Back to Journals » Open Access Emergency Medicine » Volume 17
Challenges in the Literature Around Context-Sensitive Implementation of Shared Decision Making in Emergency Medicine: A Scoping Review
Authors Wehking F ![]() , Geiger F, Scheibler F
, Geiger F, Scheibler F ![]() , Stolz-Klingenberg C, Monsef I, Litsch D, Hemmer S, Lewejohann JC
, Stolz-Klingenberg C, Monsef I, Litsch D, Hemmer S, Lewejohann JC
Received 8 January 2025
Accepted for publication 15 August 2025
Published 13 September 2025 Volume 2025:17 Pages 267—287
DOI https://doi.org/10.2147/OAEM.S516347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Amit Agrawal
Felix Wehking,1 Friedemann Geiger,2 Fueloep Scheibler,2 Constanze Stolz-Klingenberg,2 Ina Monsef,3 Daniel Litsch,1 Stefanie Hemmer,1 Jan-Christoph Lewejohann1
1Department of Emergency Medicine, University Hospital Jena, Jena, Germany; 2National Competency Centre for Shared Decision Making, University Medical Centre Schleswig-Holstein, Kiel, Germany; 3Institute of Public Health, University Hospital Cologne, Köln, Germany
Correspondence: Felix Wehking, Klinik für Notfallmedizin, Universitätsklinikum Jena, Am Klinikum 1, Jena, 07747, Germany, Tel +4936419322001, Email [email protected]
Background: Shared decision making is a healthcare method in which health personnel and patients collaboratively evaluate different management options for medical decisions. Despite possible restraints this method encounters in the context of emergency medicine, there is a growing body of evidence. This article critically appraises the current literature and challenges to inform future research efforts.
Methods: This scoping review respects the PRISMA- and PECOS-methodologies. Qualitative- and quantitative studies were included when exposing emergency health personnel or patients to collaborative care for medical decisions with multiple reasonable management options. PubMed, CENTRAL, APA PsycINFO, Web of Science, reference lists and research group remarks served as data sources. Three researchers handled title- and abstract screening; one researcher extracted and synthesized data. Basic data on study design, publication date, country of origin, estimates for time consumption and more were extracted through standardized forms for all publications. All outcomes from the randomized clinical trials were included and reported, following the authors’ conclusions. This includes effects on consultation times. Through tabular visualization, critical appraisal and author group discussions, challenges in the literature were summarized narratively. Neither risk of bias assessment nor meta-analysis were performed.
Results: Of 3954 hits, 3428 remained for the title- and abstract screening and 67 for data synthesis. Studies predominantly utilized observational designs (n=27), originated from the USA (n=50) and were published between 2011 and 2020 (n=46). The included randomized trials (n=6) report heterogeneous results on patient-reported outcome measures and resource utilization. Patient safety was reported as not affected. In three randomized trials, consultations were prolonged by 2 minutes on average. Through critical appraisal and author group discussions, six annotations on the literature on shared decision making in emergency medicine were stipulated.
Conclusion: Research on shared decision making in emergency medicine utilizes different, intertwined terminologies, originates mostly from the USA and focuses on decision aids. The few randomized trials exclude high-risk patients and suggest potential resource-saving effects without compromising patient safety. The formal increase in discussion times appears debatable.
Plain Language Summary: Shared decision making between health professionals and patients might be useful in situations that hold more than one reasonable management option. While health professionals offer facts on the available options, patients contribute their preferences and needs. Shared decision making has been evaluated extensively in non-emergency situations. And even in emergency medicine, there are some articles about it. This literature review aims to outline the existing publications and associated challenges around shared decision making in emergency medicine. Therefore, several literature databases were searched for existing publications by three separate researchers. All publications containing data on patient participation in emergency departments were included in the summary. The narrative synthesis resulted in five annotations: Different terms are being utilized (1); most publications originate from the USA between 2010 and 2020 (2); interventions evaluate shared decision making aids (3); few randomized trials exist and they exclude high-risk patients, yet highlight potential reductions in resource use (4); consultations are reported as slightly prolonged (5), although this effect is debatable, considering qualitative aspects of time. These results raise implications for future research efforts that might lead to beneficial effects on aspects around ethics, the economy and patient satisfaction.
Keywords: patient participation, evidence-based medicine, ethics, patient–physician collaboration, health communications, economics, future of healthcare
Introduction
Rationale and Objectives
Different perspectives emphasize the implications for patient participation in healthcare decisions. Ethicists might underline the importance of patient autonomy.1 Lawyers could add existing legal requirements for patient elucidation (§630 German Civil Code). Economists would probably highlight potential reductions in healthcare resource utilization.2 Lastly, physicians are likely to throw in possible improvements in the patient–physician relationship and treatment adherence.3 Consequently, patient-centered care has become subject to ongoing research. One modern concept around patient-centered care should be seen in shared decision making (SDM).4 Frameworks describe it as patients and providers evaluating several justifiable management options, respecting providers’ expertise and patients’ preferences likewise.5 Naturally, the terms patient participation, patient-centered care, shared decision making, informed consent and others overlap6 and are subject to constant development, depending on the underlying values, norms and understandings. This constant development also accounts specifically for the concepts around SDM.7
Emergency medicine (EM) poses no exception to efforts of patient-centered care.8 Just before the turn of the millennium, Yamamoto published two studies, exposing parents of children with fever9 and skin lacerations10 towards collaborative care. While these efforts were labeled informed consent (yet included aspects of today’s SDM), more recent literature is clearly labeled as the latter.8 At this point, one might argue that emergency departments (EDs) are barely feasible for patient participation as they contain a noisy environment, time restraints and patients potentially holding time-sensitive pathologies.8 Yet, the most recent systematic review on SDM in EDs by Ubbink et al highlights a relevant number of publications.11 In addition to their work, this article longs to examine challenges in the literature, moving the discussion from what to why. For this broad approach, a scoping review was seen as a feasible study design. Furthermore, three questions guided the methodological conception: 1. What is the current evidence on SDM in EM? 2. What effects of SDM interventions on EM do existing randomized clinical trials (RCTs) suggest? 3. Does SDM in EM lead to longer consultation times? These questions were developed together with emergency physicians who – in contrast to the academic literature – face more practical challenges around patient participation in their work. If RCTs suggested benefits in economic aspects or patients’ clinical outcomes or satisfaction, this would strengthen the implication for SDM in EM. Lastly, consultation times are repeatedly stated by clinicians as one barrier to the implementation of collaborative care.12
Materials and Methods
Protocol and Registration
This scoping review is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR)13 that is depicted in the supplementary material. The review was registered on the Open Science Framework.14
Eligibility Criteria, Information Sources and Search
An information specialist (IM) helped to develop the search strategy. It is intended to reflect the different terms used to describe attempts to foster SDM. PubMed, Cochrane Central Register of Controlled Trials, APA Psycinfo and Web of Science were searched until 21st July 2024. Reference lists of included articles and research group remarks were last appraised on 25th July 2024. All publications on human subjects were included if written in English or German. The full search strategy is provided in the supplementary material. Articles were handled in a reference manager (Clarivate End Note 21).
