Back to Journals » International Medical Case Reports Journal » Volume 18
Central Corneal Subepithelial Haze Following Keratoplasty With Interrupted Sutures: A Novel Clinical Finding
Authors Kirat O, Hawsawi R, AlHilali S ![]()
Received 13 November 2024
Accepted for publication 15 January 2025
Published 20 January 2025 Volume 2025:18 Pages 131—138
DOI https://doi.org/10.2147/IMCRJ.S504331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Omar Kirat, Rawan Hawsawi, Sara AlHilali
Anterior Segment Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Sara AlHilali, Anterior segment division King Khaled Eye Specialist Hospital, P.O.Box 7191, Riyadh, 11462, Saudi Arabia, Tel +966544017155, Email [email protected]
Purpose: This study aims to describe a newly identified clinical finding of central corneal subepithelial haze following keratoplasty (both penetrating and lamellar) with interrupted sutures, and to explore its causes and management strategies.
Methods: Case series.
Results: The study included 7 males and 3 females, with an average age of 24.89 ± 6.57 years. Eight eyes underwent lamellar keratoplasty, and two underwent penetrating keratoplasty. Subepithelial haze appeared between 2 and 5 months postoperatively, associated with central corneal steepening. The mean BCVA improved from 0.88 ± 0.50 logMAR preoperatively to 0.51 ± 0.20 at haze documentation and 0.50 ± 0.16 after haze resolution. Selective suture removal resulted in haze resolution in 9 eyes, while delayed intervention in one case led to permanent scarring.
Conclusion: Central corneal subepithelial haze following keratoplasty with interrupted sutures is linked to suture tension and central corneal steepening. Early suture adjustment or removal is essential to prevent permanent scarring. Further studies are needed to better understand this complication’s pathophysiology.
Keywords: keratoplasty, sutures, subepithelial, haze
Introduction
The cornea, with its five distinct layers, plays a pivotal role in focusing light onto the retina, and its transparency is essential for clear vision. Any disruption to its structure—whether due to disease, trauma, or surgery—can significantly impair visual quality.1,2 Corneal transplantation, or keratoplasty, can be classified into full-thickness procedures—such as penetrating keratoplasty (PK)—and partial-thickness approaches like anterior lamellar keratoplasty (ALK) and endothelial keratoplasty (EK). These surgical techniques have evolved significantly over the past few decades, offering tailored approaches for different layers of corneal pathology.2
Despite advancements, keratoplasty is not without challenges. Corneal haze, a form of opacity that can impair visual quality, may arise due to various causes after transplantation. Immune-mediated rejection is a significant cause of postoperative haze, particularly in cases of endothelial rejection, which manifests as stromal edema and Descemet’s folds. Microbial keratitis, often due to bacterial or fungal infections, can result in localized or diffuse haze with associated inflammation. Persistent epithelial defects, common in cases with poor epithelial healing, may lead to scarring and haze formation. Similarly, mechanical factors such as uneven suture tension or oversized grafts can cause central corneal steepening or edge thickening, disrupting the tear film and inducing localized subepithelial haze.2
Suture-related complications, in particular, are more prevalent in PK and ALK where interrupted or continuous sutures, or a combination of both, are used.3 The adjustment of sutures intraoperatively and postoperatively plays a pivotal role in determining postoperative corneal curvature and astigmatism, as well as influencing overall graft survival.
While many suture-related complications, such as wound leaks, loose sutures, astigmatism, and cheese-wiring, are well-documented, we describe a new clinical finding observed in patients who underwent PK or lamellar keratoplasty with interrupted sutures. This finding, first noted by the primary author Dr. Kirat, is the presence of central corneal subepithelial haze, a phenomenon not previously reported in the literature and presumed to be linked to the suturing technique.
In this case series, we aim to present and describe this novel observation in a series of 10 eyes, shedding light on its potential implications for postoperative management and long-term visual outcomes following keratoplasty.
Methods
This is a descriptive, retrospective case series involving the clinical evaluation of 10 eyes from patients who developed central corneal subepithelial haze after undergoing keratoplasty for keratoconus. The study adhered to the Declaration of Helsinki and was approved by the Institutional Research Board at King Khaled Eye Specialist Hospital. A written informed consent was obtained from all participants in this study publish the data.
