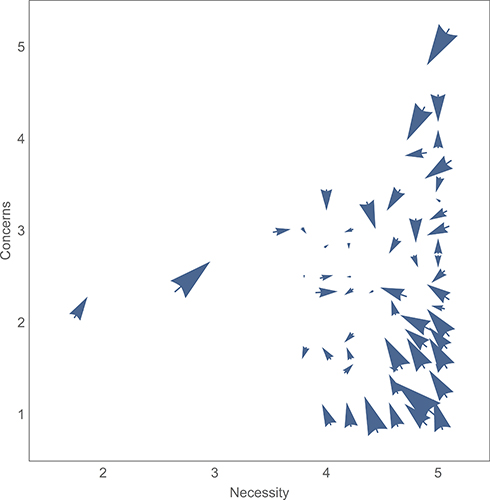 |
Figure 3 Evolution of treatment necessity and concerns beliefs during Phase I and II (n=134). Notes: X-axis represents the treatment necessity score, where a higher number corresponds to higher needs. Y-axis represents the treatment concern score, where a higher number corresponds to higher concerns. The arrows show the development of individual beliefs during two measurements. Each arrow corresponds to one specific score where a larger arrow size corresponds to a larger number of patients with the same beliefs. |
The NCF indicated that 79 patients showed accepting and 14 had ambivalent views about their immunosuppressants during both study phases. A distinctive change was reported by 18 patients, modifying their views from ambivalent to accepting. Conversely, 21 patients changed their views from accepting to ambivalent. Nevertheless, no significant pattern in remaining in either category was revealed over time.
Adherence to Immunosuppressants
Implementation and discontinuation patterns in medication adherence were evaluated by two different questionnaires (Table 2). Non-adherence to the exact timing was assessed only in Phase II, but over one-third of patients showed taking their immunosuppressants more than two hours before or after the prescribed time within the last 4 weeks. Excluding timing, overall non-adherence was reported in about 12% patients in each phase, of which 8 patients were non-adherent in both phases. Discontinuation was not reported by any patient.
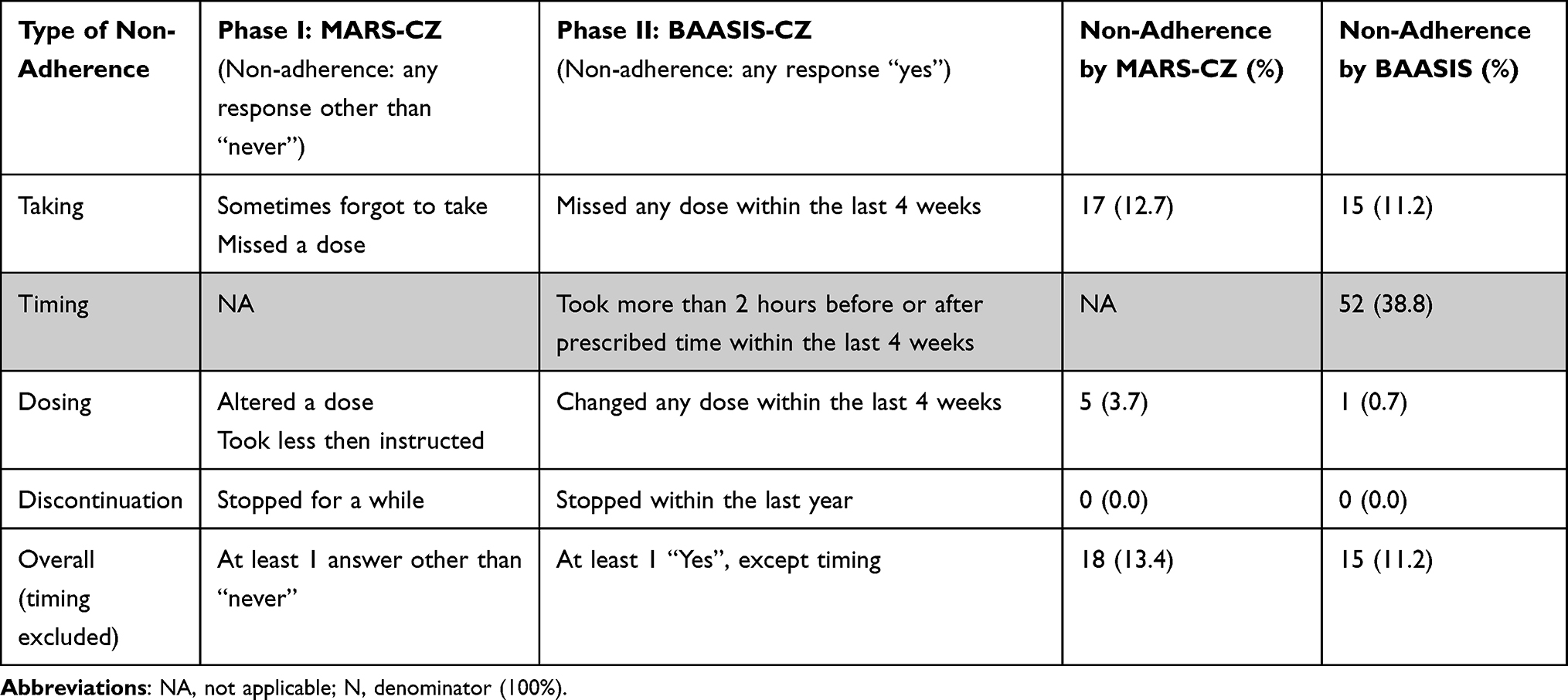 |
Table 2 Comparison of Questionnaires Measuring Self-Reported Adherence (N=134) |
Medication adherence in Phase I was significantly associated with the Concerns score (p=0.0445) with a mean score of 2.09 ± 0.88 for fully adherent and 2.66 ± 1.14 for non-adherent patients. Necessity scores revealed close but non-significant association with adherence by MARS-CZ (p=0.0526) with a mean score of 4.79 ± 0.36 for fully adherent and 4.44 ± 0.89 for non-adherent patients. No significant associations were observed between adherence measured by BAASIS© and BMQ-CZ specific subscale in Phase II.
Association Between Beliefs About Immunosuppressants and Kidney Function
Complete GFR data was provided by 130 out of 134 patients. Higher baseline treatment necessity beliefs were significantly associated with better kidney function over time calculated as TWA (p=0.0206, medium effect size η2=0.059). An increase by one point in the total Necessity score predicts an increase in the average weighted kidney function of 0.15 mL/s. For example, an increase by one score on the Necessity scale means an increase by 0.3 mL/s. Moreover, the evident influence of the patient´s age on the change in kidney function over time (p=0.0076, medium effect size η2=0.055) confirmed the association of higher perception of treatment necessity beliefs with better TWA even after adjusting for age (p=0.0059). Concerns scale scores and the NCD were not significant in relation to TWA in any study phase.
