Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
CHA2DS2-VASc Score Predicts Prognosis in Patients with Acute Coronary Syndrome without Atrial Fibrillation Undergoing Percutaneous Coronary Intervention
Authors Long X, Jin Q, Jiang L, Chen R, Hu L
Received 1 August 2025
Accepted for publication 25 October 2025
Published 25 November 2025 Volume 2025:21 Pages 1595—1602
DOI https://doi.org/10.2147/TCRM.S551947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Xiao Long, Qiao Jin, Luping Jiang, Ran Chen, Lu Hu
Department of Cardiovascular Medicine, Changsha Central Hospital, Changsha, People’s Republic of China
Correspondence: Xiao Long, Department of Cardiovascular Medicine, Changsha Central Hospital, No. 161, Shaoshan South Road, Changsha, 410004, People’s Republic of China, Tel +86 0731 85667902, Email [email protected]
Purpose: To evaluate the prognostic value of the CHA2DS2-VASc score for 12-month major adverse cardiovascular events (MACE) in Chinese patients with acute coronary syndrome (ACS) without atrial fibrillation (AF) undergoing percutaneous coronary intervention (PCI).
Patients and Methods: This retrospective study included 992 consecutive ACS patients without AF who underwent PCI from January 2019 to December 2022. Patients were stratified into low- (0– 1), moderate- (2), and high-risk (> 2) groups based on the CHA2DS2-VASc score. The primary endpoint was MACE, defined as a composite of all-cause mortality, non-fatal myocardial infarction, and non-fatal stroke. Multivariate Cox regression was used to evaluate the association between risk groups and outcomes.
Results: During the 12-month follow-up, MACE occurred in 12.7%, 21.4%, and 28.8% of the low-, moderate-, and high-risk groups, respectively (P< 0.01). After adjusting for confounders, the CHA2DS2-VASc score remained independently associated with MACE (HR=2.27, 95% CI: 1.34– 3.86 for moderate risk; HR=3.83, 95% CI: 1.90– 7.69 for high risk; both P< 0.01).
Conclusion: The CHA2DS2-VASc score independently predicts 12-month MACE in non-AF ACS patients after PCI, with risks 2.27-fold higher in moderate-risk and 3.83-fold higher in high-risk patients compared with low-risk patients. This simple, readily available tool may help identify patients at higher risk for MACE and inform secondary prevention strategies.
Keywords: CHA2DS2-VASc score, acute coronary syndrome, percutaneous coronary intervention, major adverse cardiovascular events, risk stratification
Introduction
Acute coronary syndrome (ACS), comprising ST-segment elevation myocardial infarction (STEMI), non-STEMI (NSTEMI), and unstable angina, continues to impose a substantial burden on public health.1 Each year, an estimated 7–9 million new ACS cases occur worldwide, with incidence rising due to aging populations and lifestyle-related risk factors such as hypertension and diabetes.2 Of particular note, the China Acute Myocardial Infarction (CAMI) registry indicates that Chinese ACS patients experience significantly higher mortality rates compared to their Western counterparts, with in-hospital mortality reaching 4.9% for STEMI and 4.2% for NSTEMI.3,4 More concerningly, nearly 30% of Chinese ACS survivors experience recurrent cardiovascular events within two years, highlighting the need for more effective secondary prevention strategies.5
The CHA2DS2-VASc score, originally developed to assess stroke risk in patients with atrial fibrillation (AF), incorporates several key cardiovascular risk factors: congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke/transient ischemic attack (TIA), vascular disease, age 65–74 years, and female sex. Recently, this score has attracted interest for its potential utility in risk stratification among ACS patients.6 Unlike established ACS-specific risk models such as the Global Registry of Acute Coronary Events (GRACE), Thrombolysis In Myocardial Infarction (TIMI), or Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery (SYNTAX) scores—which require multiple laboratory, electrocardiographic, or angiographic parameters—the CHA2DS2-VASc score relies solely on routinely available clinical variables. This simplicity may make it particularly valuable in emergency or resource-limited settings where rapid risk assessment is essential.
