Back to Journals » International Journal of Women's Health » Volume 18
Cervical Ultrasound Assessment vs Bishop Score in Predicting Labor Induction Outcomes Among Nulliparous Women
Authors Li P, Xu J, Ouyang L, Fan J, Guo H, Huang Z
Received 5 March 2026
Accepted for publication 6 June 2026
Published 17 June 2026 Volume 2026:18 603281
DOI https://doi.org/10.2147/IJWH.S603281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Ping Li,1,* Jingying Xu,2,* Liping Ouyang,1 Jianhui Fan,1 Huanyi Guo,2 Zeping Huang2
1Department of Obstetrics, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Department of Ultrasonography, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huanyi Guo, Department of Ultrasonography, The Third Affiliated Hospital of Sun Yat-Sen University, No. 600, Tianhe Road, Guangzhou, 510630, People’s Republic of China, Tel/Fax +86 020 85273030, Email [email protected] Zeping Huang, Department of Ultrasonography, The Third Affiliated Hospital of Sun Yat-Sen University, No. 600, Tianhe Road, Guangzhou, 510630, People’s Republic of China, Tel/Fax +86 020 85253030, Email [email protected]
Objective: Induction of labor (IOL) failure increases the risk of maternal and neonatal complications. The traditional Bishop score (BS) for cervical assessment is limited by subjectivity and inter - observer variability. This study aimed to evaluate cervical status via ultrasound examination (UE) as an alternative to vaginal examination (VE), and compare its predictive performance for IOL outcomes with the BS.
Methods: In this prospective observational study, 106 nulliparous women with singleton pregnancy requiring IOL were enrolled from January 2024 to August 2025. Of these participants, 83 had successful IOL and 75 achieved vaginal delivery (VD). Cervical length (CL), posterior cervical angle (PCA), angle of progression (AoP), and cervical shear wave elastography (SWE) were measured, and compared with the conventional BS. The primary outcomes were successful IOL and VD. Multivariate logistic analysis was performed to identify independent influencing factors for the two outcomes, and ROC curve analysis was used to evaluate their predictive efficacy.
Results: Significant differences were observed in ultrasound parameters between groups stratified by both outcomes (P < 0.05), whereas BS indicators showed no significant differences (all P > 0.05). Multivariate logistic analysis showed that only cervical SWE was independently correlated with successful IOL and VD (P < 0.05), with superior predictive power compared with BS (AUC of 0.78 vs 0.53 for successful IOL and 0.78 vs 0.56 for VD). Significant differences in pain perception existed between VE and UE (χ2 = 212.00, P < 0.001). All participants suffered moderate to severe pain after VE, while nearly 85% felt pain - free and none had moderate or severe pain after UE.
Conclusion: Ultrasound outperformed BS in evaluating cervical morphology owing to its objectivity, repeatability, and visualization capability in routine practice, and also yielded a better patient experience before IOL. Cervical stiffness appears to be an important influencing factor for IOL success, and SWE shows potential as a promising predictive approach for IOL outcome.
Keywords: cervical ultrasound assessment, Bishop score, shear wave elastography, induction of labor, prediction
Introduction
Induction of labor (IOL) is one of the most common obstetric interventions, performed in up to one-third of pregnancies for maternal or fetal indications.1–3 Approximately 20% of IOL attempts end in failure,4,5 which frequently leads to emergency cesarean delivery. Such failure is associated with elevated risks of maternal and neonatal complications, prolonged hospital stay, increased medical costs, and heightened maternal psychological burden.6 Accordingly, accurate pre-IOL assessment is clinically crucial.
Cervical status is the key determinant of the difficulty and likelihood of successful IOL.7,8 Currently, the Bishop Score (BS) remains the most widely used method for evaluating cervical ripeness.9,10 Based on digital vaginal examination (VE), it assesses five cervical parameters: effacement, position, consistency, dilatation, and fetal head station. Despite its simplicity, the BS is highly operator-dependent, resulting in inherent subjectivity and poor reproducibility. Furthermore, VE is frequently associated with patient pain, anxiety, and discomfort;11,12 additionally, its predictive value for IOL outcomes is suboptimal (area under the curve [AUC] ≈ 0.6),13,14 with accumulating evidence questioning its utility in clinical decision-making.15–17 These limitations underscore the need for an alternative cervical assessment method.
Ultrasound has emerged as a promising method that offers objective, reproducible, and visualized results.18 It could provide quantitative parameters corresponding to BS components: cervical length (CL) as a surrogate for effacement, posterior cervical angle (PCA) for cervical position, cervical funneling (CF) for cervical dilatation (CD), and angle of progression (AoP) for fetal head station. However, most previous studies have evaluated only single or partial ultrasound parameters that do not fully align with the comprehensive BS criteria, and the predictive values for IOL outcomes remain inconsistent.19–21 Furthermore, cervical stiffness—an important parameter for assessing cervical ripeness—is often lacking in assessment.
Elastography is an imaging technique enabling objective measurement of tissue stiffness,22 which has been confirmed to exhibit high accuracy in evaluating tissue hardness in the liver and thyroid, thereby supporting clinical diagnosis.23,24 In 2007, Yamaguchi et al first applied cervical elastography (CE) to assess cervical ripening during pregnancy.25 To date, uniform measurement approaches and evaluation standards for cervical stiffness using CE remain absent, which gives rise to discrepancies in relevant research and limits general acceptance.26–29 Furthermore, pre-induction cervical ultrasound assessment (CUA) is seldom conducted locally, and relevant clinical evidence remains scarce. Given the above background, this study adopted ultrasonic indicators matching conventional BS items to evaluate cervical condition, and further compared their predictive efficacy for IOL outcomes.
Materials and Methods
Subjects
This prospective observational study was conducted at the Third Affiliated Hospital of Sun Yat-sen University between January 2024 and August 2025. Eligible participants were nulliparous women requiring IOL. Inclusion criteria were: a singleton pregnancy, ≥37 gestational weeks, cephalic presentation, intact amniotic membranes, estimated fetal weight (EFW) ≤ 4500g, no history of uterine surgery, and no contraindications to vaginal delivery (VD). Exclusion criteria included: refusal to participate, spontaneous onset of labor upon admission, request for cesarean section after assessment, a positive oxytocin stress test, meconium stain detected during amniotomy, or placental abruption following amniotomy.
Written informed consents were obtained from all women prior to their enrollment in the study. The study was approved by the Human Research Ethics Committee of the Third Affiliated Hospital of Sun Yat - Sen University (approval number: 2023 - 297 - 02, Dec 13, 2023) and complies with the declaration of Helsinki. The clinical trial registration number was ChiCTR2400092572.
Sample Size Calculation
BS ≤6 corresponded to a 60% IOL success rate, with a BS specificity of 50% for predicting failed induction. All participants underwent both CUA and BS examinations. We hypothesized a 25% absolute improvement in specificity (75% for CUA vs 50% for BS). Sample size was determined using two‑sided McNemar’s test (α = 0.05, power = 0.85), assuming an overall 80% IOL success rate; 92 paired subjects were required. After accounting for 10% follow‑up dropout, the target sample size was set at 103 nulliparous women.