Selection of Sources of Evidence
Utilizing a PECOS framework (Box 1),15 all publications on settings in the ED and resuscitation services were included. They had to expose patients or health personnel to concepts of collaborative care like patient participation, patient-centered care or informed consent. More than one available and reasonable management option had to be present. Qualitative and quantitative data were eligible from both prospective and retrospective study designs. In detail, RCTs, pre-post-designs, hypothetical scenarios, interrupted time series and observational studies were included. Purely theoretical studies presenting frameworks without new primary or secondary data were omitted. Also, case reports, opinion pieces, editorials, comments, newspapers, letters and grey literature were excluded. Lastly, articles were omitted when examining patients’ intention to participate in research, as this poses no decision related to patients’ medical treatment in the ED.
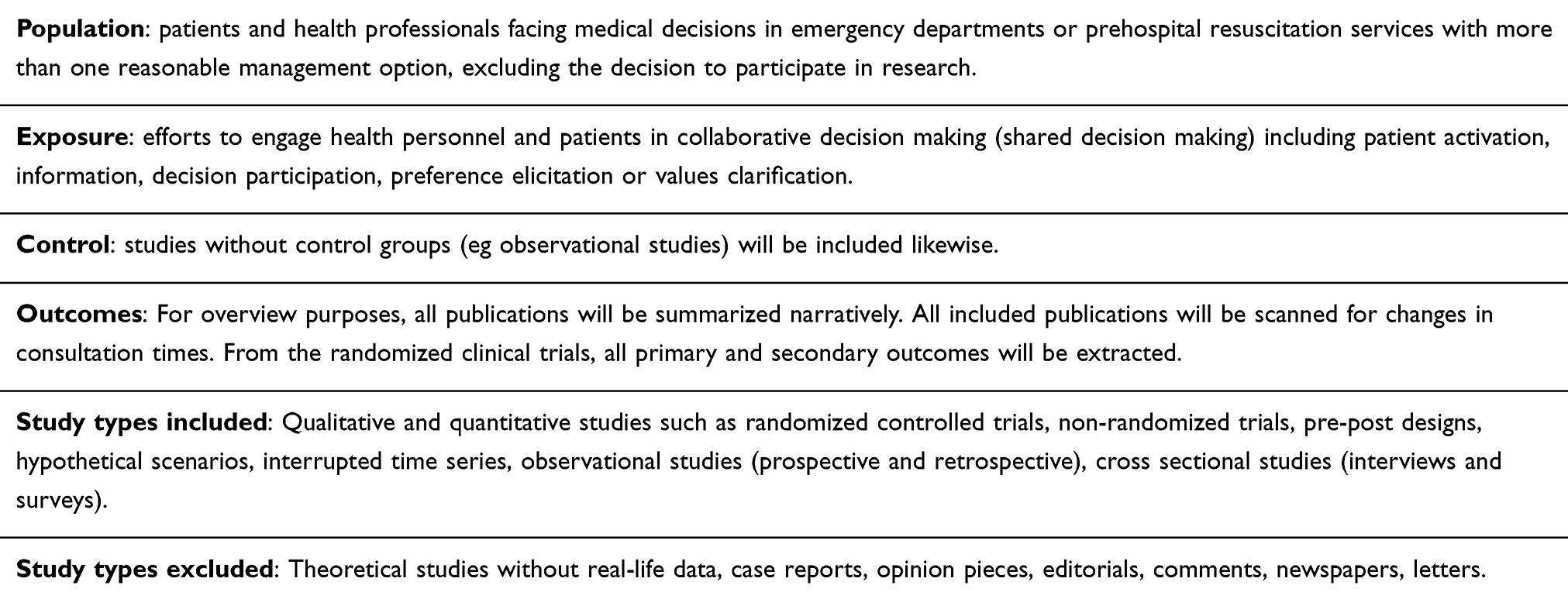 |
Box 1 PECOS-Scheme |
Two researchers (FW and DL) independently screened titles and abstracts for eligibility without automation tools. In case of discrepancies, a third author (FS) arbitrated. The same three researchers appraised the articles’ full texts afterward.
Data Charting Process and Data Items
One author (FW) extracted data from the included studies. First, on all publications, basic information was retrieved, including first author, publication date, country, topic, participant numbers, study design and a short narrative summary of the authors’ conclusions. Second, all included publications were scanned in full text for the effects of SDM on consultation times in EM. The average consultation times were extracted alongside the standard deviation and p-values. Third, all outcomes from the RCTs were collected and their results stated according to the authors’ conclusions. RCTs were chosen as the only source for outcome results as their design offers a solid level of scientific validity.
All extracted data were visualized in separate forms created in a word processing program (Microsoft Word). Compared to the initial study protocol, these sheets received modifications during the extraction process.
Synthesis of Results
For overview purposes, five major study design categories were defined: (1) observational (including interviews, surveys, etc).; (2) development and implementation reports; (3) non-randomized interventions and hypothetical scenarios; (4) randomized interventions and their secondary analyses; (5) literature reviews; (6) mixed methods designs. Each publication was sorted into one category and results were visualized in a hierarchical figure. Apart from that, the countries were displayed on a world map. Lastly, the results from RCTs alongside effects on consultation times were summarized in tables.
The resulting tables and figures were critically appraised and discussed within the author group, respecting all included publications. Results were described narratively. Neither meta-analysis nor statistical evaluation were performed.
Results
Selection of Sources of Evidence
The search strategy yielded 3954 hits, of which 3428 remained after duplicate removal. Sorting out 3359 of them during title- and abstract screening and 10 during full-text appraisal left 59 publications for data extraction. On the other hand, 8 publications were added by searching through the included publications’ reference lists or by research group remarks.16,34,46,55,56,59,68,76 This process resulted in a total of 67 publications included in further data synthesis (Figure 1).9,10,12,16–79 All articles removed during full-text appraisal are listed in the supplementary material.80–89
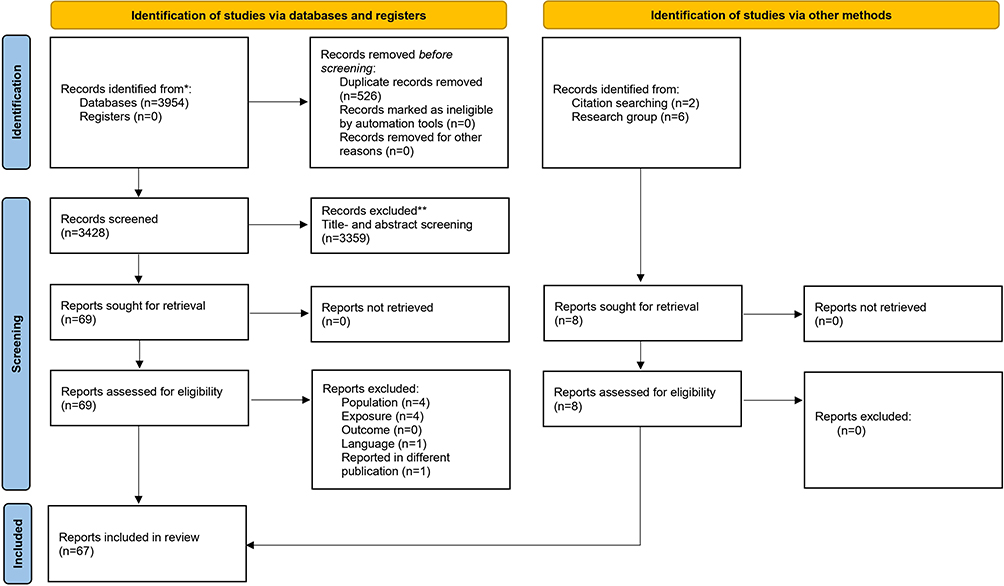 |
Figure 1 Adapted search flow diagram following the PRISMA 2020 statements. Notes: PRISMA figure adapted from Tricco AC, Lillie E, Zarin W et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018 Oct 2;169(7):467–473. doi: 10.7326/M18-0850. Epub 2018 Sep 4. PMID: 30178033. Creative Commons.13 |
Characteristics and Results of Sources of Evidence
All included publications are listed in Table 1. As for study designs, 27 publications are of observational design and 12 publications report on developments or implementations of interventions, teaching programs or tools to measure SDM. Furthermore, 10 publications depict hypothetical scenarios or non-randomized interventions. Aside, 4 publications utilize mixed-method designs. An additional 6 publications report on randomized contorlled trials and 4 on secondary analyses of those RCTs. Lastly, 4 publications are literature reviews (Figure 2).