In the Chinese ACS population, the relevance of CHA2DS2-VASc may be especially pronounced due to the high prevalence of its component risk factors. Over 50% of Chinese ACS patients have hypertension, and approximately 35% have diabetes—both exceeding global averages.7,8 Moreover, given China’s high stroke burden, 15–20% of ACS patients have a prior history of cerebrovascular events.9 These unique epidemiological features suggest that the CHA2DS2-VASc score may offer distinct prognostic value in this population, even in the absence of AF.
Therefore, this study aimed to evaluate the prognostic value of CHA2DS2-VASc score in Chinese ACS patients without AF, with particular focus on its ability to predict long-term major adverse cardiovascular events (MACE).
Materials and Methods
Patients
This retrospective study included consecutive patients diagnosed with ACS who were admitted to our hospital between January 2019 and December 2022. No selective sampling was performed. Patients were eligible for inclusion if they met the following criteria: (1) age ≥18 years; (2) diagnosis of ACS, including unstable angina, NSTEMI, or STEMI, based on clinical presentation, electrocardiography, and cardiac biomarkers; (3) no history or documented diagnosis of AF; (4) underwent percutaneous coronary intervention (PCI) during hospitalization; and (5) complete data available to calculate the CHA2DS2-VASc score at admission.
The PCI procedures were performed in accordance with standard clinical guidelines and performed by experienced interventional cardiologists with extensive expertise in coronary interventions. A loading dose of aspirin (300 mg) and either clopidogrel (300 mg) or ticagrelor (180 mg) was administered prior to the procedure, unless the patient had already received antiplatelet therapy. After PCI, all patients were prescribed lifelong aspirin and a P2Y12 inhibitor for at least 12 months. Coronary angiography and PCI were conducted using standard techniques. The procedural strategy—including pre-dilatation, stent implantation, and the choice of specific balloons or stents—was determined at the discretion of the operating cardiologist based on individual lesion characteristics and intraoperative findings.
The study was approved by the Ethics Committee of Changsha Central Hospital (approval No. 20240121). All procedures were conducted according to the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Due to its retrospective nature, informed consent was waived by the Ethics Committee of Changsha Central Hospital. All data were de-identified and handled in accordance with the Declaration of Helsinki and relevant national ethical guidelines.
Data Collection
Baseline demographic data, clinical data, medical history, and laboratory measurements were collected from the hospital’s electronic medical record system. Demographic data included age, sex, and body mass index (BMI). Clinical data included smoking status, ACS types, and left ventricular ejection fraction (LVEF). Medical history included hypertension, diabetes mellitus, dyslipidemia, prior stroke or TIA, heart failure, and documented vascular disease (including previous myocardial infarction or peripheral artery disease). Laboratory measurements included brain natriuretic peptide (BNP), lipid profile (total cholesterol, LDL-C, HDL-C, triglycerides), fasting plasma glucose (FPG), glycated hemoglobin (HbA1c), and serum creatinine.
The CHA2DS2-VASc score was calculated for all patients during the index hospitalization based on the presence of the following clinical variables: congestive heart failure or left ventricular dysfunction (1 point), hypertension (1 point), age ≥75 years (2 points), diabetes mellitus (1 point), prior stroke or transient ischemic attack (2 points), vascular disease (including prior myocardial infarction, peripheral artery disease, or aortic plaque; 1 point), age 65–74 years (1 point), and female sex (1 point). Each patient’s total score was obtained by summing the points corresponding to their individual risk factors. Patients were stratified into three groups according to their CHA2DS2-VASc score: 0–1 (low risk), 2 (moderate risk), and >2 (high risk), as applied in previous studies evaluating this score in non-AF populations.
