Back to Journals » Clinical Interventions in Aging » Volume 15
Cerebral Thrombolysis in Rural Residents Aged ≥ 80
Authors Sobolewski P ![]() , Brola W
, Brola W ![]() , Wilczyński J
, Wilczyński J ![]() , Szczuchniak W, Wójcik T
, Szczuchniak W, Wójcik T ![]() , Wach-Klink A, Kos M, Kozera G
, Wach-Klink A, Kos M, Kozera G ![]()
Received 30 March 2020
Accepted for publication 5 August 2020
Published 24 September 2020 Volume 2020:15 Pages 1737—1751
DOI https://doi.org/10.2147/CIA.S256070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Piotr Sobolewski,1,2 Waldemar Brola,1,3 Jacek Wilczyński,1 Wiktor Szczuchniak,2 Tomasz Wójcik,1 Aleksandra Wach-Klink,2 Marek Kos,2,4 Grzegorz Kozera5
1Collegium Medicum, Jan Kochanowski University, Kielce, Poland; 2Department of Neurology and Stroke Unit, Holy Spirit Specialist Hospital in Sandomierz, Sandomierz, Poland; 3Department of Neurology and Stroke Unit, Saint Lukas Hospital in Końskie, Końskie, Poland; 4Department of Public Health, Medical University of Lublin, Lublin, Poland; 5Medical Simulation Center, Medical University of Gdańsk, Gdańsk, Poland
Correspondence: Piotr Sobolewski
Collegium Medicum, Jan Kochanowski University, 19 IX Wieków Kielc Str, Kielce 25-217, Poland
Tel +48 608510991
Fax +48 158330593
Email [email protected]
Purpose: The proportion of older people in Poland is higher in rural areas than in urban areas. Thus, we aimed to evaluate treatment rate and factors associated with outcome and safety of intravenous thrombolysis (IVT) in rural residents aged ≥ 80 years admitted to primary stroke centers.
Patients and Methods: This study was a retrospective, observational cohort study of 873 patients treated with recombinant tissue plasminogen activator (rt-PA) in primary stroke centers between February 1, 2009 and December 31, 2017. Among them were 527 rural residents and 231 (26.5%) were ≥ 80 years of age. The analyses between rural and urban patients aged ≥ 80 and between rural patients aged < 80 and aged ≥ 80 were performed.
Results: The proportion of patients aged ≥ 80 treated with rt-PA was comparable in rural and urban residents (27.9% vs 24.3% p = 0.24). Rural patients aged ≥ 80 were also characterized by lower incidence of cardiovascular risk factors and better patients’ conditions on admission to hospital. Symptomatic intracerebral hemorrhage rate among ≥ 80-year-old stroke patients was lower in those living in rural areas than in those living in urban areas (5.4% vs 14.3%, p = 0.02); there were no differences regarding mortality and 3-month functional outcome between both populations. The older group of rural patients was characterized by a higher 3-month mortality (28.5% vs 12.6%, p < 0.001) and lower functional independence rate (34.0% vs 50.5%, p < 0.001) than rural younger patients. Antiplatelet (OR 2.43, 95% CI 1.04– 5.66, p = 0.04) and anticoagulant therapy before stroke (OR 3.64, 95% CI 1.21– 10.99, p = 0.022), early ischemic changes in baseline computerized tomograprpahy (OR 2.65, 95% CI 1.03– 6.82, p = 0.043) were associated with unfavorable outcome; and higher National Institute of Health Stroke Scale score on admission (OR 1.01, 95% CI 1.01– 1.20, p = 0.039), higher baseline count of white blood cells (OR 1.33, 95% CI 1.10– 0.62, p = 0.003) were associated with mortality in rural patients over 80.
Conclusion: We suggest that rural patients aged ≥ 80 may be safely treated with IVT in routine practice. However, lower efficacy and a higher mortality must be considered in former use of Vitamin K antagonist and antiplatelet or high white blood cells count.
Keywords: ischemic stroke, rural patients aged ≥ 80, intravenous thrombolysis, atrial fibrillation, VKA
Introduction
Benefits arising from the development of modern diagnostic methods and therapies, as well as healthy lifestyle modifications, resulted in lengthened life expectancy. Thus, demographic characteristics in Poland have shifted with expansion in the oldest-old population. According to information from the Ministry of Health, the highest increase concerned people aged at least 80 and their proportion in Polish population doubled, from just under 2% in 1989 to 4% in 2014.1
Due to the aging population, the number of acute ischemic stroke (AIS) strokes in Poland, as worldwide, is increasing.2,3 In recent years, significant progress of evidence-based care for patients with stroke has resulted in a higher number of specific treatments, including intravenous thrombolysis (IVT) with use of recombinant tissue plasminogen activator (rt-PA) and endovascular procedures.4–6 With the new recommendations, although with certain restrictions, IVT is allowed in patients over 80.7–9 The Polish recommendation (2013) listed age restrictions on IVT which still remains the most frequent method of effective stroke treatment despite the introduction of endovascular thrombectomy.10
The share of older people in the age structure is higher in rural areas than in urban areas.11 Sparse studies have previously reported on the safety and efficacy of thrombolytic therapy in patients from rural regions, showing inequalities compared to urban areas.12–15 However, data regarding specific aspects of IVT therapy in the oldest population are unknown. Thus, we aimed to assess the rate and results of IVT treatment of stroke patients from the rural region in primary stroke units in patients aged ≥80 and to evaluate factors associated with outcome, mortality and presence of hemorrhagic complications (symptomatic intracerebral hemorrhage, SICH).
Patients and Methods
Study Design and Population
This study was a retrospective, two-center, observational cohort study of data collected prospectively from 873 patients consecutively treated with rt-PA at primary stroke centers between 01 February 2009 and 31 December 2017. From this group 527 patients lived in rural areas, and 231 were aged (26.5%) ≥80 years. Recruiting study centers are recognized as stroke units according to the Polish national criteria and international recommendation and are equipped with the proper monitoring and diagnostic facilities.3,16-19 The Emergency Departments (ED) are staffed 24 hours 7 days a week with both a senior neurologist and a senior radiologist.
The tele-stroke services were unavailable for the rural areas considered in our study.