 |
Table 1 Included Publications |
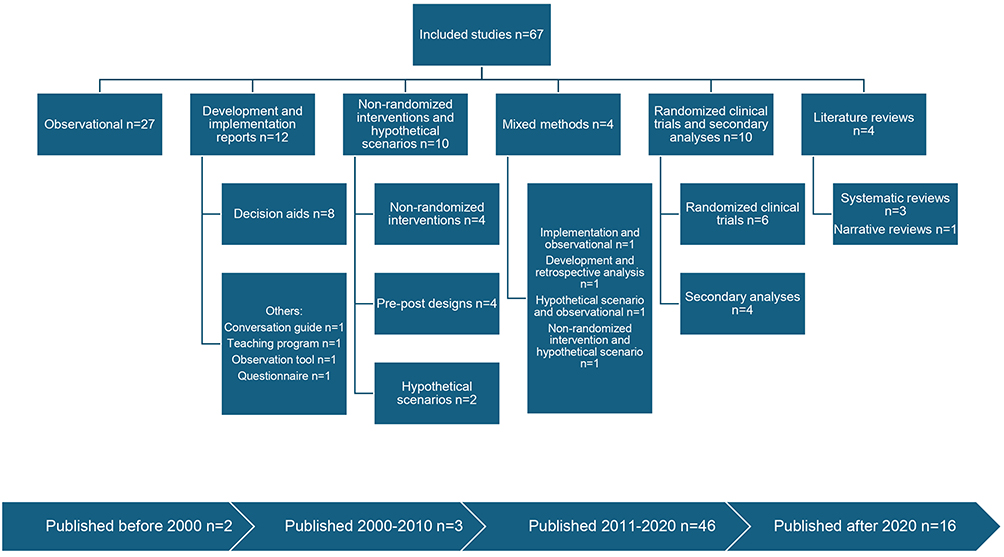 |
Figure 2 Designs and publication dates of included studies. |
Looking at geographic distributions, 50 of the 67 publications originate from the USA and 9 from Nordic countries (Norway 1, Denmark 2, Sweden 6). Germany, the UK, Canada and Taiwan all contribute 1 article each. The remaining reports (4) are literature reviews (Figure 3). As for publication dates, 2 articles were published before 2000, 3 between 2000 and 2010, 46 between 2011 and 2020 and 16 after 2020. Different topics are depicted in the studies, ranging from general perceptions of SDM by patients71 and healthcare providers12 over deciding between different treatment options (eg oral vs venous rehydration in children with vomiting and diarrhea)55 up to medication decisions in older patients.31 Study participant numbers range from n=936 to n=13445.40
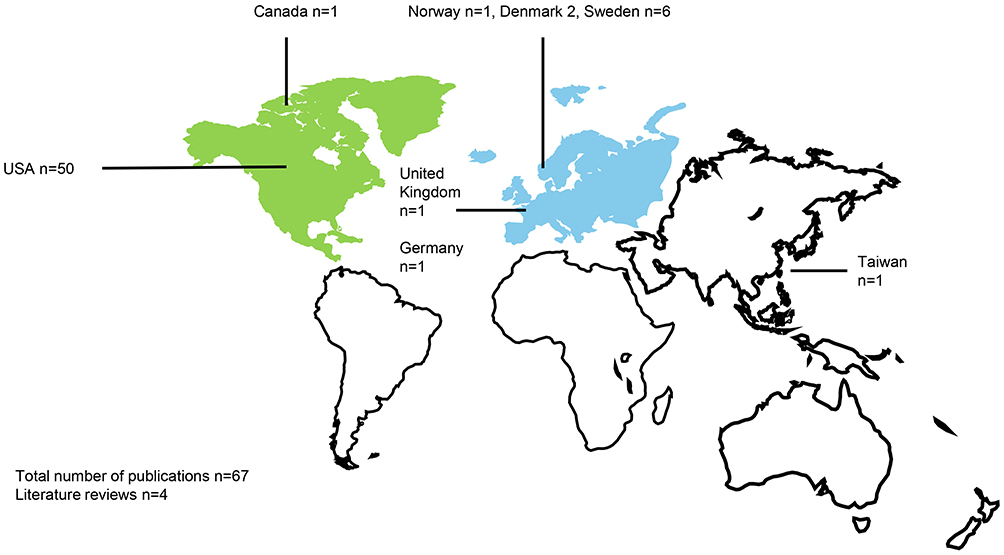 |
Figure 3 Publications sorted by country. |
All outcomes in the 6 RCTs44–46,59,61,65 were extracted and appraised, following the authors’ conclusions (Table 2). Apart from patient-reported outcome measures (PROMs),44–46,59,61,65 studies examined effects on resource utilization rates,44–46,59,61,65 clinical outcomes59,61 and patient safety.44–46,59,65 These outcome effects are reported with heterogeneous effects – ranging from no effect to improvements. While clinical outcomes and patient safety are described as not being affected, the results for PROMs and resource utilization rates differ between improvement and no change. No declines are reported.
 |
Table 2 Outcome Effects in Randomized Clinical Trials on Shared Decision Making in Emergency Medicine According to Authors’ Conclusions |
Respecting all 67 included studies for estimates of discussion time modifications through SDM suggests an average increase of 2 minutes in 3 randomized trials.44,45,65 Another study (decision aid development report)34 solely reported on how long participants spent with the developed information material (Table 3).