Primary and Secondary Outcomes
The primary outcome was the occurrence of MACE within 12 months of admission, defined as a composite of all-cause mortality, non-fatal myocardial infarction, and non-fatal stroke. Secondary outcomes included individual components of MACE, specifically all-cause mortality and non-fatal stroke. Outcome data were collected through review of follow-up records and/or structured telephone interviews.
Statistical Analysis
A power analysis based on previous studies of 12-month MACE incidence indicated that the total sample of 992 patients (high-risk = 369, moderate-risk = 234, low-risk = 389) provided >90% power at a two-sided alpha level of 0.05 to detect a 10% difference in 12-month MACE incidence among groups.
Continuous variables were expressed as mean ± standard deviation (SD) and compared using one-way analysis of variance (ANOVA) across CHA2DS2-VASc score groups. Categorical variables were presented as frequencies and percentages and compared using the chi-square test or Fisher’s exact test, as appropriate. Missing covariate data were handled using multiple imputation to reduce potential bias. Patients who were lost to follow-up were censored at their last follow-up date.
Kaplan–Meier survival curves were generated for each CHA2DS2-VASc risk group, and differences were assessed using the Log rank test. Patients were censored at the time of death, loss to follow-up, or at 12 months after index admission, whichever came first. The association between the CHA2DS2-VASc score and clinical outcomes was further evaluated using multivariate Cox proportional hazards regression models, after adjusting for potential confounders including baseline demographic data, clinical data, medical history, and laboratory measurements.
All statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). A two-tailed P value of <0.05 was considered statistically significant.
Results