Discussion
This follow-up study is the first research in the Czech Republic that focuses on changes in behavioral patterns of taking immunosuppressants carried out in an outpatient transplantation setting. Paired difference tests revealed a decrease in perceived treatment necessity beliefs and an increase in treatment concerns over the 3-year period, which was translated into a significant decrease in the NCD. For almost all patients, the NCD remained positive, indicating that the perceived benefits were expected to outweigh the risks in the long-term treatments. Furthermore, high treatment necessity beliefs for the immunosuppressants after KTx reflected the fact that most patients accepted these medicines. Self-reported non-adherence (except ‘timing‘) was approximately 12% in both observation measurements. However, targeted questions on strict ‘timing‘ of immunosuppressants addressed in the follow-up revealed non-adherence in 39% patients.
The major strength of this study was repeated measurement of beliefs and adherence as they are dynamic in nature. Follow-ups are more often applied in intervention studies, where the effect of such intervention is tested instead of the natural evaluation of patients’ attitudes over time. Unlike for adherence, much less information is available in the literature regarding the effect of time on beliefs of KTx patients. In line with Massey et al,25 we found decreasing treatment necessity beliefs and increasing treatment concerns over time with large and moderate effect sizes, respectively. Two cross-sectional studies described the correlation between lower treatment necessity beliefs and higher age at the time of measurement or higher age at the time of KTx as well as higher treatment concerns and increasing time after KTx with small or moderate effect sizes, respectively.14,26 Therefore, decreasing treatment necessity beliefs and increasing treatment concerns is of clinical relevance in KTx patients and the examination of the patients’ attitudes towards immunosuppressants should be included in personalized management at health care facilities.
Alongside other chronic conditions, non-adherence to immunosuppressants usually increases with time after KTx.7–9 Interestingly, we found a stable adherence to immunosuppressants over the 3 years, which can be explained by under-reporting. Contrary to our expectations, employing different ways of data collection (interview vs written response), which can play a role in patients truly admitting adherence and beliefs, did not show any difference in adherence.