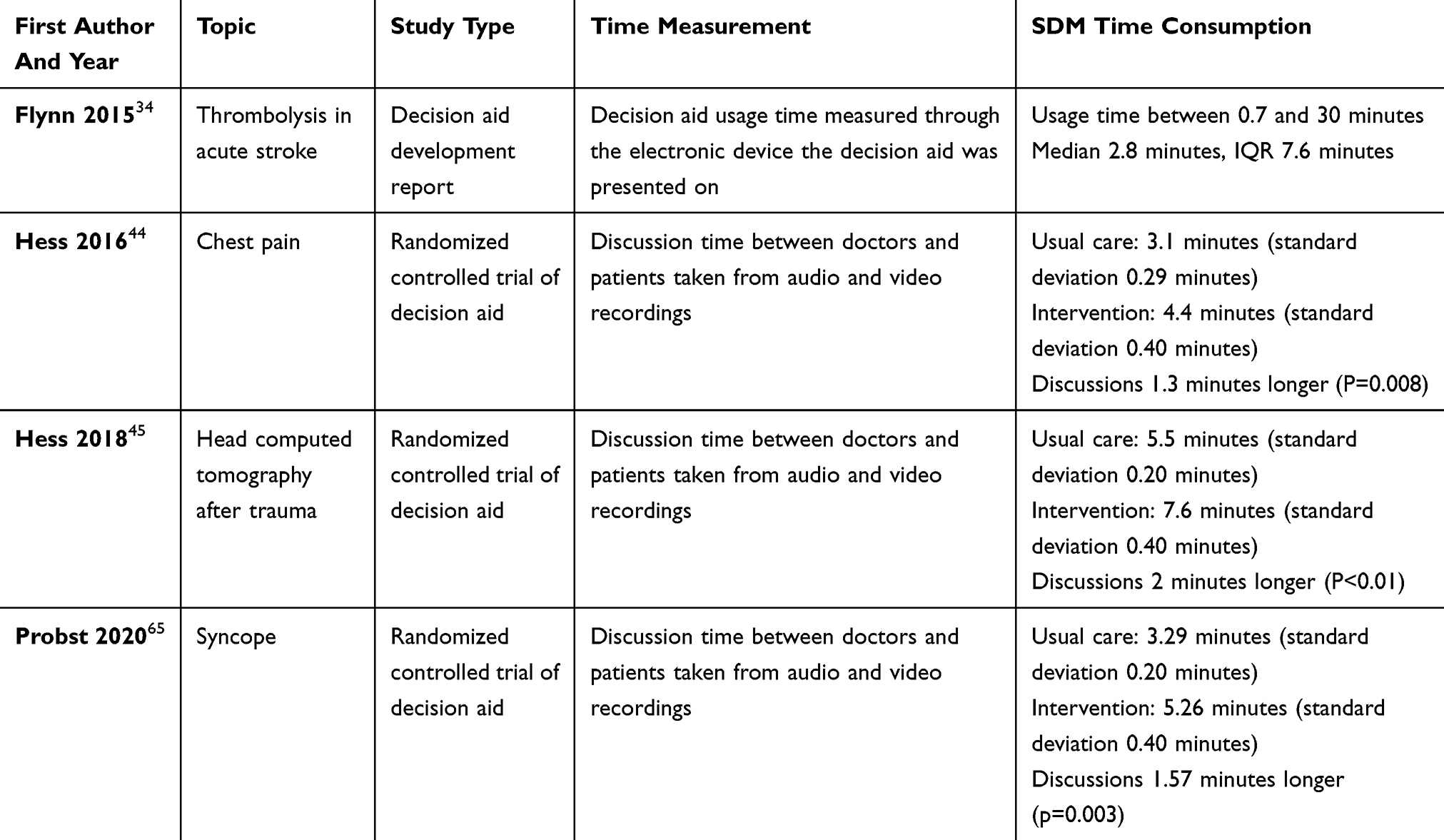 |
Table 3 Effects of Shared Decision Making Interventions on Consultation Times in Emergency Medicine |
Discussion
Summary of Evidence
This scoping review includes 67 publications reporting qualitative and/or quantitative data on SDM in EM.9,10,12,16–79 They utilize different observational and interventional study designs. All publications were sorted according to their study design, country and reported results. During the subsequent discussion within the author group, five annotations were phrased.
Annotation #1
Certain terms and definitions are blurry and intertwined.
Substantiation
Human communication involves language, interactions, social norms and more. The definitions and concepts around these intertwine and evolve. This also accounts for SDM.6 Looking specifically at EM, the terms informed consent, patient participation and SDM are used with different yet partially overlapping operationalizations. While Yamamoto in 1997 used the term informed consent when exposing children alongside their parents to different possible managements in fever9 or skin lacerations,10 more recent interventions by Hess in patients with nontraumatic chest pain are labeled shared decision making.44 At the same time, these publications show parallels in their intervention designs. The range in terminologies should be considered when appraising the literature, as some reports might otherwise be missed. More recent and (partially) consented concepts for SDM are described in the papers published by members of the International Shared Decision Making Society (ISDM).90 Apart from that, another potential misunderstanding occurred: the term decision aid is sometimes used to describe clinician-directed tools that assess patients’ risk profiles or illustrate management pathways.91 This is in contrast to the concept of decision aids by the ISDM. Here, decision aids depict material that informs and activates patients, supporting their decision process.92 To clarify this, future interventions could utilize the term shared decision making aid.
Annotation #2
The available literature predominantly originates from the USA between 2011 and 2020.
Substantiation
While Denmark, Norway, Germany and Canada contribute single publications, the majority is reported from studies in the USA. In a brainstorming approach, one could postulate several reasons for explanation: a) EM is a standalone medical specialty in the USA, b) SDM is supposed to meet medicolegal and economic expectations – both important parts of emergency healthcare in the USA, c) the American emergency healthcare system might be more curious towards innovations. Definite proof of such assumptions lies beyond the scope of this review.
Annotation #3
Interventions focus on evaluating shared decision making aids.
Substantiation
While the spectrum of included topics varies, shared decision making aids depict the preponderant part of evaluated interventions – apart from one training program for residents.54 Decision aids are evidence-supported information and activation sources assisting patients throughout the decision process. Their focus lies in enabling the patient to make medical decisions that are in line with existing needs and predilections (preference sensitivity). The existing IPDAS-criteria frame methodologies around decision aid development.82 An extensive Cochrane review revealed the potential of decision aids to positively influence various aspects of healthcare.93
Annotation #4
Few randomized SDM interventions have been enrolled. They exclude high-risk patients and suggest potential reductions in healthcare resource utilization in certain patient groups.
Substantiation
A total of 6 publications, plus additional secondary analyses, report on RCTs evaluating shared decision making aids. While their effects on patient-reported outcome measures differ, 3 studies around chest pain44,46 and head computed tomography45 highlight potential reductions in resource utilization without affecting patients’ safety. This is also described in the most recent meta-analysis by Ubbink et al.11 It should be noted that these results are limited to patients with certain leading symptoms and low to intermediate risk profiles. One might insinuate that such low-risk patients probably receive overdiagnosis, which could safely be omitted, or, through SDM, collaboratively prevented. While all randomized interventions currently originate from the USA using shared decision making aids, there might be different outcome effects in future, multimodal interventions from other countries.
Annotation #5
The effects on consultation times appear debatable.