Computed tomography (CT), magnetic resonance imaging (MRI), angio-CT and angio-MRI are easily available within 24 hours. CT scans or less frequently MRI were performed upon admission to the hospital in order to establish the indication for treatment, between 22 and 36 hours and on the seventh day after IVT. To evaluate the etiology of the stroke, transcranial Doppler (TCD), carotid duplex ultrasonography, Holter electrocardiography (Holter ECG), transthoracic echocardiography (TTE) and in the case of some patients transesophagal echocardiography (TEE) were performed. The severity of stroke symptoms was assessed using the National Institute of Health Stroke Scale (NIHSS).20 The 90-day stroke outcomes were measured using the modified Rankin scale (mRS).21 A favorable outcome was defined as an mRS score ≤2 points. In all patients IVT was performed within a regular time window (up to 4.5 hours), five patients who received treatment combined with endovascular intervention were excluded from the analysis.
Hemorrhagic transformation (HT) and SICH rates were assessed according to the ECASS II (European Cooperative Acute Stroke Study II) and III criteria.22,23
The ethics committee approved all data of analysis (Ethics Committee of Świętokrzyska Medical Chamber). All patients consented to the treatment method and participation in the study according to the Declaration of Helsinki.
Statistical Analysis
This study was based on a retrospective data analysis. The comparisons between rural and urban patients aged ≥80 and between rural patients aged <80 and aged ≥80 were performed. Data gathering, characteristics, and univariate analysis were performed using Microsoft Excel 2017. Logistic regression was performed with STATISTICA v. 9.1. All continuous variables were tested for a normal distribution and equality of variances. Because of the non-normality of the variables, non-parametric Mann–Whitney U-tests were used to perform the univariate analysis of the continuous variables. Categorical data were compared using chi square tests; p values <0.05 were considered statistically significant. The multivariate analysis was performed using multiple logistic regression models. Factors identified in the univariate analysis with a p value <0.05 were then examined using a multivariate model.
Results
The proportion of patients aged ≥80 treated with rt-PA did not differ in rural and urban residents (27.9% vs 24.3%, p = 0.24, ChiSq 1.4). SICH rate was lower in rural patients over 80 (5.4% vs 14.3%, p = 0.02); there were no differences regarding mortality and 3-month functional outcome. The older group of rural patients was characterized by lower incidence of cardiovascular risk factors such as arterial hypertension and previous heart infarct, and better patients conditions on admission to hospital, i.e. lower mean arterial pressure (MAP), higher hemoglobin and glomerular filtration rate (GFR) levels, percentage of normal baseline CT and lower incidence of HT and SICH in patients aged ≥80 living in rural areas. Among subjects aged ≥80 years living in rural areas a higher frequency of prior history of transient ischemic attack (TIA) and lower rate of renal insufficiency were found. They have also showed a trend towards a higher presence of atrial fibrillation (AF) (Table 1).
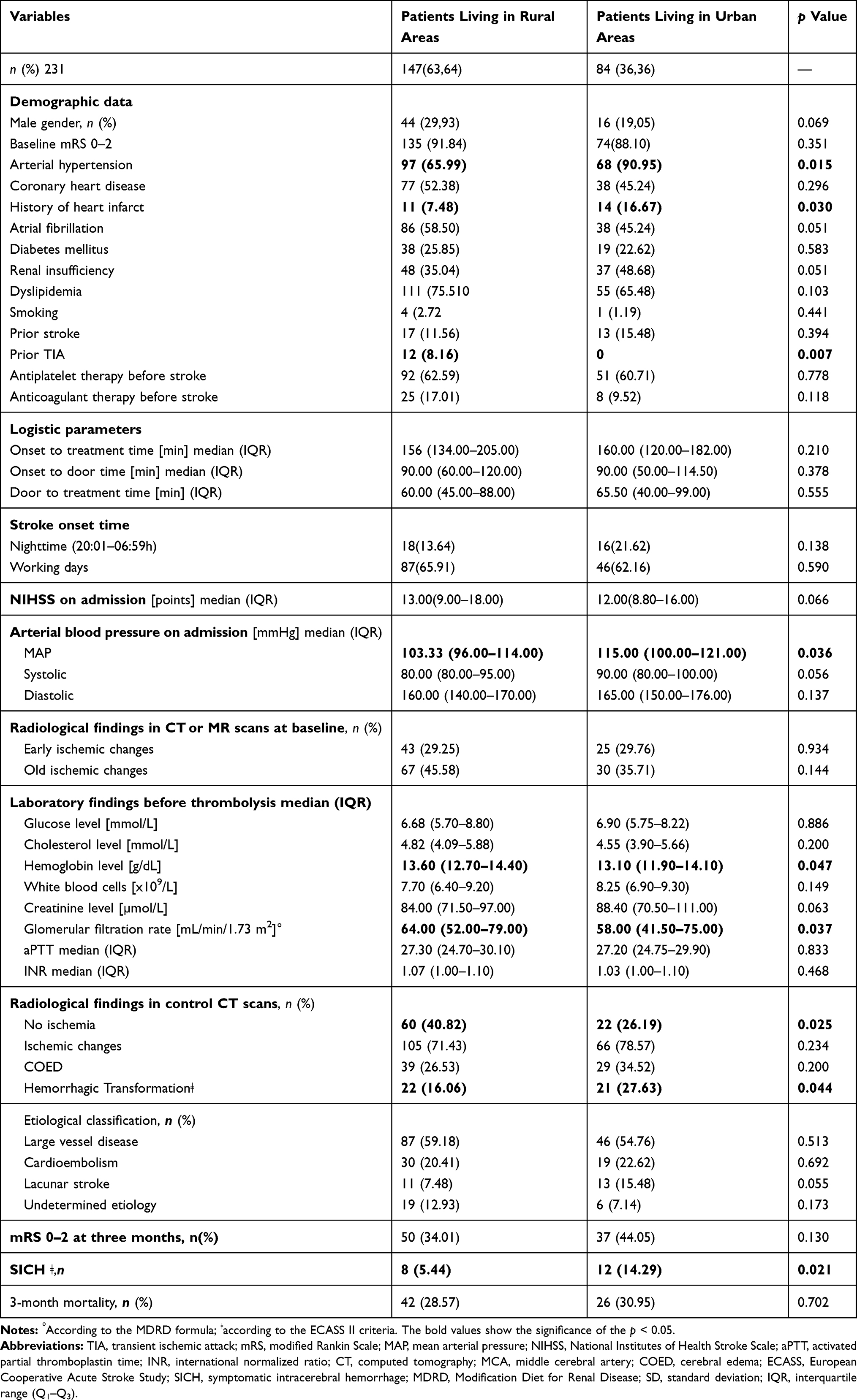 |
Table 1 The Clinical Characteristics of the Subgroups of Stroke Patients Treated with iv-Thrombolysis Aged ≥80 Living in Rural and Urban Areas |
Univariate analysis showed, that patients aged ≥80 living in rural areas were characterized by lower percentage of male gender, prior stroke and TIA, smoker, COED (cerebral edema) in the control CT, nighttime onset of stroke, lacunar stroke, mRS 0–2 after 3 months from stroke onset, SICH, lower MAP, level of GFR, and higher percentage of AF, renal insufficiency, anticoagulant therapy before stroke, old ischemic changes in baseline CT, higher median NIHSS on admission, and higher mortality than patients aged <80 (Table 2).