A total of 992 patients were included in this study; they were categorized into high- (n=369), moderate- (n=234), and low-risk (n=389) groups based on their CHA2DS2-VASc scores. The baseline characteristics of patients in the three groups are presented in Table 1. The high-risk group was significantly older, had a higher proportion of females, and lower LVEF compared to the low-risk group (P<0.01). Comorbidities such as hypertension, diabetes, prior stroke/TIA, heart failure, and vascular disease were more prevalent in the high-risk group (P<0.01). Laboratory findings showed higher BNP, fasting glucose, and HbA1c levels in the high-risk group (P<0.01), while lipid profiles and renal function were comparable across groups.
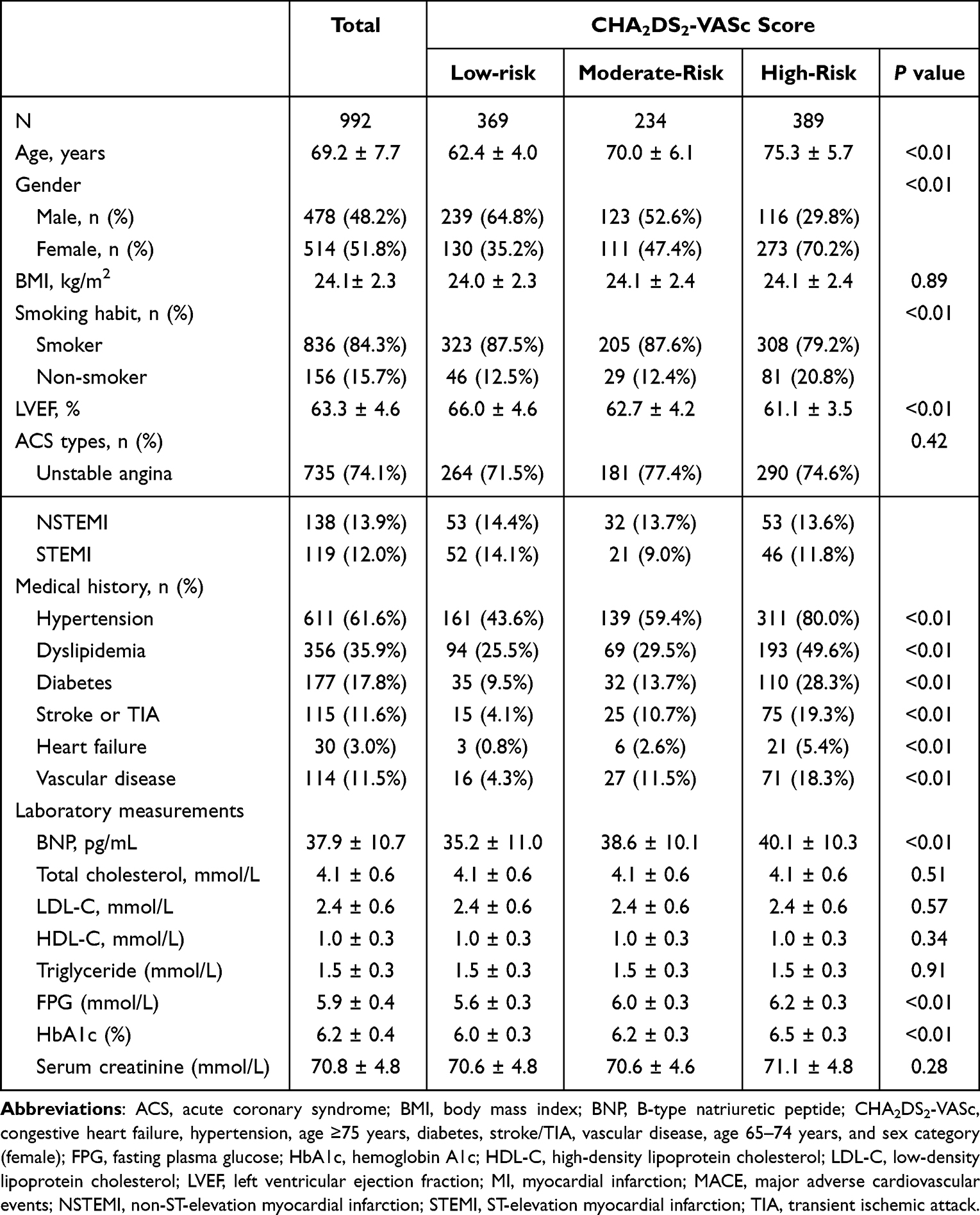 |
Table 1 Baseline Characteristics of the Study Population Stratified by CHA2DS2-VASc Score |
Among the 992 patients included, 11 (1.1%) were lost to follow-up during the 12-month period and were censored at their last follow-up date, indicating a high follow-up completeness. As shown in Figure 1, the incidence of MACE during the 12-month follow-up was significantly higher in the high-risk group (112/389, 28.8%) compared to the moderate-risk (50/234, 21.4%) and low-risk (47/369, 12.7%) groups (P<0.01). Notably, the rates of all-cause mortality (high-risk: 76/389, 19.5% vs moderate-risk: 31/234, 13.2% vs low-risk: 26/369, 7.0%; P<0.01) and stroke (high-risk: 19/389, 10.0% vs moderate-risk: 10/234, 4.3% vs low-risk: 6/369, 1.6%; P<0.01) were significantly higher in the high-risk group compared to those in the moderate-risk group and low-risk group. Although the incidence of myocardial infarction was also higher in the high-risk group (32/389, 8.2%) and moderate-risk group (15/234, 6.4%) than that in the low-risk group (16/369, 4.3%), the difference did not reach statistical significance (P=0.09). Kaplan-Meier survival curves (Figure 2) showed that, compared to the low-risk group, the risks of MACE, all-cause mortality, myocardial infarction, and stroke were significantly higher in those with high and moderate risks (all P<0.01).