Substantiation
As for quantitative aspects, the existing trials suggest an increase of about two minutes on average.44,45,65 However, this should not be deemed a certainty at this point. Discussion times were measured after intervention implementation and clinicians probably had to adapt to the concepts of SDM. In the long term, the increase in discussion times could be reversed. Here, long-term data is missing. Furthermore, avoiding one hospital admission in a patient with nontraumatic chest pain includes a greater reduction in resource utilization than two additional minutes in discussion times poses an increase. Apart from these economic evaluations, one might even ask whether increasing patients’ autonomy and participation justifies increased consultation times (qualitative vs quantitative aspects of time).94
Respecting these five annotations led to a range of potential implications for future research around SDM in EM (Box 2). They include new concepts for patients’ SDM-feasibility, training programs for clinicians, measurement tools and implementation through complex interventions that demonstrated efficacy outside the emergency context.95
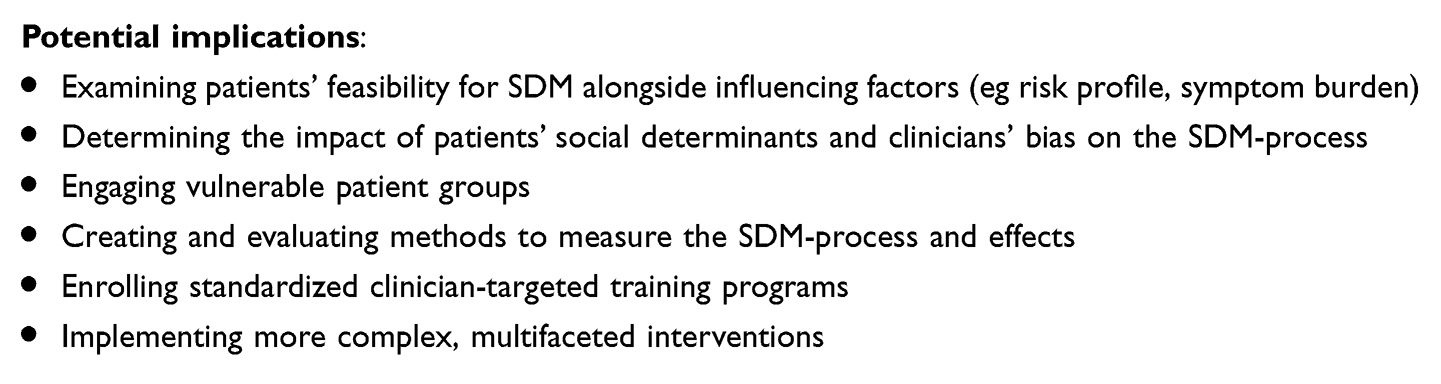 |
Box 2 Implications for Future Research Around Shared Decision Making in Emergency Medicine |
Limitations
Although a broad search strategy was installed using different terms and databases, some existing publications might have been missed. This is due to the different labeling of interventions (like shared decision making, patient-centered care, informed consent, decision support, patient participation …). These intertwingled terms depict dynamic concepts with evolving definitions and understandings. Also, some studies were excluded as their subjects greatly differed from the idea that SDM requires more than one reasonable management option. Here, one cannot argue with definite certainty as to what studies to in- or exclude. As for now, the most comprehensive definition of SDM could be seen in the consensus papers of the International Shared Decision Making Society80 and officially validated frameworks such as the IPDAS criteria.82
Apart from these inaccuracies around the concepts of SDM, it is even debatable where EM begins. In this article, it is operationalized as happening in EDs or rescue services. Yet, there are also interventions aimed at primary care practices where patients present with acute problems. This would result in a greater number of studies being included. However, it appears reasonable to define EM as happening in EDs and resuscitation services, as both are scientifically targetable organizational structures.
Lastly, two limitations should be noted. While readers find a comprehensive overview of the current state of literature on SDM in EM, no meta-analysis or statistical evaluations were performed. Therefore, definite certainty in the quantitative estimates is not given, although the narrative results in this review predominantly match with the meta-analysis by Ubbink et al.11 Lastly, data extraction was performed by a single researcher, potentially enabling bias. However, results were appraised and discussed within the author group afterwards.
Conclusions
Through a scoping review approach, five remarks on the current literature around SDM in EM were stipulated: First, the underlying terms and definitions hold partially varying and evolving terminologies. Second, most studies originate from the USA between 2011 and 2020 and utilize observational study designs. Third, interventional studies focus on evaluating shared decision making aids. Fourth, randomized trials exclude patients at high risk of serious conditions or adverse events. Utilizing SDM for diagnostic and disposition decisions in low to moderate-risk patients with nontraumatic chest pain reduced resource utilization while not affecting patient safety. The number of randomized trials is yet limited. Fifth, consultation times in EM were prolonged through SDM by about two minutes on average, although qualitative aspects of time might diminish this prolongation. Future research projects could include more extensive implementation through complex interventions or more differentiated concepts around patients’ feasibility for SDM.
Abbreviations
ED, Emergency department; EM, Emergency Medicine; SDM, Shared decision making; RCT, Randomized controlled trial; PROM, Patient-reported outcome measure
Data Sharing Statement
The study protocol and reference manager dataset are accessible through a data repository within the Open Science Framework (https://doi.org/10.17605/OSF.IO/CA7XU).14
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Disclosure
FW, FG, FS and CSK were members of the special project “MAKING SHARED DECISION MAKING A REALITY” which was funded by the German Federal Joint Committee (funding code: 01NVF17009). FG and FS are founders and shareholders of the “SHARE TO CARE GmbH”. Friedemann Geiger reports grants from German Innovation Fund and EU outside the submitted work. Fueloep Scheibler reports grants from Innovation Fund and Drug Companies outside the submitted work. Constanze Stolz-Klingenberg reports personal fees from Biomarin Pharmaceutical, Alexion Pharma Germany and Almirall Hermal outside the submitted work. Apart from that, other authors declare no competing interests.
References
1. Sandman L, Munthe C. Shared decision-making and patient autonomy. Theor Med Bioeth. 2009;30(4):289–310. doi:10.1007/s11017-009-9114-4
2. Wehking F, Debrouwere M, Danner M, et al. Impact of shared decision making on healthcare in recent literature: a scoping review using a novel taxonomy. J Public Health. 2024;32:2255–2266. doi:10.1007/s10389-023-01962-w
3. Deniz S, Akbolat M, Çimen M, Unal O. The mediating role of shared decision-making in the effect of the patient-physician relationship on compliance with treatment. J Patient Exp. 2021;8:23743735211018066. doi:10.1177/23743735211018066
4. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–692. doi:10.1016/S0277-9536(96)00221-3
5. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
6. Páez G, Forte DN, Gabeiras MDPL. Exploring the relationship between shared decision-making, patient-centered medicine, and evidence-based medicine. Linacre Q. 2021;88(3):272–280. doi:10.1177/00243639211018355
7. Clayman ML, Scheibler F, Rüffer JU, Wehkamp K, Geiger F. The six steps of SDM: linking theory to practice, measurement and implementation. BMJ Evid Based Med. 2024;29(2):75–78. doi:10.1136/bmjebm-2023-112289
8. Probst MA, Kanzaria HK, Schoenfeld EM, et al. Shared decisionmaking in the emergency department: a guiding framework for clinicians. Ann Emerg Med. 2017;70(5):688–695. doi:10.1016/j.annemergmed.2017.03.063
9. Yamamoto LG. Application of informed consent principles in the emergency department evaluation of febrile children at risk for occult bacteremia. Hawaii Med J 1997;56:313–7,20–2.