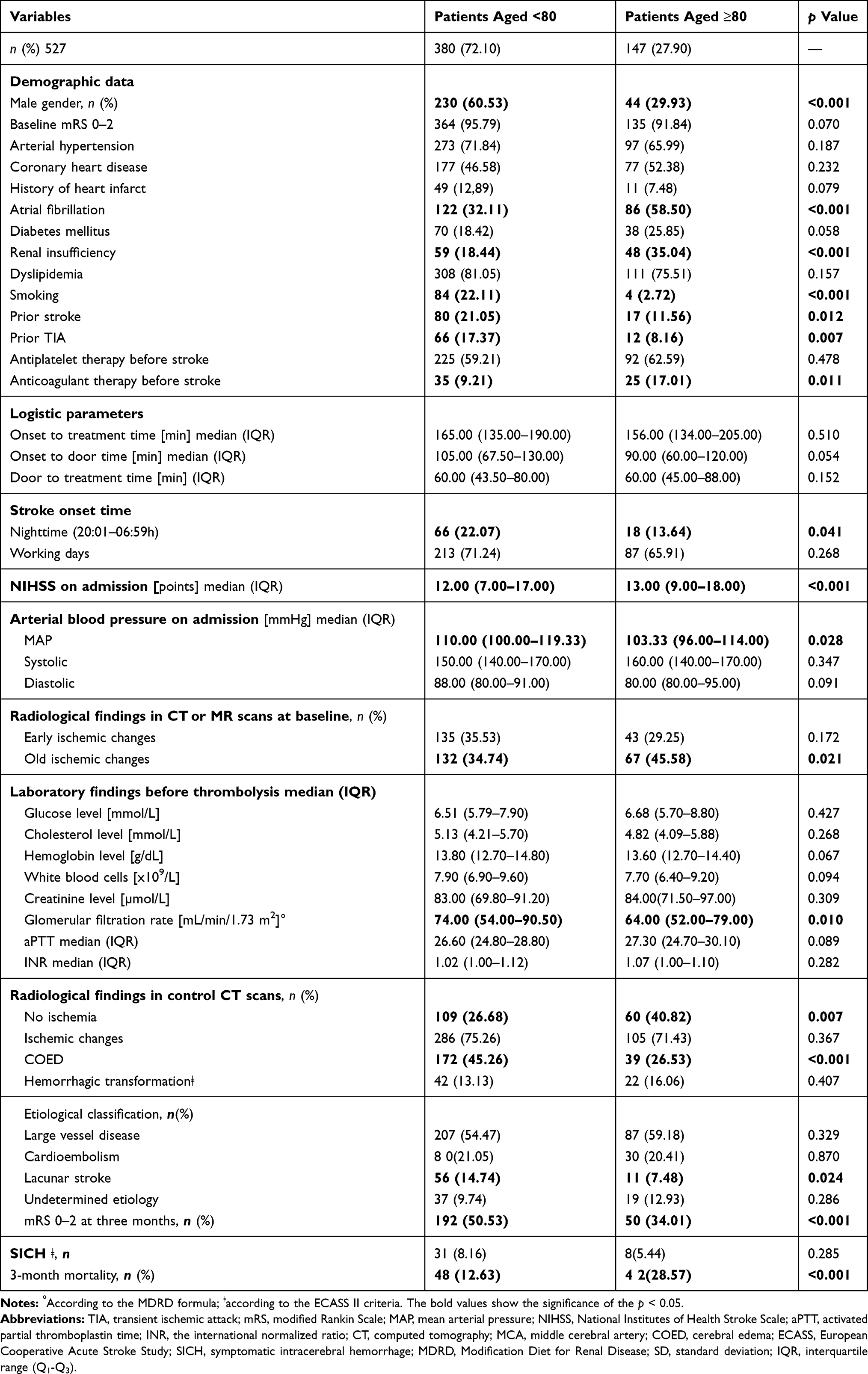 |
Table 2 The Clinical Characteristics of the Subgroups of Stroke Patients Treated with iv-Thrombolysis Aged <80 and ≥80 Living in Rural Regions |
Univariate analysis showed that in group of patients living in rural areas treated with rt-PA AF, prior stroke and TIA, anticoagulant therapy before stroke, ischemic changes and COED in control CT, large vessel disease and SICH, higher median NIHSS, MAP, SBP (systolic blood pressure), lower hemoglobin and GFR level were associated with unfavorable long-term outcome and baseline mRS 0–2 was associated with a lower proportion of unfavorable outcome (mRS 3–5); age ≥89, renal insufficiency, prior TIA, ischemic changes and COED in control CT, large vessel disease, SICH, higher median NIHSS, higher glucose, white blood cells, creatinine and INR (international normalized ratio) level were associated with mortality and shorter median onset-to-door time was associated with lower mortality; and age 80–89 and >89, antiplatelet before stroke, longer onset-to-door time, higher median NIHSS, early ischemic changes in baseline CT, higher cholesterol, white blood cells, INR and lower GFR level, ischemic changes and COED in control CT, large vessel disease and mortality were associated with SICH (Table 3).