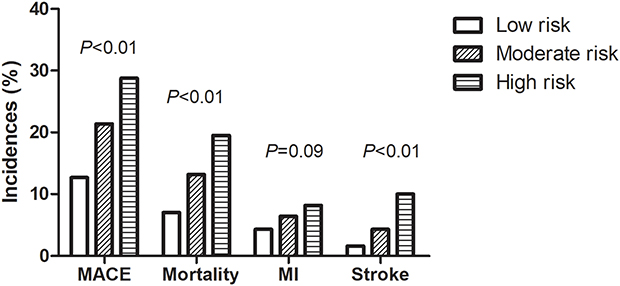 |
Figure 1 Incidence of MACE, mortality, myocardial infarction (MI), and stroke across CHA2DS2-VASc risk categories in acute coronary syndrome patients without atrial fibrillation. |
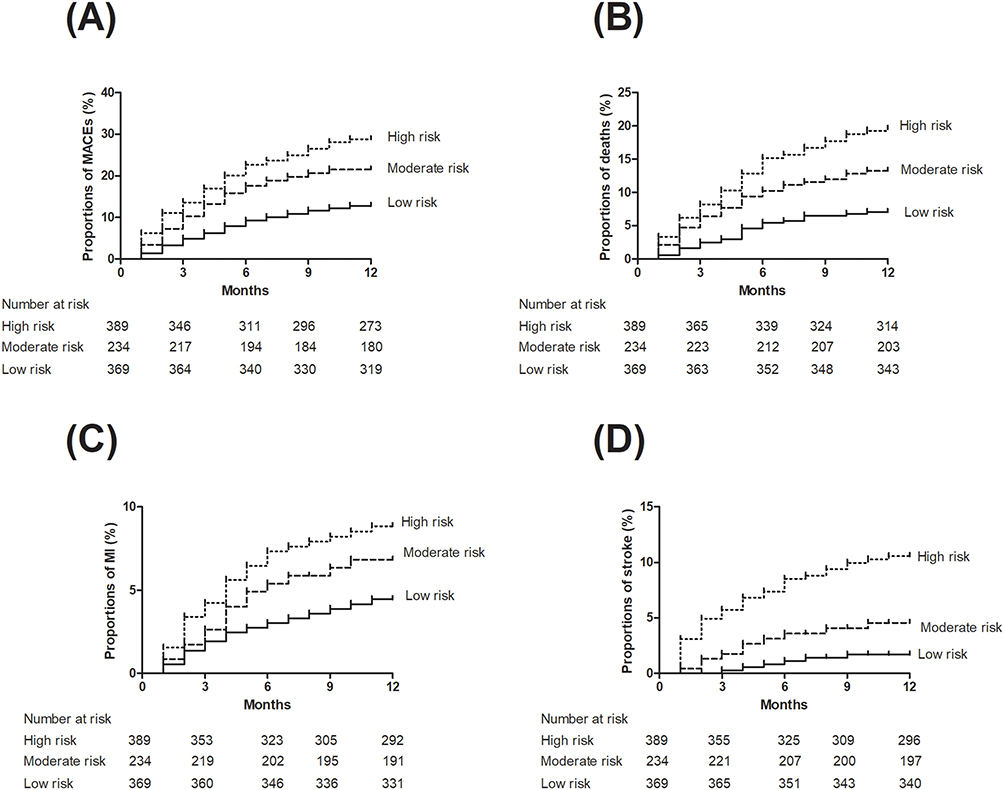 |
Figure 2 Kaplan–Meier survival curves for 1-year risk of (A) MACE, (B) mortality, (C) myocardial infarction (MI), and (D) stroke in acute coronary syndrome patients without atrial fibrillation, stratified by CHA2DS2-VASc score. Patients with moderate (2) and high (>2) scores showed significantly higher risks compared to those with low (0–1) scores. |
Multivariate Cox proportional hazard regression analysis was performed to identify prognostic factors associated with the risk of outcomes (Table 2). The proportional hazards assumption for Cox models was verified using Schoenfeld residuals, and no significant violations were detected (P>0.05 for all models). After adjusting for potential confounding factors, compared to the low-risk group, the hazard ratio (HR) of MACE occurrence was 3.83 (95% CI: 1.90–7.69; P<0.01) for high-risk group and 2.27 (95% CI: 1.34–3.86; P<0.01) for moderate-risk group, respectively. Regarding the individual components of MACE, the risk of all-cause mortality was significantly elevated in the moderate-risk group (HR=2.14; 95% CI: 1.08–4.24; P=0.03) and further increased in the high-risk group (HR=3.32; 95% CI: 1.36–8.10; P<0.01). For myocardial infarction, the high-risk group demonstrated a markedly higher risk (HR= 7.53; 95% CI: 2.13–26.59; P<0.01), while the moderate-risk group also showed a significant association (HR: 2.96; 95% CI: 1.15–7.61; P=0.03). As for stroke, both the moderate-risk (HR=5.26; 95% CI: 1.09–25.51; P=0.04) and high-risk groups (HR=14.63; 95% CI: 2.05–104.62; P<0.01) had significantly higher risks compared to the low-risk group. These findings suggest that the CHA2DS2-VASc score is independently associated not only with the overall risk of MACE, but also with increased risks of its individual components, including mortality, myocardial infarction, and stroke.