10. Yamamoto LG, Young LL, Roberts JL. Informed consent and parental choice of anesthesia and sedation for the repair of small lacerations in children. Am J Emerg Med 1997;15:285–289. doi:10.1016/S0735-6757(97)90017-6
11. Ubbink DT, Matthijssen M, Lemrini S, van Etten-Jamaludin FS, Bloemers FW. Systematic review of barriers, facilitators, and tools to promote shared decision making in the emergency department. Acad Emerg Med. 2024;31(10):1037–1049. doi:10.1111/acem.14998
12. Schoenfeld EM, Goff SL, Elia TR, et al. Physician-identified barriers to and facilitators of shared decision-making in the emergency department: an exploratory analysis. Emerg Med J. 2019;36(6):346–354. doi:10.1136/emermed-2018-208242
13. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
14. Wehking F. Scoping review about the current state of shared decision making in emergency departments. OSF. 2024. doi:10.17605/OSF.IO/CA7XU
15. Morgan RL, Whaley P, Thayer KA, Schünemann HJ. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018;121(Pt 1), 1027–1031. doi:10.1016/j.envint.2018.07.015
16. Anderson JL, Oliveira JESL, Brito JP, Hargraves IG, Hess EP. Development of an electronic conversation aid to support shared decision making for children with acute otitis media. JAMIA Open. 2021;4(2):ooab024. doi:10.1093/jamiaopen/ooab024
17. Aronson PL, Politi MC, Schaeffer P, et al. Development of an app to facilitate communication and shared decision-making with parents of febrile infants ≤ 60 days old. Acad Emerg Med. 2021;28(1):46–59. doi:10.1111/acem.14082
18. Aronson PL, Schaeffer P, Fraenkel L, Shapiro ED, Niccolai LM. Physicians’ and nurses’ perspectives on the decision to perform lumbar punctures on febrile infants ≤8 weeks old. Hosp Pediatr. 2019;9(6):405–414. doi:10.1542/hpeds.2019-0002
19. Aronson PL, Schaeffer P, Niccolai LM, Shapiro ED, Fraenkel L. Parents’ perspectives on communication and shared decision making for febrile infants ≤60 days old. Pediatr Emerg Care. 2021;37(12):e1213–e1219. doi:10.1097/PEC.0000000000001977
20. Aronson PL, Schaeffer P, Ponce KA, et al. Stakeholder perspectives on hospitalization decisions and shared decision-making in bronchiolitis. Hosp Pediatr. 2022;12(5):473–482. doi:10.1542/hpeds.2021-006475
21. Aronson PL, Shapiro ED, Niccolai LM, Fraenkel L. Shared decision-making with parents of acutely ill children: a narrative review. Acad Pediatr. 2018;18(1):3–7. doi:10.1016/j.acap.2017.06.009
22. Barnes GD, Izzo B, Conte ML, Chopra V, Holbrook A, Fagerlin A. Use of decision aids for shared decision making in venous thromboembolism: a systematic review. Thromb Res. 2016;143:71–75. doi:10.1016/j.thromres.2016.05.009
23. Bean G, Krishnan U, Stone JR, Khan M, Silva A. Utilization of chest pain decision aids in a community hospital emergency department: a mixed-methods implementation study. Crit Pathw Cardiol. 2021;20(4):192–207. doi:10.1097/HPC.0000000000000269
24. Billah T, Gordon L, Schoenfeld EM, Chang BP, Hess EP, Probst MA. Clinicians’ perspectives on the implementation of patient decision aids in the emergency department: a qualitative interview study. J Am Coll Emerg Physicians Open. 2022;3(1)e12629. doi:10.1002/emp2.12629
25. Chartash D, Sharifi M, Emerson B, et al. Documentation of shared decisionmaking in the emergency department. Ann Emerg Med. 2021;78(5):637–649. doi:10.1016/j.annemergmed.2021.04.038
26. Coronado-Vázquez V, Gómez-Salgado J, Cerezo-Espinosa de Los Monteros J, García-Colinas MA. Shared decision-support tools in hospital emergency departments: a systematic review. J Emerg Nurs. 2019;45(4):386–393. doi:10.1016/j.jen.2019.01.002
27. Cullison K, Carpenter CR, Milne WK. Hot off the press: use of shared decision-making for management of acute musculoskeletal pain in older adults discharged from the emergency department. Acad Emerg Med. 2016;23(8):956–958. doi:10.1111/acem.12985
28. Dubois H, Creutzfeldt J, Manser T. Behavioural observation tool for patient involvement and collaboration in emergency care teams (PIC-ET-tool). BMC Emerg Med. 2023;23(1):74. doi:10.1186/s12873-023-00841-7
29. Dyrstad DN, Testad I, Storm M. Older patients’ participation in hospital admissions through the emergency department: an interview study of healthcare professionals. BMC Health Serv Res. 2015;15:475. doi:10.1186/s12913-015-1136-1
30. Eriksson‐Liebon M, Roos S, Hellström I. Patients’ expectations and experiences of being involved in their own care in the emergency department: a qualitative interview study. J Clin Nurs. 2021;30(13–14):1942–1952. doi:10.1111/jocn.15746
31. Fabricius PK, Aharaz A, Stefánsdóttir NT, et al. Shared decision making with acutely hospitalized, older poly-medicated patients: a mixed-methods study in an emergency department. Int J Environ Res Public Health. 2022;19(11):6429. doi:10.3390/ijerph19116429
32. Fabricius PK, Andersen O, Steffensen KD, Kirk JW. The challenge of involving old patients with polypharmacy in their medication during hospitalization in a medical emergency department: an ethnographic study. PLoS One. 2021;16(12):e0261525. doi:10.1371/journal.pone.0261525
33. Flynn D, Knoedler MA, Hess EP, et al. Engaging patients in health care decisions in the emergency department through shared decision-making: a systematic review. Acad Emerg Med. 2012;19(8):959–967. doi:10.1111/j.1553-2712.2012.01414.x
34. Flynn D, Nesbitt DJ, Ford GA, et al. Development of a computerised decision aid for thrombolysis in acute stroke care. BMC Med Inform Decis Mak. 2015;15:6. doi:10.1186/s12911-014-0127-1
35. Frank C, Asp M, Dahlberg K. Patient participation in emergency care - a phenomenographic analysis of caregivers’ conceptions. J Clin Nurs. 2009;18(18):2555–2562. doi:10.1111/j.1365-2702.2008.02477.x
36. Frank C, Asp M, Dahlberg K. Patient participation in emergency care - a phenomenographic study based on patients’ lived experience. Int Emerg Nurs. 2009;17(1):15–22. doi:10.1016/j.ienj.2008.09.003
37. Frank C, Asp M, Fridlund B, Baigi A. Questionnaire for patient participation in emergency departments: development and psychometric testing. J Adv Nurs. 2011;67(3):643–651. doi:10.1111/j.1365-2648.2010.05472.x
38. Frank C, Fridlund B, Baigi A, Asp M. Patient participation in the emergency department: an evaluation using a specific instrument to measure patient participation (PPED). J Adv Nurs. 2011;67(4):728–735. doi:10.1111/j.1365-2648.2010.05524.x
39. Freeman P, Couperus K, Walsh R, Ward MJ, McNaughton CD, Bothwell J. “Your finger or mine?”-Patient preferences in the collection of fecal occult blood testing in the emergency department. Mil Med. 2020;185(9–10):e1393–e1396. doi:10.1093/milmed/usz429
40. Gafni-Pappas G, DeMeester SD, Boyd MA, et al. The HAS-Choice study: utilizing the HEART score, an ADP, and shared decision-making to decrease admissions in chest pain patients. Am J Emerg Med. 2018;36(10):1825–1831.