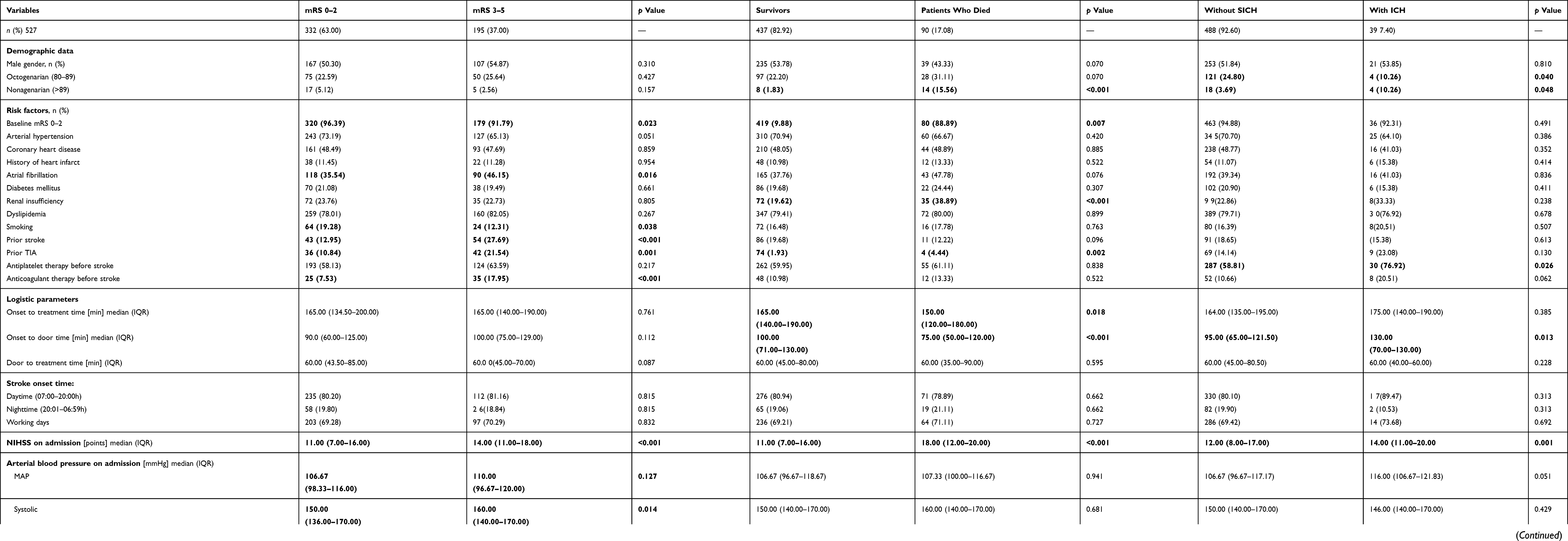 |
Table 3 Univariate Analysis Shoving Factors Associated with Unfavorable Outcome (mRS 3–5), 3-Month Mortality and SICH in Patients Living in Rural Areas |
In patients living in rural areas, multivariate regression analysis identified prior stroke, anticoagulant therapy before stroke, higher NIHSS on admission, SBP, ischemic changes in control CT and LVD (large vessel disease) as a predictor of unfavorable outcome; age ≥80, higher NIHSS on admission, INR and SICH as a predictor of mortality and early ischemic changes, LVD and mortality as a predictor of SICH. Prior TIA and shorter onset-to-door time were a predictor of lower mortality (Figure 1).
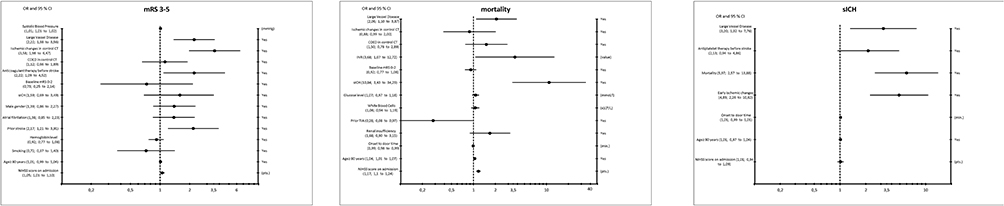 |
Figure 1 Multivariate logistic regression models showing factors associated with 90 days unfavorable outcome, 3-month mortality and SICH in patients treated with iv-thrombolysis living in rural areas. |
Univariate analysis showed that in a group of patients aged ≥80 living in rural areas, female gender, antiplatelet and anticoagulant therapy before stroke, shorter door-to-treatment time, lower MAP, early ischemic changes in baseline CT, ischemic changes and COED in control CT were associated with unfavorable long-term outcome; higher NIHSS, higher baseline count of white blood cells (WBC) and SICH were associated with mortality and higher NIHSS and mortality were associated with SICH (Table 4).
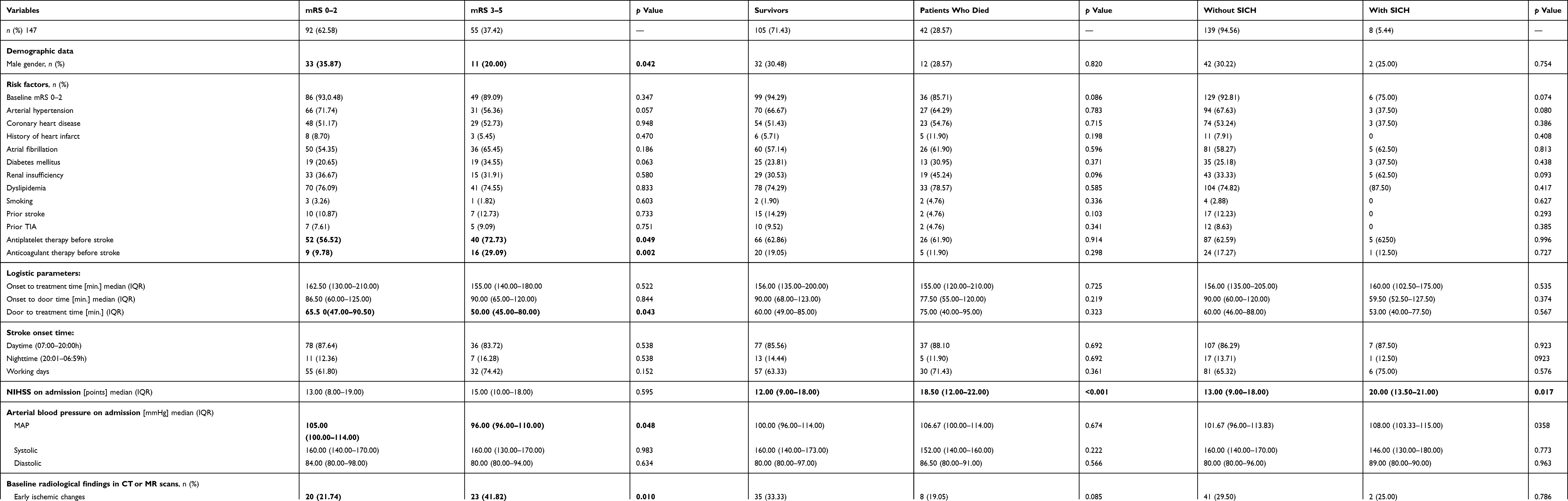 |
Table 4 Univariate Analysis Shoving Factors Associated with Unfavorable Outcome (mRS 3–5), 3-Months Mortality and sICH in Patients Aged ≥80 Living in Rural Areas |
Multivariate regression analysis confirmed that antiplatelet and anticoagulant therapy before stroke and early ischemic changes in baseline CT were predictors of unfavorable long-term outcome in rural octogenarians. Higher NIHSS score on admission and higher baseline count of white blood cells were predictors of mortality and mortality during 90 days after IVT were associated with SICH (Figure 2).