A comprehensive chart review was conducted to collect the following data: patient age, gender, laterality, and type of keratoplasty. Visual acuity assessments included both uncorrected distance visual acuity (UCDVA) and best spectacle corrected distance visual acuity (BSCVA), measured using Snellen charts and subsequently converted to logMAR values for analysis.
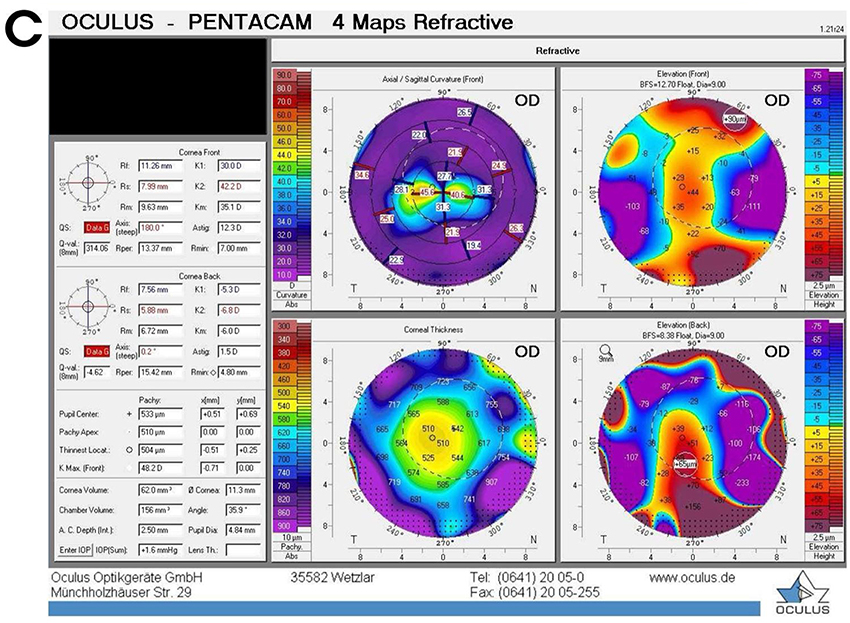
Each patient underwent slit-lamp biomicroscopy, and additional corneal imaging was performed using a Pentacam HR Scheimpflug rotating camera to assess key corneal parameters. These included the thinnest corneal thickness, maximum keratometry values (Kmax), mean keratometry values (Kmean), and corneal astigmatism at 1, 3, and 6 months postoperatively.
Additionally, the onset, progression, and location of corneal haze were documented and analyzed using slit-lamp photography and anterior segment optical coherence tomography (OCT). As this study is a case series involving a small number of eyes (n=10), only descriptive analysis was performed to characterize the clinical findings, without statistical hypothesis testing.
Results
A total of ten eyes from ten patients were included in the analysis, consisting of seven males (70%) and three females (30%). All patients had undergone keratoplasty for keratoconus. Eight eyes underwent lamellar keratoplasty, while two eyes underwent penetrating keratoplasty. Of the surgeries, six were performed on the right eye, and four on the left. (Table 1) The corneal grafts were oversized by 0.25mm relative to the recipient trephination diameter in all cases to ensure adequate graft-host junction stability. None of the included eyes had undergone corneal cross-linking (CXL) prior to keratoplasty, the patients presented with advanced keratoconus, beyond the suitability criteria for CXL.