Clinical Data Collection
Baseline characteristics were recorded in the database of the hospital medical system at the time of admission, including age, pre-gestational body mass index (BMI, BMI=weight (kg) / height (m2)), prenatal BMI, EFW (ultrasound examination within one week before IOL) and indications for IOL (including prolonged pregnancy (≥ 41 gestational weeks), fetal growth restriction, gestational diabetes mellitus, oligohydramnios, or other pregnancy complications). A digital VE was performed prior to IOL by obstetricians with at least 5 years of experience, who were blinded to the study. BS was calculated for a score ranging from 0 to 13.30–32 In addition, a visual analogue pain scale (VAS) was administered to all participants to collect their experiences after VE and ultrasound examination (UE) at the time of admission. Participants were asked to select a pain score ranging from 0 to 10, which was then categorized into four grades according to internationally recognized criteria: no pain (VAS: 0), mild pain (VAS: 1–3), moderate pain (VAS: 4–6), and severe pain (VAS: 7–10).
Cervical Ultrasound Assessment (CUA)
All enrolled patients underwent UE performed by two sonographers with >10 years of routine obstetric ultrasound experience and ≥5 years of elastography practice. Both operators completed standardized pre-study training to unify scanning and measurement standards. Transvaginal scanning (3–10 MHz 3D probe) and transperineal scanning (1–8 MHz 3D probe) were carried out using Mindray Nuewa R9 ultrasound system integrated with elastography software. CUA parameters were selected to match the components of BS, including CL, PCA, CF, AoP, and shear wave elastography (SWE). All measurements were performed following the 2021 expert consensus guidelines.18
Participants emptied bladders 30 minutes before scanning to avoid imaging artifacts, and were placed in lithotomy position. The probe was gently inserted 3–5 cm into the vagina under B-mode guidance without compressing the cervix. Standard measurements were defined as follows. CL (Figure 1a) was the linear distance between internal and external cervical os on midsagittal view. PCA (Figure 1b) referred to the angle between cervical midline and posterior uterine wall tangent. CF (Figure 1c) was defined as wedge dilatation of internal os. AoP (Figure 1d) was formed by pubic symphysis midline and tangent line to fetal head. SWE (Figure 1e) was acquired with clear cervical structure display. The internal os was set as region of interest (ROI), given its superior predictive value for labor induction outcome.29,33 The system generated shear waves automatically, and data were collected after wave propagation stabilized. Each parameter was measured three times, with the mean value used for subsequent analysis. All ultrasound images were digitally stored and post-delivery analyzed.
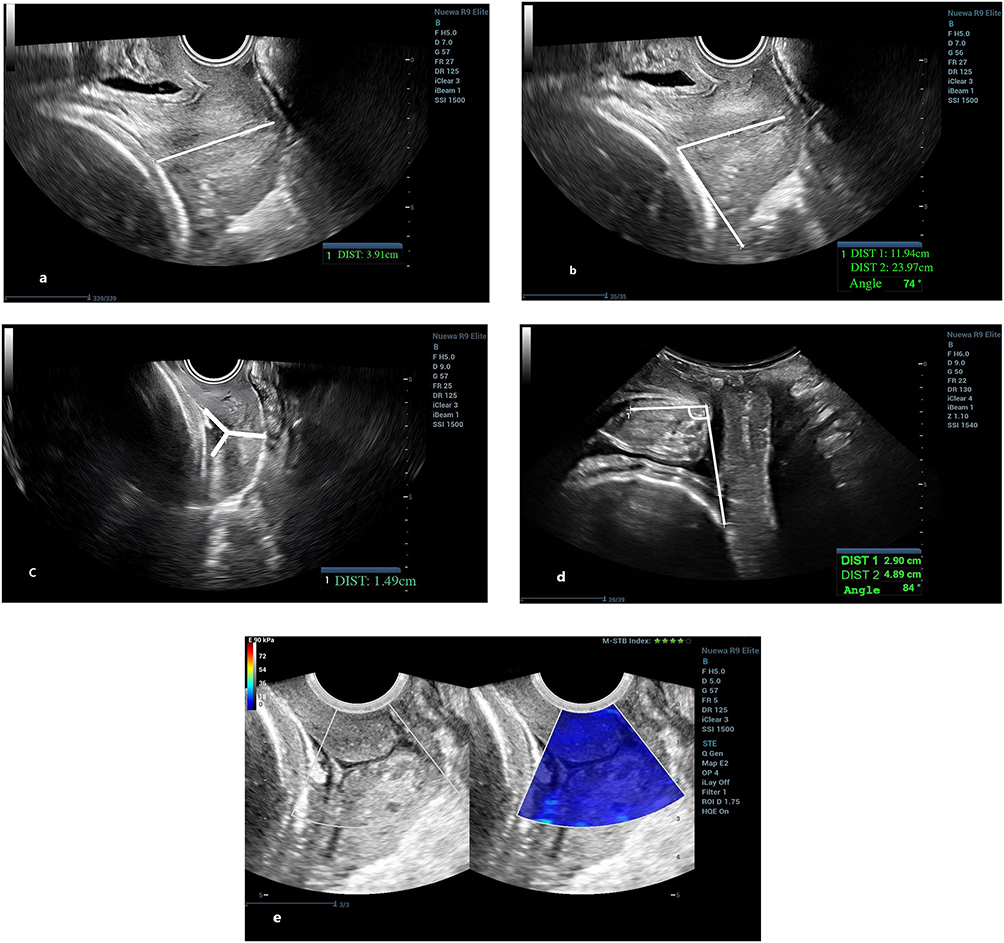 |
Figure 1 Ultrasound-Based Parameters Corresponding to Bishop Score (BS) Components: (a) Cervical length (CL): straight distance between the external and internal os in the midsagittal plane. (b) Posterior cervical angle (PCA): posterior angle between the line connecting the internal and external os and the line along the lower posterior uterine wall. (c) Cervical funnel (CF): wedge-shaped dilation of the internal cervical os. (d) Angle of progression (AoP): angle between the pubic symphysis longitudinal axis and a tangent line from its inferior edge to the fetal skull surface. (e) Shear wave elastography (SWE): performed with clear visualization of the cervical canal, internal/external os, and cervicovaginal junction; the region of interest (ROI) is placed at the internal cervical os. |
IOL
Women with BS ≥ 6 underwent primary amniotomy, with oxytocin infusion started if no regular contractions developed within 30 minutes. Those with BS < 6 received 12-hour Cook balloon cervical ripening, followed by timely amniotomy whenever feasible. Oxytocin was supplemented in the absence of effective uterine contractions within 30 minutes. Early balloon expulsion was managed with amniotomy, and oxytocin was administered if regular contractions failed to appear. Epidural analgesia was offered at 1–3 cm cervical dilation based on maternal demand.
Outcome Measures
The study evaluated two primary outcomes which were considered as the most relevant for assessing the success of IOL: 1) success of IOL (Per Chinese national labor management guidelines,34 induction failure was defined as failure to reach active labor (cervical dilation ≥ 5 cm) within 18 hours after membrane rupture and regular uterine contractions).; 2) success of vaginal delivery (VD).