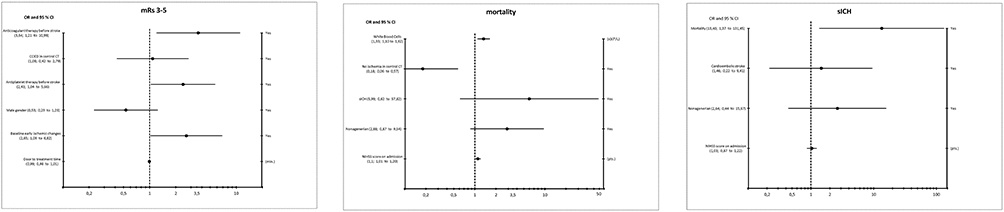 |
Figure 2 Multivariate logistic regression models showing factors associated with 90 days unfavorable outcome, 3-month mortality and SICH in patients aged ≥80 treated with iv-thrombolysis living in rural areas. |
Discussion
This study reports that rural patients over 80 may be effectively and safely treated with IVT in routine practice. Similarly, the former analysis of randomized studies of patients undergoing IVT from the Cochrane Database showed that participants aged over 80 years benefited equally to those aged under 80 years, particularly if treated within 3 hours from stroke onset. This analysis was mainly based on the results of the International Stroke Trial 3 (IST-3) in which 53% of participants were aged over 80.24,25 The beneficial effects of alteplase particularly if given within 3 hours was observed in the Thrombolysis in Elderly Stroke Patients in Italy (TESPI) Trial and the updated meta-analysis showed consistent results with prior estimates. However, all our patients were treated in the time window up to 4.5 hours.26 Regarding our results, lower efficacy and a higher mortality is to be considered in the presence of oral anticoagulant and antiplatelet therapy prior stroke onset and a high WBC count on admission. The latter finding is to be evaluated in further analysis.
The former result showed lower IVT rate in rural patients.14 Because our findings were published 10 years ago, they have indicated noticeable improvement in stroke care quality in rural areas. However, there are no publications discussing the outcome and safety issues or IVT in elderly rural populations. Małopolska region, the area from which patients were recruited for this study, is characterized by very diverse environmental conditions. The terrains are varied, from lowlands to highlands, but only some of them are transformed due to industrialization and urbanization. In the region, there are no highways or expressways in the region, air transport for stroke patients was practically not used. The furthest village from which patients were delivered is located 72 km from the stroke center.
We did not observe differences between rural and urban population over 80 in terms of long-term outcome and mortality. The CANSEART Stroke Study showed that stroke mortality is higher in rural than in urban areas. The authors reckon that the reason is of higher stroke incidence in rural areas rather than stroke care.27 As the results of other studies showed, among high HDI (Human Development Index) countries, stroke mortality was higher in rural than in urban areas in contrast to countries with low HDI in which mortality was higher in the cities.28
Previous studies showed that in many countries, the population living in rural areas is older than in urban areas, which is related to the migration of working-age people to cities.29–31 Our analysis showed that population of patients aged ≥80 living in rural areas characterized by lower incidence of cardiovascular risk factors. Cardiovascular risk factors are slightly different in the rural population than in the urban population;32–34 however, we did not have data for older people. Rural risk factors for health disparities include some kind of geographic isolation, lower socioeconomic status, higher rates of health behaviors, limited access to healthcare specialist, and limited job opportunities.35 Health care for patients from rural and urban areas is different. As shown by a survey conducted in the United States, rural health priorities have changed little in the last decade and access to health care continues to be the most frequently identified health priority.36 The prevalence of cardiovascular risk factors, including arterial hypertension and smoking, in various regions of Poland was mostly explained by varying degrees of urbanization.37
In the population of patients from Peru, hypertension was more prevalent among the urban (29%) compared to the rural group (11%).35 The result of the PURE study showed that in urban communities the awareness, treatment, and control of hypertension were higher compared with rural ones.37 Płaszkiewicz et al have found that in south-eastern Poland between 1997 and 2009 year the number of rural patients with high blood pressure decreased by nearly a half.33 Contrary to the results of the studies presented above, the results of a study by Lindroth et al indicate that residents of rural areas were more often treated for hypertension and hyperlipidemia, hospitalized for myocardial infarction and diagnosed with diabetes; however, after adjusting for age and gender there were no differences.29 An increase of 30% in the prevalence of hypertension in rural populations between 1991 and 2011 was also confirmed by a Chinese study.38
Our results showed the connection between an unfavorable outcome and a finding of early ischemic changes in baseline CT. The presence of early ischemic changes in CT remains one of the questionable inclusion/exclusion criteria for IVT.39 To date, we do not have had clear criteria for assessing early ischemic changes, and in previous randomized trials different criteria were used. Topographic assessment of acute ischemic changes using Alberta Stroke Program Early Computed Tomography Score (ASPECTS) can predict disability, death in anterior circulation stroke and risk of developing SICH.40 Zou at al indicated that diagnosis of hyperdense middle cerebral artery sign is associated with increased risk of HT after IVT but not with SICH.41 A recently published study by Tanaka et al showed that the detection of early ischemic changes using ASPECTS in CT (CT-ASPECT) and in MRI with sequence diffusion weight imaging (DWI-ASPECT) predict SICH in patients with AIS in anterior circulation receiving IVT, but our data did not show such correlation.42
In contrast to previous findings, the impact of antiplatelet and anticoagulant therapy before stroke on unfavorable outcome in analyzed patients was found. Age should not be considered a barrier for implementation of optimal secondary prevention interventions. The available evidence supports benefit from secondary preventive cardiovascular events in the elderly.43 Antiplatelets impair thrombocyte function and might, therefore, increase the risk of SICH in patients undergoing IVT and despite this, the benefit of IVT for AIS is greater in patients using antiplatelets before stroke.44,45 Treatment with antiplatelets is not a contraindication to IVT; however, this does not concern the oldest but all treated patients.46 IVT is allowed for AIS patients on Vitamin K antagonist (VKA) with INR ≤1.7. Literature data suggest that the course of acute-phase cardiogenic stroke and long-term prognosis is more favorable in patients taking oral anticoagulant.47