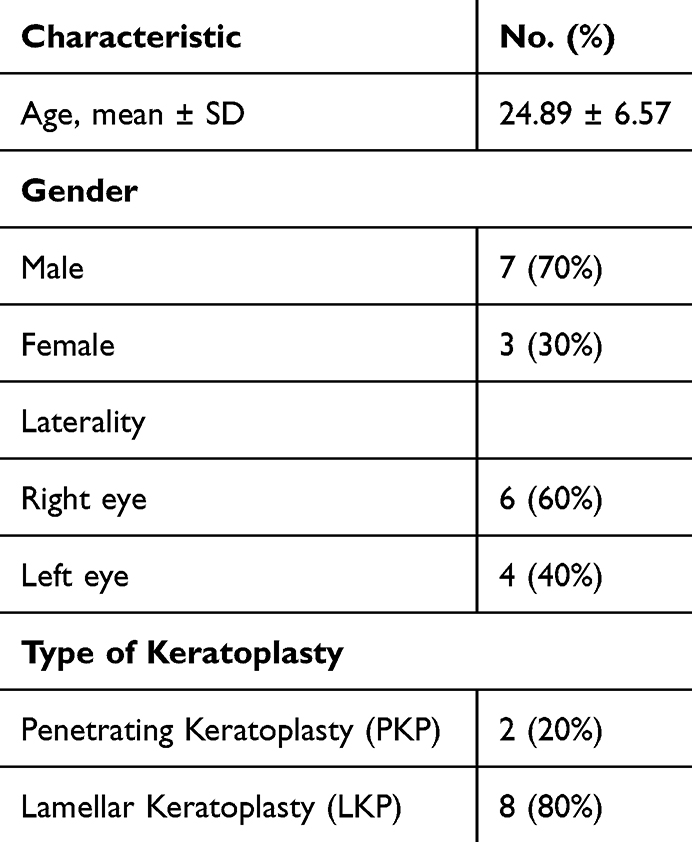 |
Table 1 Participant Characteristics (n=10) |
Preoperative best-corrected visual acuity (BCVA) in logMAR was 0.88 (±0.50). At the time of documented subepithelial haze, BSCVA improved to 0.51 (±0.20), and upon haze resolution, it stabilized at 0.50 (±0.16). Mean keratometry values were noted to be flatter during the presence of the haze, with an average Kmean of 36.9 (±3.3), and showed a slight increase to 43.4 (±1.6) following haze resolution (Table 2).
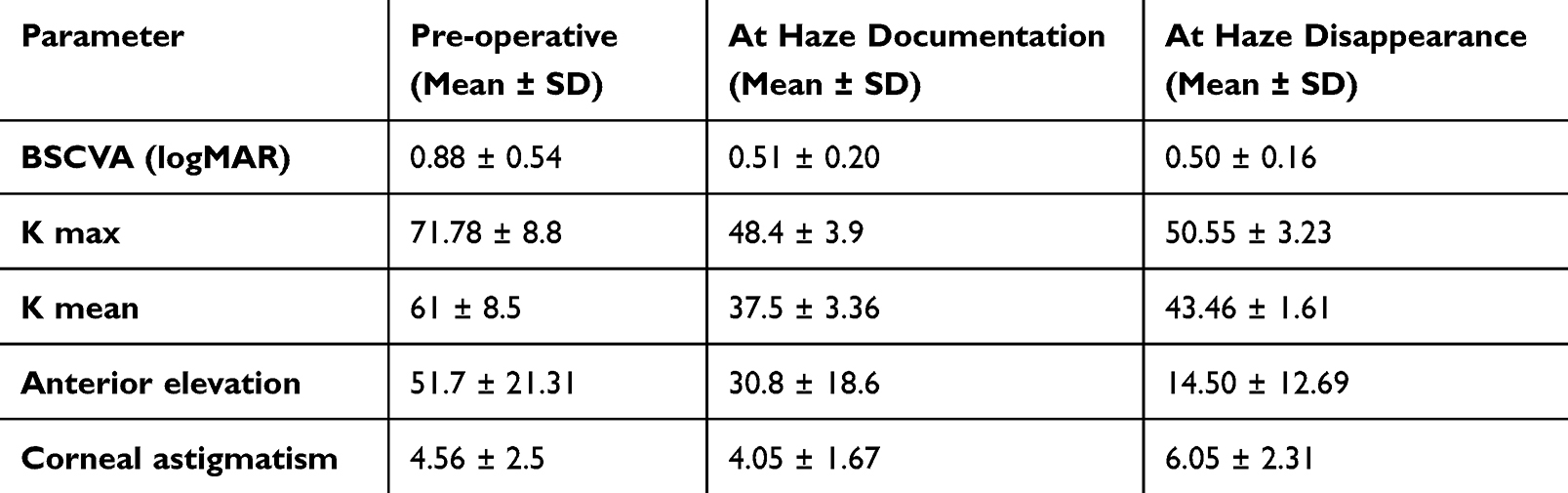 |
Table 2 Clinical Parameters Before Surgery, at Haze Documentation, and Haze Resolution |
Postoperatively, all patients were prescribed prednisolone acetate 1% eye drops in tapering doses over several weeks based on individual clinical progress. None of the patients received cyclosporine during the follow-up period. Preservative-free artificial tears were prescribed to all patients and were used 4–6 times daily.