Statistical Analysis
SPSS 23.0 software (IBM Corp., Armonk, NY, USA) was used for data analysis. Continuous data were presented as mean ± SD or median (interquartile range) based on normality, while categorical data were expressed as frequency (percentage). Group differences were analyzed using independent samples t-test, Mann–Whitney U-test, or Chi-square test, as appropriate. Multivariate logistic analysis was performed to identify independent predictors of IOL and VD outcomes. We ultimately included 8 variables in the stepwise regression model based on positive event counts. Variable selection followed hierarchical criteria: significant univariate factors (P < 0.05) were prioritized, then borderline factors (P < 0.1) and clinically relevant predictors. Despite insignificant univariate results, BS was forcibly incorporated as a confounder to correct treatment bias and objectively assess ultrasonic predictive values. Collinearity was verified via variance inflation factor (VIF < 10). Model fitness was evaluated using the Hosmer-Lemeshow test. Receiver operating characteristic (ROC) curves were plotted to evaluate the predictive performance, and pairwise comparisons of AUCs were performed using DeLong’s test. Results of logistic regression were presented as odds ratios (ORs) with 95% confidence intervals (95% CIs). P < 0.05 was considered statistically significant.
Results
Patient Enrollment
Of the 126 initially enrolled eligible women, 20 were excluded before the active phase: 12 withdrew voluntarily post-assessment, 4 had positive oxytocin stress tests, 3 had severe meconium staining and 1 suspected placental abruption during artificial amniotomy before the onset of labor. This resulted in a final analytic cohort of 106 participants. For the primary outcome of successful IOL, 83 cases were classified as successful, whereas 23 cases were deemed failed (defined as failure to enter the active phase within 18 hours of amniotomy despite regular uterine contractions). For the secondary outcome of VD, 75 women achieved vaginal delivery (73 spontaneous; 2 vacuum-assisted due to prolonged second stage of labor), and 31 underwent cesarean section. Indications for cesarean section were fetal distress (n = 12; 10 with abnormal fetal electronic monitoring, 2 with severe meconium staining), protracted active phase (n = 8), suspected intrauterine infection (n = 6), persistent occiput posterior dystocia (n = 4), and severe hypertension during the active phase precluding short-term vaginal delivery (n = 1) (Figure 2).
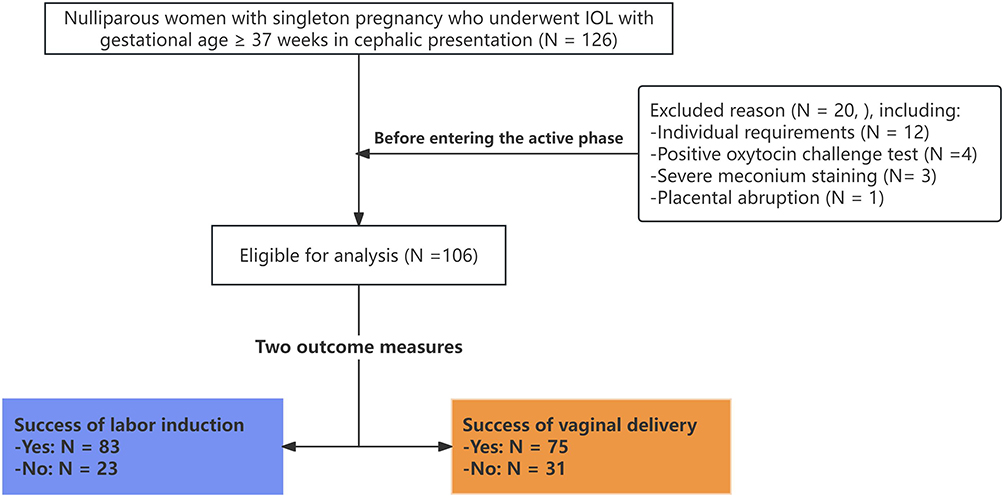 |
Figure 2 Flowchart of women enrollment for uncomplicated singleton term pregnancies, planned for induction of labor (IOL). |
Baseline Characteristics
Baseline characteristics indicated that prenatal BMI was significantly higher among women with unsuccessful outcomes compared to those with successful outcomes (IOL: 27.90 vs 25.60, P = 0.011; VD: 27.70 vs 25.50, P = 0.010). Among women with successful IOL and VD, the EFW was lighter than in unsuccessful women (VD: 3131.04 ± 371.77 g vs 3291.00 ± 360.23 g, P = 0.045; IOL: 3141.82 ± 378.67 g vs 3307.74 ± 332.22 g, P = 0.059). No significant differences were found in induction success rates between groups. Women with successful labor induction and vaginal delivery received epidural analgesia more often (91.57% vs 69.57%, P = 0.016; 92.00% vs 74.19%, P = 0.032). Maternal age, prepregnancy BMI, induction indications and approaches showed no intergroup differences (all P > 0.05) (Table 1).
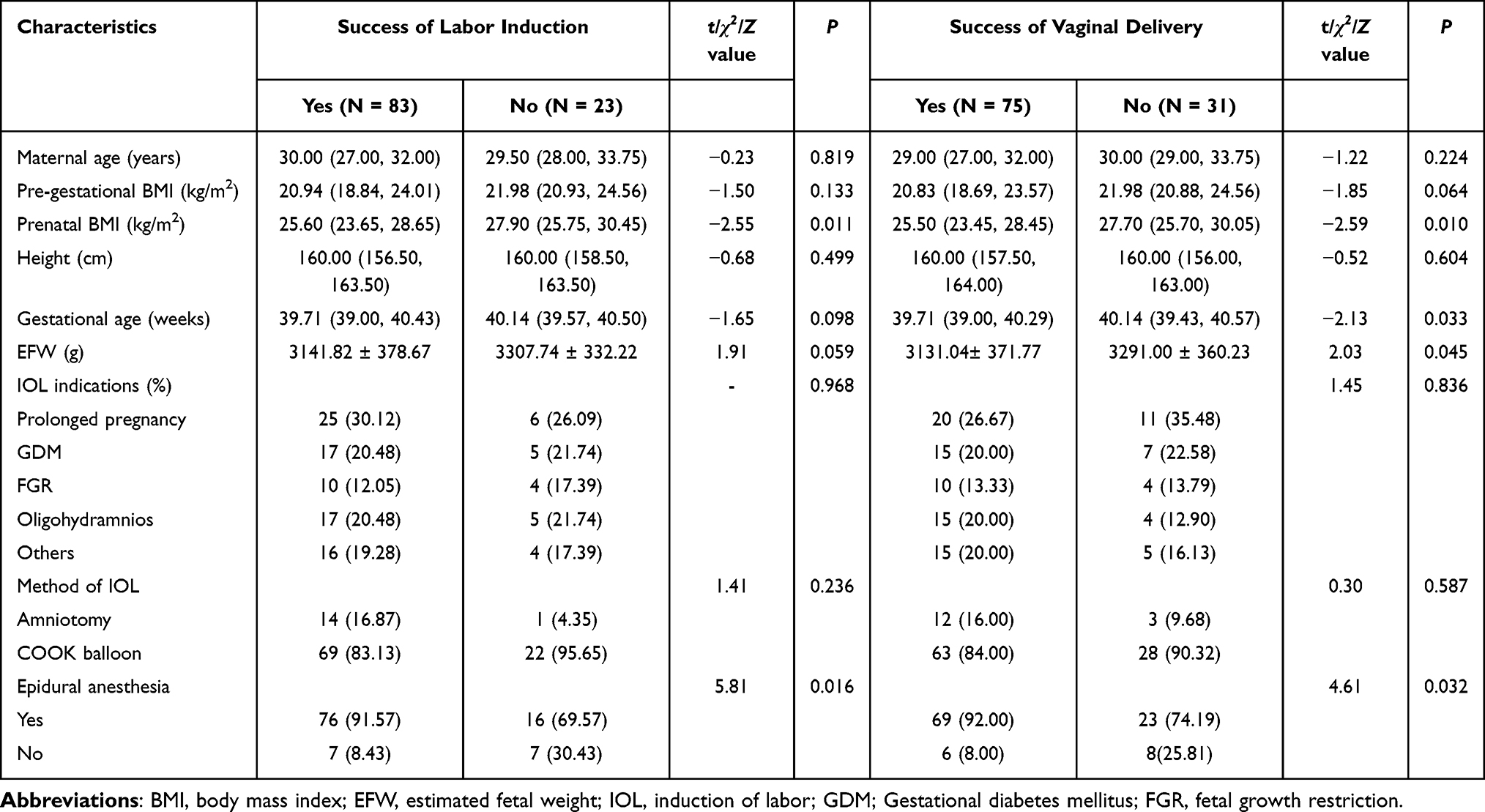 |
Table 1 Clinical Characteristics of the Study Participants According to Two Different Outcome Measurement Methods: Success of Labor Induction and Success of Vaginal Delivery |
Experience After VE and UE
There were also significant differences in the pain experience of participants between VE and UE (χ2 = 212.00, P <0.001). Participants suffered moderate (42.40%, 45/106) or severe (57.60%, 61/106) pain during VE. By comparison, 84.90% (90/106) reported no pain and 15.10% (16/106) had only mild discomfort after UE, with no moderate or severe pain recorded (Figure 3).