Octogenarians living in rural areas had a higher incidence of AF compared to patients living in urban areas or younger patients living in rural areas, respectively. However, despite the fact that patients in rural areas had a higher incidence of AF, they had a higher percentage of large vessel occlusions and territorial strokes. That may be explained by the fact, that within the recruitment period, the vast majority of patients used warfarin, as novel oral anticoagulants (NOAC) were not reimbursed by the insurer for AF prophylaxis. Additionally, in all patients qualified for treatment with rt-PA the value of the INR was non-therapeutic (≤1.7). Probably, anticoagulant therapy with warfarin was poorly managed in patients living in rural areas, in terms of adequate monitoring of INR due to logistic reasons: no possibilities to reach the laboratory, unavailable system for collecting blood tests in the patient’s home. This is in line with previous reports showing that residency in rural areas was one of the strongest predictors of uncontrolled anticoagulation and indicated the logistical difficulties of systematically controlling of INR in a rural environment.48–50 In our opinion, this is also a reason why a prior anticoagulant therapy was found as an independent predictor of unfavorable outcome in our cohort of rural patients, including octogenarians. A higher frequency of AF without effective anticoagulation among rural patients from our study group can also explain why they tended toward more severe strokes in terms of baseline NIHSS despite the lower incidence of other cardiovascular risk factors and, apparently, better baseline health status than in the urban counterpart. Similarly, the high NIHSS score in rural patients was indicated in previous studies.51–55
One should be aware that prognosis for elderly patients is less favorable than for younger patients because observational studies suggest slightly higher incidence of SICH.56 Therefore, most of the expert groups’ guidelines recommend caution in the use of rt-PA in patients over 80.
In many studies, including ours, the connection between high baseline NIHSS, high WBC count and mortality has been shown. The severity of the neurological syndrome is the most important factor referring to both the chance of survival and functional status in long-term observation.57 Patients with severe stroke were burdened with much higher risk and worse prognosis than lighter patients.58 Also, previous studies indicated that elevated WBC counts in patients treated with rt-PA predict poor long-term outcome.59
The present study has some limitation. This was an observational study and the group of analyzed patients was not large. Although the data collection was conducted in a prospective study, the analysis was retrospective. The study population was limited to two primary stroke centers and was recruited in anon-industrial area. We did not compare it to industrial populations. Thus, we realize that prospective studies are warranted to evaluate the studied clinical issue due to its growing importance.
Based on our results, we suggest that rural patients aged ≥80 may be safely treated with IVT in routine practice. However, especially in patients who use VKA and antiplatelet therapy, with baseline high NIHSS and with high WBC count, it should be carefully considered, in terms of lower efficacy and higher rate of complications. We believe that our findings provide a certain benefit to the assessment of safety of IVT in elderly patients.
Disclosure
P. Sobolewski has had lectureship fees covered by Boehringer-Ingelheim, Everpharma, Allergan and travel expenses to scientific conferences covered by Boehringer-Ingelheim, Ipsen and Ever Pharma.
W. Brola reports personal fees from Bayer, Sanofi Genzyme, and Novartis, and grants from Biogen, Merck, and Roche, during the conduct of the study. He has received speaker fees from and/or served on Advisory Boards for Bayer, Biogen, Sanofi Genzyme, Merck, Novartis and Roche. He also received support for congress participation, travel and accommodation grants from Biogen, Merck, Roche and Sanofi Genzyme.
G. Kozera’s research activities have been funded by the Ministry of Science and High Education, Poland, Office of the Governor of Pomerania, Poland; he has received speaker’s honoraria from the Boehringer-Ingelheim, Everpharma, Bayer and Phizer.
J. Wilczyski, W. Szczuchniak, T. Wójcik, A. Wach-Klink and M. Kos declare that they have no conflicts of interest in this work.
References
1. Information of the Minister of Health on the impact of demographic changes and an aging population on the organization of the health care system and the National Health Program (on 19.02.2016). Available from: https://stat.gov.pl/files/gfx/portalinformacyjny/pl/defaultaktualnosci/5468/24/1/1/ludnosc_w_wieku_60._struktura_demograficzna_i_zdrowie.pdf.
2. Feigin VL, Forouzanfar MH, Krishnamurthi R, et al. Global burden of diseases, injuries, and risk factors study 2010 (GBD 2010) and the GBD stroke experts group. Global and regional burden of stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet. 2014;383(9913):245–254. doi:10.1016/S0140-6736(13)61953-4
3. Błażejewska-Hyżorek B, Czernuszenko A, Członkowska A, et al. Postępowanie w udarze mózgu: wytyczne Grupy Ekspertów Sekcji Chorób Naczyniowych Polskiego Towarzystwa Neurologicznego. Neurol Neurochir Pol. 2012;46(1):3–78. doi:10.5114/ninp.2012.27179
4. Scott PA, Meurer WJ, Frederiksen SM, et al. A multilevel intervention to increase community hospital use of alteplase for acute stroke (INSTINCT): a cluster-randomised controlled trial. Lancet Neurol. 2013;12(2):139–148. doi:10.1016/S1474-4422(12)70311-3
5. Kunisawa S, Kobayashi D, Lee J, et al. Factors associated with the administration of tissue plasminogen activator for acute ischemic stroke. J Stroke Cerebrovasc Dis. 2014;23(4):724–731. doi:10.1016/j.jstrokecerebrovasdis.2013.06.033
6. Strbian D, Michel P, Ringleb P, et al. Relationship between onset-to-door time and door-to-thrombolysis time: a pooled analysis of 10 dedicated stroke centers. Stroke. 2013;44(10):2808–2813. doi:10.1161/STROKEAHA.113.000995
7. Paul CL, Ryan A, Rose S, et al. How can we improve stroke thrombolysis rates? A review of health system factors and approaches associated with thrombolysis administration rates in acute stroke care. Implement Sci. 2016;11:51. doi:10.1186/s13012-016-0414-6
8. Boulanger JM, Lindsay MP, Gubitz G, et al. Canadian stroke best practice recommendations for acute stroke management: prehospital, emergency department, and acute inpatient stroke care, 6th edition, update 2018. Int J Stroke. 2018;13(9):949–984. doi:10.1177/1747493018786616
9. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the guidelines for early management of acute ischemic stroke: a guideline for health care professionals from American heart association/American stroke association. Stroke. 2019;50(12):e344–e418. doi:10.1161/STR.0000000000000211
10. Błażejewska-Hyżorek B, Czernuszenko A, Członkowska A, et al. Wytyczne postępowania w udarze mózgu. Polski Przeglad Neurologiczny. 2019;15(suppl.A):30–92. doi:10.5603/PPN.2019.0001