41. George WM, Steidl S, Papke J, Wiese CHR. Decision support for emergency physicians in the care of patients at the end of life. Notarzt. 2022;38(01):28–35.
42. Geyer BC, Xu M, Kabrhel C. Patient preferences for testing for pulmonary embolism in the ED using a shared decision-making model. Am J Emerg Med. 2014;32(3):233–236. doi:10.1016/j.ajem.2013.11.019
43. Hadden KB, McLemore H, White W, Marks MH, Gan JM, Seupaul RA. Implementation of a health-literate patient decision aid for chest pain in the emergency department. Patient Educ Couns. 2020;103(4):864–869. doi:10.1016/j.pec.2019.11.009
44. Hess EP, Hollander JE, Schaffer JT, et al. Shared decision making in patients with low risk chest pain: prospective randomized pragmatic trial. BMJ. 2016;355
45. Hess EP, Homme JL, Kharbanda AB, et al. Effect of the head computed tomography choice decision aid in parents of children with minor head trauma: a cluster randomized trial. JAMA Network Open. 2018;1(5):e182430. doi:10.1001/jamanetworkopen.2018.2430
46. Hess EP, Knoedler MA, Shah ND, et al. The chest pain choice decision aid: a randomized trial. Circ Cardiovasc Qual Outcomes. 2012;5(3):251–259. doi:10.1161/CIRCOUTCOMES.111.964791
47. Holland WC, Hunold KM, Mangipudi SA, Rittenberg AM, Yosipovitch N, Platts-Mills TF. A prospective evaluation of shared decision-making regarding analgesics selection for older emergency department patients with acute musculoskeletal pain. Acad Emerg Med. 2016;23(3):306–314. doi:10.1111/acem.12888
48. Hull A, Friedman T, Christianson H, Moore G, Walsh R, Wills B. Risk acceptance and desire for shared decision making in pediatric computed tomography scans: a survey of 350. Pediatr Emerg Care. 2015;31(11):759–761. doi:10.1097/PEC.0000000000000467
49. Hung CH, Lee YH, Lee DC, Chang YP, Chow CC. The mediating and moderating effects of shared decision making and medical autonomy on improving medical service satisfaction in emergency observation units. Int Emerg Nurs. 2022;60:101101. doi:10.1016/j.ienj.2021.101101
50. Ijaz H, Michel C, Kulie PE, Richards LM, Meltzer AC. Patient preference to participate in shared decision making for performing a CT scan in the emergency department. Am J Emerg Med. 2017;35(12):1969–1970. doi:10.1016/j.ajem.2017.06.020
51. Ijaz H, Wong C, Weaver J, et al. Exploring the attitudes & practices of shared decision-making for CT scan use in emergency department patients with abdominal pain. Am J Emergency Med. 2018;36(12):2263–2267. doi:10.1016/j.ajem.2018.09.029
52. Isaacs CG, Kistler C, Hunold KM, et al. Shared decision‐making in the selection of outpatient analgesics for older individuals in the emergency department. J Am Geriatr Soc. 2013;61(5):793–798. doi:10.1111/jgs.12207
53. Kanzaria HK, Brook RH, Probst MA, Harris D, Berry SH, Hoffman JR. Emergency physician perceptions of shared decision-making. Acad Emerg Med. 2015;22(4):399–405. doi:10.1111/acem.12627
54. Kanzaria HK, Chen EH. Shared decision making for the emergency provider: engaging patients when seconds count. MedEdPORTAL. 2020;16:10936. doi:10.15766/mep_2374-8265.10936
55. Karpas A, Finkelstein M, Reid S. Parental preference for rehydration method for children in the emergency department. Pediatr Emerg Care. 2009;25(5):301–306. doi:10.1097/PEC.0b013e3181a34144
56. Karpas A, Finkelstein M, Reid S. Which management strategy do parents prefer for their head-injured child: immediate computed tomography scan or observation? Pediatr Emerg Care. 2013;29(1):30–35. doi:10.1097/PEC.0b013e31827b5090
57. Melnick ER, Hess EP, Guo G, et al. Patient-centered decision support: formative usability evaluation of integrated clinical decision support with a patient decision aid for minor head injury in the emergency department. J Med Internet Res. 2017;19(5):e174. doi:10.2196/jmir.7846
58. Merck LH, Ward LA, Applegate KE, Choo E, Lowery-North DW, Heilpern KL. Written informed consent for computed tomography of the abdomen/pelvis is associated with decreased CT utilization in low-risk emergency department patients. West J Emerg Med. 2015;16(7):1014–1024. doi:10.5811/westjem.2015.9.27612
59. Minneci PC, Cooper JN, Leonhart K, et al. Effects of a patient activation tool on decision making between surgery and nonoperative management for pediatric appendicitis: a randomized clinical trial. JAMA Network Open. 2019;2(6):e195009. doi:10.1001/jamanetworkopen.2019.5009
60. Obadeyi O, Baffoe N, Paxton J. A patient’s decision aid for vascular access placement in the emergency department. J Vasc Access. 2020;21(4):419–425. doi:10.1177/1129729819879828
61. Omaki E, Castillo R, McDonald E, et al. A patient decision aid for prescribing pain medication: results from a pilot test in two emergency departments. Patient Educ Couns. 2021;104(6):1304–1311. doi:10.1016/j.pec.2020.11.022
62. Poitras M-E, Légaré F, Tremblay Vaillancourt V, et al. High users of healthcare services: development and alpha testing of a patient decision aid for case management. Patient. 2020;13(6):757–766. doi:10.1007/s40271-020-00465-0
63. Probst MA, Hess EP, Breslin M, et al. Development of a patient decision aid for syncope in the emergency department: the SynDA tool. Acad Emerg Med. 2018;25(4):425–433. doi:10.1111/acem.13373
64. Probst MA, Kanzaria HK, Frosch DL, et al. Perceived appropriateness of shared decision-making in the emergency department: a survey study. Acad Emerg Med. 2016;23(4):375–381. doi:10.1111/acem.12904
65. Probst MA, Lin MP, Sze JJ, et al. Shared decision making for syncope in the emergency department: a randomized controlled feasibility trial. J Article Acad Emerg Med. 2020;27(9):
66. Probst MA, Tschatscher CF, Lohse CM, Fernanda Bellolio M, Hess EP. Factors associated with patient involvement in emergency care decisions: a secondary analysis of the chest pain choice multicenter randomized trial. J Article Acad Emerg Med. 2018;25(10):
67. Rising KL, Hollander JE, Schaffer JT, et al. Effectiveness of a decision aid in potentially vulnerable patients: a secondary analysis of the Chest Pain Choice multicenter randomized trial. Med Decis Mak. 2018;38(1):69–78. doi:10.1177/0272989X17706363
68. Rodriguez RM, Henderson TM, Ritchie AM, et al. Patient preferences and acceptable risk for computed tomography in trauma. Injury. 2014;45(9):1345–1349. doi:10.1016/j.injury.2014.03.011