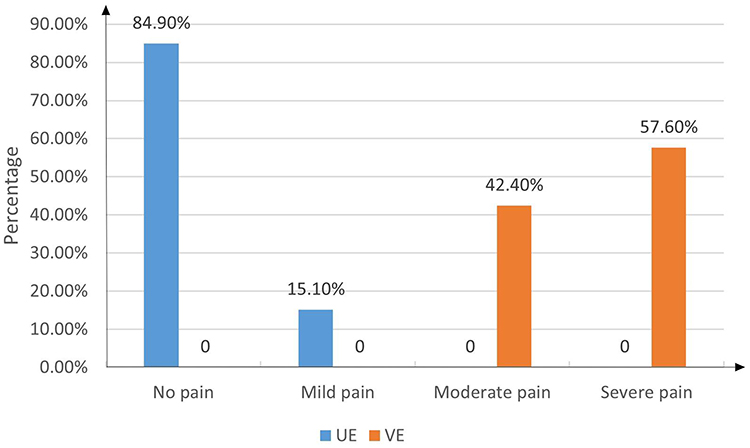 |
Figure 3 The visual analogue pain scale (VAS) for participants after vaginal examination (VE) and ultrasound examination (UE) (no pain: 0, mild pain: 1 ~ 3, moderate pain: 4 ~ 6, severe pain: 7 ~ 10). |
Comparison of BS and CUA
The comparison of individual components of the BS and CUA with respect to both outcomes was summarized (Table 2). Across groups stratified by either IOL success or VD, significant differences were observed in CUA indicators, whereas no significant differences were detected in BS parameters (all P > 0.05). Women with successful IOL and those with VD exhibited shorter CL (25.77 ± 8.25 vs 30.96 ± 7.73, P = 0.008; 25.55 ± 8.05 vs 30.16 ± 8.40, P = 0.009), a larger PCA (104.63 ± 23.99 vs 89.22 ± 25.16, P = 0.008; 107.17 ± 22.78 vs 87.03 ± 24.58, P < 0.001) and AoP (98.02 ± 13.22 vs 88.61 ± 14.03, P = 0.004; 98.61 ± 13.38 vs 89.61 ± 13.21, P = 0.002), and a lower cervical SWE (3.95 vs 6.30, P < 0.001; 3.90 vs 6.13, P < 0.001). However, whether the CF was present or not did not have any predictive value for either of the two outcomes (all P > 0.05).
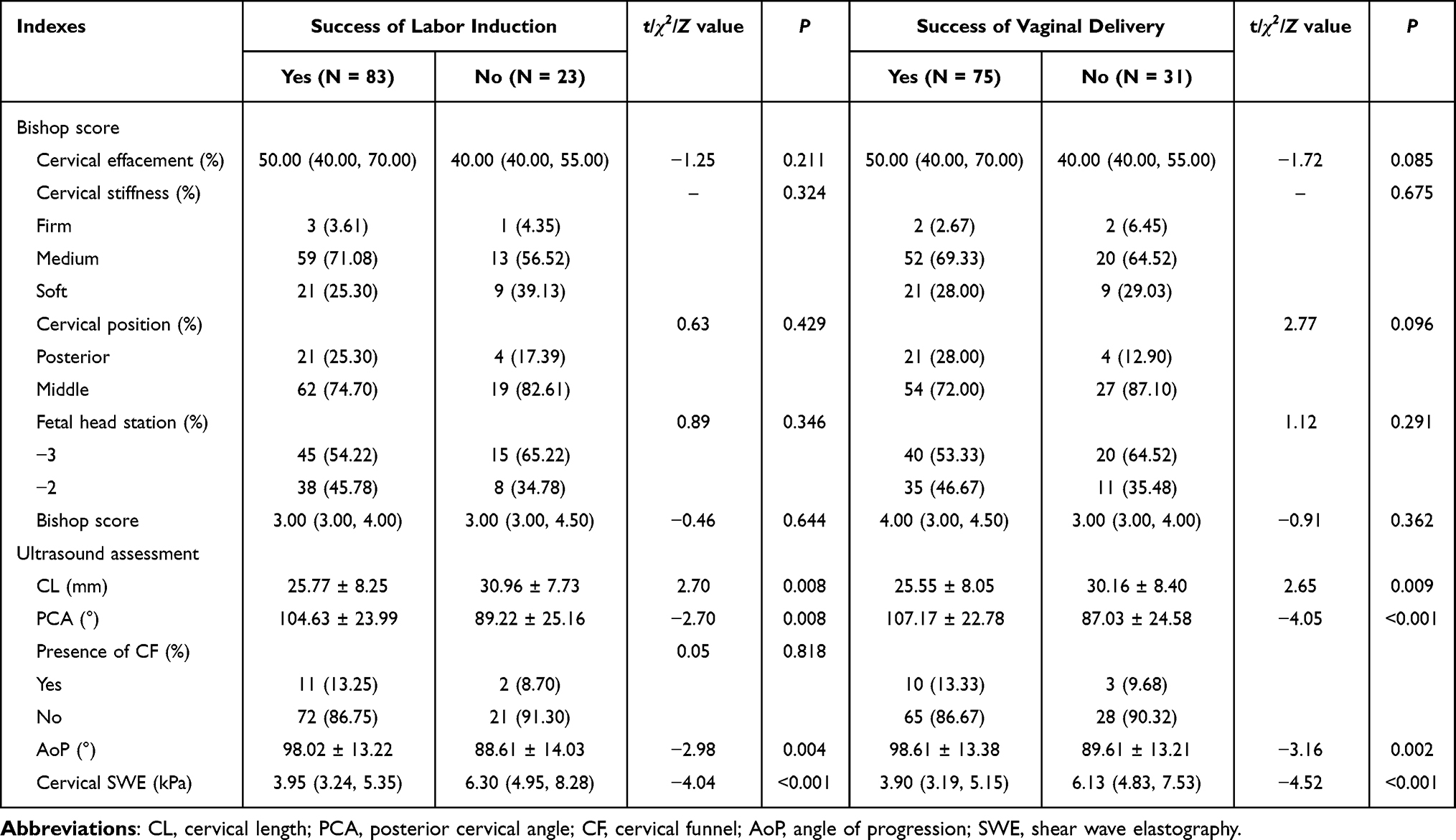 |
Table 2 Comparison of the Various Components of Bishop Score and Cervical Ultrasound Assessment According to the Two Different Outcome Measurements: Success of Labor Induction and Success of Vaginal Delivery |
Univariate and Multivariate Analyses
Univariate and multivariate logistic analyses were performed to evaluate factors associated with successful IOL and VD (Table 3). Univariate analyses were conducted to analyze potential influencing factors for the two primary outcomes (including maternal age, maternal height, pre - gestational BMI, prenatal BMI, EFW, indications for induction of labor, epidural anesthesia, BS, CL, PCA, CF, AoP and SWE, etc). Eight variables were finally enrolled. Due to sample size constraints and event-per-variable principle, BS was prioritized over gestational age for multivariate analysis, whose association was described in univariate results. The Hosmer-Lemeshow test demonstrated good model fit for both successful IOL (χ2 = 6.695, P = 0.548 > 0.05) and VD (χ2 = 2.185, P = 0.975 > 0.05). In the multivariate analysis, SWE emerged as a strong independent risk factor for successful IOL (P = 0.024, OR of 0.79 (95% CI: 0.63 ~ 0.97)) (Figure 4a) and VD (P = 0.027, OR of 0.79 (95% CI: 0.63 ~ 0.97)) (Figure 4b). No significant correlation was observed between BS and the two outcomes.