 |
Table 2 Univariate and Multivariate Cox Regression for Exploring the Association of CHA2DS2-VASc Score and Prognosis at 12 months |
A subgroup analysis by ACS type (STEMI and NSTEMI/unstable angina) demonstrated similar trends in the association between CHA2DS2-VASc score and 12-month MACE across both subgroups. The adjusted hazard ratios for high versus low risk were 3.54 (95% CI: 1.61–7.77; P<0.01) in STEMI and 8.47 (95% CI: 1.73–41.39; P<0.01) in NSTEMI/unstable angina patients.
Discussion
In this retrospective cohort study involving 992 Chinese patients with ACS undergoing PCI and without AF, we demonstrated that the CHA2DS2-VASc score was significantly associated with adverse cardiovascular outcomes over a 12-month follow-up period. Patients classified as high- and moderate-risk according to the CHA2DS2-VASc score exhibited significantly increased risks of MACE, including all-cause mortality, myocardial infarction, and stroke, compared to their low-risk counterparts. These associations remained robust after adjusting for a broad range of clinical and laboratory confounders, supporting the score’s prognostic utility beyond its traditional role in AF-related stroke risk stratification.
Our findings align with and expand upon prior studies suggesting that the CHA2DS2-VASc score may have broader cardiovascular applications. Several recent investigations have proposed that this scoring system, originally developed for estimating thromboembolic risk in AF, may also predict cardiovascular events in patients without AF, particularly those with established coronary artery disease. For instance, Song et al10 and Koene et al11 found that CHA2DS2-VASc scores effectively predicted the risk of MACE in acute ischemic stroke patients without AF and in community-dwelling individuals without AF, respectively. Recently, an increasing number of studies have explored the predicting value of CHA2DS2-VASc score in prognosis after ACS. In a Chinese study conducted by Ma et al.12 CHA2DS2-VASc score (HR=1.15; 95% CI: 1.04–1.27; P =.007) remained a useful predictor of MACE after adjusting for potential confounding factors; however, CHADS2 score was no longer associated with increased risk of MACE. Similarly, an Israel study conducted by Teodorovich et al13 showed that an elevated CHA2DS2-VASC score of ≥4 was independently associated with higher mortality (HR=2.12, CI: 1.29–3.25, P=0.001). However, their cohort included both patients with and without AF. Our study further validates and extends these findings by focusing exclusively on a well-defined cohort of ACS patients without AF, thereby eliminating the potential confounding influence of AF and providing more targeted evidence that the CHA2DS2-VASc score is a robust predictor of adverse cardiovascular events in this distinct subgroup. These results underscore that the score’s prognostic utility extends beyond its original role in AF-related stroke prediction, reflecting instead the cumulative impact of systemic vascular risk factors that are equally relevant in the broader ACS population. By isolating patients without known arrhythmias, our study provides a clearer understanding of the score’s independent predictive value and supports its potential application in routine risk stratification for non-AF ACS patients.