The subepithelial haze appeared postoperatively and was transient in all cases except one eye which had permanent scarring even after complete suture removal. The median duration from haze documentation to haze resolution was 7 months. The median time from haze documentation to the start of suture removal was 5 months, while the duration from the beginning of suture removal to the resolution of haze was a median of 4 months (Table 3).
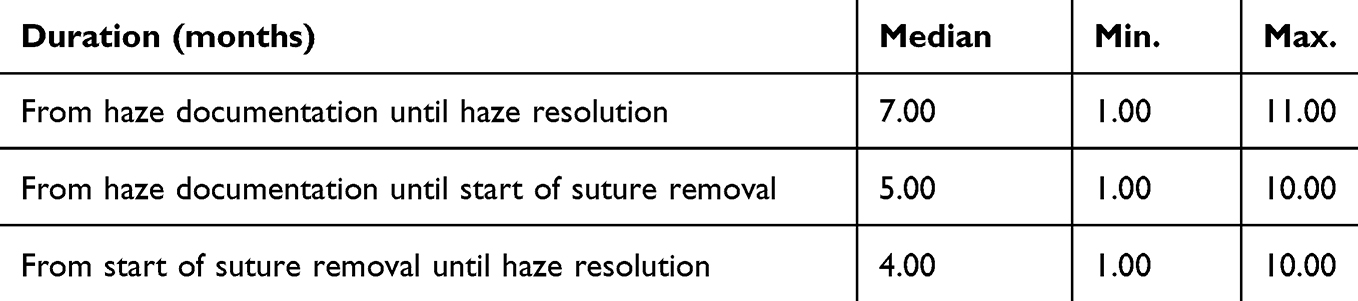 |
Table 3 Durations Related to Haze Onset and Disappearance |
Discussion
Corneal haze, a form of corneal opacity, can manifest at different layers of the cornea depending on the underlying etiology. Subepithelial haze is frequently observed post-refractive surgeries, particularly after procedures like LASIK or PRK, where it is a known complication of epithelial disruption.4–6 In contrast, stromal haze can emerge after interventions like corneal crosslinking (CXL), often regarded as an indication of successful treatment.7,8 However, corneal haze is not exclusive to these procedures and can arise as part of the healing process following surgical or infectious insults to the corneal tissue.
While corneal haze generally has a limited impact on visual acuity, in some cases, it can significantly degrade the quality of vision by inducing light scatter.9 This is particularly concerning for patients whose visual function may be compromised even in the absence of significant changes in corrected visual acuity.9 In our study, we describe a novel pattern of corneal subepithelial haze that appeared centrally following keratoplasty with interrupted sutures, occurring in both lamellar and penetrating procedures for keratoconus patients.
In all 10 eyes, the subepithelial haze developed centrally, in the graft zone, where the most significant elevation occurred due to tight sutures. (Figure 1) This pattern is unique and previously unreported in the literature, first recognized and described by Dr. Kirat. The onset of haze ranged from as early as two months postoperatively to as late as 5 months, illustrating the variability in the healing process and the potential delayed effects of suture tension on corneal architecture.
 |
Figure 1 (A–C) Slit lamp photography of three eyes with central corneal subepithelial haze. |