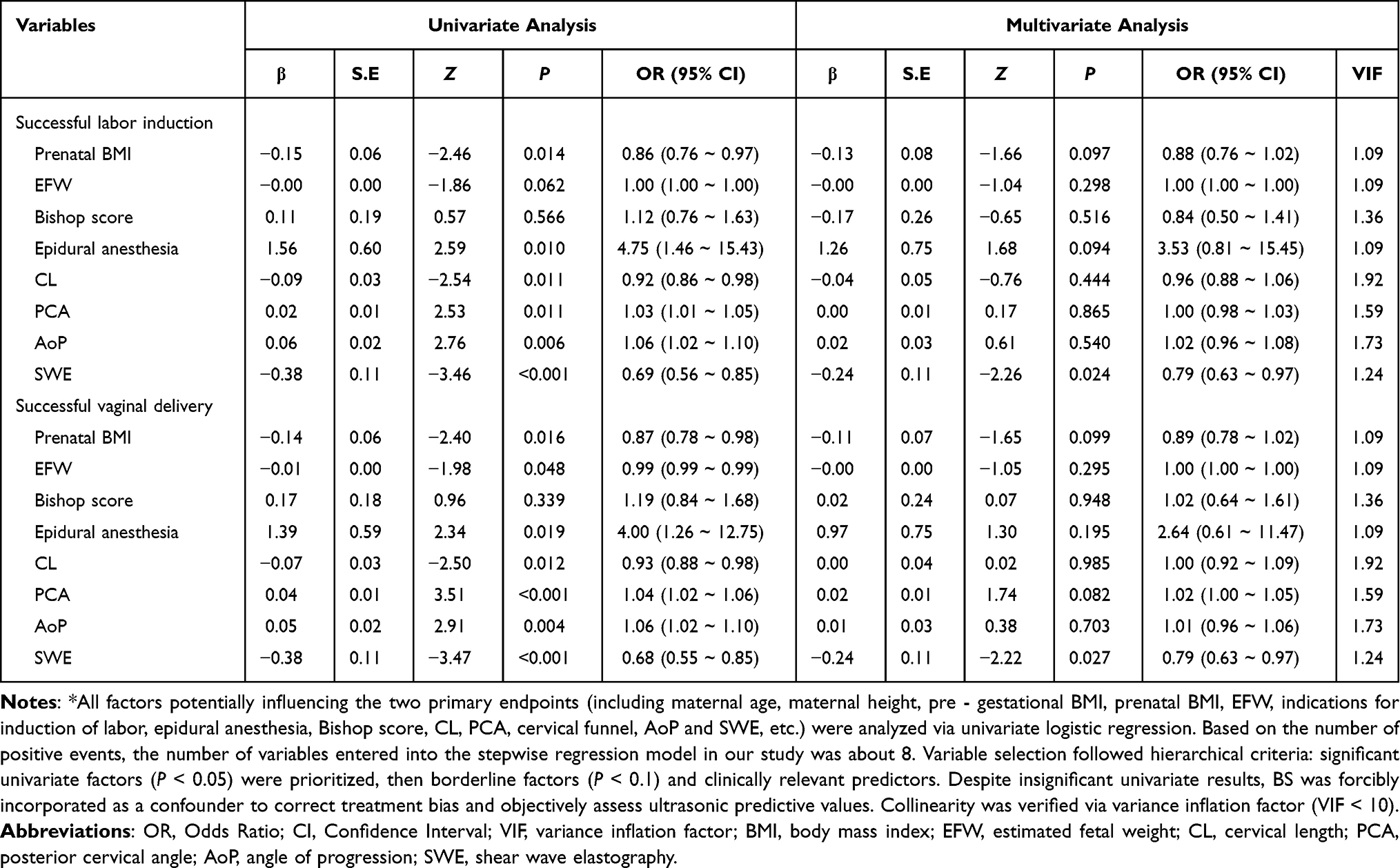 |
Table 3 Univariate and Multivariate Analysis of the Various Components for the Incidence of Successful Labor Induction and Successful Vaginal Delivery* |
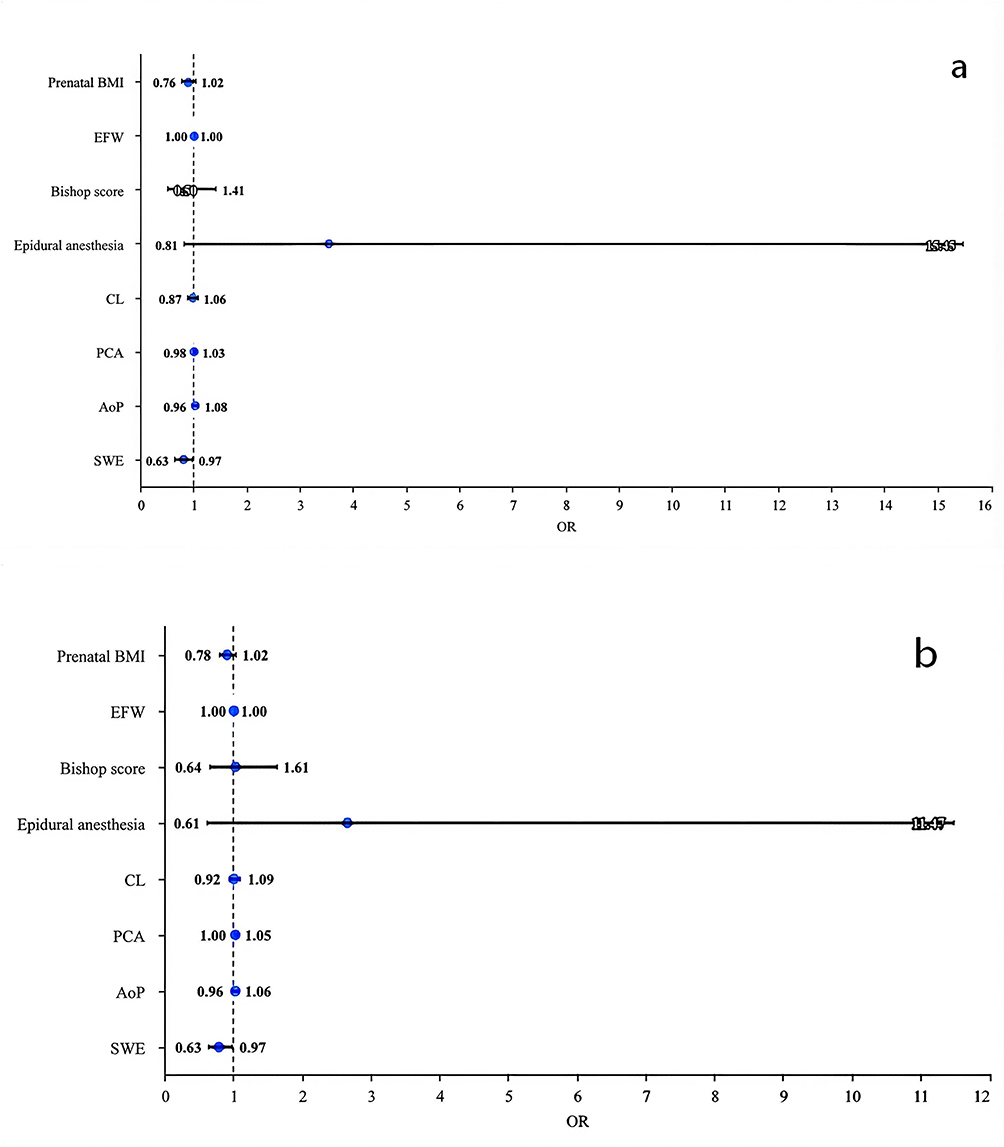 |
Figure 4 Forest plot of odds ratios (OR) and 95% confidence intervals (CI) for factors associated with successful induction of labor (a) and vaginal delivery (b). |
Compare the Predicted Values of SWE and BS
ROC curves were plotted to compare the predictive efficacy of SWE and BS for the two primary outcomes. For successful IOL, SWE yielded a significantly higher AUC than BS (0.78, 95% CI: 0.67–0.88 vs 0.53, 95% CI: 0.39–0.67), with a significant difference confirmed by DeLong’s test (P = 0.001, Z = 3.28, Figure 5a). Similarly, SWE presented superior predictive performance for VD (AUC = 0.78, 95% CI: 0.69–0.87) relative to BS (AUC = 0.56, 95% CI: 0.43–0.68, P = 0.001, Z = 3.43, Figure 5b). The optimal SWE cut-off values were 4.72 kPa for successful IOL and 3.96 kPa for VD.
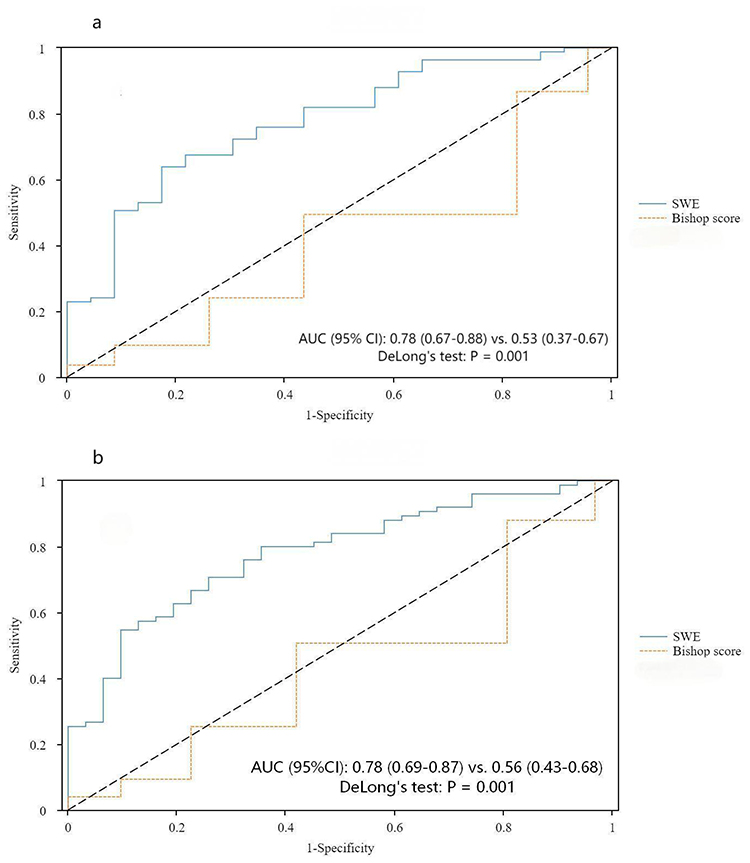 |
Figure 5 Comparing receiver operating characteristic (ROC) curves for predicting the success of labor induction (a) and vaginal delivery (b) using the shear wave elastography at the internal cervical os and the Bishop score. |
Discussion
Given that cervical status is a key determinant of IOL success, this study aimed to address BS limitations using comparable ultrasound parameters and compare CUA’s predictive value with BS. Key findings are as follows: 1) CUA parameters (CL, PCA, SWE, AoP) showed significant differences between successful and unsuccessful groups in both IOL and VD cohorts, whereas no BS component exhibited such differences; 2) ultrasound assessment improved patient experience, with a markedly lower VAS grades; 3) after adjusting for confounding factors via multivariate logistic analysis, SWE demonstrated better predictive value for IOL and VD success, with superior accuracy (AUC = 0.78 for both endpoints) compared with BS.