It is worth noting that using international validated questionnaires, we were able to compare different aspects of medication adherence at one specific time-point. In our study, adherence was measured by two self-reported tools suitable for patients taking immunosuppressants and no issue was found in the discontinuation phase of medication adherence. However, the implementation phase may pose a challenge in the clinical practice, particularly in terms of the exact timing of immunosuppressants. For instance, the BAASIS© was used in a multicentric cross-sectional BRIGHT study with 1397 heart transplant patients and in multicentric cross-sectional ADHERE BRAZIL28 study with 1105 KTx patients. The rate in ′taking′ in our study (11.2%) was similar as the findings in the BRIGHT study (17.4%),27 as well as in the ADHERE BRAZIL study (14.3%).28 However, issues with ′timing′ were found in 33.8%, 26.5%27 and 30.6%28 cases, respectively.
Furthermore, the comparison between studies is complicated by the various study designs and differences in understanding adherence29 even though we used the most recent adherence-based taxonomy.5,30 Adherence assessment itself is not without any limitation. For example, there is a clinical difference between adherence to taking immunosuppressants as such, and adherence to the accurate timing of taking them. Moreover, it has to be taken into account that the illness-related behavior is a part of patient self-regulation.13 In this context, patient perceptions of illness, and of medicines, can motivate them to withstand the illness by way of adherence.31,32 For instance, the association between medication adherence and beliefs was found only with higher treatment concerns related to non-adherence at the baseline (albeit, not at the follow-up), which can be explained by the similar construct of BMQ© and MARS-5© derived from greater subjective benevolence of responses using a Likert scale, showing either intentional and unintentional behavior. On the other hand, the overall high adherence in our study population does not allow the generalization of the results. Different views on self-efficacy can also be mediated by the evaluation of patients’ knowledge of immunosuppressants, which increased over time as a possible outcome of advanced perception of the importance of immunosuppressants by the patients themselves. This observation supports previous findings, namely that the measurement itself may affect the outcome.33
Previous studies have shown that even small deviations from the prescribed immunosuppressive regimen were associated with negative clinical outcomes.16,34–36 In our study, we found that higher baseline treatment necessity beliefs for immunosuppressants corresponded with better kidney functioning. This might be caused by the overall better adherence among these patients, even though the relationship between adherence and clinical outcomes was not analyzed because of a strong ceiling effect. It may also be worth mentioning that, due to routine measurement of kidney functioning, patients may perceive the stability or progression of their disease, which may be reflected in their beliefs on the effect of immunosuppressants, regardless of whether the drugs worked or not, and also on how much the therapy was actually needed.
There are some limitations that should be pointed out. Our results may have been affected by under-reporting in all self-reports, which lead to non-adherent patients being categorized as adherent. Beliefs, on the other hand, were measured on a continuous scale showing attitudes of patients regarding their immunosuppressants, which can show some important behavioral patterns over time. Furthermore, a small study sample limited our possibilities to detect differences and the statistical relationship between beliefs and adherence. Nevertheless, when evaluating the sample representativeness, we found no difference regarding gender, age, and time after KTx. The relationship between beliefs and kidney functioning showed a possible prediction of patients’ perception of this clinical parameter. However, as the association was not demonstrated in the follow-up, it is necessary to be analyzed further.
A major implication of this study is that adherence management comprising the evaluation of patients’ beliefs should be part of the KTx follow-up care. Consistent with our findings, compelling evidence shows that one-time discharge education or providing an educational booklet alone is ineffective in changing behavior in long-term treatments. Also, self-reported questionnaires provide an easy and inexpensive tool for regular adherence measurement.1 Once identified, non-adherent patients should be targeted with proper interventions including examining the patients’ attitudes. The interventions demand the involvement of both patients and stakeholders as well as the implementation science approach to ensure its sustainability in clinical practice.37,38
Conclusion
Higher treatment necessity beliefs for post-transplant immunosuppressants corresponded with better kidney functioning, whereas higher treatment concerns were related to medication non-adherence at the beginning of the observed period. Still, overall positive NCD reflected the fact that most patients accepted their immunosuppressants that do not come without risk. Nevertheless, decreasing treatment necessity beliefs and increasing treatment concerns over time, post-transplant, should be considered in clinical practice.
Ethics Statement
Ethical approval was obtained from the University Hospital Hradec Kralove (No. 201902 S21P). All patients signed a written consent to participate in the study and agreed with the dissemination of anonymized results.