The haze was typically accompanied by a steepening of the central cornea and flattening of the periphery, a phenomenon well-documented by corneal topography. (Figure 2) This steep central zone, juxtaposed against a flatter periphery, suggests an imbalance in suture tension leading to localized stress on the corneal surface. Anterior segment OCT revealed central and anterior hyper-reflectivity at the site of corneal haze, further confirming the localized nature of the corneal changes. (Figure 3) Interestingly, the haze resolved in all cases except one following selective suture removal, highlighting the importance of early intervention. In one eye, the delay in suture removal led to permanent central scarring, emphasizing the need for timely management. Figure 2 Continued. Figure 2 (A–C) Pentacam images of three eyes with central corneal subepithelial haze showing central steepening with flattening of the corneal periphery.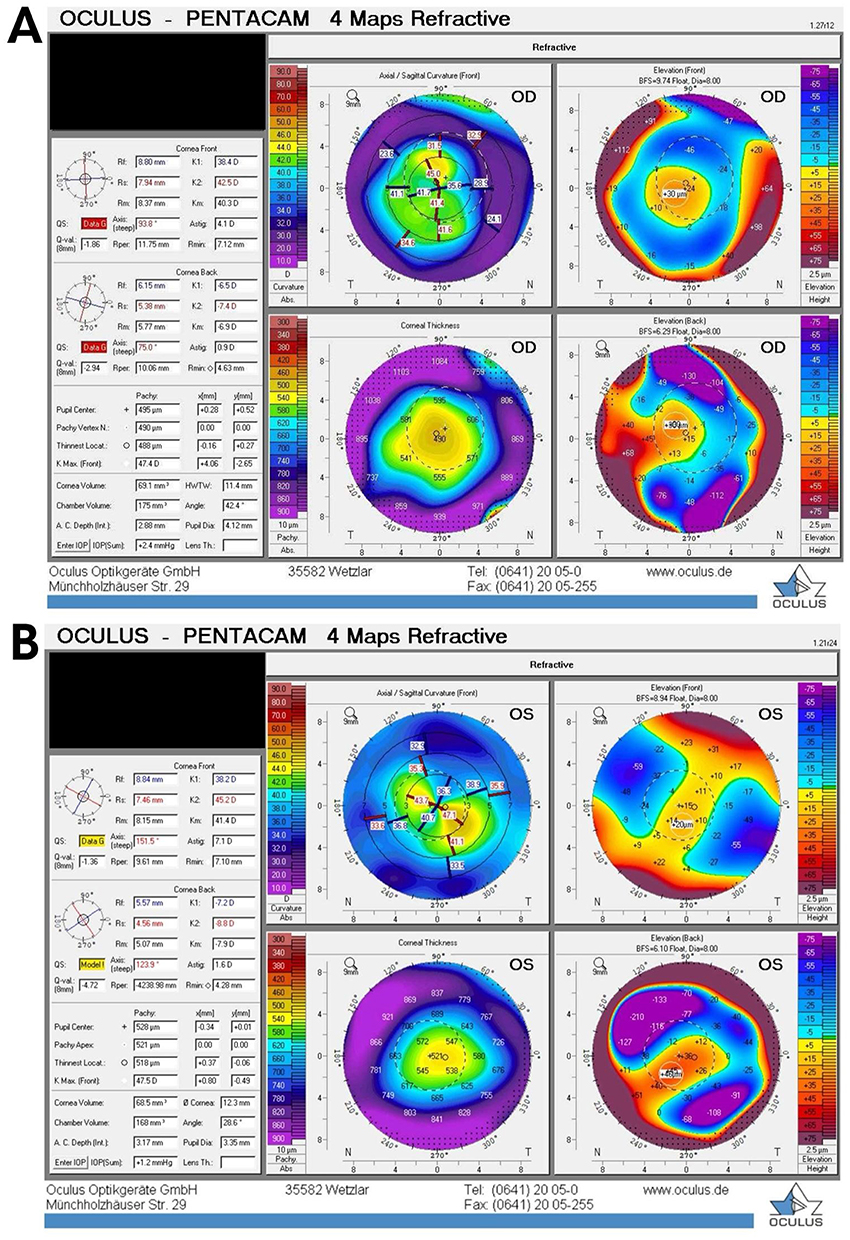
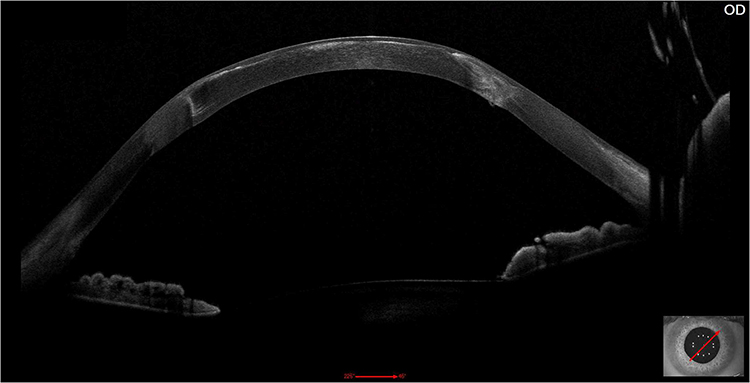 |
Figure 3 Anterior segment OCT showing the central and anterior hyper-reflectivity at the site of corneal subepithelial haze. |
The role of tight sutures in inducing corneal haze likely extends beyond simple mechanical distortion of the cornea. We hypothesize that the significant central steepening, which disrupts the tear film, could contribute to the development of haze by causing localized corneal dryness.10 This mechanism has been observed in other conditions characterized by corneal steepening, such as in hyperopic corrections post-LASIK or PRK, where central stromal necrosis and subepithelial scarring are linked to an irregular tear film and subsequent dry eye syndrome.4,5
A related observation is that of Kaye’s dots, which have been linked to tight sutures.11 These dots may reflect abnormal epithelial healing at the periphery of graft and are often associated with an iron line in the affected area.11 Typically, Kaye’s dots resolve rapidly after suture removal, except in cases where subepithelial fibrosis has developed in the same region of tight sutures.12 Over time, excessively tight sutures may also lead to subepithelial fibrosis, and keratoscopic examination can reveal flattening of the corneal surface in such areas.12
Our study sheds light on a newly identified complication of keratoplasty involving interrupted sutures, where significant central steepening, induced by tight sutures, can lead to the development of a central subepithelial haze. This finding underscores the critical importance of suture management in the postoperative period, not only for controlling astigmatism but also for preventing secondary complications such as haze and, potentially, permanent scarring. Early intervention, either through suture adjustment or selective suture removal, can prevent the progression of haze and mitigate the risk of permanent visual impairment.