Traditional BS assessment is highly operator-dependent, resulting in poor reproducibility and unstable evaluation results due to subjective manual examination. Increasing studies have confirmed that ultrasound-derived cervical parameters are equivalent or even surpass of BS in predicting delivery outcomes. Hamza et al26 incorporated multiple ultrasound parameters—including CL, CF, CE, lower uterine segment thickness, and strain values—demonstrating that these parameters yield superior predictive value for IOL outcomes compared to the BS. Notably, this study omitted assessments of fetal head station and cervical position, which are clinically relevant cervical characteristics. Eggebø et al35 compared CL, PCA, HPD, and CD with BS and confirmed that the combination of these four ultrasound parameters can effectively predicts IOL success and serve as an alternative to BS. Nevertheless, they excluded cervical stiffness, a key biomechanical property of the cervix that contributes to its functional status. Wei et al28 included CL and CE in their CUA and also reported that both these parameters had the same predictive value for IOL outcomes as BS. However, there are also studies suggesting that CUA has no predictive value for the outcome of IOL. Racene et al36 selected CL, CD, HPD, and PCA for CUA; however, neither their ultrasound panel nor BS achieved satisfactory predictive performance (all area under the curve [AUC] < 0.70). In our study, CUA demonstrated distinctly better predictive efficacy for IOL outcomes than BS. Unlike most prior research, our analysis integrated all core BS-related indicators, including CL, PCA, CF presence, AoP and cervical SWE, enabling accurate identification of key factors impacting IOL outcomes.