Acknowledgments
The authors acknowledge the University Hospital Hradec Kralove for providing the clinical data for this research, the nurses (particularly Zuzana Sircekova and Alena Molnarova) at the Transplantation Clinic for their contribution in addressing patients to participate in the study, the Patients’ Organization Alzbeta for their help in developing and piloting the testing of the self-reported tools, and patients who participated in this study. The authors also acknowledge Professor Sabina M. De Geest from the University of Basel for granting permission to use the BAASIS© scale and Professor Rob Horne from the University College London for granting permission to use the MARS-5© and BMQ© scales.
Funding
This study was supported by Charles University (Project SVV 260551, PROGRES Q40/14 and Q42) and by the Ministry of Health, the Czech Republic (CZ NU20-02-00086).
Disclosure
Professor Rob Horne is supported by the National Institute for Health Research (NIHR, Collaboration for Leadership in Applied Health Research and Care (CLAHRC), North Thames at Bart’s Health NHS Trust and Asthma UK (AUKCAR). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health; also reports personal fees from Speaker engagements with honoraria with the following companies: AbbVie, Abbott, Amgen, Astellas, AstraZeneca, Boehringer Ingelheim, Biogen, Gilead Sciences, GlaxoSmithKline, Janssen, Merck Sharp Dohme, Merck, Novartis, Pfizer, Procter & Gamble, Roche, Sanofi, Shire Pharmaceuticals, TEVA, UCB. In addition, Professor Rob Horne is Founding Director of UCL-Business company (Spoonful of Sugar Ltd) providing consultancy on treatment engagement and patient support programmes to healthcare policy makers, providers and pharmaceutical industry outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Neuberger JM, Bechstein WO, Kuypers DR, et al. Practical Recommendations for Long-term Management of Modifiable Risks in Kidney and Liver Transplant Recipients: a Guidance Report and Clinical Checklist by the Consensus on Managing Modifiable Risk in Transplantation (COMMIT) Group. Transplantation. 2017;101(4SSuppl 2):S1–S56.
2. Data of the WHO-ONT. Global Observatory on Donation and Transplantation; WHO-ONT collaboration; 2016. Available from: http://www.transplant-observatory.org/data-charts-and-tables/chart/.
3. Data of the Coordination Center for Transplantation. Prague; 2019. Available from: https://kst.cz/en/.
4. Purnajo I, Beaumont JL, Polinsky M, Alemao E, Everly MJ. Trajectories of health-related quality of life among renal transplant patients associated with graft failure and symptom distress: analysis of the BENEFIT and BENEFIT-EXT trials. Am J Transplant. 2020;20(6):1650–1658.
5. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705.
6. De Geest S, Burkhalter H, Bogert L, et al. Describing the evolution of medication nonadherence from pretransplant until 3 years post-transplant and determining pretransplant medication nonadherence as risk factor for post-transplant nonadherence to immunosuppressives: the Swiss Transplant Cohort Study. Transpl Int. 2014;27(7):657–666.
7. Couzi L, Moulin B, Morin MP, et al. Factors predictive of medication nonadherence after renal transplantation: a French observational study. Transplantation. 2013;95(2):326–332.
8. De Geest S, Burkhalter H, Bogert L, Berben L, Glass TR, Denhaerynck K; Psychosocial Interest Group; Swiss Transplant Cohort Study. Describing the evolution of medication nonadherence from pretransplant until 3 years post-transplant and determining pretransplant medication nonadherence as risk factor for post-transplant nonadherence to immunosuppressives: the Swiss Transplant Cohort Study. Transpl Int. 2014;27(7):657–666.
9. Villeneuve C, Rousseau A, Rerolle JP, et al. Adherence profiles in kidney transplant patients: causes and consequences. Patient Educ Couns. 2020;103(1):189–198.
10. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14:1–24.
11. Griva K, Davenport A, Harrison M, et al. Non-adherence to immunosuppressive medications in kidney transplantation: intent vs. forgetfulness and clinical markers of medication intake. Ann Behav Med. 2012;44(1):85–93.
12. Chisholm-Burns M, Pinsky B, Parker G, et al. Factors related to immunosuppressant medication adherence in renal transplant recipients. Clin Transplant. 2012;26:706–713.
13. Horne R, Chapman SC, Parham R, et al. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS One. 2013;8(12):e80633.
14. Vankova B, Mala-Ladova K, Kubena AA, et al. Immunosuppressive therapy related adherence, beliefs and self-management in kidney transplant outpatients. Patient Prefer Adherence. 2018;12:2605–2613.
15. Horne R, Cooper V, Wileman V, et al. Supporting adherence to medicines for long-term conditions: a perceptions and practicalities approach based on an extended common-sense model. Eur Psychol. 2019;24(1):82–96.