11. Stanny M. Demographic changes of the rural population and its labor resources. Polityka Spoleczna. 2012;460(7):1–9.
12. Edwards LL. Using tPA for acute stroke in a rural setting. Neurology. 2007;68(4):292–294. doi:10.1212/01.wnl.0000253190.40728.0c
13. Vaishnav AG, Pettigrew LC, Ryan S. Telephonic guidance of systemic thrombolysis in acute ischemic stroke: safety outcome in rural hospitals. Clin Neurol Neurosurg. 2008;110(5):451–454. doi:10.1016/j.clineuro.2008.01.010
14. Kozera G, Chwojnicki K, Gójska-Grymajlo A, Gasecki D, Schminke U, Nyka WM. Pre-hospital delays and intravenous thrombolysis in urban and rural areas. Acta Neurol Scand. 2012;126(3):171–177. doi:10.1111/j.1600-0404.2011.01616.x
15. Sobolewski P, Szczuchniak W, Sobota A, Grzesik M. Are there differences between rural and urban populations in long-term outcome after systemic cerebral thrombolysis in a hospital located in an agricultural region? Rural Remote Health. 2014;14(4):2867.
16. Członkowska A, Sarzynska-Długosz I, Niewada M, Kobayashi A. Eligibility of stroke units in Poland for administration of intravenous thrombolysis. Eur J Neurol. 2006;13(3):220–224. doi:10.1111/j.1468-1331.2006.01171.x
17. Adams HP, Del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke. A guidelines for the early management of adults with ischemic stroke: a guideline from the American heart association/American stroke association stroke council, clinical cardiology council, cardiovascular radiology and intervention council, and the atherosclerotic peripheral vascular disease and quality of care outcomes in research interdisciplinary working groups. The American academy of neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115(18):e478–e534. doi:10.1161/CIRCULATIONAHA.107.181486
18. Ringleb PA, Bousser MG, Ford G, et al. European stroke organisation (ESO) executive committee; ESO writing committee. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis. 2008;25(5):457–507.
19. Członkowska A, Kobayashi A. Management of acute stroke – guidelines from the expert group of the section of cerebrovascular diseases of the polish neurological society. Update 2013: thrombolysis. Neurol Neurochir Pol. 2013;47(4):303–309. doi:10.5114/ninp.2013.36754
20. Lyden P, Brott T, Tilley B, et al. Improved reliability of the NIH stroke scale using video training. NINDS TPA stroke study group. Stroke. 1994;25(11):2220–2226. doi:10.1161/01.STR.25.11.2220
21. Bonita R, Beaglehole R. Recovery of motor function after stroke. Stroke. 1988;19(12):1497–1500. doi:10.1161/01.STR.19.12.1497
22. Hacke W, Kaste M, Fieschi C, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian acute stroke study investigators. Lancet. 1998;352(9136):1245–1251. doi:10.1016/S0140-6736(98)08020-9
23. for the ECASS Investigators; Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischaemic stroke. N Engl J Med. 2008;359(13):1317–1329. doi:10.1056/NEJMoa0804656
24. IST-3 collaborative group; Sandercock P, Wardlaw JM, Lindley RI, et al. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet. 2012;379(9834):2352–2363. doi:10.1016/S0140-6736(12)60768-5
25. Wardlaw JM, Murray V, Berge E, Del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev. 2014;2014(7):CD000213.
26. Lorenzano S, Vestri A, Bovi P, et al. Thrombolysis in elderly stroke patients in Italy (TESPI) trial and updated meta-analysis of randomized controlled trials [published online ahead of print, 2019 Oct 26]. Int J Stroke. 2019;1747493019884525.
27. Kapral MK, Austin PC, Jeyakumar G, et al. Rural-urban differences in stroke risk factors, incidence, and mortality in people with and without prior stroke the CANHEART stroke study. Circ Cardiovasc Qual Outcomes. 2019;12(2):e004973. doi:10.1161/CIRCOUTCOMES.118.004973
28. Joubert J, Prentice LF, Moulin T, et al. Stroke in rural areas and small communities. Stroke. 2008;39(6):1920–1928. doi:10.1161/STROKEAHA.107.501643
29. Lindroth M, Lundqvist R, Lilja M, Eliasson M. Cardiovascular risk factors differ between rural and urban Sweden: the 2009 Northern Sweden MONICA cohort. BMC Public Health. 2014;14:825. doi:10.1186/1471-2458-14-825
30. Rural population 2014/2015 Department of environment food and rural affairs. Available from: https://www.gov.uk/government/publications/rural-population-and-migration/rural-population-201415.
31. Baernholdt M, Yan G, Hinton I, Rose K, Mattos M. Quality of life in rural and urban adults 65 years and older: findings from the National health and nutrition examination survey. J Rural Health. 2012;28(4):339–347. doi:10.1111/j.1748-0361.2011.00403.x
32. Wach-Klink A, Paciura K, Zwadowska A, Adamczak M, Strojewska W, Frańczak-Prochowski T. The impact of selected cardiovascular factors on the safety and efficacy of intravenous thrombolysis for acute ischemic stroke in routine practice in a rural hospital. Med Stud. 2018;34(3):232–240. doi:10.5114/ms.2018.78687
33. Miranda JJ, Gilman RH, Smeeth L. Differences in cardiovascular risk factors in rural, urban and rural-to-urban migrants in Peru. Heart. 2011;97(10):787–796. doi:10.1136/hrt.2010.218537
34. Chow CK, Teo KK, Rangarajan S, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013;310(9):959–968. doi:10.1001/jama.2013.184182
35. Rural health information hub. Rural health disparities. Available from: https://www.ruralhealthinfo.org/topics/rural-health-disparities.