Cervical remodeling, a prerequisite for labor initiation, involves three sequential stages: softening, maturation, and dilatation. Since histological changes occur earlier than morphological alterations, quantitative evaluation of cervical stiffness carries important clinical value for pre-IOL assessment. CE, a non-invasive modality for quantifying tissue stiffness first applied to cervical assessment in 2007,25 has been validated for IOL outcome prediction in accumulating studies. In a meta-analysis of 4 studies involving 323 pregnant women, Londero et al37 concluded that CE demonstrates promising efficacy for predicting successful IOL and vaginal delivery. Two major elastographic techniques are currently available for cervical stiffness assessment: strain elastography (SE) and SWE.38 SE estimates tissue stiffness through manual probe compression and tissue deformation, which is prone to inter-operator variability. In contrast, SWE quantifies tissue hardness objectively by measuring the propagation velocity of acoustic shear waves, with minimal reliance on subjective operator manipulation. Therefore, SWE is increasingly regarded as a more reliable elastographic modality for predicting delivery outcomes.39 Lu et al29 showed SWE is an independent predictor of delivery outcomes, with a CL+SWE model achieving AUC of 0.82, and emphasized internal cervical os stiffness measurements yield the highest predictive efficacy. Agarwal et al40 using SE, also confirmed that elastographic indices at the internal os are optimal for forecasting IOL success. SWE assessment of the cervix requires dedicated ultrasound devices integrated with shear wave elastography modules and matched specialized probes. Strict standardized scanning protocols and professional operational training are also essential to ensure accurate and consistent measurements. Due to such hardware and technical demands, its routine clinical application before IOL is not yet prevalent across medical centers in China. Our study applied SWE to assess cervical stiffness, and found it could serve as a promising predictor for IOL outcomes, with an AUC of 0.78. As a quantitative and comparatively objective index, SWE enables quantitative evaluation of cervical stiffness, which could provide more suggestive evidence to aid clinical judgment on cervical ripening.
As an invasive procedure, VE may bring obvious physical discomfort and psychological stress to pregnant women.11,12 Negative experiences during pre-IOL VE may heighten maternal anxiety and fear toward both the induction procedure and subsequent labor. In contrast, UE offers intuitive and accurate assessments while being minimally invasive, making it generally more acceptable to patients. Our findings also support this clinical advantage.
A key strength of this study is the close alignment between CUA parameters and BS components, which effectively facilitates identification of the actual causal factors underlying IOL outcomes. Specifically, we focused on two clinically relevant primary outcomes for evaluating IOL success (IOL success and VD success) and incorporated patient experience perceptions. Nevertheless, several limitations should be acknowledged: 1) Clinical implementation of CUA (especially SWE) may be constrained by variability in trained sonographer availability and appropriate ultrasound equipment across healthcare institutions; 2) Compared with VE, CUA is potentially more time-consuming, which may hinder its widespread routine clinical application; 3) Pelvic anatomical parameter assessment via ultrasound (eg, true intercristal diameter, interischial spine diameter, pubic arch angle) was not incorporated; 4) The single-center design may limit generalizability to broader patient populations. Future studies are therefore warranted to validate CUA’s performance in diverse cohorts.
Conclusions
In conclusion, this study adopted CUA referencing the evaluation metrics of conventional BS. This method yields favorable performance and enhances the ability to predict labor induction outcomes. Cervical stiffness serves as a crucial determinant of successful induction, and SWE presents great application value in pre-induction cervical stiffness assessment. Multicenter trials will be conducted to validate CUA as an objective, precise and well-tolerated substitute for traditional BS. Relevant follow-up research can optimize clinical judgment and support individualized delivery management.
Declaration of Generative AI in Scientific Writing
The authors declare that no generative AI tools were used to analyze data or draw insights as part of the research process.
Data Sharing Statement
All the data generated or analyzed in this study are available from the corresponding author Zeping Huang upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Human Research Ethics Committee of the Third Affiliated Hospital of Sun Yat-Sen University (approval number: 2023-297-02, Dec 13, 2023). Written and informed consents were obtained from all women prior to their enrollment in the study.
Consent for Publication
The authors confirm that consent for publication has been obtained from all individuals concerned.
Acknowledgments
The authors express their gratitude to all the physicians in the Department of Obstetrics and the Department of Ultrasonography at the Third Affiliated Hospital of Sun Yat-sen University for their substantial assistance with this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Marconi AM. Recent advances in the induction of labor. F1000Res. 2019;8:F1000FacultyRev–13. doi:10.12688/f1000research.17587.1
2. Zhu J, Xue L, Shen H, et al. Labor induction in China: a nationwide survey. BMC Pregnancy Childbirth. 2022;22(1):463. doi:10.1186/s12884-022-04760-6
3. Hamilton BE, Osterman MJ. Births: provisional data for 2022. Vital statistics rapid release. no 28. Available from: https://www.cdc.gov/nchs/data/vsrr/vsrr028.pdf.
4. Melkie A, Addisu D, Mekie M, Dagnew E. Failed induction of labor and its associated factors in Ethiopia: a systematic review and meta-analysis. Heliyon. 2021;7(3):e06415. doi:10.1016/j.heliyon.2021.e06415
5. Ayele M, Tilahun BD, Yilak G, Alamrew A, Zewdie A, Lake ES. Prevalence of failed induction of labor and associated factors among women who underwent induction of labor in Ethiopia: a systematic review and meta-analysis. PLoS One. 2024;19(11):e0305384. doi:10.1371/journal.pone.0305384
6. Sandall J, Tribe RM, Avery L, et al. Short-term and long-term effects of caesarean section on the health of women and children. Lancet. 2018;392(10155):1349–1357. doi:10.1016/S0140-6736(18)31930-5
7. Levine LD. Cervical ripening: why we do what we do. Semin Perinatol. 2020;44(2):151216. doi:10.1016/j.semperi.2019.151216
8. Riskin-Mashiah S, Wilkins I. Cervical ripening. Obstet Gynecol Clin North Am. 1999;26(2):243–257. doi:10.1016/S0889-8545(05)70072-3