16. Butler JA, Roderick P, Mullee M, et al. Frequency and impact of nonadherence to immunosuppressants after renal transplantation: a systematic review. Transplantation. 2004;77(5):769–776.
17. Duncan S, Annunziato RA, Dunphy C, et al. A systematic review of immunosuppressant adherence interventions in transplant recipients: decoding the streetlight effect. Pediatr Transplant. 2018;22(1). doi:10.1111/petr.13086
18. Vrijens B, Antoniou S, Burnier M, et al. Current situation of medication adherence in hypertension. Front Pharmacol. 2017;8:100.
19. Horne R, Weinman J. Self-regulation and self-management in asthma: exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol Health. 2002;17(1):17–32.
20. Matoulkova P, Krulichova IS, Macek K, et al. Chronically ill Czech patients’ beliefs about medicines: the psychometric properties and factor structure of the BMQ-CZ. Ther Innov Regul Sci. 2013;47(3):341–348.
21. Ladova K, Matoulkova P, Zadak Z, et al. Self-reported adherence by Mars-CZ reflects LDL cholesterol goal achievement among statin users: validation study in the Czech Republic. J Eval Clin Pract. 2014;20(5):671–677.
22. Dobbels F, Berben L, De Geest S, et al. The psychometric properties and practicability of self-report instruments to identify medication nonadherence in adult transplant patients: a systematic review. Transplantation. 2010;90(2):205–219.
23. Chater AM, Parham R, Riley S, Hutchison AJ, Horne R. Profiling patient attitudes to phosphate binding medication: a route to personalising treatment and adherence support. Psychol Health. 2014;29(12):1407–1420.
24. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for Patient-Reported Outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104.
25. Massey EK, Tielen M, Laging M, et al. Discrepancies between beliefs and behavior: a prospective study into immunosuppressive medication adherence after kidney transplantation. Transplantation. 2015;99(2):375–380.
26. Bünemann M, Bauer-Hohmann M, Klewitz F, et al. Beliefs about immunosuppressant medication and correlates in a German kidney transplant population. J Psychosom Res. 2020;132:109989.
27. Denhaerynck K, Berben L; BRIGHT study team, et al. Multilevel factors are associated with immunosuppressant nonadherence in heart transplant recipients: the international BRIGHT study. Am J Transplant. 2018;18(6):1447–1460.
28. Marsicano-Souza EO, Colugnati F, Geest S, Sanders-Pinheiro H. Nonadherence to immunosuppressives and treatment in kidney transplant: ADHERE Brazil Study. Rev Saude Publica. 2021;55:33.
29. Gokoel SRM, Gombert-Handoko KB, Zwart TC, et al. Medication non-adherence after kidney transplantation: a critical appraisal and systematic review. Transplant Rev. 2020;34(1):100511.
30. De geest S, Zullig LL, Dunbar-Jacob J, et al. ESPACOMP medication adherence reporting guideline (EMERGE). Ann Intern Med. 2018;169(1):30–35.
31. Massey EK, Tielen M, Laging M, et al. The role of goal cognitions, illness perceptions and treatment beliefs in self-reported adherence after kidney transplantation: a cohort study. J Psychosom Res. 2013;75(3):229–234.
32. Unni E, Shiyanbola OO, Farris KB. Change in medication adherence and beliefs in medicines over time in older adults. Glob J Health Sci. 2015;8(5):39–47.
33. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;2014(11):CD000011.
34. Takemoto S, Pinsky B, Schnitzler M, et al. A retrospective analysis of immunosuppression compliance, dose reduction and discontinuation in kidney transplant recipients. Am J Transplant. 2007;7(12):2704–2711.
35. Michelon T, Piovesan F, Garcia V, et al. Noncompliance as a cause of renal graft loss. Transplant Proc. 2002;34(7):2768–2770.
36. Gaynor JJ, Ciancio G, Guerra G, et al. Graft failure due to noncompliance among 628 kidney transplant recipients with long-term follow-up: a single-center observational study. Transplantation. 2014;97(9):925–933.
37. Kostalova B, Ribaut J, Dobbels F, et al. Medication adherence interventions in transplantation lack information on how to implement findings from randomized controlled trials in real-world settings: a systematic review. Transplant Rev. 2022;36(1):100671.
38. Zullig LL, Deschodt M, Liska J, et al. Moving from the trial to the real world: improving medication adherence using insights of implementation science. Annu Rev Pharmacol Toxicol. 2019;59:423–445.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.