While the visual acuity in our patients remained largely unaffected, the presence of haze did have implications for visual quality. This highlights the need for ophthalmic surgeons to be vigilant in postoperative management, particularly in the early detection of haze, and to adopt prompt intervention strategies.
The limitations of our study include the small sample size and the absence of histopathological analysis to further elucidate the underlying mechanism of haze formation. Future studies with larger cohorts and a detailed histological examination of the corneal tissue are necessary to fully understand the pathophysiology of this phenomenon. Nonetheless, our findings contribute valuable insights into the relationship between suture tension and corneal healing, and we advocate for heightened awareness among corneal surgeons of this potential complication.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. DelMonte DW, Kim T. Anatomy and physiology of the cornea. J Cataract Refract Surg. 2011;37:588–598. doi:10.1016/J.JCRS.2010.12.037
2. Liu S, Wong YL, Walkden A. Current perspectives on corneal transplantation. Clin Ophthalmol. 2022;16:631–646. doi:10.2147/OPTH.S289359
3. Christo CG, Van Rooij J, Geerards AJM, et al. Suture-related complications following keratoplasty: a 5-year retrospective study. Cornea. 2001;20:816–819. doi:10.1097/00003226-200111000-00008
4. Pietilä J, Mäkinen P, Pajari S, et al. Excimer laser photorefractive keratectomy for hyperopia. J Refract Surg. 1997;13:504–510. doi:10.3928/1081-597X-19970901-06
5. Prasher P. Salzmann nodular degeneration after photorefractive keratectomy for hyperopia. Asian J Ophthalmol. 2015;14:77–81. doi:10.35119/ASJOO.V14I2.101
6. Moshirfar M, Wang Q, Theis J, et al. Management of corneal haze after photorefractive keratectomy. Ophthalmol Ther. 2023;12:2841. doi:10.1007/S40123-023-00782-1
7. Kim BZ, Jordan CA, McGhee CNJ, et al. Natural history of corneal haze after corneal collagen crosslinking in keratoconus using scheimpflug analysis. J Cataract Refract Surg. 2016;42:1053–1059. doi:10.1016/J.JCRS.2016.04.019
8. Peponis V, Kontomichos L, Chatziralli I, et al. Late onset corneal haze after corneal cross-linking for progressive keratoconus. Am J Ophthalmol Case Rep. 2019;14:64. doi:10.1016/J.AJOC.2019.02.008
9. Spadea L, Maraone G, Verboschi F, et al. Effect of corneal light scatter on vision: a review of the literature. Int J Ophthalmol. 2016;9:459. doi:10.18240/IJO.2016.03.24
10. Meyer JJ, Gokul A, Wang MTM, et al. Alterations in the ocular surface and tear film following keratoplasty. Scientific Rep. 2022;12(1):1–6. doi:10.1038/s41598-022-16191-6
11. Kaye DB. Epithelial response in penetrating keratoplasty. Am J Ophthalmol. 1980;89:381–387. doi:10.1016/0002-9394(80)90008-2
12. Geggel HS. Effect of peripheral subepithelial fibrosis on corneal transplant topography. J Cataract Refract Surg. 1996;22:135–138. doi:10.1016/S0886-3350(96)80282-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.