36. Bolin JN, Bellamy GR, Ferdinand AO, et al. Rural healthy people 2020: new decade, same challenges. J Rural Health. 2015;31(3):326–333. doi:10.1111/jrh.12116
37. Płaczkiewicz D, Puźniak M, Kleinrok A. Prevalence of hypertension and major cardiovascular risk factors in healthy residents of a rural region in south-eastern Poland – 1997–2008/9. Ann Agric Environ Med. 2016;23(3):476–481. doi:10.5604/12321966.1219191
38. Wang J, Ning X, Yang L, et al. Trends of hypertension prevalence, awareness, treatment and control in rural areas of northern China during 1991–2011. J Hum Hypertens. 2014;28(1):25–31. doi:10.1038/jhh.2013.44
39. Wardlaw JM, Dorman PJ, Lewis SC, Sandercock PA. Can stroke physicians and neuroradiologists identify signs of early cerebral infarction on CT? J Neurol Neurosurg Psychiatry. 1999;67(5):651–653. doi:10.1136/jnnp.67.5.651
40. Menon BK, Puetz V, Kochar P, Demchuk AM. ASPECTS and other neuroimaging scores in the triage and prediction of outcome in acute stroke patients. Neuroimaging Clin N Am. 2011;21(2):407–423. doi:10.1016/j.nic.2011.01.007
41. Zou M, Churilov L, He A, Campbell B, Davis SM, Yan B. Hyperdense middle cerebral artery sign is associated with increased risk of hemorrhagic transformation after intravenous thrombolysis for patients with acute ischaemic stroke. J Clin Neurosci. 2013;20(7):984–987. doi:10.1016/j.jocn.2012.10.013
42. Tanaka K, Matsumoto S, Furuta K, et al. Modified diffusion-weighted imaging-Alberta Stroke Program Early Computed Tomography Score including deep white matter lesions predicts symptomatic intracerebral hemorrhage following intravenous thrombolysis. J Thromb Thrombolysis. 2019:1–7. doi:10.1007/s11239-019-01979-7
43. Alhusban A, Fagan SC. Secondary prevention of stroke in the elderly: a review of the evidence. Am J Geriatr Pharmacother. 2011;9(3):143–152. doi:10.1016/j.amjopharm.2011.04.002
44. Uyttenboogaart M, Koch MW, Koopman K, Vroomen PC, De Keyser J, Luijckx GJ. Safety of antiplatelet therapy prior to intravenous thrombolysis in acute ischemic stroke. Arch Neurol. 2008;65(6):607–611. doi:10.1001/archneur.65.5.noc70077
45. Hacke W, Lichy C. Thrombolysis for acute stroke under antiplatelet therapy: safe enough to be beneficial? Nat Rev Neurol. 2008;4(9):474–475. doi:10.1038/ncpneuro0867
46. Diedler J, Ahmed N, Sykora M, et al. Safety of intravenous thrombolysis for acute ischemic stroke in patients receiving antiplatelet therapy at stroke onset. Stroke. 2010;41(2):288–294. doi:10.1161/STROKEAHA.109.559724
47. Xian Y, O’Brien EC, Liang L, et al. Association of predicting Antithrombotic Treatment with acute ischemic stroke severity and in-hospital outcomes among patients with atrial fibrillation. JAMA. 2017;317(10):1057–1067. doi:10.1001/jama.2017.1371
48. Martín-Pérez M, Gaist D, de Abajo FJ, García Rodríguez LA. Predictors of over-anticoagulation in warfarin users in the UK general population: a nested case-control study in a primary health care database. Thromb Haemost. 2019;119(1):66–76. doi:10.1055/s-0038-1676519
49. Le Reste JY, Chiron B, Le Floch B, et al. There are considerable drawbacks to oral anticoagulant for monitoring patients at home which should lead family physicians to discuss alternative or enhanced solutions: a cross-sectional study. BMC Cardiovasc Disord. 2013;13:71. doi:10.1186/1471-2261-13-71
50. Dennis J, Majoni W, Tinsley J, Kangaharan N. Safety and efficacy of warfarin therapy in remote communities of the top end of Northern Australia. Heart Lung Circ. 2017;26(12):1291–1296. doi:10.1016/j.hlc.2017.01.004
51. Wang S, Gross H, Lee SB, et al. Remote evaluation of acute ischemic stroke in rural community hospitals in Georgia. Stroke. 2004;35(7):1763–1768. doi:10.1161/01.STR.0000131858.63829.6e
52. Charipar R, Charipar E. Administration of tissue plasminogen activator for acute ischemic stroke in a rural Wisconsin hospital. WMJ. 2008;107(4):176–180.
53. Muengtaweepongsa S, Prapa-Anantachai P, Dharmasaroja PA. Not only the Sugar, Early infarct sign, hyperDense middle cerebral artery, Age, Neurologic deficit score but also atrial fibrillation is predictive for symptomatic intracranial hemorrhage after intravenous recombinant tissue plasminogen activator. J Neurosci Rural Pract. 2017;8(1):49–54. doi:10.4103/0976-3147.193548
54. Di Carlo A, Lamassa M, Baldereschi M, et al. Risk factors and outcome of subtypes of ischemic stroke. Data from a multicenter multinational hospital-based registry. The European Community Stroke Project. J Neurol Sci. 2006;244(1–2):143–150. doi:10.1016/j.jns.2006.01.016
55. Sandercock P, Bamford J, Dennis M, et al. Atrial fibrillation and stroke: prevalence in different types of stroke and influence on early and long term prognosis (Oxfordshire community stroke project). BMJ. 1992;305:1460–1465. doi:10.1136/bmj.305.6867.1460
56. Touzé E, Gruel Y, Gouin-Thibault I, et al. Intravenous thrombolysis for acute ischaemic stroke in patients on direct oral anticoagulants. Eur J Neurol. 2018;25(5):747–e52. doi:10.1111/ene.13582
57. Demaerschalk BM, Kleindorfer DO, Adeoye OM, et al. American heart association stroke council and council on epidemiology and prevention. Scientific rationale for the inclusion and exclusion criteria for intravenous alteplase in acute ischemic stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(2):581–641. doi:10.1161/STR.0000000000000086
58. Emberson J, Lees KR, Lyden P, et al. Stroke Thrombolysis Trialists’ Collaborative Group. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384(9958):1929–1935. doi:10.1016/S0140-6736(14)60584-5
59. Qu X, Shi J, Cao Y, Zhang M, Xu J. Prognostic value of white blood cells counts and c reactive protein an acut ischemic stroke patients after intravenous thrombolysis. Curr Neurovasc Res. 2018;15(1):10–17. doi:10.2174/1567202615666180326101524
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.