The prognostic value of the CHA2DS2-VASc score in our study likely stems from its inclusion of multiple traditional cardiovascular risk factors, such as advanced age, hypertension, diabetes mellitus, and prior stroke or vascular disease. These factors are not only independently associated with adverse outcomes but also synergistically increase the risk of plaque instability, thrombosis, and poor post-PCI recovery.14 Notably, the score includes both age-related and vascular-related components, making it well-suited to capture the complex comorbidity burden in elderly ACS patients. Moreover, the strong association we observed between high CHA2DS2-VASc scores and stroke—despite the absence of AF—may reflect the presence of other underlying mechanisms, such as endothelial dysfunction or atherosclerotic burden, that contribute to cerebrovascular risk in this population.
Previous research has demonstrated that traditional ACS-specific models such as the GRACE, SYNTAX and TIMI scores provide reliable prognostic value but require multiple laboratory and hemodynamic parameters that may not be readily available at all care levels.15,16 In contrast, the CHA2DS2-VASc score relies solely on routine clinical characteristics and can be rapidly calculated at the bedside without additional tests, offering practical advantages, particularly in resource-limited settings. Although our study did not directly compare its predictive accuracy with these established models, prior reports have shown that the CHA2DS2-VASc score achieves comparable discrimination for long-term mortality and MACE in ACS patients.17,18 Clinically, our findings support the use of CHA2DS2-VASc as a simple, accessible, and complementary tool—rather than a replacement—for early risk stratification in ACS. It may help identify high-risk patients who could benefit from intensified secondary prevention strategies, such as aggressive lipid lowering, optimized glycemic control, or prolonged dual antiplatelet therapy, and could potentially enhance prognostic precision when integrated with GRACE, SYNTAX or TIMI models in future studies.
Despite these strengths, several limitations should be acknowledged. First, this was a single-center, retrospective study, which may limit the generalizability of our findings and introduce potential selection bias. Although multivariable adjustments were performed, residual confounding cannot be completely ruled out. Second, despite the robust predictive value for MACE, the wide confidence intervals for stroke reflect the relatively small number of cerebrovascular events, suggesting limited statistical power for this endpoint. Larger multicenter studies are needed to confirm the predictive consistency of CHA2DS2-VASc for individual outcomes, particularly stroke. Third, the CHA2DS2-VASc score was calculated only at baseline and may not reflect dynamic changes in patient status over time.
Conclusion
In conclusion, CHA2DS2-VASc appears to be an independent predictor of 12-month adverse cardiovascular outcomes in patients with ACS without AF. Given its simplicity and wide availability, this score may complement established ACS-specific risk models such as GRACE, SYNTAX or TIMI in identifying high-risk individuals. In clinical practice, patients with higher CHA2DS2-VASc scores may warrant closer follow-up and optimization of secondary prevention strategies, including intensive lipid-lowering therapy, strict blood pressure and glucose control, and consideration of prolonged dual antiplatelet therapy. Future multicenter, prospective studies are needed to validate whether management guided by CHA2DS2-VASc–based stratification can improve clinical outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rao SV, O’Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;151:e771–e862. doi:10.1161/CIR.0000000000001328