9. Bishop EH. Pelvic scoring for elective induction. Obstet Gynecol. 1964;24:266–268.
10. Edwards RK, Richards DS. Preinduction cervical assessment. Clin Obstet Gynecol. 2000;43(3):440–446. doi:10.1097/00003081-200009000-00004
11. Jenkins H, Jessiman WC, Hubbard G, O’Malley C. Exploring women’s experiences, views and understanding of vaginal examinations during intrapartum care: a meta-ethnographic synthesis. Midwifery. 2023;124:103746. doi:10.1016/j.midw.2023.103746
12. Ying Lai C, Levy V. Hong Kong Chinese women’s experiences of vaginal examinations in labour. Midwifery. 2002;18(4):296–303. doi:10.1054/midw.2002.0326
13. Ding W, Chim S, Wong K, et al. Prediction of vaginal birth after induction of labor with maternal circulating RNA transcripts. Am J Obstet Gynecol. 2025;233(5):490.e1–490.e21. doi:10.1016/j.ajog.2025.06.023
14. Abdullah Z, Chew KT, Velayudham V, et al. Pre-induction cervical assessment using transvaginal ultrasound versus Bishops cervical scoring as predictors of successful induction of labour in term pregnancies: a hospital-based comparative clinical trial. PLoS One. 2022;17(1):e0262387. doi:10.1371/journal.pone.0262387
15. de Klerk HW, Boere E, van Lunsen RH, Bakker J. Women’s experiences with vaginal examinations during labor in the Netherlands. J Psychosom Obstet Gynaecol. 2018;39(2):90–95. doi:10.1080/0167482X.2017.1291623
16. Hendrix NW, Chauhan SP, Morrison JC, Magann EF, Martin JN, Devoe LD. Bishop score: a poor diagnostic test to predict failed induction versus vaginal delivery. South Med J. 1998;91(3):248–252. doi:10.1097/00007611-199803000-00006
17. Kolkman DG, Verhoeven CJ, Brinkhorst SJ, et al. The bishop score as a predictor of labor induction success: a systematic review. Am J Perinatol. 2013;30(8):625–630. doi:10.1055/s-0032-1331024
18. Kamel R, Garcia F, Poon LC, Youssef A. The usefulness of ultrasound before induction of labor. Am J Obstet Gynecol MFM. 2021;3(6S):100423. doi:10.1016/j.ajogmf.2021.100423
19. Chan W, Chaemsaithong P, Lim WT, et al. Pre-induction transperineal ultrasound assessment for the prediction of labor outcome. Fetal Diagn Ther. 2019;45(4):256–267. doi:10.1159/000489122
20. Yang Q, Zhou CC, Chen Y, Pei JD, Hua XL, Yao LP. Prediction model for successful induction of labor by cervical strain elastography diagnosed at late-term pregnancy in nulliparous women: a prospective cohort study. BMC Pregnancy Childbirth. 2023;23(1):114. doi:10.1186/s12884-023-05426-7
21. Volpe N, Ramirez Zegarra R, Melandri E, et al. Association between the cervical sliding sign and successful induction of labor in women with an unfavorable cervix: a prospective observational study. Eur J Obstet Gynecol Reprod Biol. 2022;278:16–21. doi:10.1016/j.ejogrb.2022.09.004
22. Ophir J, Céspedes I, Ponnekanti H, Yazdi Y, Li X. Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrason Imaging. 1991;13(2):111–134. doi:10.1177/016173469101300201
23. European Association for the Study of the Liver. EASL clinical practice guidelines on non-invasive tests for evaluation of liver disease severity and prognosis - 2021 update. J Hepatol. 2021;75(3):659–689. doi:10.1016/j.jhep.2021.05.025
24. Cosgrove D, Barr R, Bojunga J, et al. WFUMB guidelines and recommendations on the clinical use of ultrasound elastography: part 4. Thyroid Ultrasound Med Biol. 2017;43(1):4–26. doi:10.1016/j.ultrasmedbio.2016.06.022
25. Yamaguchi S, Kamei Y, Kozuma S, Taketani Y. Tissue elastography imaging of the uterine cervix during pregnancy. J Med Ultrason. 2007;34(4):209–210. doi:10.1007/s10396-007-0150-2
26. Hamza A, Radosa J, Gerlinger C, Solomayer EF, Ströder R, Meyberg-Solomayer G. Cervical and lower uterine parameter ultrasound and elastographic parameters for the prediction of a successful induction of labor. Ultraschall Med. 2021;42(5):520–528. doi:10.1055/a-1131-7736
27. Ileri A, Yıldırım Karaca S, Gölbaşı H, et al. Diagnostic accuracy of pre-induction cervical elastography, volume, length, and uterocervical angle for the prediction of successful induction of labor with dinoprostone. Arch Gynecol Obstet. 2023;308(4):1301–1311. doi:10.1007/s00404-023-07076-8
28. Wei N, Wang Z. Multivariate analysis of determinants and development of a predictive algorithm for successful labor induction in nulliparous women. BMC Pregnancy Childbirth. 2025;25(1):1207. doi:10.1186/s12884-025-08315-3
29. Lu J, Cheng Y, Ho S, et al. The predictive value of cervical shear wave elastography in the outcome of labor induction. Acta Obstet Gynecol Scand. 2020;99(1):59–68. doi:10.1111/aogs.13706
30. Xie X, Duan T. Obstetrics and Gynecology.
31. Dashe JS, Bloom SL, Spong CY, Hoffman BL. Induction and augmentation of labor [Chapter]. In: Williams Obstetrics.
32. Robinson D, Campbell K, Hobson SR, MacDonald WK, Sawchuck D, Wagner B. Guideline No. 432a: cervical ripening and induction of labour - general information. J Obstet Gynaecol Can. 2023;45(1):35–44.e1. doi:10.1016/j.jogc.2022.11.005
33. Swiatkowska-Freund M, Preis K. Elastography of the uterine cervix: implications for success of induction of labor. Ultrasound Obstet Gynecol. 2011;38(1):52–56. doi:10.1002/uog.9021
34. Obstetrics Subgroup, Chinese Society of Obstetrics and Gynecology, Chinese Medical Association. Expert consensus: new production process standards and handling. Chin J Obstetric Gynecol. 2014;49(7):486.
35. Eggebø TM, Økland I, Heien C, Gjessing LK, Romundstad P, Salvesen KA. Can ultrasound measurements replace digitally assessed elements of the bishop score. Acta Obstet Gynecol Scand. 2009;88(3):325–331. doi:10.1080/00016340902730417
36. Rācene L, Ķīse L, Pitkēviča I, et al. The significance of ultrasound parameters and clinical factors in predicting successful labor induction among nulliparous women. J Matern Fetal Neonatal Med. 2025;38(1):2450405. doi:10.1080/14767058.2025.2450405
37. Londero AP, Schmitz R, Bertozzi S, Driul L, Fruscalzo A. Diagnostic accuracy of cervical elastography in predicting labor induction success: a systematic review and meta-analysis. J Perinat Med. 2016;44(2):167–178. doi:10.1515/jpm-2015-0035
38. Swiatkowska-Freund M, Preis K. Cervical elastography during pregnancy: clinical perspectives. Int J Womens Health. 2017;9:245–254. doi:10.2147/IJWH.S106321
39. Fruscalzo A, Mazza E, Feltovich H, Schmitz R. Cervical elastography during pregnancy: a critical review of current approaches with a focus on controversies and limitations. J Med Ultrason (2001). 2016;43(4):493–504. doi:10.1007/s10396-016-0723-z
40. Agarwal M, Sinha S, Nitu N, et al. Quantitative sonoelastography of the uterine cervix in predicting successful outcome of induction of labour. SAGE Open Med. 2023;11:20503121231166637. doi:10.1177/20503121231166637
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.