69. Rosen JE, Yang FF, Liao JM, et al. Development and feasibility testing of a decision aid for acute appendicitis. J Surg Res. 2023;289:82–89. doi:10.1016/j.jss.2023.03.028
70. Schaffer JT, Hess EP, Hollander JE, et al. Impact of a shared decision making intervention on health care utilization: a secondary analysis of the chest pain choice multicenter randomized trial. Acad Emerg Med. 2018;25(3):293–300. doi:10.1111/acem.13355
71. Schoenfeld EM, Goff SL, Downs G, Wenger RJ, Lindenauer PK, Mazor KM. A qualitative analysis of patients’ perceptions of shared decision making in the emergency department: “let me know i have a choice”. Acad Emerg Med. 2018;25(7):716–727. doi:10.1111/acem.13416
72. Schoenfeld EM, Goff SL, Elia TR, et al. The physician-as-stakeholder: an exploratory qualitative analysis of physicians’ motivations for using shared decision making in the emergency department. Acad Emerg Med. 2016;23(12):1417–1427. doi:10.1111/acem.13043
73. Schoenfeld EM, Goff SL, Elia TR, et al. A qualitative analysis of attending physicians’ use of shared decision-making: implications for resident education. J Grad Med Educ. 2018;10(1):43–50. doi:10.4300/JGME-D-17-00318.1
74. Schoenfeld EM, Houghton C, Patel PM, et al. Shared decision making in patients with suspected uncomplicated ureterolithiasis: a decision aid development study. Acad Emerg Med. 2020;27(7):554–565. doi:10.1111/acem.13917
75. Schoenfeld EM, Kanzaria HK, Quigley DD, et al. Patient preferences regarding shared decision making in the emergency department: findings from a multisite survey. Acad Emergency Med. 2018;25(10):1118–1128. doi:10.1111/acem.13499
76. Schoenfeld EM, Mader S, Houghton C, et al. The effect of shared decisionmaking on patients’ likelihood of filing a complaint or lawsuit: a simulation study. Ann Emerg Med. 2019;74(1):126–136. doi:10.1016/j.annemergmed.2018.11.017
77. Schoenfeld EM, Probst MA, Quigley DD, et al. Does shared decision making actually occur in the emergency department? looking at it from the patients’ perspective. Acad Emerg Med. 2019;26(12):1369–1378. doi:10.1111/acem.13850
78. Skains RM, Kuppermann N, Homme JL, et al. What is the effect of a decision aid in potentially vulnerable parents? Insights from the head CT choice randomized trial. Health Expectations. 2020;23(1):63–74. doi:10.1111/hex.12965
79. Walker LE, Bellolio MF, Dobler CC, et al. Paths of emergency department care: development of a decision aid to facilitate shared decision making in goals of care discussions in the acute setting. MDM Policy Pract. 2021;6(2)23814683211058082. doi:10.1177/23814683211058082
80. Alqaydi A, Williams E, Nanji S, Zevin B. Optimizing the consent process for emergent laparoscopic cholecystectomy using an interactive digital education platform: a randomized control trial. Surg Endosc. 2024;38(5):2593–2601. doi:10.1007/s00464-024-10775-1
81. Cardy C, Ardisson KM, Widmar SB. Atrial fibrillation clinical decision aid for emergency medicine providers: an initiative to improve quality healthcare outcomes in adults with new-onset atrial fibrillation. Heart Lung. 2018;47(4):314–321. doi:10.1016/j.hrtlng.2018.05.007
82. Chesney T, Devon K. Training surgical residents to use a framework to promote shared decision-making for patients with poor prognosis experiencing surgical emergencies. Can J Surg. 2018;61(2):114–120. doi:10.1503/cjs.011317
83. Cobianchi L, Dal Mas F, Agnoletti V, et al. Time for a paradigm shift in shared decision-making in trauma and emergency surgery? Results from an international survey. World J Emerg Surg. 2023;18(1)14. doi:10.1186/s13017-022-00464-6
84. Coronado-Vázquez V, Navarro-Abal Y, Magallón-Botaya R, et al. Aplicabilidad de las herramientas de ayuda a la toma de decisiones compartidas en los servicios de Urgencias: una revisión exploratoria [Applicability of decision aids in emergency departments: an exploratory review]. Rev Esp Salud Publica. 2019;93.
85. Couët N, Desroches S, Robitaille H, et al. Assessments of the extent to which health‐care providers involve patients in decision making: a systematic review of studies using the OPTION instrument. Health Expectations. 2015;18(4):542–561. doi:10.1111/hex.12054
86. Dale J, Sandhu H, Lall R, Glucksman E. The patient, the doctor and the emergency department: a cross-sectional study of patient-centredness in 1990 and 2005. Patient Educ Couns. 2008;72(2):320–329. doi:10.1016/j.pec.2008.02.005
87. Gehi AK, Armbruster T, Walker J, et al. Implementation of an atrial fibrillation decision aid care pathway in the emergency department reduces atrial fibrillation hospitalizations. Circ Cardiovasc Qual Outcomes. 2023;16(9):e009808. doi:10.1161/CIRCOUTCOMES.122.009808
88. Griffey RT, Probst MA, Tschatscher CF, Fernanda Bellolio M, Hess EP, Lohse CM. Factors associated with patient involvement in emergency care decisions: a secondary analysis of the chest pain choice multicenter randomized trial. J Article Acad Emerg Med. 2018;25(10):
89. Höglund AT, Winblad U, Arnetz B, Arnetz JE. Patient participation during hospitalization for myocardial infarction: perceptions among patients and personnel. Scand J Caring Sci. 2010;24(3):482–489. doi:10.1111/j.1471-6712.2009.00738.x
90. Bravo P, Härter M, McCaffery K, Giguère A, Hahlweg P, Elwyn G. Editorial: 20 years after the start of international Shared Decision-Making activities: is it time to celebrate? Probably…. Z Evid Fortbild Qual Gesundhwes. 2022;171:1–4. doi:10.1016/j.zefq.2022.05.009
91. Kanzaria HK, Chen EH. (2020). “Shared decision making for the emergency provider: engaging patients when seconds count.” MedEdPORTAL 16: 10936.
92. Stacey D, Volk RJ; IPDAS Evidence Update Leads (Hilary Bekker,Karina Dahl Steffensen,Tammy C.Hoffmann,Kirsten McCaffery,Rachel Thompson,Richard Thomson,Lyndal Trevena,Trudy van der Weijden, and Holly Witteman). The international patient decision aid standards (IPDAS) collaboration: evidence update 2.0. Med Decis Making. 2021;41(7):729–733. doi:10.1177/0272989X211035681
93. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):CD001431. doi:10.1002/14651858.CD001431.pub5
94. Yahanda AT, Mozersky J. What’s the role of time in shared decision making? AMA J Ethics. 2020;22(5):E416–E422.
95. Geiger F, Novelli A, Berg D, et al. The hospital-wide implementation of shared decision-making–initial findings of the kiel share to care program Dtsch Arztebl Int. 2021;118(13):225–226.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.