2. Timmis A, Kazakiewicz D, Townsend N, Huculeci R, Aboyans V, Vardas P. Global epidemiology of acute coronary syndromes. Nat Rev Cardiol. 2023;20:778–788. doi:10.1038/s41569-023-00884-0
3. Chan MY, Du X, Eccleston D, et al. Acute coronary syndrome in the Asia-Pacific region. Int J Cardiol. 2016;202:861–869. doi:10.1016/j.ijcard.2015.04.073
4. Xu H, Li W, Yang J, et al. The China Acute Myocardial Infarction (CAMI) Registry: a national long-term registry-research-education integrated platform for exploring acute myocardial infarction in China. Am Heart J. 2016;175:193–201e193. doi:10.1016/j.ahj.2015.04.014
5. Luca F, Oliva F, Rao CM, et al. Appropriateness of dyslipidemia management strategies in post-acute coronary syndrome: a 2023 update. Metabolites. 2023;14:13. doi:10.3390/metabo14010013
6. Nasifov M, Ozmen E, Deniz C, et al. Association of CHA2DS2-VASc score with successful recanalization in acute ischemic stroke patients undergoing endovascular thrombectomy. Postepy Kardiol Interwencyjnej. 2022;18:269–275. doi:10.5114/aic.2022.122027
7. Lin Y, Pan W, Ning S, Song X, Jin Z, Lv S. Prevalence and management of hypertension in patients with acute coronary syndrome vary with gender: observations from the Chinese registry of acute coronary events (CRACE). Mol Med Rep. 2013;8:173–177. doi:10.3892/mmr.2013.1461
8. Zhou M, Liu J, Hao Y, et al. Prevalence and in-hospital outcomes of diabetes among patients with acute coronary syndrome in China: findings from the improving care for cardiovascular disease in China-acute coronary syndrome project. Cardiovasc Diabetol. 2018;17:147. doi:10.1186/s12933-018-0793-x
9. Qanitha A, Alkatiri AH, Qalby N, et al. Determinants of stroke following percutaneous coronary intervention in patients with acute coronary syndrome: a systematic review and meta-analysis. Ann Med. 2025;57:2506481. doi:10.1080/07853890.2025.2506481
10. Song M, Chen X. CHA(2)DS(2)-VASc score is associated with prognosis in patients with acute ischemic stroke without atrial fibrillation. Tex Heart Inst J. 2025;52:e248450.
11. Koene RJ, Alraies MC, Norby FL, et al. Relation of the CHA(2)DS(2)-VASc score to risk of thrombotic and embolic stroke in community-dwelling individuals without atrial fibrillation (From The Atherosclerosis Risk in Communities [ARIC] Study). Am J Cardiol. 2019;123:402–408. doi:10.1016/j.amjcard.2018.10.037
12. Ma X, Shao Q, Dong L, et al. Prognostic value of CHADS2 and CHA2DS2-VASc scores for post-discharge outcomes in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Medicine. 2020;99:e21321. doi:10.1097/MD.0000000000021321
13. Teodorovich N, Gandelman G, Jonas M, et al. The CHA(2)DS(2)-VAS(C) score predicts mortality in patients undergoing coronary angiography. Life. 2023;13. doi:10.3390/life13102026
14. Asher E, Abu-Much A, Bragazzi NL, et al. CHADS2 and CHA2DS2-VASc scores as predictors of platelet reactivity in acute coronary syndrome. J Cardiol. 2021;77:375–379. doi:10.1016/j.jjcc.2020.09.010
15. Kumar D, Ashok A, Saghir T, et al. Prognostic value of GRACE score for in-hospital and 6 months outcomes after non-ST elevation acute coronary syndrome. Egypt Heart J. 2021;73:22. doi:10.1186/s43044-021-00146-9
16. Correia LC, Garcia G, Kalil F, et al. Prognostic value of TIMI score versus GRACE score in ST-segment elevation myocardial infarction. Arq Bras Cardiol. 2014;103:98–106. doi:10.5935/abc.20140095
17. Fang C, Chen Z, Zhang J, Jin X, Yang M. Association of CHA2DS2-VASC score with in-hospital cardiovascular adverse events in patients with acute st-segment elevation myocardial infarction. Int J Clin Pract. 2022;2022:3659381. doi:10.1155/2022/3659381
18. Orvin K, Bental T, Assali A, Lev EI, Vaknin-Assa H, Kornowski R. Usefulness of the CHA2DS2-VASC score to predict adverse outcomes in patients having percutaneous coronary intervention. Am J Cardiol. 2016;117:1433–1438. doi:10.1016/j.amjcard.2016.02.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.